

Are Ratings of Perceived Exertion during Endurance Tasks of Predictive Value? Findings in Trunk Muscles Require Special Attention


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
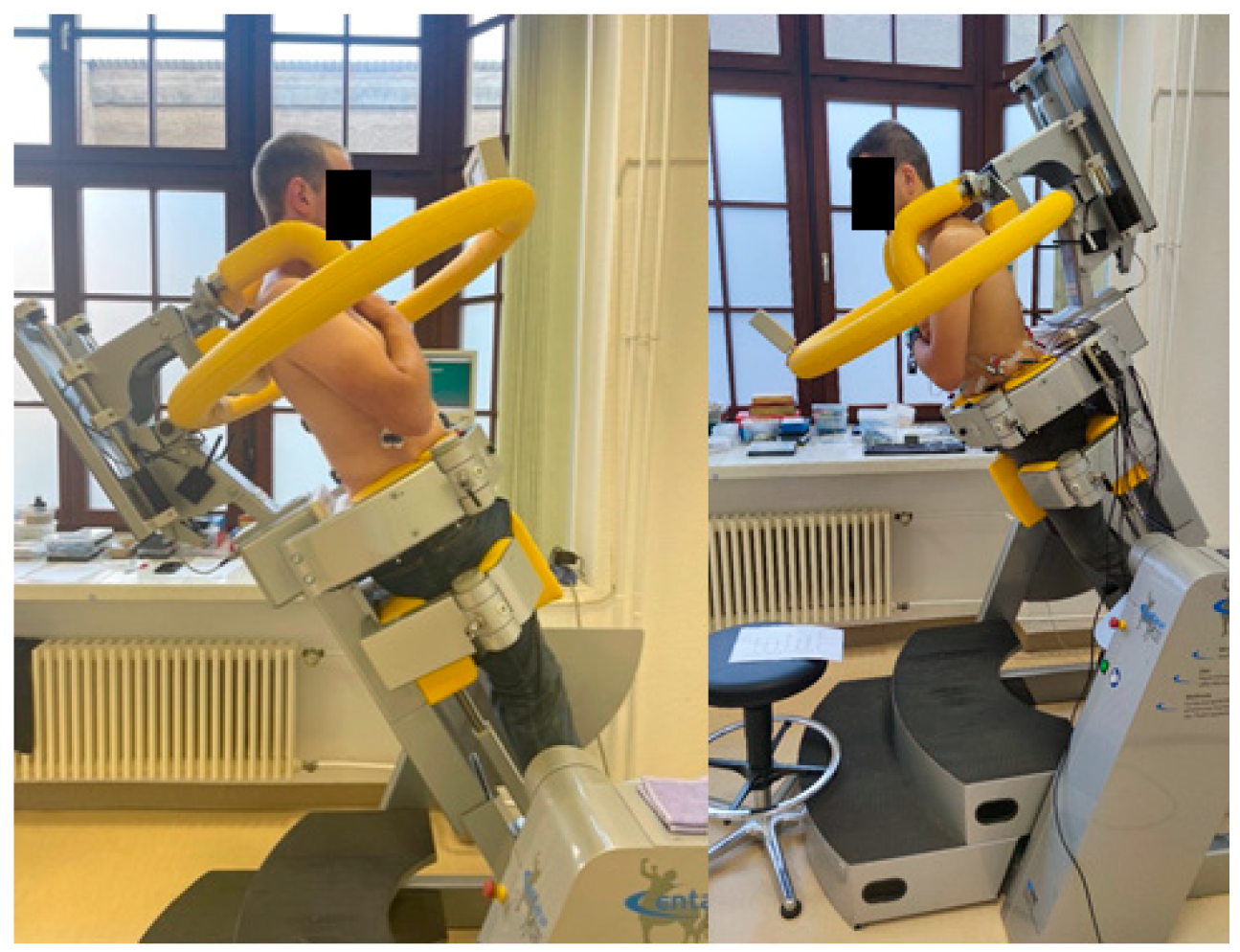
2.2. Investigation
2.3. Definition of Subgroups
2.4. Data Analysis and Statistics
3. Results
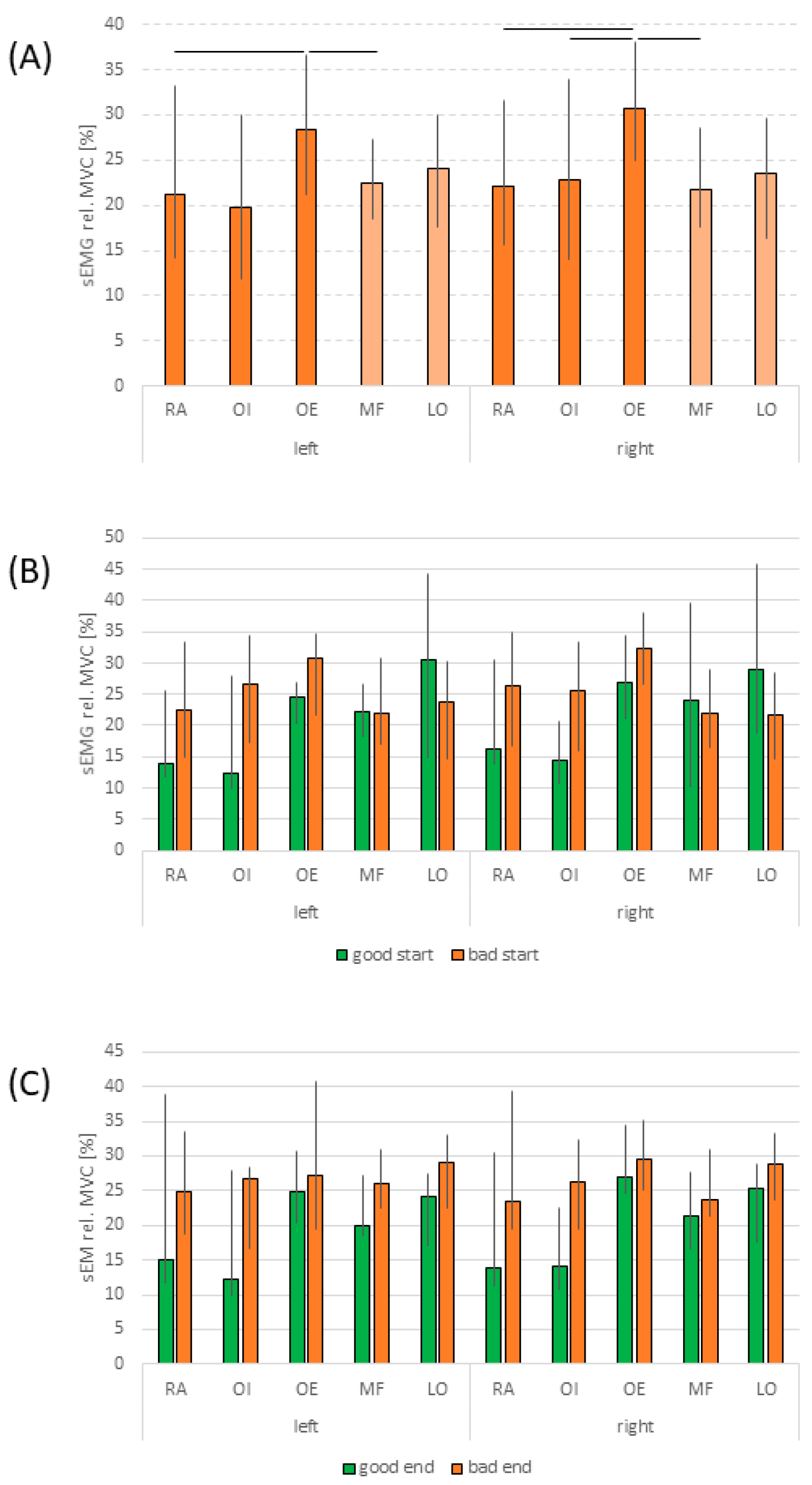
3.1. Relative Load Levels of Muscles
3.2. Perceived Exertion
4. Discussion
Limitations
5. Conclusions
Practical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luttmann, A.; Jäger, M.; Sökeland, J.; Laurig, W. Electromyographical study on surgeons in urology. II Determination of muscular fatigue. Ergonomics 1996, 39, 298–313. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, G.V.; Arabadzhiev, T.I.; Hogrel, J.Y.; Dimitrova, N.A. Simulation analysis of interference EMG during fatiguing voluntary contractions. Part II—Changes in amplitude and spectral characteristics. J. Electromyogr. Kinesiol. 2008, 18, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, N.A.; Dimitrov, G.V. Interpretation of EMG changes with fatigue: Facts, pitfalls, and fallacies. J. Electromyogr. Kinesiol. 2003, 13, 13–36. [Google Scholar] [CrossRef]
- Clark, B.C.; Collier, S.R.; Manini, T.M.; Ploutz-Snyder, L.L. Sex differences in muscle fatigability and activation patterns of the human quadriceps femoris. Eur. J. Appl. Physiol. 2005, 94, 196–206. [Google Scholar] [CrossRef]
- Champagne, A.; Descarreaux, M.; Lafond, D. Back and hip extensor muscles fatigue in healthy subjects: Task-dependency effect of two variants of the Sorensen test. Eur. Spine J. 2008, 17, 1721–1726. [Google Scholar] [CrossRef]
- Mörl, F.; Anders, C.; Grassme, R. An easy and robust method for ECG artifact elimination of SEMG signals. In Proceedings of the XVII Congress of the International Society of Electrophysiology and Kinesiology, Aalborg, Denmark, 16–19 June 2010. [Google Scholar]
