
Clinical Effects of L-Carnitine Supplementation on Physical Performance in Healthy Subjects, the Key to Success in Rehabilitation: A Systematic Review and Meta-Analysis from the Rehabilitation Point of View





Abstract
1. Introduction
2. Methods
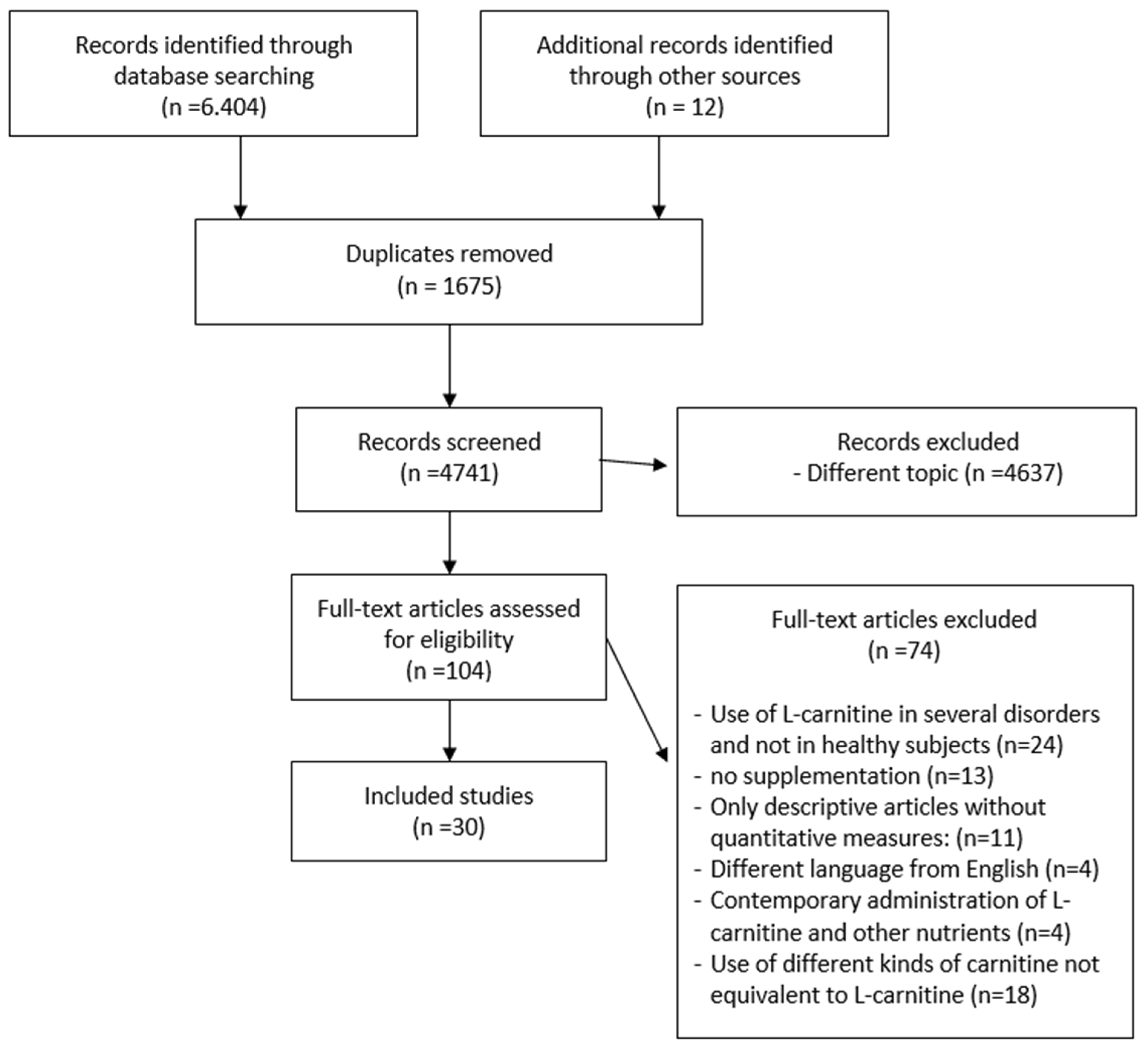
2.1. Search Strategy
2.2. Study Selection
2.3. Data Collection Process, Data Extraction and Outcomes
2.4. Risk of Bias
2.5. Quality of Outcomes
2.6. Meta-Analysis Calculations
3. Results
3.1. Variations of Experimental Conditions across the Studies
3.2. Participants, Interventions and Comparators
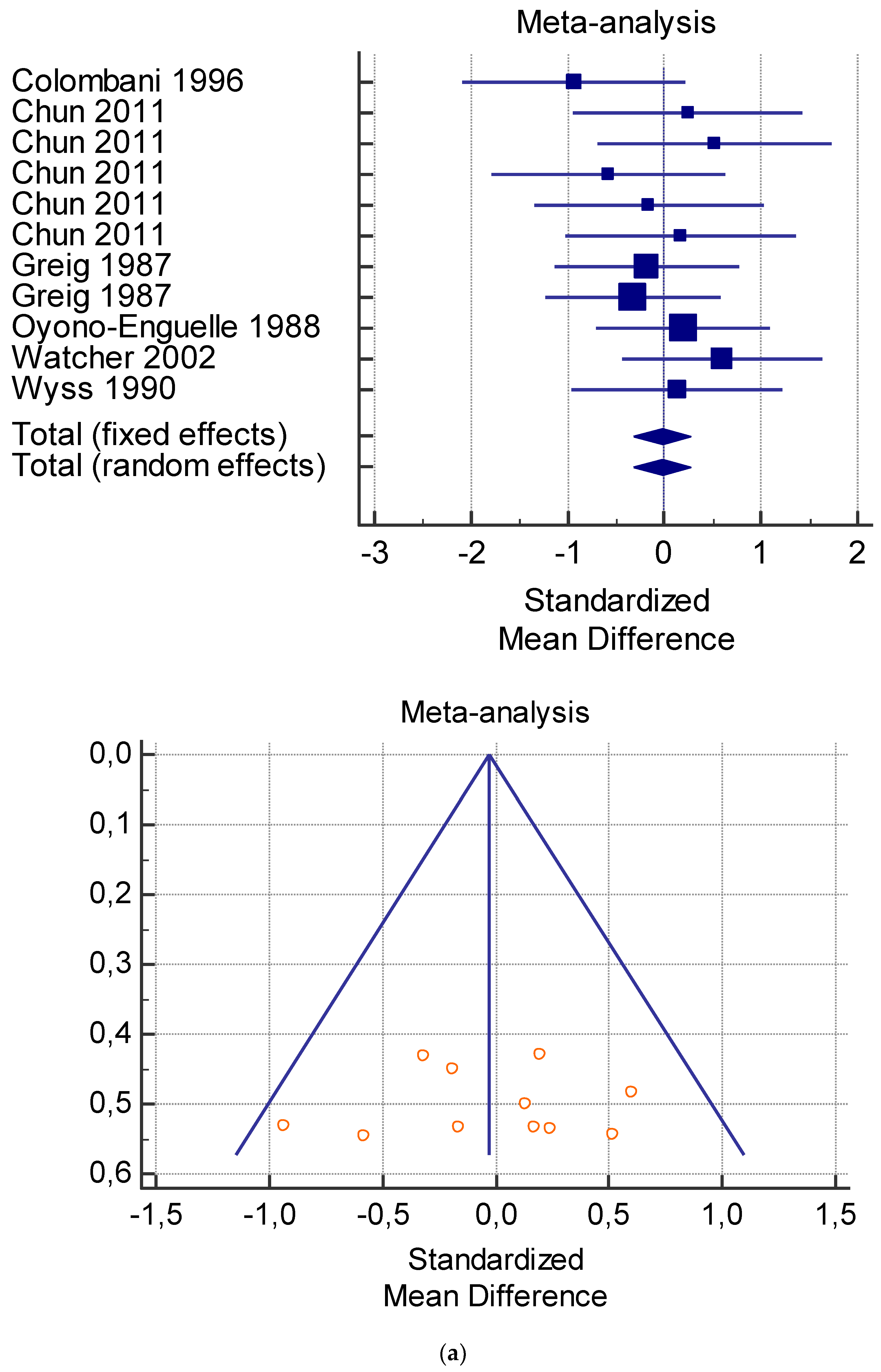
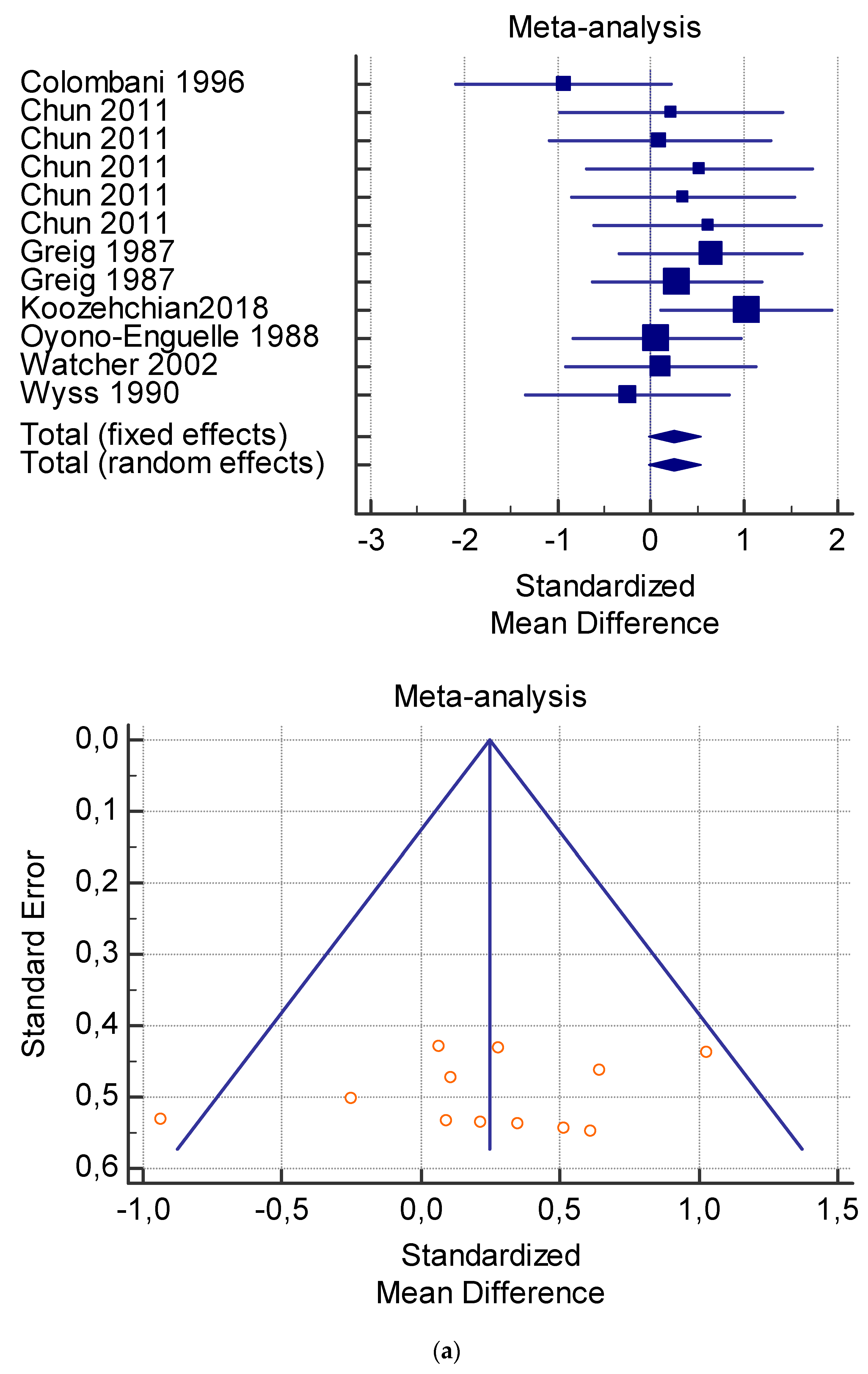
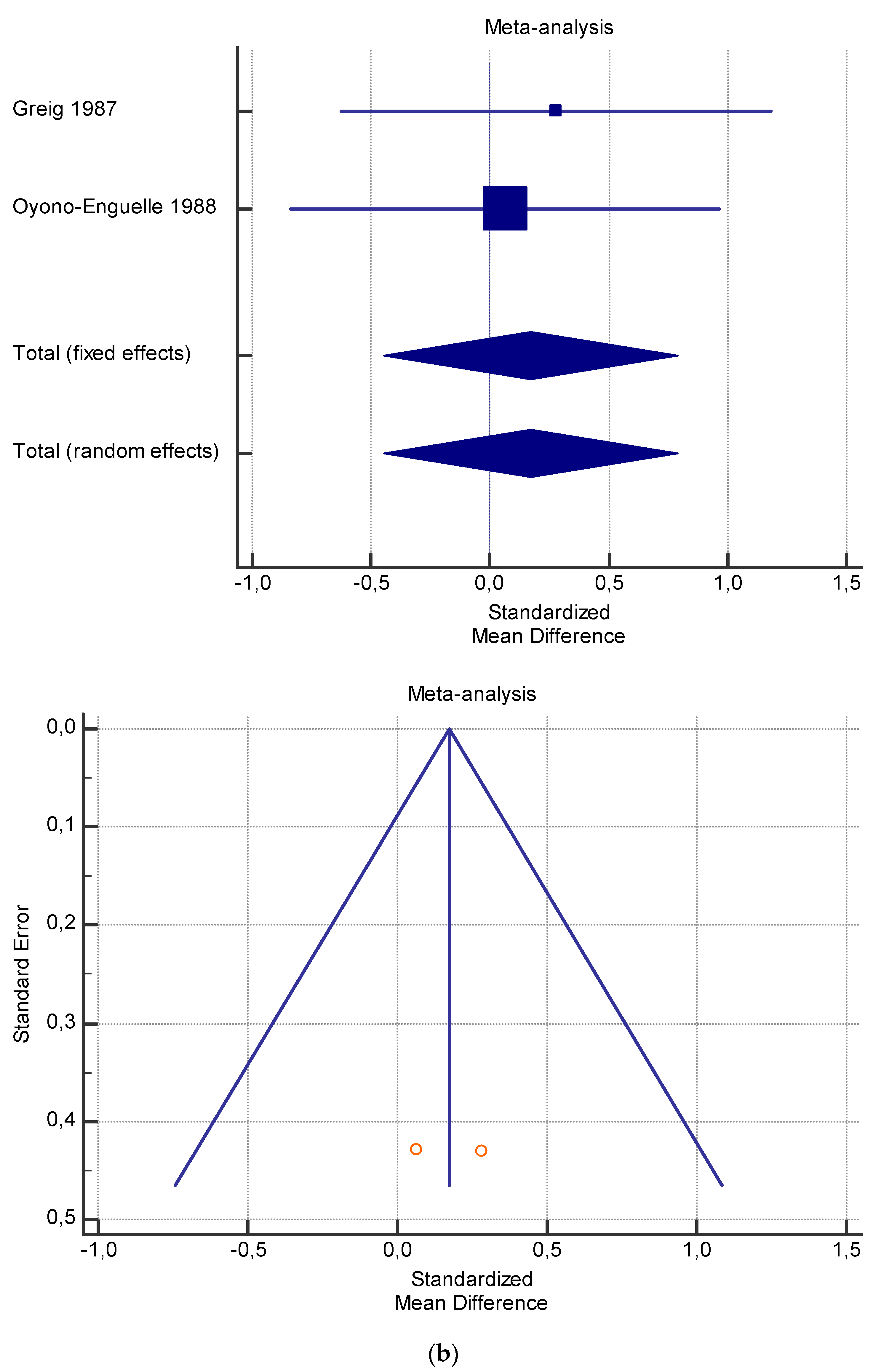
3.3. Meta-Analysis Results
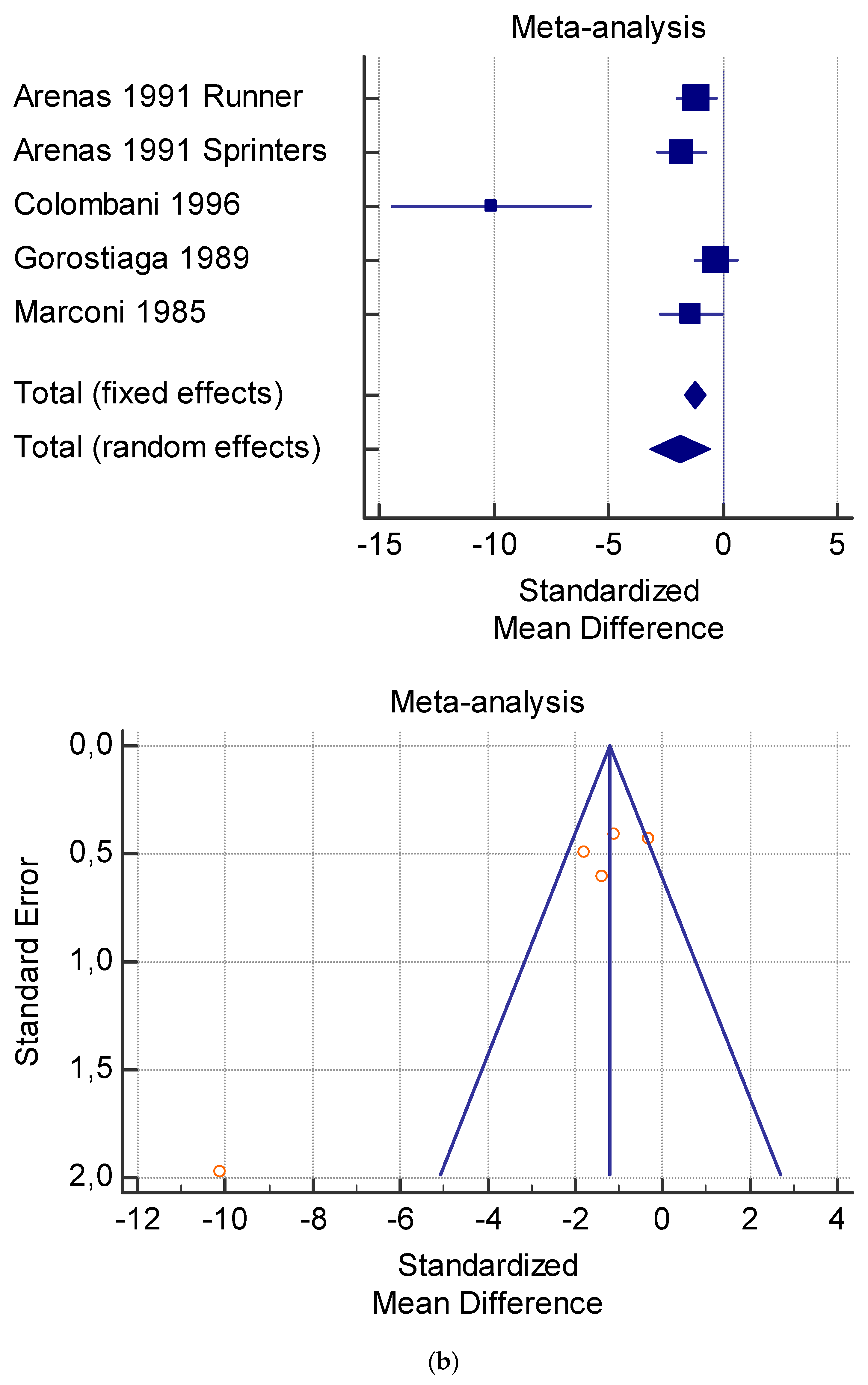
3.4. Heterogeneity and Publication Bias
3.5. Comparing Studies
3.6. Posology and Timeframe
4. Discussion
4.1. Implication in Sports and Rehabilitation
4.2. Ineffective Use of L-Carnitine
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chun, Y.; Lee, K.; Kang, S.; Lee, N.; Kim, J. Influence of L-Carnitine intake for maximal exercise performance and fatigue recovery exercise athletes: Based on elite soccer plaers. Phys. Act. Nutr. 2011, 6, 28–34. [Google Scholar] [CrossRef]
- Cruciani, R.A.; Zhang, J.J.; Manola, J.; Cella, D.; Ansari, B.; Fisch, M.J. L-Carnitine Supplementation for the Management of Fatigue in Patients with Cancer: An Eastern Cooperative Oncology Group Phase III, Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Oncol. 2012, 30, 3864–3869. [Google Scholar] [CrossRef]
- De Simone, C.; Tzantzoglou, S.; Famularo, G.; Moretti, S.; Paoletti, F.; Vullo, V.; Delia, S. High dose L-carnitine improves immunologic and metabolic parameters in AIDS patients. Immunopharmacol. Immunotoxicol. 1993, 15, 1–12. [Google Scholar] [CrossRef]
- Siami, G.; Clinton, M.E.; Mrak, R.; Griffis, J.; Stone, W. Evaluation of the Effect of Intravenous L-Carnitine Therapy on Function, Structure and Fatty Acid Metabolism of Skeletal Muscle in Patients Receiving Chronic Hemodialysis. Nephron 1991, 57, 306–313. [Google Scholar] [CrossRef]
- Silvério, R.; Laviano, A.; Fanelli, F.R.; Seelaender, M. L-carnitine and cancer cachexia: Clinical and experimental aspects. J. Cachex-Sarcopenia Muscle 2011, 2, 37–44. [Google Scholar] [CrossRef]
- Vecchio, M.; Malaguarnera, G.; Giordano, M.; Malaguarnera, M.; Li Volti, G.; Galvano, F.; Drago, F.; Basile, F.; Malaguarnera, M. A Musician’s Dystonia. Lancet 2012, 379, 2116. [Google Scholar] [CrossRef]
- Malaguarnera, M.; Cammalleri, L.; Gargante, M.P.; Vacante, M.; Colonna, V.; Motta, M. L-Carnitine treatment reduces severity of physical and mental fatigue and increases cognitive functions in centenarians: A randomized and controlled clinical trial. Am. J. Clin. Nutr. 2007, 86, 1738–1744. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Volek, J.S.; Spiering, B.A.; Vingren, J.L. L-Carnitine Supplementation: A New Paradigm for its Role in Exercise. Mon. Für Chem. /Chem. Mon. 2005, 136, 1383–1390. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, 7647. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in EpidemiologyA Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Collaboration: Oxford, UK, 2008. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y. GRADE guidelines: 4. Rating the quality of evidence—Study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence—Publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE guidelines: 8. Rating the quality of evidence—indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Br. Med. J. 2011, 343, 889–893. [Google Scholar] [CrossRef]
- Brass, E.P.; Hoppel, C.L.; Hiatt, W.R. Effect of intravenous L-carnitine on carnitine homeostasis and fuel metabolism during exercise in humans. Clin. Pharmacol. Ther. 1994, 55, 681–692. [Google Scholar] [CrossRef]
- Colombani, P.; Wenk, C.; Kunz, I.; Krähenbühl, S.; Kuhnt, M.; Arnold, M.; Frey-Rindova, P.; Frey, W.; Langhans, W. Effects of L-carnitine supplementation on physical performance and energy metabolism of endurance-trained athletes: A double-blind crossover field study. Eur. J. Appl. Physiol. Occup. Physiol. 1996, 73, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Marconi, C.; Sassi, G.; Carpinelli, A.; Cerretelli, P. Effects of L-carnitine loading on the aerobic and anaerobic performance of endurance athletes. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 131–135. [Google Scholar] [CrossRef]
- Greig, C.; Finch, K.M.; Jones, D.A.; Cooper, M.; Sargeant, A.J.; Forte, C.A. The effect of oral supplementation with l-carnitine on maximum and submaximum exercise capacity. Graefe’s Arch. Clin. Exp. Ophthalmol. 1987, 56, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Koozehchian, M.S.; Daneshfar, A.; Fallah, E.; Agha-Alinejad, H.; Samadi, M.; Kaviani, M.; Kaveh B, M.; Jung, Y.P.; Sablouei, M.H.; Moradi, N.; et al. Effects of nine weeks L-Carnitine supplementation on exercise performance, anaerobic power, and exercise-induced oxidative stress in resistance-trained males. J. Exerc. Nutr. Biochem. 2018, 22, 7–19. [Google Scholar] [CrossRef]
