
Does Pelvic Tilt Angle Influence the Isokinetic Strength of the Hip and Knee Flexors and Extensors?



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
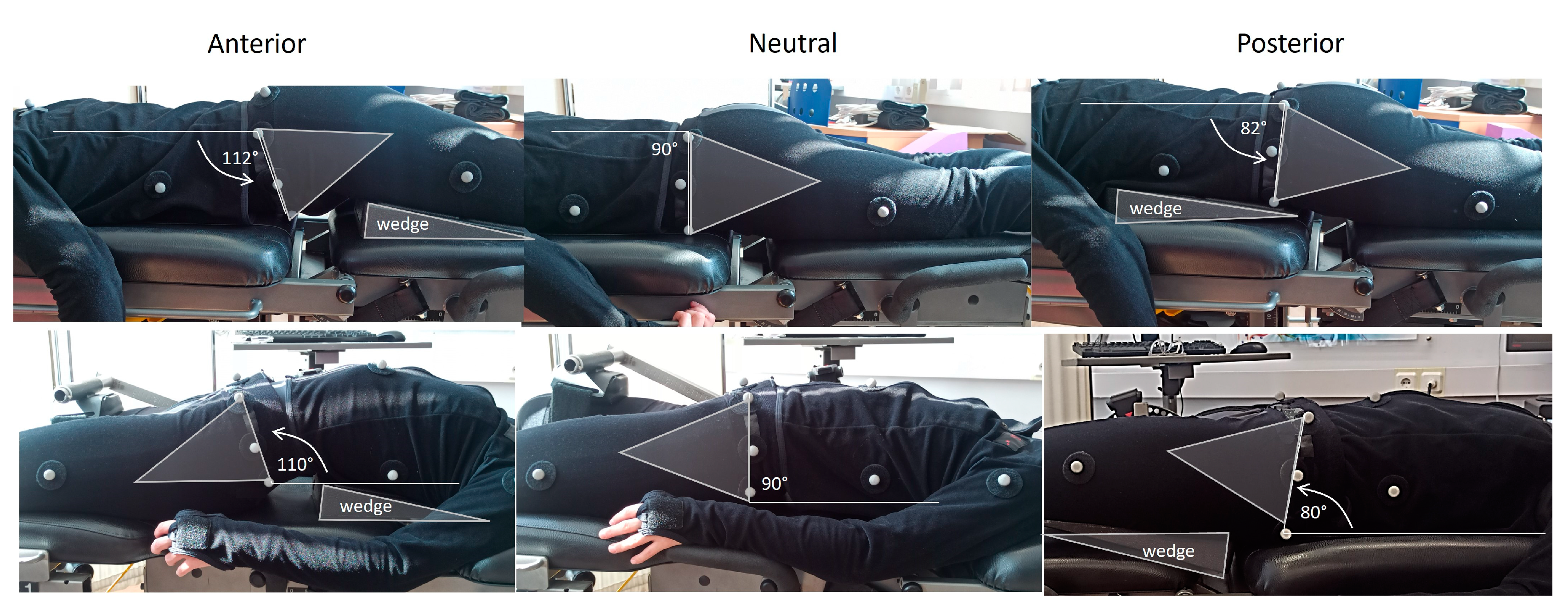
2.3. Procedures
2.4. Data Analysis
2.5. Statistical Analyses
3. Results
3.1. Reliability Measurements
3.2. Maximum Torque Values
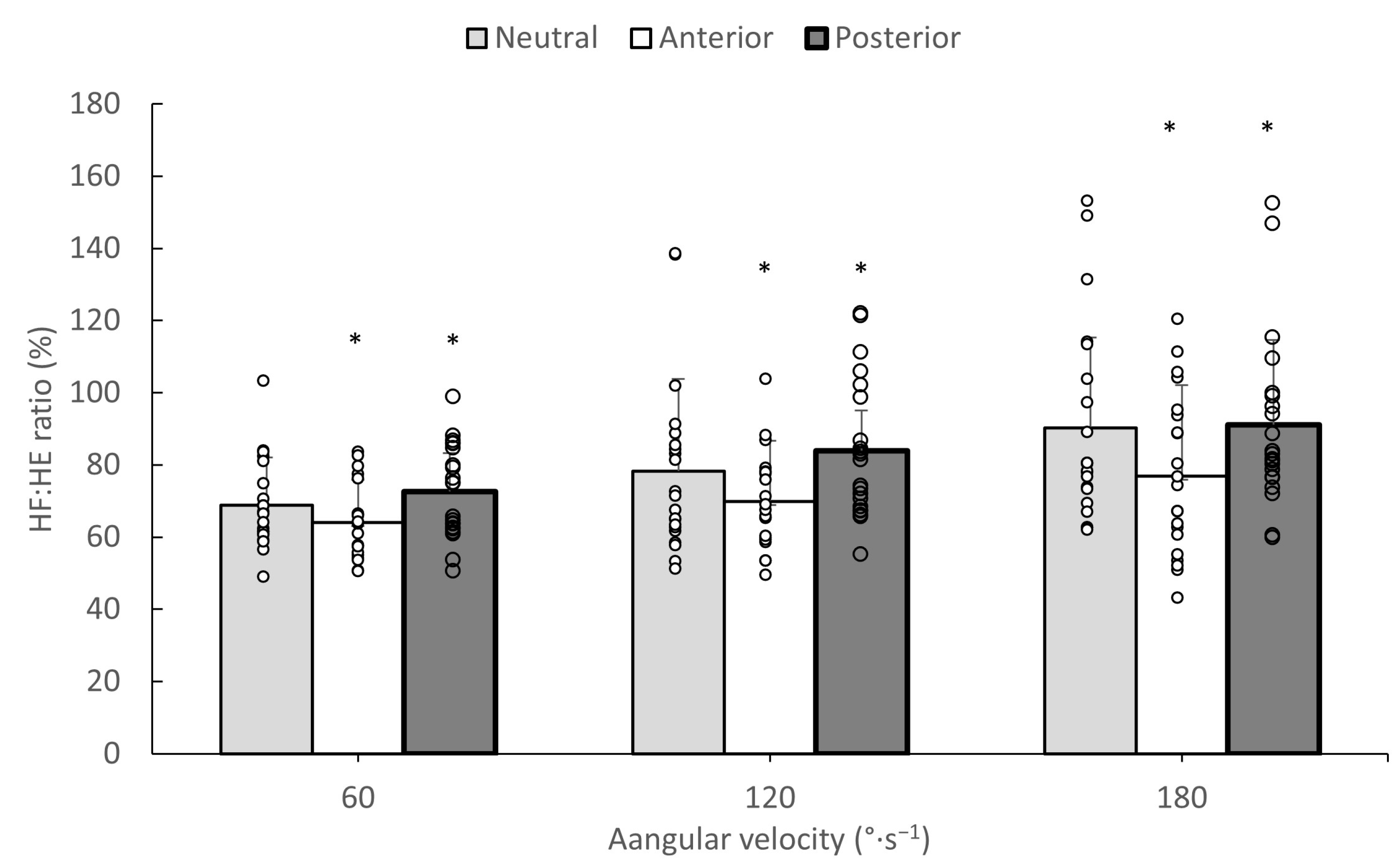
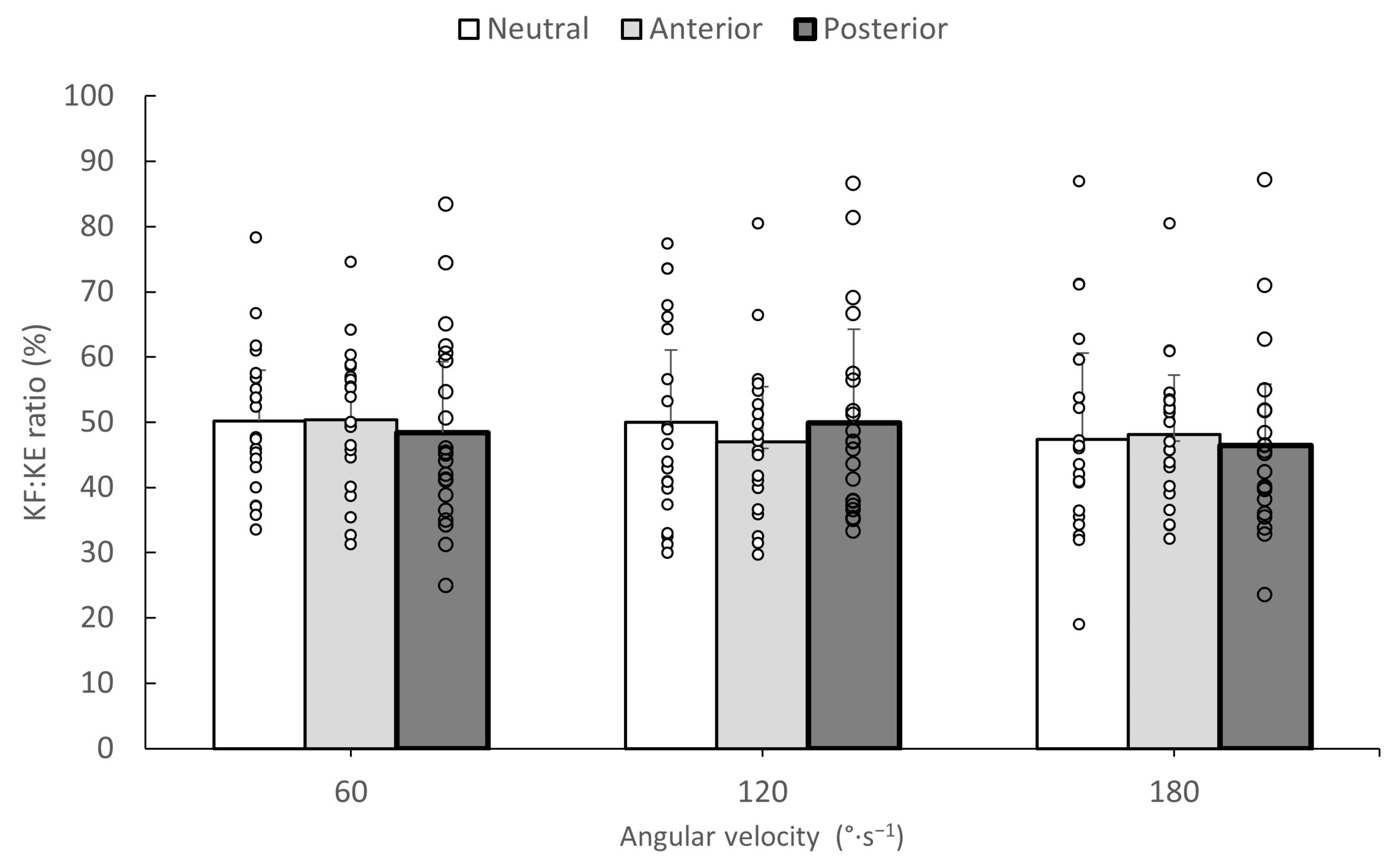
3.3. HF/HE and KF/KE Torque Ratios
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kellis, E.; Blazevich, A.J. Hamstrings Force-Length Relationships and Their Implications for Angle-Specific Joint Torques: A Narrative Review. BMC Sports Sci. Med. Rehabil. 2022, 14, 166. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Rudy, T.W.; Sakane, M.; Kanamori, A.; Ma, C.B.; Woo, S.L.Y. The Importance of Quadriceps and Hamstring Muscle Loading on Knee Kinematics and In-Situ Forces in the ACL. J. Biomech. 1999, 32, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Kekelekis, A.; Manuel Clemente, F.; Kellis, E. Muscle Injury Characteristics and Incidence Rates in Men’s Amateur Soccer: A One Season Prospective Study. Res. Sports Med. 2024, 32, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Opar, D.A.; Timmins, R.G.; Behan, F.P.; Hickey, J.T.; van Dyk, N.; Price, K.; Maniar, N. Is Pre-Season Eccentric Strength Testing During the Nordic Hamstring Exercise Associated with Future Hamstring Strain Injury? A Systematic Review and Meta-Analysis. Sports Med. 2021, 51, 1935–1945. [Google Scholar] [CrossRef]
- Kellis, E.; Sahinis, C.; Baltzopoulos, V. Is Hamstrings-to-Quadriceps Torque Ratio Useful for Predicting Anterior Cruciate Ligament and Hamstring Injuries? A Systematic and Critical Review. J. Sport Health Sci. 2023, 12, 343–358. [Google Scholar] [CrossRef]
