
Assessing the Effects and Challenges of Total Hip Arthroplasty before Pregnancy and Childbirth: A Systematic Review


 ,
,  , , , , ,
, , , , ,
Abstract
1. Introduction
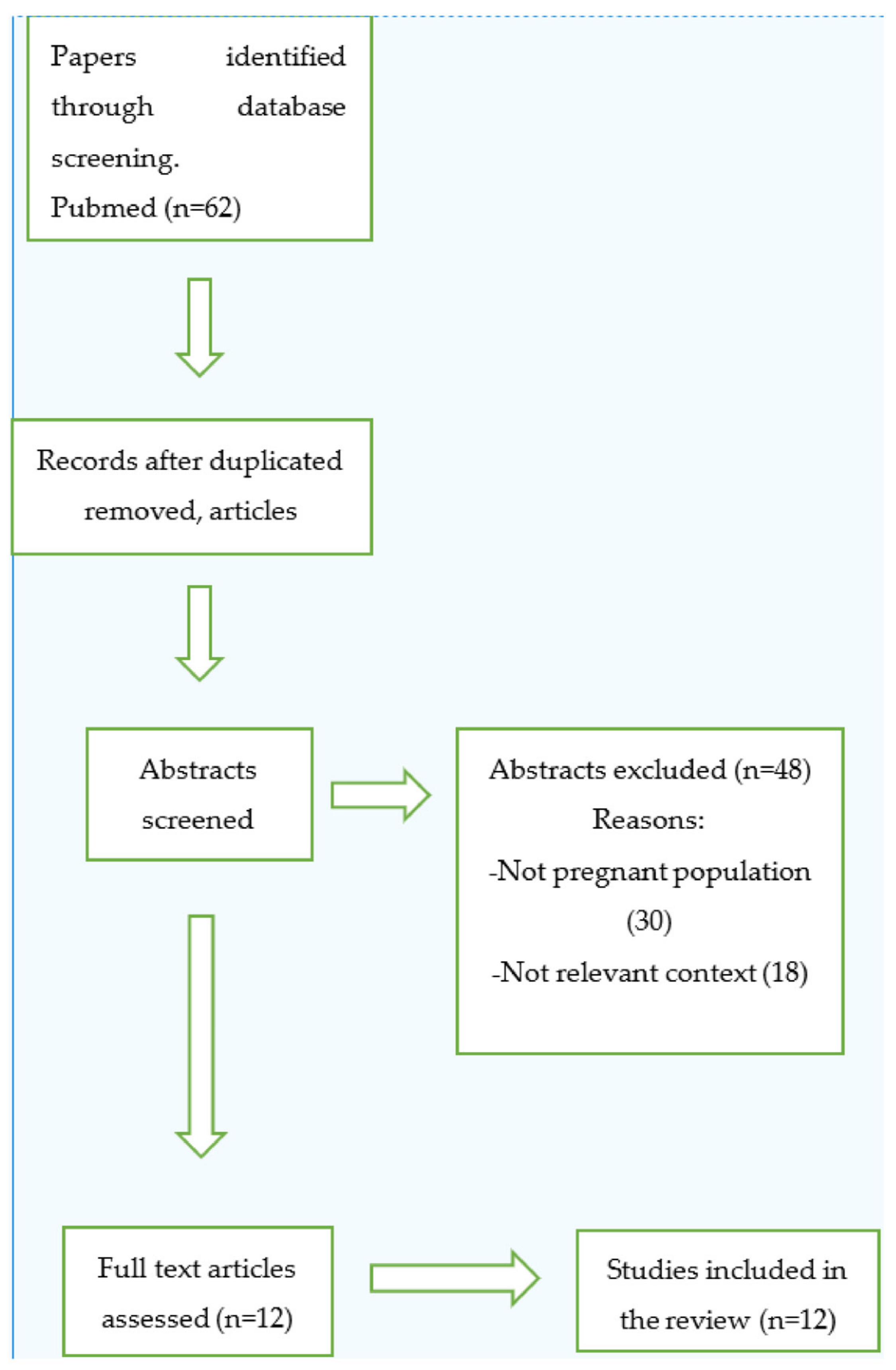
2. Materials and Methods
3. Results
3.1. Early Case Reports
3.2. First Research Examining THA Impact and Later Larger Scale Studies
3.3. Studies from Finland
3.4. Studies concerning Metal-on-Metal Hip Implants and Potential Effects on Newborns
4. Discussion
4.1. Previous Total Hip Arthroplasty or Not Having any THA and Pregnancy Rates
4.2. Hip Pain Levels of Women with THA History during Gestation
4.3. Hip Implants and Mode of Delivery
4.4. Revision Rates in Women with Previous Hip Arthroplasty and Subsequent Pregnancy
4.5. Newborns of Women with Previous Total Hip Arthroplasty and Potential Congenital Defects and Complications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DDH | dysplasia of the hip |
| FAI | femoro-acetabular impingement |
| AVN | avascular necrosis |
| RA | rheumatoid arthritis |
| THA | total hip arthroplasty |
| HRA | hip resurfacing arthroplasty |
| MMHRA | metal-on-metal hip resurfacing arthroplasty |
| MoM-THA | metal-on-metal total hip arthroplasty |
| WOMAC | Western Ontario and McMaster Universities Arthritis Index |
| IAs | induced abortions |
| SGA | small-for-gestational-age |
References
- Smith, S.E.; Estok, D.M.; Harris, W.H. 20-yr experience with cemented primary and conversion total hip arthroplasty using so-called second-generation cementing techniques in patients aged 50 years or younger. J. Arthroplast. 2000, 15, 263–273. [Google Scholar] [CrossRef]
- Duffy, G.P.; Berry, D.J.; Rowland, C.; Cabanela, M.E. Primary uncemented total hip arthroplasty in patients 40 years old: 10- to 14-year results using first-generation proximally porous-coated implants. J. Arthroplast. 2001, 16 (Suppl. S1), 140–144. [Google Scholar] [CrossRef]
- Malchau, H.; Herberts, P.; Eisler, T.; Garellick, G.; Söderman, P. The Swedish Total Hip Replacement Register. J. Bone Jt. Surg. Am. 2002, 84 (Suppl. S2), 2–20. [Google Scholar] [CrossRef] [PubMed]
- Gross, T.P. Is female gender an absolute or relative contraindication? Ann. Joint 2021, 6, 23. [Google Scholar] [CrossRef]
- Samuel, L.T.; Rabin, J.M.; Arnold, N.R.; Munim, M.; Brooks, P.J.; Mont, M.A. Metal-on-metal (MoM) hip implants and pregnancy: Are MoM implants good for mom?-a systematic review. Ann. Transl. Med. 2023, 11, 363. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, R.L.; Areia, A.L.; Mota Pinto, A.; Donato, H. Advanced Maternal Age: Adverse Outcomes of Pregnancy, A Meta-Analysis. Acta Med. Port. 2019, 32, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Oliviero, A.; Aicale, R.; Maffulli, N. Pregnancy and parturition after hip arthroplasty. Surgeon 2022, 20, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Acar, B.S.; Mihcin, S. Vehicle internal design improvement guidelines by using the computational pregnant occupant model ‘Expecting’. Int. J. Hum. Factors Model. Simul. 2010, 1, 380–389. [Google Scholar] [CrossRef]