- Vecchiet, L.; Di Lisa, F.; Pieralisi, G.; Ripari, P.; Menabò, R.; Giamberardino, M.A.; Siliprandi, N. Influence of L-carnitine administration on maximal physical exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 61, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Stuessi, C.; Hofer, P.; Meier, C.; Boutellier, U. L -Carnitine and the recovery from exhaustive endurance exercise: A randomised, double-blind, placebo-controlled trial. Eur. J. Appl. Physiol. 2005, 95, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Orer, G.E.; Guzel, N.A. The Effects of Acute L-carnitine Supplementation on Endurance Performance of Athletes. J. Strength Cond. Res. 2014, 28, 514–519. [Google Scholar] [CrossRef]
- Siliprandi, N.; Di Lisa, F.; Pieralisi, G.; Ripari, P.; Maccari, F.; Menabo, R.; Giamberardino, M.A.; Vecchiat, L. Metabolic changes induced by maximal exercise in human subjects following L-carnitine administration. Biochim. Biophys. Acta (BBA)-Gen. Subj. 1990, 1034, 17–21. [Google Scholar] [CrossRef]
- Soop, M.; Björkman, O.; Cederblad, G.; Hagenfeldt, L.; Wahren, J. Influence of carnitine supplementation on muscle substrate and carnitine metabolism during exercise. J. Appl. Physiol. 1988, 64, 2394–2399. [Google Scholar] [CrossRef]
- Wyss, V.; Ganzit, G.P.; Rienzi, A. Effects of L-carnitine administration on VO2max and the aerobic-anaerobic threshold in normoxia and acute hypoxia. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mor, A.; Baynaz, K.; Ipekoglu, G.; Arslanoglu, C.; Acar, K.; Cakir, H.I.; Arslanoglu, E. Effect of L-Carnitine Supplementation on Weight Loss and Body Composition of Taekwondo Players. J. Sports Educ. 2018, 1, 1–8. [Google Scholar]
- Cooper, M.B.; Jones, D.A.; Edwards, R.H.T.; Corbucci, C.; Montanari, G.; Trevisani, C. The effect of marathon running on carnitine metabolism and on some aspects of muscle mitochondrial activities and antioxidant mechanisms. J. Sports Sci. 1986, 4, 79–87. [Google Scholar] [CrossRef]
- Müller, D.M.; Seim, H.; Kiess, W.; Ster, H.L.; Richter, T. Effects of oral L-carnitine supplementation on in vivo long-chain fatty acid oxidation in healthy adults. Metabolism 2002, 51, 1389–1391. [Google Scholar] [CrossRef][Green Version]
- Parandak, K.; Arazi, H.; Khoshkhahesh, F.; Nakhostin-Roohi, B. The Effect of Two-Week L-Carnitine Supplementation on Exercise -Induced Oxidative Stress and Muscle Damage. Asian J. Sports Med. 2014, 5, 123–128. [Google Scholar] [PubMed]
- Giamberardino, M.A.; Dragani, L.; Valente, R.; Di Lisa, F.; Saggin, R.; Vecchiet, L. Effects of Prolonged L-Carnitine Administration on Delayed Muscle Pain and CK Release After Eccentric Effort. Endoscopy 1996, 17, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Arenas, J.; Huertas, R.; Campos, Y.; Díaz, A.E.; Villalón, J.M.; Vilas, E. Effects of L-carnitine on the pyruvate dehydrogenase complex and carnitine palmitoyl transferase activities in muscle of endurance athletes. FEBS Lett. 1994, 341, 91–93. [Google Scholar] [CrossRef]
- Gorostiaga, E.; Maurer, C.; Eclache, J. Decrease in Respiratory Quotient During Exercise Following L-Carnitine Supplementation. Int. J. Sports Med. 1989, 10, 169–174. [Google Scholar] [CrossRef]
- Huertas, R.; Campos, Y.; Díaz, E.; Esteban, J.; Vechietti, L.; Montanari, G.; D’Iddio, S.; Corsi, M.; Arenas, J. Respiratory chain enzymes in muscle of endurance athletes: Effect of L-carnitine. Biochem. Biophys. Res. Commun. 1992, 188, 102–107. [Google Scholar] [CrossRef]
- Oyono-Enguelle, S.; Freund, H.; Ott, C.; Gartner, M.; Heitz, A.; Marbach, J.; Maccari, F.; Frey, A.; Bigot, H.; Bach, A.C. Prolonged submaximal exercise and L-carnitine in humans. Graefe’s Arch. Clin. Exp. Ophthalmol. 1988, 58, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Swart, I.; Rossouw, J.; Loots, J.; Kruger, M. The effect of L-carnitine supplementation on plasma carnitine levels and various performance parameters of male marathon athletes. Nutr. Res. 1997, 17, 405–414. [Google Scholar] [CrossRef]
- Badrasawi, M.; Shahar, S.; Zahara, A.M.; Nor Fadilah, R.; Singh, D.K. Efficacy of L-carnitine supplementation on frailty status and its biomarkers, nutritional status, and physical and cognitive function among prefrail older adults: A double-blind, randomized, placebo-controlled clinical trial. Clin. Interv. Aging 2016, 11, 1675–1686. [Google Scholar] [CrossRef] [PubMed]
- Wächter, S.; Vogt, M.; Kreis, R.; Boesch, C.; Bigler, P.; Hoppeler, H.; Krähenbühl, S. Long-term administration of l-carnitine to humans: Effect on skeletal muscle carnitine content and physical performance. Clin. Chim. Acta 2002, 318, 51–61. [Google Scholar] [CrossRef]
- DrĂgan, I.G.; Vasiliu, A.; Georgescu, E.; Eremia, N. Studies concerning chronic and acute effects of L-carnitina in elite athletes. Physiologie 1989, 26, 111–129. [Google Scholar] [PubMed]
- Natali, A.; Santoro, D.; Brandi, L.S.; Faraggiana, D.; Ciociaro, D.; Pecori, N.; Buzzigoli, G.; Ferrannini, E. Effects of acute hypercarnitinemia during increased fatty substrate oxidation in man. Metabolism 1993, 42, 594–600. [Google Scholar] [CrossRef]