- Krantz, M.M.; Åström, M.; Drake, A.M. Strength and Fatigue Measurements of the Hip Flexor and Hip Extensor Muscles: Test-Retest Reliability and Limb Dominance Effect. Int. J. Sports Phys. Ther. 2020, 15, 967–976. [Google Scholar] [CrossRef] [PubMed]
- Kellis, E.; Baltzopoulos, V. Isokinetic Eccentric Exercise. Sports Med. 1995, 19, 202–222. [Google Scholar] [CrossRef]
- van Wingerden, J.P.; Vleeming, A.; Snijders, C.J.; Stoeckart, R. A Functional-Anatomical Approach to the Spine-Pelvis Mechanism: Interaction between the Biceps Femoris Muscle and the Sacrotuberous Ligament. Eur. Spine J. 1993, 2, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Zawadka, M.; Skublewska-Paszkowska, M.; Gawda, P.; Lukasik, E.; Smolka, J.; Jablonski, M. What Factors Can Affect Lumbopelvic Flexion-Extension Motion in the Sagittal Plane?: A Literature Review. Hum. Mov. Sci. 2018, 58, 205–218. [Google Scholar] [CrossRef]
- Schuermans, J.; Van Tiggelen, D.; Witvrouw, E. Prone Hip Extension Muscle Recruitment Is Associated with Hamstring Injury Risk in Amateur Soccer. Int. J. Sports Med. 2017, 38, 696–706. [Google Scholar] [CrossRef][Green Version]
- Kuszewski, M.T.; Gnat, R.; Gogola, A. The Impact of Core Muscles Training on the Range of Anterior Pelvic Tilt in Subjects with Increased Stiffness of the Hamstrings. Hum. Mov. Sci. 2018, 57, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, A.M.W.; McKenzie, C.S.; Pan, X.; Oñate, J.A. Lumbopelvic Control and Days Missed Because of Injury in Professional Baseball Pitchers. Am. J. Sports Med. 2014, 42, 2734–2740. [Google Scholar] [CrossRef] [PubMed]