- Wittich, A.C. Successful pregnancy and delivery following bilateral total hip replacement: Report of case. J. Am. Osteopath. Assoc. 1982, 81, 773–775. [Google Scholar] [CrossRef]
- Monaghan, J.; Lenehan, P.; Stronge, J.; Gallagher, J. Pregnancy and vaginal delivery following bilateral total hip replacement. Eur. J. Obstet. Gynecol. Reprod. Biol. 1987, 26, 261–264. [Google Scholar] [CrossRef]
- McDowell, C.M.; Lachiewicz, P.F. Pregnancy after total hip arthroplasty. J. Bone Jt. Surg. Am. 2001, 83, 1490–1494. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, R.; Feinberg, J.R.; Capello, W.N.; Detterline, A.J. Clinical outcome and incidence of pregnancy after bipolar and total hip arthroplasty in young women. J. Arthroplast. 2003, 18, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Lally, L.; Mandl, L.A.; Huang, W.T.; Goodman, S.M. Pregnancy Does Not Adversely Affect Postoperative Pain and Function in Women with Total Hip Arthroplasty. J. Clin. Rheumatol. 2015, 21, 323–325. [Google Scholar] [CrossRef] [PubMed]
- Yazici, Y.; Erkan, D.; Zuniga, R.; Bateman, H.; Salvati, E.A.; Magid, S.K. Pregnancy outcomes following total hip arthroplasty: A preliminary study and review of the literature. Orthopedics 2003, 26, 75–76. [Google Scholar] [CrossRef]
- Sierra, R.J.; Trousdale, R.T.; Cabanela, M.E. Pregnancy and childbirth after total hip arthroplasty. J. Bone Jt. Surg. Br. 2005, 87, 21–24. [Google Scholar] [CrossRef]
- Stea, S.; Bordini, B.; De Clerico, M.; Traina, F.; Toni, A. Safety of pregnancy and delivery after total hip arthroplasty. J. Women’s Health 2007, 16, 1300–1304. [Google Scholar] [CrossRef]
- Kuitunen, I.; Artama, M.; Eskelinen, A.; Skyttä, E.T.; Huhtala, H.; Uotila, J. Pregnancy outcome in women after total hip replacement: A population-based study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 238, 143–147. [Google Scholar] [CrossRef]
- Kuitunen, I.; Skyttä, E.T.; Artama, M.; Huhtala, H.; Eskelinen, A. No effect of delivery on total hip replacement survival: A nationwide register study in Finland. Acta Orthop. 2019, 90, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Artama, M.; Skyttä, E.T.; Huhtala, H.; Leino, M.; Kuitunen, I.; Eskelinen, A. Lower birth rate in patients with total hip replacement. Acta Orthop. 2016, 87, 492–496. [Google Scholar] [CrossRef]
- Kuitunen, I.; Skyttä, E.T.; Eskelinen, A.; Huhtala, H.; Artama, M. Induced Abortions Among Women Having Undergone Total Hip Replacement: A Nationwide Register Study in Finland. Scand. J. Surg. 2019, 108, 258–264. [Google Scholar] [CrossRef]
- Ziaee, H.; Daniel, J.; Datta, A.K.; Blunt, S.; McMinn, D.J. Transplacental transfer of cobalt and chromium in patients with metal-on-metal hip arthroplasty: A controlled study. J. Bone Jt. Surg. Br. 2007, 89, 301–305. [Google Scholar] [CrossRef]