- Jo, D.; Bilodeau, M. Rating of perceived exertion (RPE) in studies of fatigue-induced postural control alterations in healthy adults: Scoping review of quantitative evidence. Gait Posture 2021, 90, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Masumoto, K.; Shono, T.; Hotta, N.; Fujishima, K. Muscle activation, cardiorespiratory response, and rating of perceived exertion in older subjects while walking in water and on dry land. J. Electromyogr. Kinesiol. 2008, 18, 581–590. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [CrossRef]
- Mottram, C.J.; Jakobi, J.M.; Semmler, J.G.; Enoka, R.M. Motor-unit activity differs with load type during a fatiguing contraction. J. Neurophysiol. 2005, 93, 1381–1392. [Google Scholar] [CrossRef]
- Staiano, W.; Bosio, A.; de Morree, H.M.; Rampinini, E.; Marcora, S. The cardinal exercise stopper: Muscle fatigue, muscle pain or perception of effort? Prog. Brain Res. 2018, 240, 175–200. [Google Scholar] [CrossRef] [PubMed]
- Barroso, R.; Cardoso, R.K.; do Carmo, E.C.; Tricoli, V. Perceived exertion in coaches and young swimmers with different training experience. Int. J. Sports Physiol. Perform. 2014, 9, 212–216. [Google Scholar] [CrossRef]
- Daikoku, R.; Saito, Y. Differences between novice and experienced caregivers in muscle activity and perceived exertion while repositioning bedridden patients. J. Physiol. Anthropol. 2008, 27, 333–339. [Google Scholar] [CrossRef]
- Mahon, A.D.; Gay, J.A.; Stolen, K.Q. Differentiated ratings of perceived exertion at ventilatory threshold in children and adults. Eur. J. Appl. Physiol. Occup. Physiol. 1998, 78, 115–120. [Google Scholar] [CrossRef]
- Essendrop, M.; Schibye, B.; Hye-Knudsen, C. Intra-abdominal pressure increases during exhausting back extension in humans. Eur. J. Appl. Physiol. 2002, 87, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Schönau, T.; Anders, C. Force capacity of trunk muscle extension and flexion in healthy inactive, endurance and strength-trained subjects—A pilot study. Ger. J. Exerc. Sport. Res. 2023, 54, 213–220. [Google Scholar] [CrossRef]