- Daly, C.; McCarthy Persson, U.; Twycross-Lewis, R.; Woledge, R.C.; Morrissey, D. The Biomechanics of Running in Athletes with Previous Hamstring Injury: A Case-Control Study. Scand. J. Med. Sci. Sports 2016, 26, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Schuermans, J.; Van Tiggelen, D.; Palmans, T.; Danneels, L.; Witvrouw, E. Deviating Running Kinematics and Hamstring Injury Susceptibility in Male Soccer Players: Cause or Consequence? Gait Posture 2017, 57, 270–277. [Google Scholar] [CrossRef] [PubMed]
- da Silva, R.A.; Larivière, C.; Arsenault, A.B.; Nadeau, S.; Plamondon, A. Effect of Pelvic Stabilization and Hip Position on Trunk Extensor Activity during Back Extension Exercises on a Roman Chair. J. Rehabil. Med. 2009, 41, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Hasegawa, S.; Umegaki, H.; Nishishita, S.; Kobayashi, T.; Fujita, K.; Tanaka, H.; Ibuki, S.; Ichihashi, N. The Difference in Passive Tension Applied to the Muscles Composing the Hamstrings—Comparison among Muscles Using Ultrasound Shear Wave Elastography. Man. Ther. 2016, 24, 1–6. [Google Scholar] [CrossRef]
- Deighan, M.A.; Serpell, B.G.; Bitcon, M.J.; De Ste Croix, M. Knee Joint Strength Ratios and Effects of Hip Position in Rugby Players. J. Strength Cond. Res. 2012, 26, 1959–1966. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.; Eng, J.J.; MacIntyre, D.L. Reliability of Surface EMG during Sustained Contractions of the Quadriceps. J. Electromyogr. Kinesiol. 2005, 15, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates, Publishers: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Tateuchi, H.; Taniguchi, M.; Mori, N.; Ichihashi, N. Balance of Hip and Trunk Muscle Activity Is Associated with Increased Anterior Pelvic Tilt during Prone Hip Extension. J. Electromyogr. Kinesiol. 2012, 22, 391–397. [Google Scholar] [CrossRef]
- Neumann, D.A. Kinesiology of the Hip: A Focus on Muscular Actions. J. Orthop. Sports Phys. Ther. 2010, 40, 82–94. [Google Scholar] [CrossRef]