- DeSouza, R.M.; Wallace, D.; Costa, M.L.; Krikler, S.J. Transplacental passage of metal ions in women with hip resurfacing: No teratogenic effects observed. Hip Int. 2012, 22, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Kuitunen, I.; Eskelinen, A.; Skyttä, E.T.; Huhtala, H.; Artama, M. Congenital anomalies in the offspring of women with total hip replacement: A nationwide register study in Finland. Hip Int. 2021, 31, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.J.; Yoo, J.J.; Yoon, K.S.; Koo, K.H.; Kim, H.J. Alumina-on-alumina THA performed in patients younger than 30 years: A 10-year minimum followup study. Clin. Orthop. Relat. Res. 2012, 470, 3530–3536. [Google Scholar] [CrossRef]
- Smith, M.W.; Marcus, P.S.; Wurtz, L.D. Orthopedic issues in pregnancy. Obstet. Gynecol. Surv. 2008, 63, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.Q.; Woolson, S.T. Referral patterns of hip pain in patients undergoing total hip replacement. Orthopedics 1998, 21, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Crowther, J.D.; Lachiewicz, P.F. Survival and polyethylene wear of porous-coated acetabular components in patients less than fifty years old: Results at nine to fourteen years. J. Bone Jt. Surg. Am. 2002, 84, 729–735. [Google Scholar] [CrossRef]
- Mohaddes, M.; NaucléR, E.; Kärrholm, J.; Malchau, H.; Odin, D.; Rolfson, O. Implant survival and patient-reported outcome following total hip arthroplasty in patients 30 years or younger: A matched cohort study of 1008 patients in the Swedish Hip Arthroplasty Register. Acta Orthop. 2019, 90, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Tsukanaka, M.; Halvorsen, V.; Nordsletten, L.; EngesæTer, I.Ø.; EngesæTer, L.B.; Fenstad, A.M.; Röhrl, S.M. Implant survival and radiographic outcome of total hip replacement in patients less than 20 years old. Acta Orthop. 2016, 87, 479–484. [Google Scholar] [CrossRef]
- Nam, D.; Nunley, R.M.; Berend, M.E.; Berend, K.R.; Lombardi, A.V.; Barrack, R.L. Residual Symptoms and Function in Young, Active Hip Arthroplasty Patients: Comparable to Normative Controls? J. Arthroplast. 2016, 31, 1492–1497. [Google Scholar] [CrossRef]
- Mihcin, S.; Sahin, A.M.; Yilmaz, M.; Alpkaya, A.T.; Tuna, M.; Akdeniz, S.; Korkmaz, N.C.; Tosun, A.; Sahin, S. Database covering the prayer movements which were not available previously. Sci. Data 2023, 10, 276. [Google Scholar] [CrossRef] [PubMed]
- Ladon, D.; Doherty, A.; Newson, R.; Turner, J.; Bhamra, M.; Case, C.P. Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J. Arthroplast. 2004, 19 (Suppl. S3), 78–83. [Google Scholar] [CrossRef] [PubMed]