- Pistone, G.; Marino, A.; Leotta, C.; Dell’Arte, S.; Finocchiaro, G.; Malaguarnera, M. Levocarnitine administration in elderly subjects with rapid muscle fatigue: Effect on body composition, lipid profile and fatigue. Drugs Aging 2003, 20, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Nüesch, R.; Rossetto, M.; Martina, B. Plasma and urine carnitine concentrations in well-trained athletes at rest and after exercise. Influence of L-carnitine intake. Drugs Exp. Clin. Res. 1999, 25, 167–171. [Google Scholar]
- Hiatt, W.R.; Regensteiner, J.G.; Wolfel, E.E.; Ruff, L.; Brass, E.P. Carnitine and acylcarnitine metabolism during exercise in humans. Dependence on skeletal muscle metabolic state. J. Clin. Investig. 1989, 84, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.C.; Foster, C.V.; Hultman, E. Acetylcarnitine formation during intense muscular contraction in humans. J. Appl. Physiol. 1987, 63, 440–442. [Google Scholar] [CrossRef]
- Carlin, J.I.; Reddan, W.G.; Sanjak, M.; Hodach, R. Carnitine metabolism during prolonged exercise and recovery in humans. J. Appl. Physiol. 1986, 61, 1275–1278. [Google Scholar] [CrossRef] [PubMed]
- Janssen, G.M.E.; Scholte, H.R.; Vaandrager-Verduin, M.H.M.; Ross, J.D. Muscle Carnitine Level in Endurance Training and Running a Marathon. Int. J. Sports Med. 1989, 10, S153–S155. [Google Scholar] [CrossRef]
- Arenas, J.; Ricoy, J.R.; Encinas, A.R.; Pola, P.; D’Iddio, S. Carnitine in muscle, serum, and urine of nonprofessional athletes: Effects of physical exercise, training, and L-carnitine administration. Muscle Nerve 1991, 14, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Drăgan, G.I.; Vasiliu, A.; Georgescu, E.; Dumas, I. Studies concerning chronic and acute effects of L-carnitine on some biological parameters in elite athletes. Physiologie 1987, 24, 23–28. [Google Scholar]
- Drăgan, G.I.; Wagner, W.; Ploeşteanu, E. Studies concerning the ergogenic value of protein supply and 1-carnitine in elite junior cyclists. Physiologie 1988, 25, 129–132. [Google Scholar] [PubMed]
- Geidl, W.; Wais, J.; Fangmann, C.; Demisse, E.; Pfeifer, K.; Sudeck, G. Physical activity promotion in daily exercise therapy: The perspectives of exercise therapists in German rehabilitation settings. BMC Sports Sci. Med. Rehabil. 2019, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- Constantin-Teodosiu, D.; Carlin, J.I.; Cederblad, G.; Harrist, R.C.; Hultman, E. Acetyl group accumulation and pyruvate dehydrogenase activity in human muscle during incremental exercise. Acta Physiol. Scand. 1991, 143, 367–372. [Google Scholar] [CrossRef]
- Lennon, D.L.; Stratman, F.W.; Shrago, E.; Nagle, F.J.; Madden, M.; Hanson, P.; Carter, A.L. Effects of acute moderate-intensity exercise on carnitine metabolism in men and women. J. Appl. Physiol. 1983, 55, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, G.; Catania, V.E.; Bonfiglio, C.; Bertino, G.; Vicari, E.; Malaguarnera, M. Carnitine Serum Levels in Frail Older Subjects. Nutrients 2020, 12, 3887. [Google Scholar] [CrossRef] [PubMed]
- Roepstorff, C.; Halberg, N.; Hillig, T.; Saha, A.K.; Ruderman, N.B.; Wojtaszewski, J.F.P.; Richter, E.A.; Kiens, B. Malonyl-CoA and carnitine in regulation of fat oxidation in human skeletal muscle during exercise. Am. J. Physiol. Metab. 2005, 288, E133–E142. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J. Nutritional ergogenic aids and exercise performance. Nutr. Res. Rev. 1999, 12, 255–280. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, yr | Study Design; Evidence Levels | Population, Y | Comparison Samples | Intervention: L-Carnitine Dosage | Outcomes |
|---|---|---|---|---|---|
| Marconi 1985 | RT; Level 2 | 6 competitive walkers m 25.3 y | A: Before supplementation B: After supplementation | 4 g/d, 2 w | Increased serum L-carnitine, no change in blood lactate concentrations and R at fixed workload. The 6% increase in VO2 was not significantly related to carnitine intake. |
| Cooper 1986 | CT; Level 1 | 10 marathon runners m 19–25 y | A: Before supplementation B: After supplementation | 4 g/d, 10 d | L-carnitine supplementation increased the tissue content of oxidized glutathione. |
| Drăgan 1987 | RT; Level 2 | 7 athletes | A: Before supplementation B: After supplementation | 1 g/d for 6 w + 2 g/d for 10 d | Carnitine group showed better obtained higher performances. |
| Greig 1987 | CT; Level 1 | 19 healthy subjects, 7 m/12 f 27.1 ± 4.6 y | A: 9 s, 3 m, 6 f B: 10 s, 4 m, 6 f | A: 2 g/d, 2 w B: 2 g/d, 4 w | No change in maximum oxygen uptake (VO2, R). |
| Drăgan 1988 | RT; Level 2 | 110 healthy subjects | A: Before supplementation B: After supplementation | 1 g/d for 3 w | Improved athletic performance, lower lactic acid. |
| Oyono-Enguelle 1988 | RT; Level 2 | 10 exercising subjects - | A: Before supplementation B: After supplementation | 2 g/d, 4 w | After L-carnitine intake, the levels returned to their initial values 6–8 w after cessation of the supply. |
| Soop 1988 | RT; Level 2 | 7 moderately trained subjects 19–31 y | A: Before supplementation B: After supplementation | 5 g/d, 5 d | No change in O2 uptake and arterial levels and turnover of FFA after L-carnitine supplementation. |