- Mendiguchia, J.; Gonzalez De la Flor, A.; Mendez-Villanueva, A.; Morin, J.-B.; Edouard, P.; Garrues, M.A. Training-Induced Changes in Anterior Pelvic Tilt: Potential Implications for Hamstring Strain Injuries Management. J. Sports Sci. 2021, 39, 760–767. [Google Scholar] [CrossRef] [PubMed]
- Cibulka, M.T.; Rose, S.J.; Delitto, A.; Sinacore, D.R. Hamstring Muscle Strain Treated by Mobilizing the Sacroiliac Joint. Phys. Ther. 1986, 66, 1220–1223. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.-Y.; Lee, M.-R.; An, D.-H. Effect of Initial Position on the Muscle Activity of the Hip Extensors and Amount of Pelvic Tilt during Prone Hip Extension. J. Phys. Ther. Sci. 2015, 27, 1195–1197. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, A.C.L.; Teixeira-Salmela, L.F.; Rodrigues De Paula, F.; Guimarães, C.Q.; Faria, C.D.C.M. Gluteus Maximus and Semitendinosus Activation during Active Prone Hip Extension Exercises. Rev. Bras. Fisioter. 2009, 13, 335–342. [Google Scholar] [CrossRef]
- Preece, S.J.; Tan, Y.F.; Alghamdi, T.D.A.; Arnall, F.A. Comparison of Pelvic Tilt Before and After Hip Flexor Stretching in Healthy Adults. J. Manip. Physiol. Ther. 2021, 44, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Takaki, S.; Kaneoka, K.; Okubo, Y.; Otsuka, S.; Tatsumura, M.; Shiina, I.; Miyakawa, S. Analysis of Muscle Activity during Active Pelvic Tilting in Sagittal Plane. Phys. Ther. Res. 2016, 19, 50–57. [Google Scholar] [CrossRef]
- Small, K.; McNaughton, L.R.; Greig, M.; Lohkamp, M.; Lovell, R. Soccer Fatigue, Sprinting and Hamstring Injury Risk. Int. J. Sports Med. 2009, 30, 573–578. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pelvic Tilt | |||
|---|---|---|---|
| Neutral | Anterior | Posterior | |
| Hip extension | |||
| 60°·s−1 | 0.87 (0.63–0.96) | 0.88 (0.67–0.96) | 0.91 (0.75–0.97) |