- Kállai, I.; Barke, A.; Voss, U. The effects of experimenter characteristics on pain reports in women and men. Pain 2004, 112, 142–147. [Google Scholar] [CrossRef]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Kendall, F.P.; Kendall Mc Geary, E.; Provance, P.G.; Rodgers, M.M.; Romani, W.A. Muscles Testing and Function with Posture and Pain, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Haggmark, T.; Thorstensson, A. Fibre types in human abdominal muscles. Acta Physiol. Scand. 1979, 107, 319–325. [Google Scholar] [CrossRef]
- Thorstensson, A.; Carlson, H. Fibre types in human lumbar back muscles. Acta Physiol. Scand. 1987, 131, 195–202. [Google Scholar] [CrossRef]
- Johnson, M.A.; Polgar, J.; Weightman, D.; Appleton, D. Data on the distribution of fibre types in thirty-six human muscles. An autopsy study. J. Neurol. Sci. 1973, 18, 111–129. [Google Scholar] [CrossRef] [PubMed]
- Kalimo, H.; Rantanen, J.; Viljanen, T.; Einola, S. Lumbar muscles: Structure and function. Ann. Med. 1989, 21, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Mannion, A.F. Fibre type characteristics and function of the human paraspinal muscles: Normal values and changes in association with low back pain. J. Electromyogr. Kinesiol. 1999, 9, 363–377. [Google Scholar] [CrossRef]
- Sirca, A.; Kostevc, V. The fibre type composition of thoracic and lumbar paravertebral muscles in man. J. Anat. 1985, 141, 131–137. [Google Scholar]
- Hansen, L.; Anders, C. Influence of different control strategies on muscle activation patterns in trunk muscles. Physiol. Rep. 2014, 2, e12229. [Google Scholar] [CrossRef]
- Hansen, L.C.; Anders, C. Trunk muscle amplitude-force relationship is only quantitatively influenced by control strategy. J. Biomech. 2016, 49, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Perdios, A.; Sawatzky, B.J.; Sheel, A.W. Effects of camber on wheeling efficiency in the experienced and inexperienced wheelchair user. J. Rehabil. Res. Dev. 2007, 44, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Manini, T.M.; The, D.J.; Doldo, N.A.; Ploutz-Snyder, L.L. Gender differences in skeletal muscle fatigability are related to contraction type and EMG spectral compression. J. Appl. Physiol. 2003, 94, 2263–2272. [Google Scholar] [CrossRef]