| Gorostiaga 1989 | RT; Level 2 | 10 trained athletes, 9 m/1 f 25.8 ± 2.2 y | A: Before supplementation B: After supplementation | 2 g/d, 4 w | Reduced R during submaximal exercise after supplementation. Increased lipid use by muscles during exercise. Oxygen uptake, heart rate, blood glycerol and resting plasma free fatty acid concentrations presented a nonsignificant trend. |
| Siliprandi 1990 | CT; Level 1 | 10 moderately trained subjects 23–30 y | A: Before supplementation B: After supplementation | 2 g/d, 2 d | L-carnitine supplementation decreased plasma lactate and pyruvate concentration. |
| Vecchiet 1990 | CT; Level 1 | 10 moderately trained subjects 22–30 y | A: Before supplementation B: After supplementation | 2 g/d, one single dosage | Increased VO2, maximal oxygen uptake, power output and reduced pulmonary ventilation and plasma lactate after L-carnitine supplementation. |
| Wyss 1990 | RT; Level 2 | 7 healthy subjects 22.2 ± 2.3 y | A: Before supplementation B: After supplementation | 3 g, 1 w | Decreased R, and rate of carbohydrate transformation during hypoxia after L-carnitine supplementation. |
| Arenas 1991 | CT; Level 1 | 24 athletes 19–27 y | A: 13 and 11 s placebo B: 11 s sprinters L-carnitine C: 13 long-distance runners | 1 g/d, 24 w | The supplementation avoids the decrease of total and free muscle carnitine due to training in athletes. |
| Huertas 1992 | CT; Level 1 | 14 athletes | A: Before supplementation B: After supplementation | 2 g/d, 4 w | Increase in respiratory-chain enzyme activities in the muscle. |
| Natali 1993 | CT; Level 1 | 20 healthy subjects A: 29.5 ± 1.7 years B: 29 ± 2 y | A: 8 healthy m B: 12 healthy | A: 1 g + 0.5 g/h iv B: 3 g, iv. 40′ before exercise | No changes during exercise with L-carnitine intake, but increased fatty acid oxidation during recovery. |
| Arenas 1994 | CT; Level 1 | 16 long-distance runners 28.3 ± 7.1 | A: 8 s placebo B: 8 s L-carnitine | 2 g/d, 4 w | The supplementation increased pyruvate dehydrogenase complex activities. |
| Brass 1994 | CT; Level 1 | 14 athletes 23–40 y | A: Before supplementation B: After supplementation | 185 μmol/kg/1 d iv | No effect on skeletal muscle carnitine homeostasis during exercise: on R, muscle lactate accumulation, plasma lactate concentration, muscle glycogen utilization, plasma p-hydroxybutyrate concentration after L-supplementation. |
| Colombani 1996 | CT; Level 1 | 7 m runners 36 ± 3 y | A: Before supplementation B: After supplementation | 4 g/d, 1 d | No effect on performance, and no changes in running time and in R after L-carnitine supplementation. |
| Giamberardino 1996 | RT; Level 2 | 6 healthy untrained subjects, 26 ± 3.8 y | A: Before supplementation B: After supplementation | A: 3 g/d, 3 w | Protective effect against pain and damage. |
| Swart 1997 | RT; Level 2 | 7 marathon runners - | A: Before supplementation B: After supplementation | 2 g/d, 6 w | After L-carnitine supplementation: increase of peak treadmill running speed of 5.68%, average VO2, free carnitine levels, decreased heart rate and respiratory exchange ratio values. |
| Nuesch 1999 | RT; Level 2 | 9 athletes | A: Before supplementation B: After supplementation | 1 g/d after treadmill | In athletes without L-carnitine intake, plasma free carnitine concentration decreased significantly 10 min after exercise compared with baseline. In athletes with oral L-carnitine supplementation, the elevated plasma concentration of free carnitine at baseline did not decrease after maximal exercise. |
| Muller 2002 | RT; Level 2 | 10 healthy untrained subjects 5 m/5 f 36.4 ± 12.8 y | A: Before supplementation B: After supplementation | 3 g/d, 10 d | Significant increase in fatty acid oxidation, muscle weight, total body water and metabolic rate. |
| Wachter 2002 | RT; Level 2 | 8 healthy subjects 23–25 y | A: Before supplementation B: After supplementation | 4 g/d, 12 w | Significant increase in physical performance after L-carnitine supplementation. |
| Stuessi 2005 | CT; Level 1 | 12 m athletes, 25 ± 3 y | A: Before supplementation B: After supplementation | 2 g/d, lump sum | No enhanced performance in endurance after L-carnitine supplementation. |
| Malaguarnera 2007 | CT; Level 1 | 64 healthy elderly subjects A: 101 ± 1.3 y B: 101 ± 1.4 y | A: 32 s L-carnitine B: 34 s placebo | 2 g/d, 24 w | Improvements in fat mass, muscle mass, blood carnitine, acylcarnitine, physical and mental fatigue. |
| Chun 2011 | RT; Level 2 | 36 m soccer players 20.67± 1.21 y | A: 6 s, 2g L-carnitine B: 6 s, 3g L-carnitine, C: 6 s, 4g L-carnitine, D: 6 s,5g L-carnitine E: 6 s, 6g L-carnitine F: 6 s, no intake | 2–6 g/d, 4 w | L-carnitine can enhance endurance and recovery from fatigue in athletes, increase VO2 and decrease lactate concentration |
| Orer 2014 | CT; Level 1 | 26 footballers 18.4 ±0.5 y | A: 12 athletes placebo B: 14 athletes L-carnitine | A; 3 g/d, 1 d B: 4 g/d, 1 d | Supplementation affected performance positively in terms of running speed corresponding to specific lactate concentrations, lactic acid and Borg scale responses corresponding to running speeds. |