- Daniel, J.; Ziaee, H.; Pradhan, C.; Pynsent, P.B.; McMinn, D.J. Blood and urine metal ion levels in young and active patients after Birmingham hip resurfacing arthroplasty: Four-year results of a prospective longitudinal study. J. Bone Jt. Surg. Br. 2007, 89, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Aljary, H.; Czuzoj-Shulman, N.; Spence, A.R.; Abenhaim, H.A. Pregnancy outcomes in women with rheumatoid arthritis: A retrospective population-based cohort study. J. Matern. Fetal Neonatal Med. 2020, 33, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Wallenius, M.; Salvesen, K.Å.; Daltveit, A.K.; Skomsvoll, J.F. Rheumatoid arthritis and outcomes in first and subsequent births based on data from a national birth registry. Acta Obstet. Gynecol. Scand. 2014, 93, 302–307. [Google Scholar] [CrossRef]
- Alpkaya, A.T.; Mihcin, S. Dynamic computational wear model of PEEK-on-XLPE bearing couple in total hip replacements. Med. Eng. Phys. 2023, 117, 104006. [Google Scholar] [CrossRef]

{kind=link}
| Reference | Title | Study Design | Results |
|---|---|---|---|
| Meldrum R et al. [12] | Clinical outcome and incidence of pregnancy after bipolar and total hip arthroplasty in young women | Retrospective study | 1. Not enhanced pregnancy-associated complications and hip-related conditions. 2. Hip arthroplasty was regarded as indication for c-section. 3. Younger women with higher functional results were more likely to get pregnant. |
| Yazici Y et al. [14] | Pregnancy outcomes following total hip arthroplasty: a preliminary study and review of the literature | Retrospective study | 1. Hip arthroplasty poses no unfavorable perils on gestation. 2. No prothesis-associated complications were detected. |
| McDowell CM et al. [11] | Pregnancy after total hip arthroplasty | Retrospective study | 1. Felicitous gestations can transpire after THA. 2. Hip implants are not adversely impacted from pregnancy. |
| Sierra R J et al. [15] | Pregnancy and childbirth after total hip arthroplasty | Prospective study | 1. Childbirth is not influenced by the existence of THA. 2. Gestation post THA is not correlated with a reduced survival of the implants. 3. Hip pain is ordinary during gestation in these patients. 4. Persistent groin pain after delivery customarily leads to THA revision. |
| Stea S et al. [16] | Safety of pregnancy and delivery after total hip arthroplasty | Retrospective study | Gestation and childbirth do not represent risk factors concerning THA survival. |
| Ziaee H et al. [21] | Transplacental transfer of cobalt and chromium in patients with metal-on-metal hip arthroplasty: a controlled study | Controlled study | 1. Both cobalt and chromium do cross the placenta. 2. The placenta exerts a regulative impact on the extent of metal transfer. |
| Hyeong Jo Yoon et al. [24] | Alumina-on-alumina THA Performed in Patients Younger Than 30 Years: A 10-year Minimum Follow up Study | Prospective study | Augmented 10-year survival rate of cementless alumina-on-alumina THA in young subjects. |