- Adedoyin, R.A.; Mbada, C.E.; Farotimi, A.O.; Johnson, O.E.; Emechete, A.A.I. Endurance of low back musculature: Normative data for adults. J. Back. Musculoskelet. Rehabil. 2011, 24, 101–109. [Google Scholar] [CrossRef]
- Nuzzo, J.L. Narrative Review of Sex Differences in Muscle Strength, Endurance, Activation, Size, Fiber Type, and Strength Training Participation Rates, Preferences, Motivations, Injuries, and Neuromuscular Adaptations. J. Strength. Cond. Res./Natl. Strength. Cond. Assoc. 2023, 37, 494–536. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Age [years] | Height [cm] | Weight [kg] | BMI [kg/m2] | |
|---|---|---|---|---|---|
| Study I | |||||
| Female (n = 24) | MW | 34.8 | 167.6 | 65.3 | 23.3 |
| SD | 7.5 | 7.0 | 7.1 | 2.7 | |
| Min | 25 | 158 | 79.4 | 19.4 | |
| Max | 47 | 186 | 51.3 | 27.9 | |
| Male (n = 23) | MW | 31.7 | 181.0 | 77.9 | 23.8 |
| SD | 5.8 | 6.0 | 8.3 | 2.1 | |
| Min | 49 | 193 | 59.8 | 20.0 | |
| Max | 25 | 168 | 94.3 | 27.0 | |
| Statistics | p-value | 0.12 | <0.01 | <0.01 | 0.52 |
| ES | 0.46 | 2.05 | 1.63 | 0.19 | |
| Study II | |||||
| Female (n = 17) | MW | 35.3 | 167.2 | 65.4 | 23.3 |
| SD | 10.0 | 7.0 | 12.2 | 3.4 | |
| Min | 24 | 154 | 41 | 16.0 | |
| Max | 48 | 180 | 91.4 | 29.2 | |
| Male (n = 15) | MW | 41.3 | 179.6 | 81.6 | 25.3 |
| SD | 6.6 | 5.2 | 8.1 | 2.1 | |
| Min | 24 | 165 | 70.8 | 21.1 | |
| Max | 52 | 190 | 103.0 | 31.5 | |
| Statistics | p-value | 0.06 | <0.01 | <0.01 | 0.06 |
| ES | 0.71 | 2.02 | 1.56 | 0.70 | |
| Study I vs. II | |||||
| Female | p-value | 0.84 | 0.88 | 0.98 | 0.97 |
| ES | 0.06 | 0.05 | 0.01 | 0.01 | |
| Male | p-value | <0.01 | 0.48 | 0.19 | 0.04 |
| ES | 1.55 | 0.24 | 0.44 | 0.71 |
| Mean | SD | Median | u. Q. | l. Q. | Max | Min | |
|---|---|---|---|---|---|---|---|
| Substudy I | |||||||
| Good start (n = 11) | 6.7 | 0.5 | 7.0 | 7.0 | 6.5 | 7 | 6 |
| Bad start (n = 12) | 11.3 | 0.5 | 11.0 | 11.0 | 11.25 | 11 | 12 |
| Good end (n = 13) | 12.8 | 2.0 | 14.0 | 14.0 | 13.0 | 14 | 7 |