| Parandak 2014 | CT; Level 1 | 21 healthy subjects A: 22.2 ± 1.1 y B: 22.0 ± 1.0 y | A: 10 L-carnitine B: 11 placebo | 2 g/d, 2 w | TAC increased significantly 14 days after supplementation. Serum MDA-TBARS, CK, TAC, LDH were significantly lower 24 h after exercise. The supplementation alleviated the effects on lipid peroxidation and muscle damage markers. |
| Bradasawi 2016 | CT; Level 1 | 50 healthy subjects A: 68.2 ± 6.3 y B: 68.2 ± 6.5 y | A: 26 s L-carnitine B: 24 s placebo | 1.5 g/d, 10 w | No significant changes in free L-carnitine, total L-carnitine, acyl L-carnitine blood level and frailty biomarkers (IL-6, TNF-α, and IGF-1) between the placebo group and carnitine group. |
| Koozehchian 2018 | CT; Level 1 | 23 trained subjects A: 24.5 ± 1.5 y B: 25.5 ±1.5 y | A: 11 s placebo B: l2 s L-carnitine | 2 g/d, 9 w | No significant influence on muscle mass though upper/lower body strength improved. |
| Mor 2018 | CT; Level 1 | 16 taekwondo players 18–28 y | A: 8 s L-carnitine B: 8 s placebo | 1 g/d, 1 w | Low body fat mass. |
| Study, Year | Random Sequence Generation | Allocation Concealment | Blinding Participants | Blinding of Outcome Assessment | Incomplete Data | Selective Reporting | Other Bias | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Arenas 1991 | + | + | + | + | + | + | + | Low risk |
| Arenas 1994 | + | + | + | + | + | + | + | Low risk |
| Bradasawi 2016 | + | + | + | + | + | + | + | Low risk |
| Brass 1994 | + | + | + | + | + | + | + | Low risk |
| Colombani 1996 | + | + | + | + | + | + | + | Low risk |
| Chun 2011 | + | + | - | - | + | + | + | Low risk |
| Cooper 1986 | - | - | - | - | + | + | - | High risk |
| Dragan 1987 | + | + | + | + | + | + | + | Low risk |
| Dragan 1988 | + | + | + | + | + | + | + | Low risk |
| Giamberardino 1996 | + | + | + | + | + | + | + | Low risk |
| Gorostiaga 1989 | - | - | + | + | + | + | + | Low risk |
| Greig 1987 | + | + | + | + | + | + | + | Low risk |
| Huertas 1992 | + | + | + | + | + | + | + | Low risk |
| Koozehchian 2018 | + | + | + | + | + | + | + | Low risk |
| Malaguarnera 2007 | + | + | + | + | + | + | + | Low risk |
| Marconi 1985 | + | + | - | - | + | + | + | Low risk |
| Mor 2018 | + | + | + | + | + | + | + | Low risk |
| Muller 2002 | - | - | - | - | + | + | + | High risk |
| Natali 1993 | + | + | - | - | + | + | + | Low risk |
| Nuesch et al.1999 | - | - | - | - | + | + | + | High risk |
| Orer 2014 | + | + | + | + | + | + | + | Low risk |
| Oyono-Enguelle 1988 | - | - | - | - | + | + | + | High risk |
| Parandak 2014 | + | + | + | + | + | + | + | Low risk |
| Siliprandi 1990 | + | + | + | + | + | + | + | Low risk |
| Soop 1988 | - | - | + | + | + | + | + | Low risk |
| Stuessi 2005 | + | + | + | + | + | + | + | Low risk |
| Swart 1997 | - | - | - | - | + | + | + | High risk |
| Vecchiet 1990 | + | + | + | + | + | + | + | Low risk |
| Wachter 2002 | - | - | - | - | + | + | + | High risk |
| Wyss 1990 | - | - | + | + | + | + | + | High risk |
| Quality Assessment | Summary of Findings | Quality of Evidence GRADE | |||||
|---|---|---|---|---|---|---|---|
| N° of studies | Limitations | Inconsistency | Indirectness | Publication bias | Characteristics of | IRR (95% CI) | |
| 30 studies | No significant limitations | No serious inconsistency | No serious indirectness | Unlikely | Population: Adults Intervention: L-carnitine intake Comparison:
| Fixed and Random effects model:Table 4, Table 5, Table 6 and Table 7 | Moderate-High |
| Authors | N 1 | N 2 | Carnitine Dosage | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fixed | Random | |||||||||||||||
| Colombani 1996 | 7 | 7 | 4 g/d. 1 d | 1.3 | 0.1 | 1.4 | 0.1 | −0.936 | 0.531 | −2.092 to 0.220 | 7.93 | 7.93 | Q | 8.0319 | ||
| Chun 2011 | 6 | 6 | 2 g/d. 4 w | 1.88 | 0.46 | 1.78 | 0.28 | 0.242 | 0.535 | −0.950 to 1.434 | 7.80 | 7.80 | DF | 10 | ||
| Chun 2011 | 6 | 6 | 3 g/d. 4 w | 1.41 | 0.80 | 1.04 | 0.49 | 0.515 | 0.543 | −0.695 to 1.725 | 7.57 | 7.57 | Significance level | p = 0.6257 | ||
| Chun 2011 | 6 | 6 | 4 g/d. 4 w | 1.10 | 0.23 | 1.29 | 0.36 | −0.580 | 0.546 | −1.796 to 0.636 | 7.49 | 7.49 | I2 (inconsistency) | 0.00% | ||
| Chun 2011 | 6 | 6 | 5 g/d. 4 w | 1.38 | 0.57 | 1.50 | 0.79 | −0.161 | 0.534 | −1.350 to 1.029 | 7.83 | 7.83 | 95% CI for I2 | 0.00 to 50.67 | ||
| Chun 2011 | 6 | 6 | 6 g/d. 4 w | 1.38 | 0.47 | 1.31 | 0.25 | 0.172 | 0.534 | −1.018 to 1.361 | 7.83 | 7.83 | ||||
| Greig 1987 | 9 | 9 | 2 g/d. 2 w | 1.04 | 0.66 | 1.14 | 0.28 | −0.188 | 0.450 | −1.142 to 0.766 | 11.02 | 11.02 | ||||
| Greig 1987 | 10 | 10 | 2 g/d. 4 w | 0.8 | 0.3 | 0.9 | 0.3 | −0.319 | 0.431 | −1.225 to 0.587 | 12.00 | 12.00 | ||||
| Oyono-Enguelle 1988 | 10 | 10 | 2 g/d. 4 w | 0.93 | 0.35 | 0.86 | 0.34 | 0.194 | 0.429 | −0.708 to 1.096 | 12.11 | 12.11 | ||||
| Watcher 2002 | 8 | 8 | 4 g/d. 12 w | 0.9 | 0.1 | 0.8 | 0.2 | 0.598 | 0.484 | −0.441 to 1.637 | 9.52 | 9.52 | ||||
| Wyss 1990 | 7 | 7 | 3 g/d. 1 w | 1.5 | 0.7 | 1.4 | 0.7 | 0.134 | 0.501 | −0.958 to 1.225 | 8.90 | 8.90 | ||||
| Total (fixed effects) | 81 | 81 | −0.0257 | 0.149 | −0.321 to 0.269 | −0.172 | 0.864 | 100.00 | 100.00 | |||||||