| Lally L et al. [13] | Pregnancy Does Not Adversely Affect Postoperative Pain and Function in Women with Total Hip Arthroplasty | Cohort study | 1. Gestation post THA was not related to worse postoperative pain or functional capacity. 2. No discrepancies in pregnancy outcomes or complications among women with post-THA gestation and those with pregnancy pre-THA. |
| Miia Artama et al. [19] | Lower birth rate in patients with total hip replacement | Cohort study | THA could induce lower birth rates in both men and women. |
| Ilari Kuitunen et al. [17] | Pregnancy outcome in women after total hip replacement: A population-based study | Cohort study | 1. Neonates born after maternal THA feature an increased peril of preterm birth, stillbirth, small size for gestational age and low birthweight. 2. Trial of labor is more likely to result in emergency cesarean section. |
| Ilari Kuitunen et al. [18] | No effect of delivery on total hip replacement survival: a nationwide register study in Finland | Cohort study | Delivery does not appear to abate THA implant-survival rates. |
| Ilari Kuitunen et al. [23] | Congenital anomalies in the offspring of women with total hip replacement: a nationwide register study in Finland | Cohort study | THA does not seem to affect the risk of major congenital anomalies or gestations ending owing to suspected fetal abnormalities. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galanis, A.; Dimopoulou, S.; Karampinas, P.; Vasiliadis, E.; Kaspiris, A.; Sakellariou, E.; Vlachos, C.; Vavourakis, M.; Papagrigorakis, E.; Marougklianis, V.; et al. Assessing the Effects and Challenges of Total Hip Arthroplasty before Pregnancy and Childbirth: A Systematic Review. J. Funct. Morphol. Kinesiol. 2024, 9, 63. https://doi.org/10.3390/jfmk9020063
Galanis A, Dimopoulou S, Karampinas P, Vasiliadis E, Kaspiris A, Sakellariou E, Vlachos C, Vavourakis M, Papagrigorakis E, Marougklianis V, et al. Assessing the Effects and Challenges of Total Hip Arthroplasty before Pregnancy and Childbirth: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2024; 9(2):63. https://doi.org/10.3390/jfmk9020063
Chicago/Turabian StyleGalanis, Athanasios, Stefania Dimopoulou, Panagiotis Karampinas, Elias Vasiliadis, Angelos Kaspiris, Evangelos Sakellariou, Christos Vlachos, Michail Vavourakis, Eftychios Papagrigorakis, Vasileios Marougklianis, and et al. 2024. "Assessing the Effects and Challenges of Total Hip Arthroplasty before Pregnancy and Childbirth: A Systematic Review" Journal of Functional Morphology and Kinesiology 9, no. 2: 63. https://doi.org/10.3390/jfmk9020063
APA StyleGalanis, A., Dimopoulou, S., Karampinas, P., Vasiliadis, E., Kaspiris, A., Sakellariou, E., Vlachos, C., Vavourakis, M., Papagrigorakis, E., Marougklianis, V., Tsalimas, G., Zachariou, D., Patilas, C., Varsamos, I., Kolovos, I., & Vlamis, J. (2024). Assessing the Effects and Challenges of Total Hip Arthroplasty before Pregnancy and Childbirth: A Systematic Review. Journal of Functional Morphology and Kinesiology, 9(2), 63. https://doi.org/10.3390/jfmk9020063