| Bad end (n = 13) | 19.5 | 0.5 | 20.0 | 20.0 | 19.0 | 19 | 20 |
| Substudy II | |||||||
| Good start (n = 9) | 6.8 | 0.4 | 7.0 | 7.0 | 7.0 | 7 | 6 |
| Bad start (n = 14) | 11.6 | 0.7 | 11.5 | 11.0 | 12.0 | 13 | 11 |
| Good end (n = 10) | 15.6 | 0.5 | 16.0 | 17.0 | 16.0 | 16 | 15 |
| Bad end (n = 8) | 20.0 | 0.0 | 20.0 | 20.0 | 20.0 | 20 | 20 |
| Time [s] | 60 | 120 | 180 | 240 | 300 | 360 | 420 | 480 | 540 | 600 |
|---|---|---|---|---|---|---|---|---|---|---|
| Abdominal muscles | ||||||||||
| Start | 0.86 | 0.85 | 0.84 | 0.77 | 0.59 | 0.56 | 0.53 | 0.50 | 0.49 | 0.50 |
| End | 0.50 | 0.69 | 0.70 | 0.81 | 0.85 | 0.85 | 0.86 | 0.85 | 0.86 | 0.90 |
| Back muscles | ||||||||||
| Start | 0.90 | 0.86 | 0.80 | 0.60 | 0.27 | 0.01 | 0.12 | 0.17 | 0.21 | 0.21 |
| End | 0.20 | 0.01 | 0.24 | 0.63 | 0.87 | 0.91 | 0.92 | 0.92 | 0.92 | 0.93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anders, C.; Mader, L.S.; Herzberg, M.; Alex, C. Are Ratings of Perceived Exertion during Endurance Tasks of Predictive Value? Findings in Trunk Muscles Require Special Attention. J. Funct. Morphol. Kinesiol. 2024, 9, 180. https://doi.org/10.3390/jfmk9040180
Anders C, Mader LS, Herzberg M, Alex C. Are Ratings of Perceived Exertion during Endurance Tasks of Predictive Value? Findings in Trunk Muscles Require Special Attention. Journal of Functional Morphology and Kinesiology. 2024; 9(4):180. https://doi.org/10.3390/jfmk9040180
Chicago/Turabian StyleAnders, Christoph, Lena Simone Mader, Max Herzberg, and Christin Alex. 2024. "Are Ratings of Perceived Exertion during Endurance Tasks of Predictive Value? Findings in Trunk Muscles Require Special Attention" Journal of Functional Morphology and Kinesiology 9, no. 4: 180. https://doi.org/10.3390/jfmk9040180
APA StyleAnders, C., Mader, L. S., Herzberg, M., & Alex, C. (2024). Are Ratings of Perceived Exertion during Endurance Tasks of Predictive Value? Findings in Trunk Muscles Require Special Attention. Journal of Functional Morphology and Kinesiology, 9(4), 180. https://doi.org/10.3390/jfmk9040180