| Total (random effects) | 81 | 81 | −0.0257 | 0.149 | −0.321 to 0.269 | −0.172 | 0.864 | 100.00 | 100.00 | |||||||
| Chun 2011 | 6 | 6 | 2 g/d. 4 w | 1.88 | 0.46 | 1.78 | 0.28 | 0.242 | 0.535 | −0.950 to 1.434 | 24.44 | 24.44 | Q | 0.9555 | ||
| Greig 1987 | 10 | 10 | 2 g/d. 4 w | 0.8 | 0.3 | 0.9 | 0.3 | −0.319 | 0.431 | −1.225 to 0.587 | 37.62 | 37.62 | DF | 2 | ||
| Oyono-Enguelle 1988 | 10 | 10 | 2 g/d. 4 w | 0.93 | 0.35 | 0.86 | 0.34 | 0.194 | 0.429 | −0.708 to 1.096 | 37.94 | 37.94 | Significance level | p = 0.6202 | ||
| Total (fixed effects) | 26 | 26 | 0.0129 | 0.264 | −0.518 to 0.544 | 0.0486 | 0.961 | 100.00 | 100.00 | I2 | 0.00% | |||||
| Total (random effects) | 26 | 26 | 0.0129 | 0.264 | −0.518 to 0.544 | 0.0486 | 0.961 | 100.00 | 100.00 | 95% CI for I2 | 0.00 to 92.98 | |||||
| Authors | N 1 | N 2 | Carn Dosage | Training | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fixed | Random | ||||||||||||||||
| Colombani 1996 | 7 | 7 | 4 g/d. 1 d | 20 km of running | 1.3 | 0.1 | 1.40 | 0.10 | −0.936 | 0.531 | −2.092 to 0.220 | 7.11 | 7.11 | Q | 10.937 | ||
| Chun 2011 | 6 | 6 | 2 g/d. 4 w | After exercise | 7.02 | 0.52 | 6.88 | 0.68 | 0.213 | 0.535 | −0.978 to 1.404 | 7.01 | 7.01 | DF | 11 | ||
| Chun 2011 | 6 | 6 | 3 g/d. 4 w | After exercise | 6.39 | 1.64 | 6.25 | 1.05 | 0.0938 | 0.533 | −1.094 to 1.282 | 7.05 | 7.05 | Significance level | p = 0.448 | ||
| Chun 2011 | 6 | 6 | 4 g/d. 4 w | After exercise | 6.80 | 2.09 | 5.87 | 1.08 | 0.516 | 0.543 | −0.694 to 1.726 | 6.79 | 6.79 | I2 (inconsistency) | 0.00% | ||
| Chun 2011 | 6 | 6 | 5 g/d. 4 w | After exercise | 6.96 | 1.87 | 6.31 | 1.56 | 0.348 | 0.537 | −0.849 to 1.546 | 6.93 | 6.93 | 95% CI for I2 | 0.00 to 58.20 | ||
| Chun 2011 | 6 | 6 | 6 g/d. 4 w | After exercise | 6.80 | 0.98 | 6.09 | 1.16 | 0.610 | 0.547 | −0.609 to 1.829 | 6.69 | 6.69 | ||||
| Greig 1987 | 9 | 9 | 2 g/d. 2 w | After 30′ of cycling | 11.7 | 2.1 | 10.10 | 2.60 | 0.645 | 0.462 | −0.334 to 1.623 | 9.40 | 9.40 | ||||
| Greig 1987 | 10 | 10 | 2 g/d. 4 w | After 30′ of cycling | 11.8 | 4.4 | 10.70 | 3.00 | 0.280 | 0.431 | −0.625 to 1.184 | 10.80 | 10.80 | ||||
| Koozehchian2018 | 11 | 11 | 2 g/d. 9 w | Maximum exercise | 5.73 | 1.14 | 4.60 | 0.97 | 1.027 | 0.438 | 0.112 to 1.942 | 10.42 | 10.42 | ||||
| Oyono-Enguelle 1988 | 10 | 10 | 2 g/d. 4 w | After 60′ cycling | 1.72 | 0.62 | 1.68 | 0.56 | 0.0648 | 0.428 | −0.835 to 0.965 | 10.91 | 10.91 | ||||
| Watcher 2002 | 8 | 8 | 4 g/d. 12 w | Power exercise | 9.3 | 0.4 | 9.20 | 1.20 | 0.106 | 0.473 | −0.909 to 1.120 | 8.95 | 8.95 | ||||
| Wyss 1990 | 7 | 7 | 3 g/d. 1 w | Maximum exercise | 8.1 | 1.7 | 8.80 | 3.30 | −0.250 | 0.503 | −1.344 to 0.845 | 7.93 | 7.93 | ||||
| Total (fixed effects) | 92 | 92 | 0.250 | 0.142 | −0.0297 to 0.529 | 1.764 | 0.079 | 100.00 | 100.00 | ||||||||
| Total (random effects) | 92 | 92 | 0.250 | 0.142 | −0.0297 to 0.529 | 1.764 | 0.079 | 100.00 | 100.00 | ||||||||
| Authors | N 1 | N 2 | Carn. Dosage | Training | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test of heterogeneity | ||
| Fixed | Random | Q | 0.1252 | ||||||||||||||
| Greig 1987 | 10 | 10 | 2 g/d. 4 w | After 30′ of cycling | 11.8 | 4.4 | 10.70 | 3.00 | 0.280 | 0.431 | −0.625 to 1.184 | 49.75 | 49.75 | DF | 1 | ||
| Oyono-Enguelle 1988 | 10 | 10 | 2 g/d. 4 w | After 60′ cycling | 1.72 | 0.62 | 1.68 | 0.56 | 0.0648 | 0.428 | −0.835 to 0.965 | 50.25 | 50.25 | Significance level | p = 0.7235 | ||
| Total (fixed effects) | 20 | 20 | 0.172 | 0.304 | −0.443 to 0.787 | 0.566 | 0.575 | 100.00 | 100.00 | I2 | 0.00% | ||||||
| Total (random effects) | 20 | 20 | 0.172 | 0.304 | −0.443 to 0.787 | 0.566 | 0.575 | 100.00 | 100.00 | 95% CI for I2 | 0.00 to 0.00 | ||||||
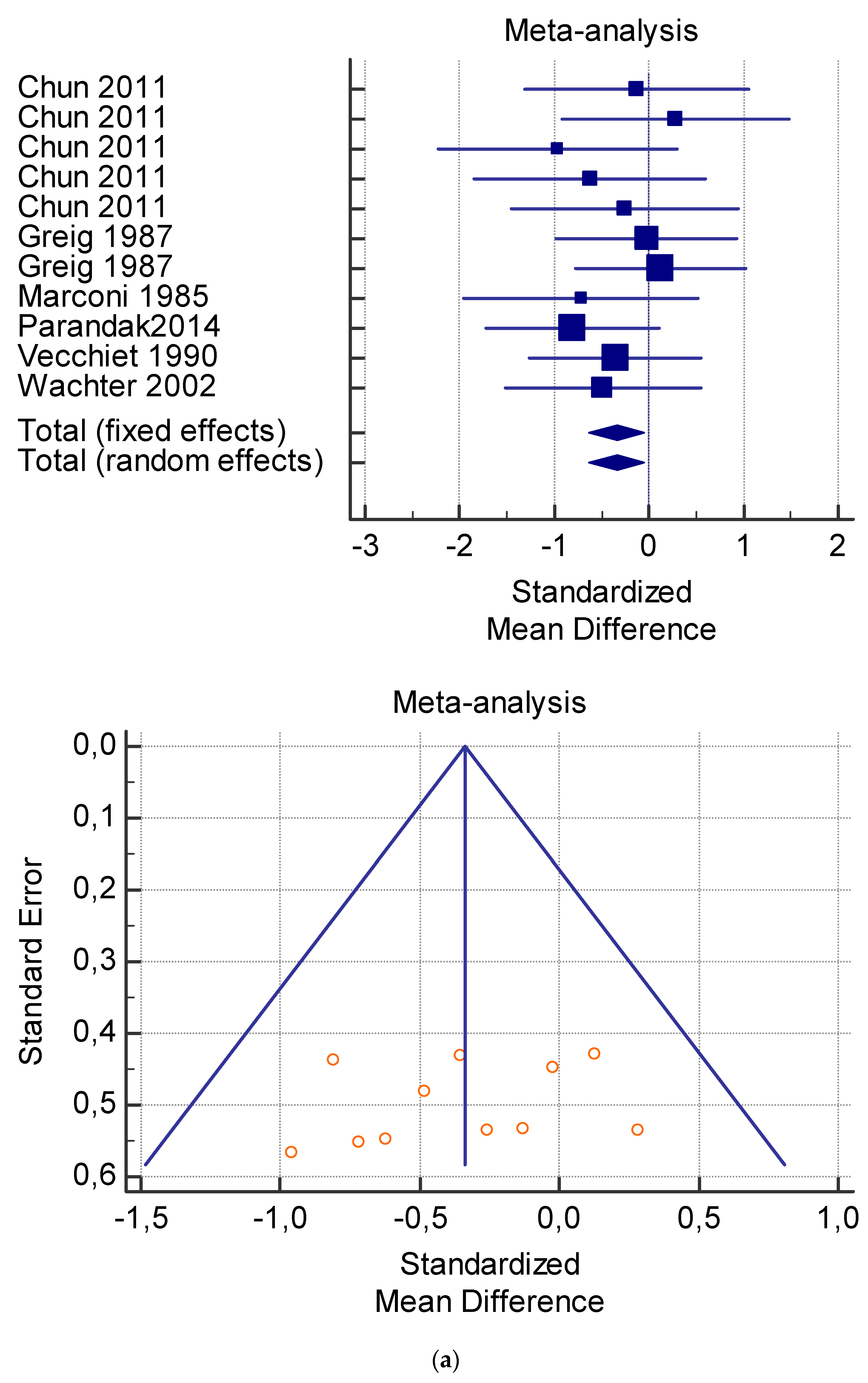
| Authors | Carnitine Dosage | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fixed | Random | |||||||||||||||
| Chun 2011 | 2 g/d, 4 w | 6 | 6 | 57.07 | 3.07 | 57.52 | 3.42 | −0.128 | 0.533 | −1.316 to 1.061 | 7.72 | 7.72 | Q | 6.3892 | ||
| Chun 2011 | 3 g/d, 4 w | 6 | 6 | 62.06 | 7.29 | 60.00 | 6.16 | 0.282 | 0.536 | −0.912 to 1.476 | 7.65 | 7.65 | DF | 10 | ||
| Chun 2011 | 4 g/d, 4 w | 6 | 6 | 59.33 | 7.57 | 67.26 | 7.66 | −0.961 | 0.568 | −2.226 to 0.304 | 6.82 | 6.82 | Significance level | p = 0.7816 | ||
| Chun 2011 | 5 g/d, 4 w | 6 | 6 | 59.78 | 6.47 | 63.64 | 4.86 | −0.622 | 0.548 | −1.843 to 0.598 | 7.32 | 7.32 | I2 (inconsistency) | 0.00% | ||
| Chun 2011 | 6 g/d, 4 w | 6 | 6 | 59.90 | 4.88 | 61.20 | 4.44 | −0.257 | 0.535 | −1.450 to 0.936 | 7.67 | 7.67 | 95% CI for I2 | 0.00 to 37.99 | ||
| Greig 1987 | 2 g/d, 2 w | 9 | 9 | 41.4 | 7.5 | 41.6 | 8.8 | −0.0233 | 0.449 | −0.975 to 0.928 | 10.90 | 10.90 | ||||
| Greig 1987 | 2 g/d, 4 w | 10 | 10 | 45.2 | 12.0 | 43.6 | 12.0 | 0.128 | 0.429 | −0.773 to 1.028 | 11.95 | 11.95 | ||||
| Marconi 1985 | 4 g/d, 2 w | 6 | 6 | 54.5 | 3.7 | 57.8 | 4.7 | −0.720 | 0.553 | −1.951 to 0.511 | 7.19 | 7.19 | ||||
| Parandak 2014 | 2 g/d, 2 w | 11 | 10 | 22.4 | 0.8 | 23.0 | 0.6 | −0.809 | 0.438 | −1.724 to 0.107 | 11.47 | 11.47 | ||||
| Vecchiet 1990 | 2 g/d, one time | 10 | 10 | 43.91 | 7.87 | 47.18 | 9.59 | −0.357 | 0.432 | −1.265 to 0.551 | 11.77 | 11.77 | ||||