| 120°·s−1 | 0.93 (0.78–0.98) | 0.88 (0.65–0.96) | 0.94 (0.84–0.98) |
| 180°·s−1 | 0.88 (0.66–0.96) | 0.77 (0.13–0.71) | 0.95 (0.86–0.98) |
| Hip flexion | |||
| 60°·s−1 | 0.89 (0.68–0.97) | 0.88 (0.66–0.96) | 0.87 (0.63–0.95) |
| 120°·s−1 | 0.88 (0.66–0.96) | 0.94 (0.81–0.97) | 0.95 (0.85–0.98) |
| 180°·s−1 | 0.93 (0.79–0.97) | 0.94 (0.83–0.98) | 0.89 (0.70–0.97) |
| HF/HE ratio | |||
| 60°·s−1 | 0.84 (0.54–0.95) | 0.87 (0.64–0.96) | 0.65 (0.19–0.87) |
| 120°·s−1 | 0.91 (0.75–0.97) | 0.93 (0.80–0.98) | 0.94 (0.82–0.98) |
| 180°·s−1 | 0.92 (0.77–0.97) | 0.85 (0.59–0.95) | 0.92 (0.77–0.97) |
| Pelvic Tilt | |||
|---|---|---|---|
| Neutral | Anterior | Posterior | |
| Knee extension | |||
| 60°·s−1 | 0.92 (0.76–0.97) | 0.96 (0.89–0.99) | 0.95 (0.86–0.98) |
| 120°·s−1 | 0.95 (0.84–0.98) | 0.98 (0.96–0.99) | 0.94 (0.83–0.98) |
| 180°·s−1 | 0.96 (0.88–0.98) | 0.95 (0.85–0.98) | 0.69 (0.24–0.89) |
| Knee flexion | |||
| 60°·s−1 | 0.91 (0.61–0.97) | 0.94 (0.81–0.98) | 0.82 (0.52–0.94) |
| 120°·s−1 | 0.86 (0.40–0.96) | 0.94 (0.71–0.98) | 0.84 (0.57–0.94) |
| 180°·s−1 | 0.88 (0.65–0.96) | 0.87 (0.55–0.96) | 0.69 (0.24–0.89) |
| KF/KE ratio | |||
| 60°·s−1 | 0.73 (0.35–0.91) | 0.95 (0.83–0.98) | 0.81 (0.51–0.94) |
| 120°·s−1 | 0.75 (0.29–0.92) | 0.91 (0.28–0.98) | 0.92 (0.76–0.97) |
| 180°·s−1 | 0.84 (0.47–0.95) | 0.87 (0.48–0.97) | 0.69 (0.25–0.99) |
| Pelvic Tilt | |||
|---|---|---|---|
| Anterior | Neutral | Posterior | |
| Hip extension | |||
| 60°·s−1 | 249.00 ± 72.07 *^# | 231.90 ± 68.24 ^# | 226.44 ± 78.24 *^# |
| 120°·s−1 | 191.85 ± 59.35 *^# | 178.66 ± 65.89 ^# | 160.41 ± 64.44 *^# |
| 180°·s−1 | 144.66 ± 61.38 *^# | 131.09 ± 40.28 ^# | 130.93 ± 56.96 *^# |
| Hip flexion | |||
| 60°·s−1 | 159.14 ± 53.01 ^ | 157.95 ± 50.52 ^ | 160.33 ± 54.44 ^ |