| Wachter 2002 | 4 g/d, 12 w | 8 | 8 | 17.1 | 1.6 | 18.0 | 1.9 | −0.484 | 0.480 | −1.515 to 0.546 | 9.52 | 9.52 | ||||
| Total (fixed effects) | 83 | 83 | −0.339 | 0.148 | −0.632 to −0.0465 | −2.288 | 0.023 | 100.00 | 100.00 | |||||||
| Total (random effects) | 83 | 83 | −0.339 | 0.148 | −0.632 to −0.0465 | −2.288 | 0.023 | 100.00 | 100.00 | |||||||
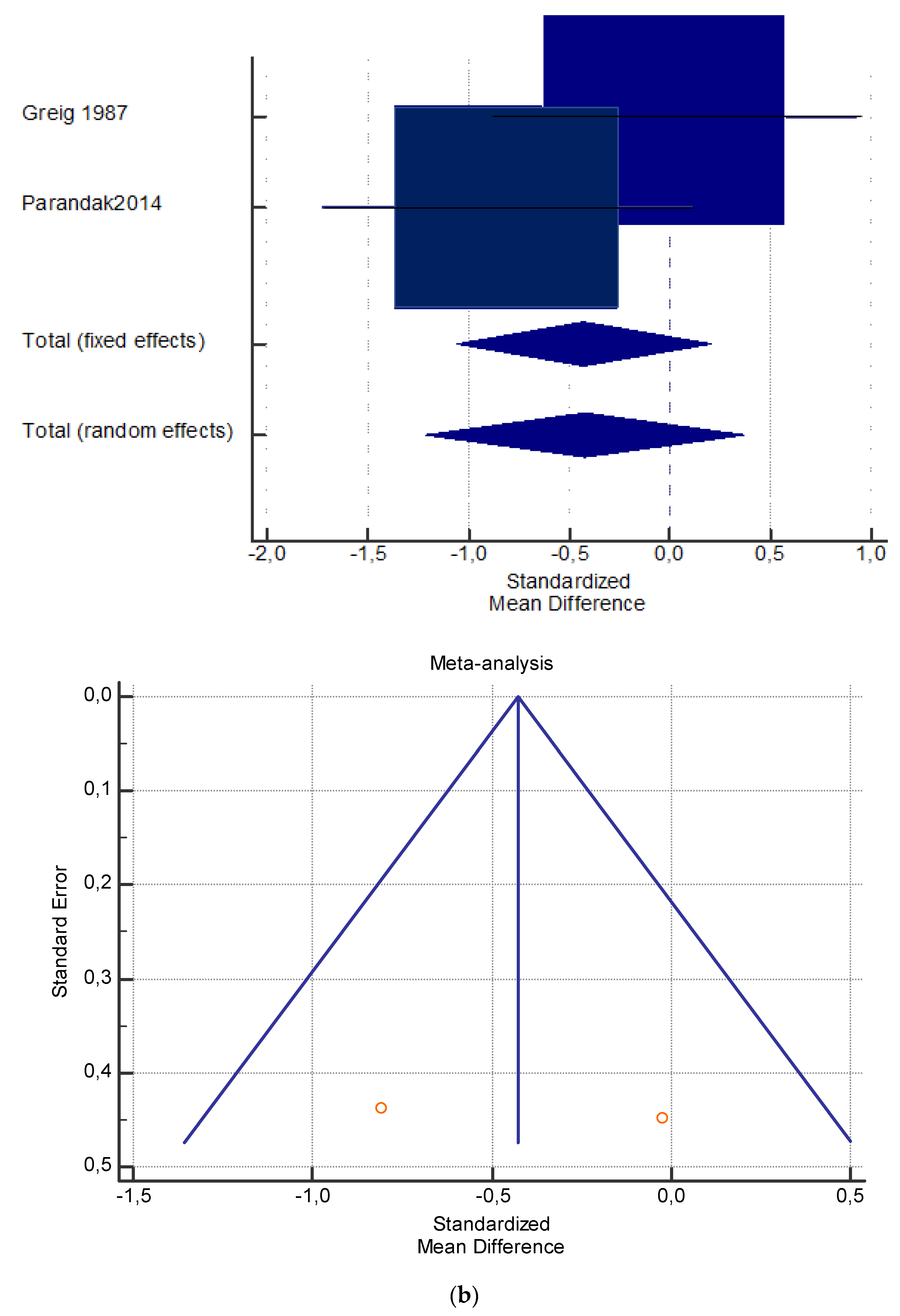
| Authors | Carnitine Dosage | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | ||
| Fixed | Random | |||||||||||||||
| Greig 1987 | 2 g/d, 2 w | 9 | 9 | 41.4 | 7.5 | 41.6 | 8.8 | −0.0233 | 0.449 | −0.975 to 0.928 | 48.72 | 49.19 | Q | 1.5691 | ||
| Parandak 2014 | 2 g/d, 2 w | 11 | 10 | 22.4 | 0.8 | 23.0 | 0.6 | −0.809 | 0.438 | −1.724 to 0.107 | 51.28 | 50.81 | DF | 1 | ||
| Total (fixed effects) | 20 | 20 | −0.426 | 0.313 | −1.061 to 0.209 | −1.359 | 0.182 | 100.0 | 100.00 | Significance level | p = 0.2103 | |||||
| Total (random effects) | 20 | 20 | −0.422 | 0.393 | −1.218 to 0.373 | −1.076 | 0.289 | 100.0 | 100.00 | I2 | 36.27% | |||||
| 95% CI for I2 | 0.00 to 0.00 | |||||||||||||||
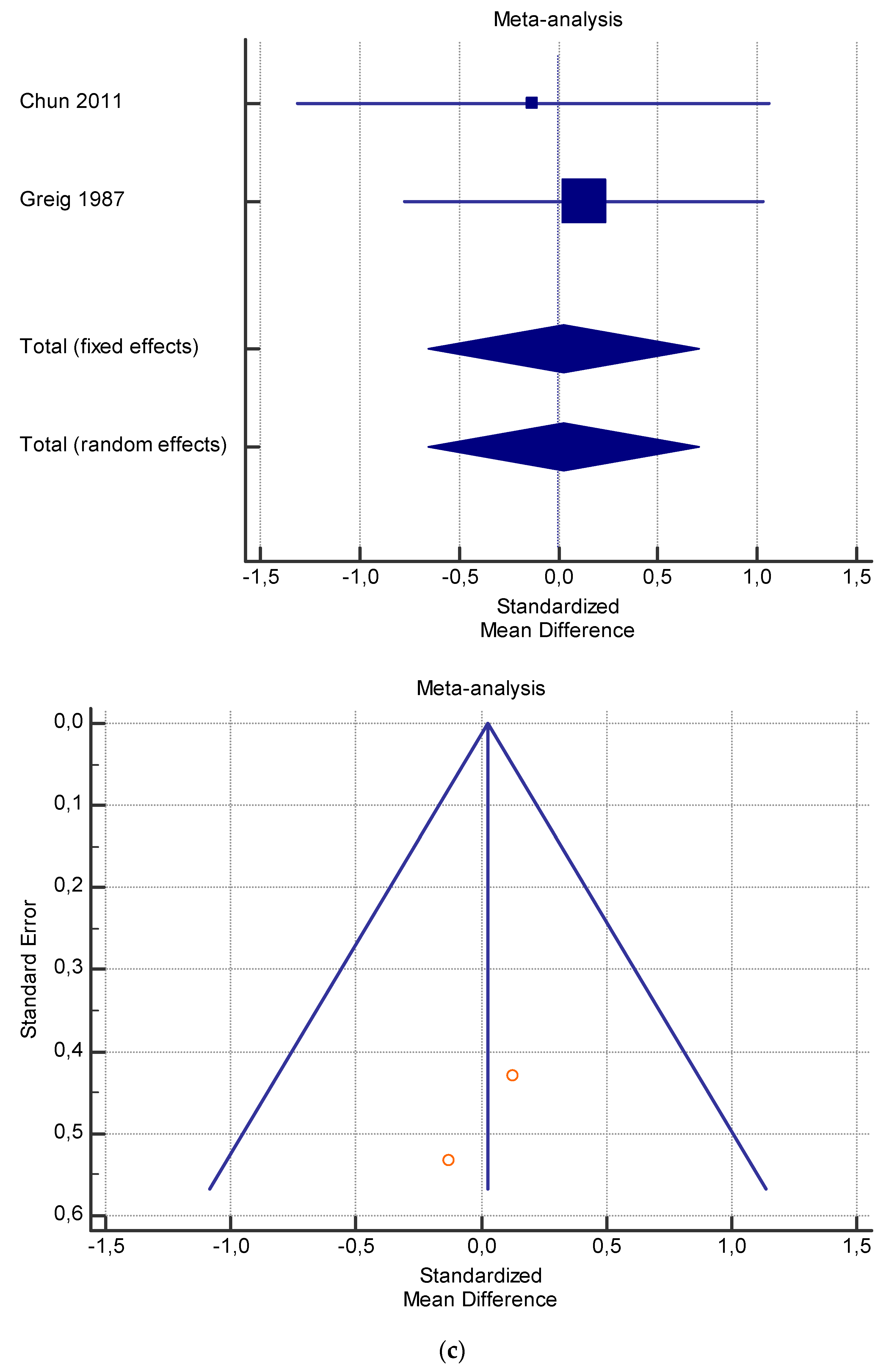
| Chun 2011 | 2 g/d, 4 w | 6 | 6 | 57.07 | 3.07 | 57.52 | 3.42 | −0.128 | 0.533 | −1.316 to 1.061 | 39.25 | 39.25 | Q | 0.1393 | ||
| Greig 1987 | 2 g/d, 4 w | 10 | 10 | 45.2 | 12.0 | 43.6 | 12.0 | 0.128 | 0.429 | −0.773 to 1.028 | 60.75 | 60.75 | DF | 1 | ||
| Total (fixed effects) | 16 | 16 | 0.0274 | 0.334 | −0.655 to 0.710 | 0.0820 | 0.935 | 100.0 | 100.00 | Significance level | p = 0.7089 | |||||
| Total (random effects) | 16 | 16 | 0.0274 | 0.334 | −0.655 to 0.710 | 0.0820 | 0.935 | 100.0 | 100.00 | I2 | 0.00% | |||||
| 95% CI for I2 | 0.00 to 0.00 | |||||||||||||||
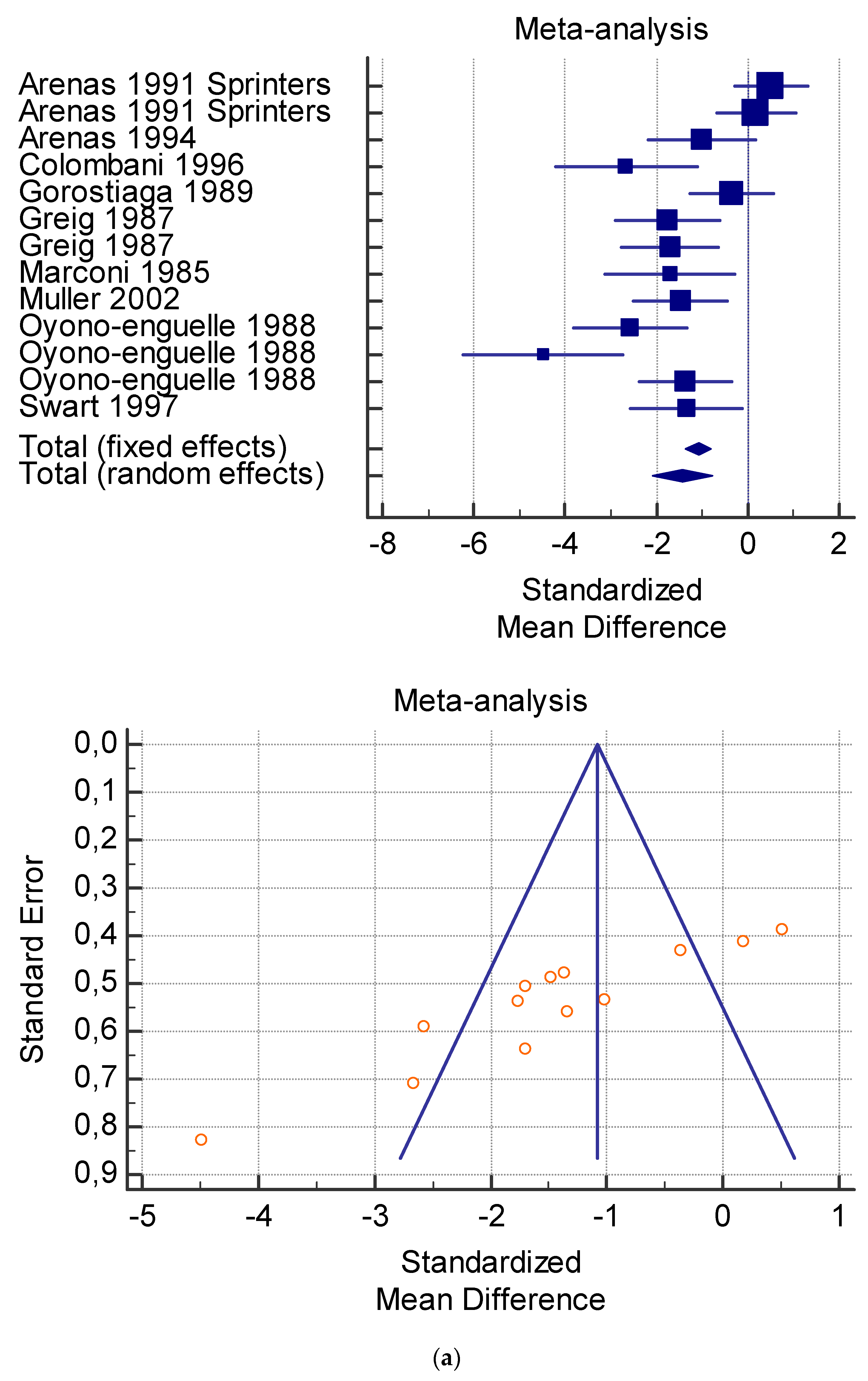
| Authors | Carnitine Dosage | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fixed | Random | ||||||||||||||||
| Arenas 1991 Runner | 1 g/d, 3 w | 13 | 13 | 28 | 2 | 26.3 | 4.134 | 0.510 | 0.386 | −0.287 to 1.308 | 13.57 | 8.60 | Q | 62.7138 | |||
| Arenas 1991 Sprinters | 1 g/d, 3 w | 11 | 11 | 22.8 | 1.8 | 22.5 | 1.4 | 0.179 | 0.411 | −0.678 to 1.036 | 11.99 | 8.47 | DF | 12 | |||
| Arenas 1994 | 2 g/d, 4 w | 7 | 7 | 30.9 | 3.8 | 34.8 | 3.4 | −1.012 | 0.536 | −2.179 to 0.155 | 7.06 | 7.76 | Significance level | p < 0.0001 | |||
| Colombani 1996 | 4 g/d, 1 d | 7 | 7 | 51.4 | 2.8 | 57.9 | 1.6 | −2.668 | 0.710 | −4.215 to −1.120 | 4.02 | 6.73 | I2 (inconsistency) | 80.87% | |||
| Gorostiaga 1989 | 2 g/d, 4 w | 10 | 10 | 44.5 | 4.5 | 46.1 | 4.0 | −0.360 | 0.432 | −1.268 to 0.548 | 10.86 | 8.35 | 95% CI for I2 | 68.26 to 88.47 | |||
| Greig 1987 | 2 g/d, 2 w | 9 | 9 | 55.3 | 7.6 | 78.9 | 16.3 | −1.767 | 0.537 | −2.905 to −0.629 | 7.03 | 7.75 | |||||
| Greig 1987 | 2 g/d, 4 w | 10 | 10 | 41.3 | 8.4 | 56.0 | 8.2 | −1.696 | 0.505 | −2.758 to −0.634 | 7.94 | 7.94 | |||||
| Marconi 1985 | 4 g/d, 2 w | 6 | 6 | 64.3 | 2.1 | 86.8 | 17.1 | −1.704 | 0.636 | −3.122 to −0.287 | 5.00 | 7.16 | |||||
| Muller 2002 | 3 g/d, 10 d | 10 | 10 | 47.07 | 6.82 | 59.86 | 9.52 | −1.479 | 0.488 | −2.504 to −0.454 | 8.51 | 8.04 | |||||
| Oyono-Eguelle 1988 | 2 g/d, 3 w | 10 | 10 | 62.0 | 3.8 | 72.9 | 4.3 | −2.572 | 0.591 | −3.813 to −1.332 | 5.81 | 7.44 | |||||
| Oyono-Enguelle 1988 | 2 g/d, 4 w | 10 | 10 | 62.0 | 3.8 | 79.8 | 3.8 | −4.486 | 0.829 | −6.227 to −2.745 | 2.95 | 6.05 | |||||
| Oyono-Enguelle 1988 | 2 g/d, 12 w | 10 | 10 | 62.0 | 3.8 | 67.4 | 3.8 | −1.361 | 0.479 | −2.368 to −0.354 | 8.82 | 8.09 | |||||
| Swart 1997 | 2 g/d, 6 w | 7 | 7 | 52.9 | 5.1 | 61.93 | 7.3 | −1.342 | 0.561 | −2.564 to −0.120 | 6.44 | 7.61 | |||||
| Total (fixed effects) | 120 | 120 | −1.085 | 0.142 | −1.366 to −0.805 | −7.624 | <0.001 | 100.00 | 100.00 | ||||||||
| Total (random effects) | 120 | 120 | −1.417 | 0.331 | −2.069 to −0.764 | −4.277 | <0.001 | 100.00 | 100.00 | ||||||||
| Authors | Carn. Dosage | Training | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | ||
| Arenas 1991 Runner | 1 g/d, 3 w | After exercise | 13 | 13 | 26.3 | 1.9 | 29.0 | 2.7 | −1.120 | 0.410 | −1.967 to −0.273 | 32.13 | 23.93 | Q | 26.2778 | ||
| Arenas 1991 Sprinters | 1 g/d, 3 w | After exercise | 11 | 11 | 21.6 | 1.5 | 24.3 | 1.4 | −1.790 | 0.491 | −2.814 to −0.766 | 22.44 | 23.00 | DF | 4 | ||
| Colombani 1996 | 4 g/d, 1 d | After running | 7 | 7 | 57.9 | 1.6 | 122.4 | 8.3 | −10.100 | 1.973 | −14.399 to −5.801 | 1.39 | 7.79 | Significance level | 84.78 | ||
| Gorostiaga 1989 | 2 g/d, 4 w | After 40′ of exercise | 10 | 10 | 47.4 | 5.9 | 49.1 | 4.9 | −0.300 | 0.431 | −1.205 to 0.605 | 29.14 | 23.70 | I2 (inconsistency) | 84.78% | ||
| Marconi 1985 | 4 g/d, 2 w | After 120′ of treadmill | 6 | 6 | 86.8 | 17.1 | 109.8 | 13.4 | −1.382 | 0.603 | −2.725 to −0.0385 | 14.89 | 21.59 | 95% CI for I2 | 66.07 to 93.17 | ||
| Total (fixed effects) | 47 | 47 | −1.195 | 0.233 | −1.657 to −0.733 | −5.138 | <0.001 | 100.00 | 100.00 | ||||||||
| Total (random effects) | 47 | 47 | −1.918 | −1.836 | −3.139 to −0.533 | −2.798 | 0.006 | 100.00 | 100.00 | ||||||||
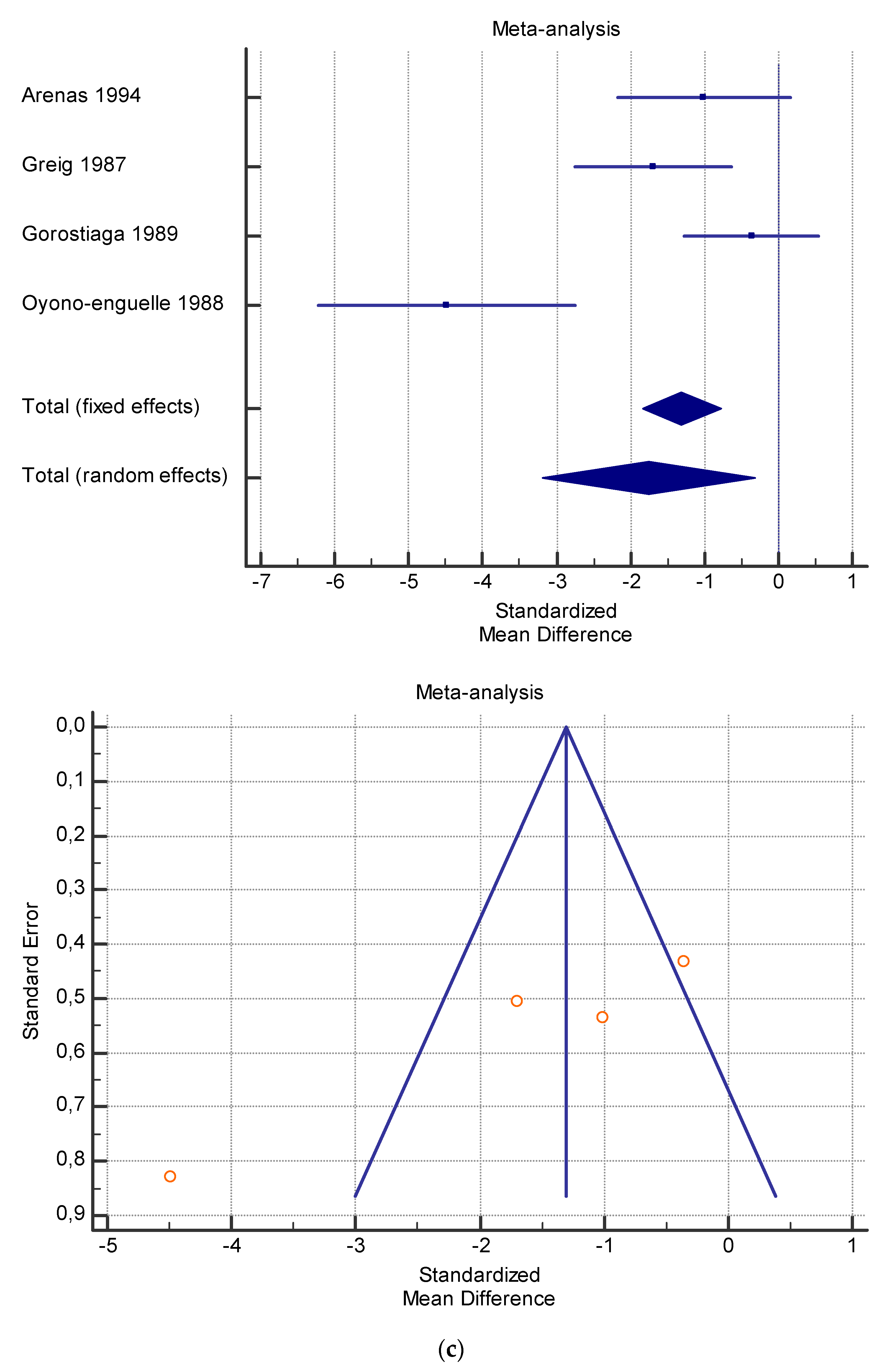