| 120°·s−1 | 131.42 ± 41.82 ^ | 131.04 ± 40.05 ^ | 133.12 ± 48.11 ^ |
| 180°·s−1 | 105.66 ± 40.77 ^ | 113.00 ± 39.28 ^ | 111.69 ± 46.72 ^ |
| Pelvic Tilt | |||
|---|---|---|---|
| Anterior | Neutral | Posterior | |
| Knee extension | |||
| 60°·s−1 | 156.85 ± 35.77 ^# | 151.57 ± 48.92 ^# | 159.53 ± 38.25 ^# |
| 120°·s−1 | 130.95 ± 50.24 ^# | 129.85 ± 51.43 ^# | 125.00 ± 42.15 ^# |
| 180°·s−1 | 109.49 ± 45.83 ^# | 105.61 ± 44.84 ^# | 110.19 ± 52.35 ^# |
| Knee flexion | |||
| 60°·s−1 | 78.44 ± 26.56 ^ | 74.61 ± 26.37 ^ | 71.38 ± 25.82 ^ |
| 120°·s−1 | 60.19 ± 22.48 ^ | 57.90 ± 20.13 ^ | 59.00 ± 18.76 ^ |
| 180°·s−1 | 50.00 ± 19.87 ^ | 47.38 ± 20.53 ^ | 47.00 ± 19.85 ^ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kellis, E.; Konstantopoulos, A.; Salonikios, G.; Ellinoudis, A. Does Pelvic Tilt Angle Influence the Isokinetic Strength of the Hip and Knee Flexors and Extensors? J. Funct. Morphol. Kinesiol. 2024, 9, 73. https://doi.org/10.3390/jfmk9020073
Kellis E, Konstantopoulos A, Salonikios G, Ellinoudis A. Does Pelvic Tilt Angle Influence the Isokinetic Strength of the Hip and Knee Flexors and Extensors? Journal of Functional Morphology and Kinesiology. 2024; 9(2):73. https://doi.org/10.3390/jfmk9020073
Chicago/Turabian StyleKellis, Eleftherios, Athanasios Konstantopoulos, Georgios Salonikios, and Athanasios Ellinoudis. 2024. "Does Pelvic Tilt Angle Influence the Isokinetic Strength of the Hip and Knee Flexors and Extensors?" Journal of Functional Morphology and Kinesiology 9, no. 2: 73. https://doi.org/10.3390/jfmk9020073
APA StyleKellis, E., Konstantopoulos, A., Salonikios, G., & Ellinoudis, A. (2024). Does Pelvic Tilt Angle Influence the Isokinetic Strength of the Hip and Knee Flexors and Extensors? Journal of Functional Morphology and Kinesiology, 9(2), 73. https://doi.org/10.3390/jfmk9020073