| Authors | Carnitine Dosage | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | |||
| Fixed | Random | ||||||||||||||||
| Arenas 1994 | 2 g/d, 4 w | 7 | 7 | 30.9 | 3.8 | 34.8 | 3.4 | −1.012 | 0.536 | −2.179 to 0.155 | 24.52 | 25.62 | Q | 20.4203 | |||
| Greig 1987 | 2 g/d, 4 w | 10 | 10 | 41.3 | 8.4 | 56.0 | 8.2 | −1.696 | 0.505 | −2.758 to −0.634 | 27.55 | 26.03 | DF | 3 | |||
| Gorostiaga 1989 | 2 g/d, 4 w | 10 | 10 | 44.5 | 4.5 | 46.1 | 4.0 | −0.360 | 0.432 | −1.268 to 0.548 | 37.68 | 26.97 | Significance level | p = 0.0001 | |||
| Oyono-Enguelle 1988 | 2 g/d, 4 w | 10 | 10 | 62.0 | 3.8 | 79.8 | 3.8 | −4.486 | 0.829 | −6.227 to −2.745 | 10.25 | 21.37 | I2 | 85.31% | |||
| Total (fixed effects) | 37 | 37 | −1.311 | 0.265 | −1.839 to −0.782 | −4.942 | <0.001 | 100.00 | 100.00 | 95% CI for I2 | 63.69 to 94.06 | ||||||
| Total (random effects) | 37 | 37 | −1.757 | 0.718 | −3.187 to −0.326 | −2.448 | 0.017 | 100.00 | 100.00 | ||||||||
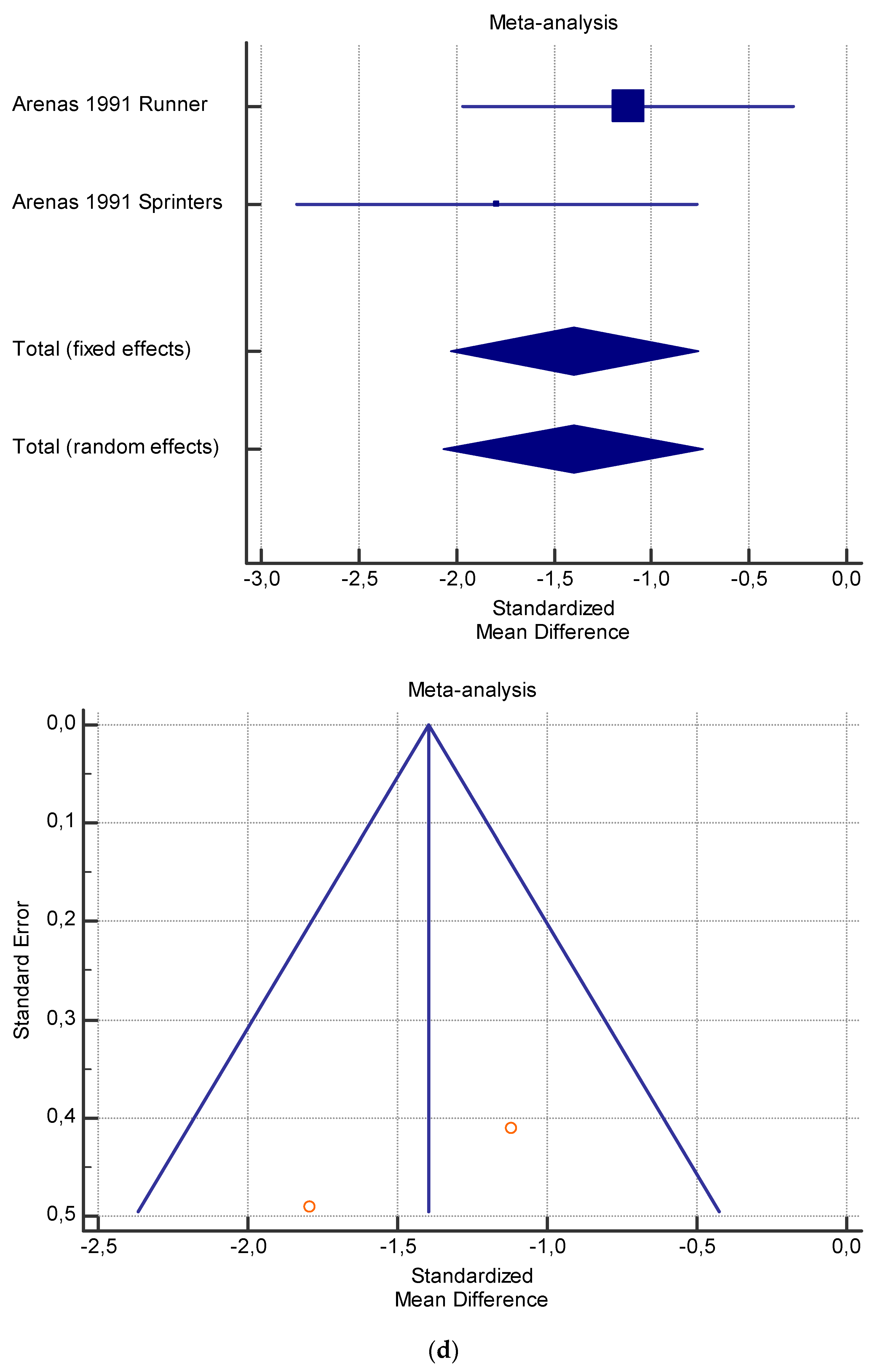
| Authors | Carn. Dosage | Training | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | ||
| Fixed | Random | ||||||||||||||||
| Arenas 1991 Runners | 1 g/d, 3 w | After exercise | 13 | 13 | 26.3 | 1.9 | 29.0 | 2.7 | −1.120 | 0.410 | −1.967 to −0.273 | 58.88 | 58.09 | Q | 1.0969 | ||
| Arenas 1991 Sprinters | 1 g/d, 3 w | After exercise | 11 | 11 | 21.6 | 1.5 | 24.3 | 1.4 | −1.790 | 0.491 | −2.814 to −0.766 | 41.12 | 41.91 | DF | 1 | ||
| Total (fixed effects) | 24 | 24 | −1.396 | 0.315 | −2.029 to −0.762 | −4.432 | <0.001 | 100.00 | 100.00 | Significance level | p = 0.2949 | ||||||
| Total (random effects) | 24 | 24 | −1.401 | 0.331 | −2.066 to −0.735 | −4.236 | <0.001 | 100.00 | 100.00 | I2 | 8.83% | ||||||
| 95% CI for I2 | 0.00 to 0.00 | ||||||||||||||||
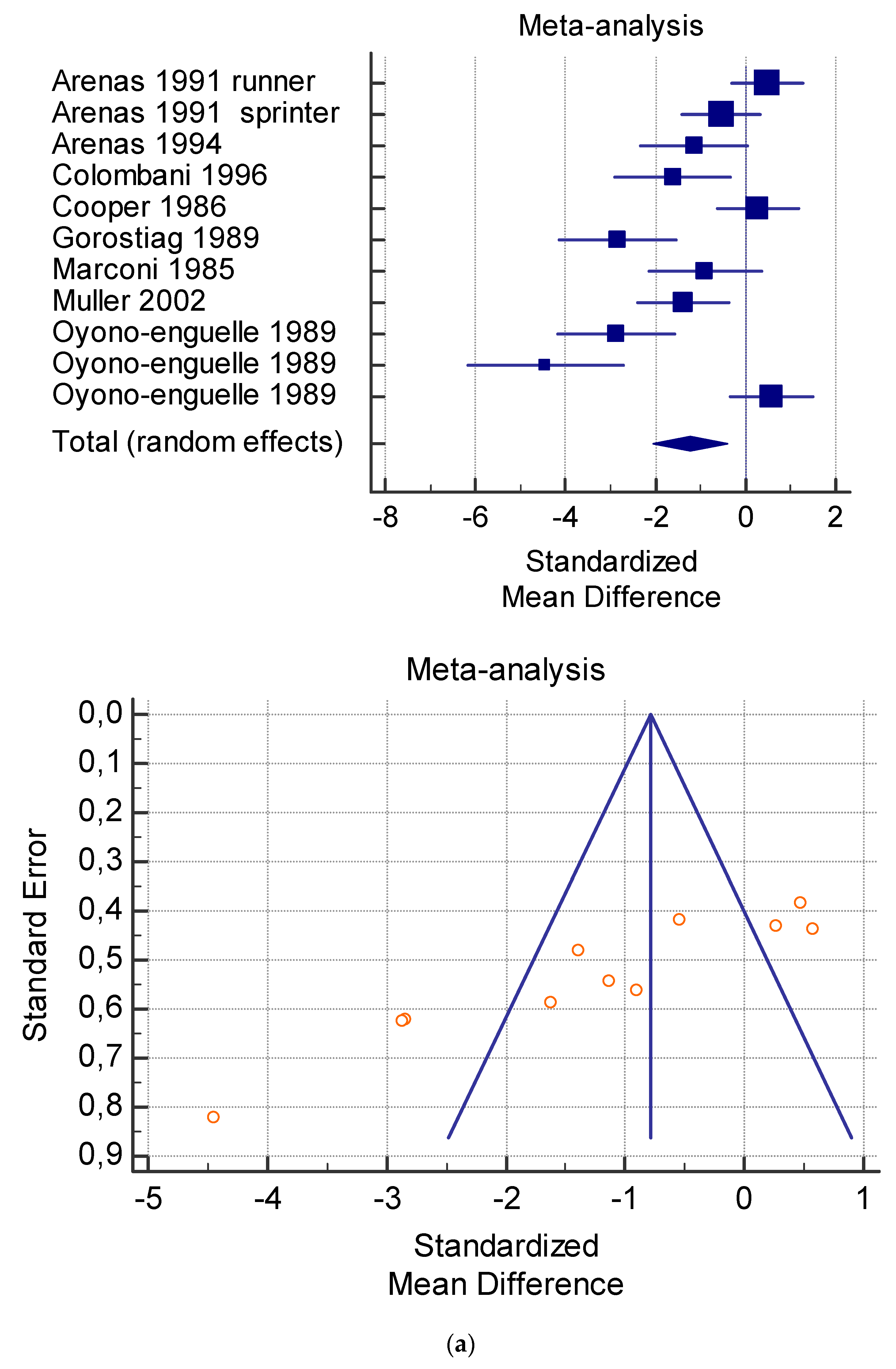
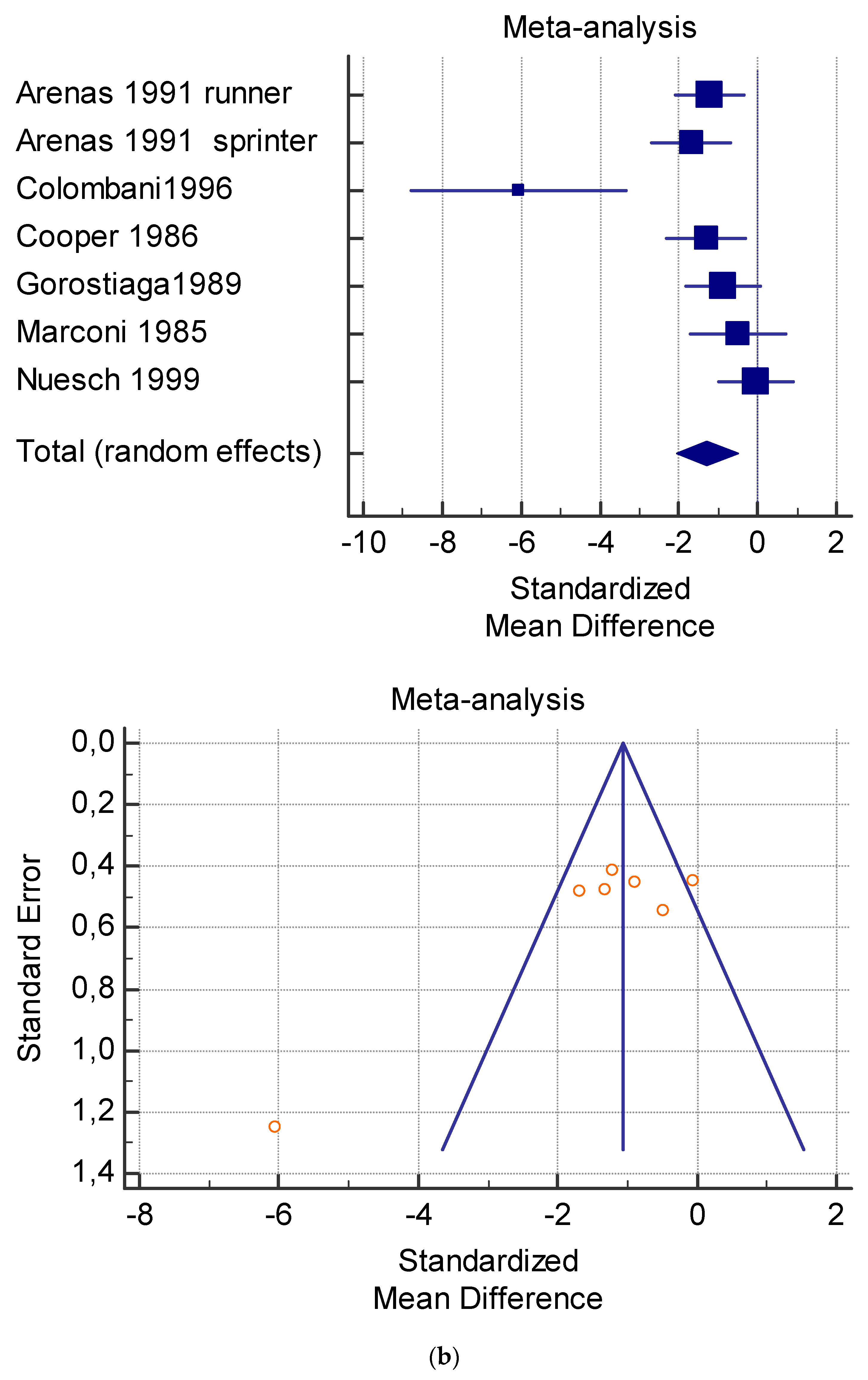
| Authors | Carnitine Dosage | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fixed | Random | Q | 72.6140 | ||||||||||||||
| Arenas 1991 runner | 1 g/d, 3 w | 13 | 13 | 40.0 | 3 | 38.0 | 5 | 0.470 | 0.385 | −0.326 to 1.265 | 15.50 | 9.84 | DF | 10 | |||
| Arenas 1991 sprinter | 2 g/d, 3 w | 11 | 11 | 34.0 | 4 | 36.0 | 3 | −0.544 | 0.418 | −1.417 to 0.328 | 13.16 | 9.70 | I2 (inconsistency) | 86.23% | |||
| Arenas 1994 | 2 g/d, 4 w | 7 | 7 | 27.8 | 3.5 | 31.7 | 2.9 | −1.136 | 0.544 | −2.322 to 0.0504 | 7.77 | 9.08 | 95% CI for I2 | 77.18 to 91.69 | |||
| Colombani 1996 | 4 g/d, 1 d | 7 | 7 | 41.5 | 2.9 | 45.8 | 2.0 | −1.616 | 0.586 | −2.893 to −0.339 | 6.70 | 8.86 | |||||
| Cooper 1986 | 4 g/d, 10 d | 10 | 10 | 35.4 | 8.9 | 33.1 | 7.9 | 0.262 | 0.430 | −0.642 to 1.166 | 12.44 | 9.64 | |||||
| Gorostiag 1989 | 2 g/d, 4 w | 10 | 10 | 31.4 | 1.7 | 39.2 | 3.3 | −2.846 | 0.621 | −4.151 to −1.541 | 5.97 | 8.67 | |||||
| Marconi 1985 | 4 g/d, 2 w | 6 | 6 | 48.0 | 8.3 | 56.8 | 9.6 | −0.905 | 0.564 | −2.161 to 0.351 | 7.24 | 8.98 | |||||
| Muller 2002 | 3 g/d, 10 d | 10 | 10 | 41.10 | 6.54 | 52.74 | 9.23 | −1.394 | 0.482 | −2.405 to −0.382 | 9.92 | 9.40 | |||||
| Oyono-Enguelle 1989 | 2 g/d, 3 w | 10 | 10 | 49.8 | 2.3 | 59.4 | 3.9 | −2.872 | 0.624 | −4.183 to −1.560 | 5.91 | 8.66 | |||||
| Oyono-Enguelle 1989 | 2 g/d, 4 w | 10 | 10 | 49.8 | 2.3 | 64.1 | 3.7 | −4.445 | 0.823 | −6.175 to −2.716 | 3.40 | 7.57 | |||||
| Oyono-Enguelle 1989 | 2 g/d, 12 w | 10 | 10 | 49.8 | 2.3 | 48.0 | 3.5 | 0.582 | 0.438 | −0.338 to 1.502 | 12.00 | 9.61 | |||||
| Total fixed effects | 104 | 104 | −0.787 | 0.152 | −1.086 to −0.488 | −5.189 | <0.001 | 100.00 | 100.00 | ||||||||
| Total random effects | 104 | 104 | −1.216 | 0.416 | −2.036 to −0.395 | −2.921 | 0.004 | 100.00 | 100.00 | ||||||||
| Authors | Carn. Dosage | Training | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | ||
| Fixed | Random | Q | 24.4106 | ||||||||||||||
| DF | 6 | ||||||||||||||||
| Arenas 1991 runner | 1 g/d, 3 w | After running | 13 | 13 | 22.9 | 1.8 | 25.7 | 2.6 | SMD | SE | 95% CI | Weight (%) | SMD | Significance level | p = 0.0004 | ||
| Arenas 1991 sprinter | 2 g/d, 3 w | After running | 11 | 11 | 18.2 | 1.5 | 21.0 | 1.7 | −1.680 | 0.482 | −2.686 to −0.675 | Fixed | 10.38 | I2 (inconsistency) | 75.42% | ||
| Colombani1996 | 4 g/d, 1 d | After running | 7 | 7 | 45.8 | 2.0 | 70.0 | 4.9 | −1.213 | 0.415 | −2.070 to −0.355 | 20.37 | −1.213 | 95% CI for I2 | 48.00 to 88.38 | ||
| Cooper 1986 | 4 g/d, 10 d | After 158′ of Marathon | 10 | 10 | 22.5 | 2.8 | 35.0 | 12.6 | −1.680 | 0.482 | −2.686 to −0.675 | 15.13 | −1.680 | ||||
| Gorostiaga1989 | 2 g/d, 4 w | After 40′ of exercise | 10 | 10 | 35.5 | 4.4 | 38.9 | 2.8 | −6.052 | 1.248 | −8.772 to −3.332 | 2.26 | −6.052 | ||||
| Marconi 1985 | 4 g/d, 2 w | After 120′ of treadmill | 6 | 6 | 56.8 | 9.6 | 62.5 | 11.6 | −1.312 | 0.476 | −2.311 to −0.312 | 15.52 | −1.312 | ||||
| Nuesch 1999 | 1 g/d | 10′ after maximal treadmill | 9 | 9 | 71.3 | 10.2 | 71.8 | 10.7 | −0.883 | 0.450 | −1.829 to 0.0635 | 17.32 | −0.883 | ||||
| Total (fixed effects) | 66 | 66 | −0.494 | 0.542 | −1.702 to 0.714 | −5.660 | <0.001 | 11.96 | −0.494 | ||||||||
| Total (random effects) | 66 | 66 | −0.0455 | 0.449 | −0.997 to 0.906 | −3.253 | 0.001 | 17.44 | −0.0455 | ||||||||
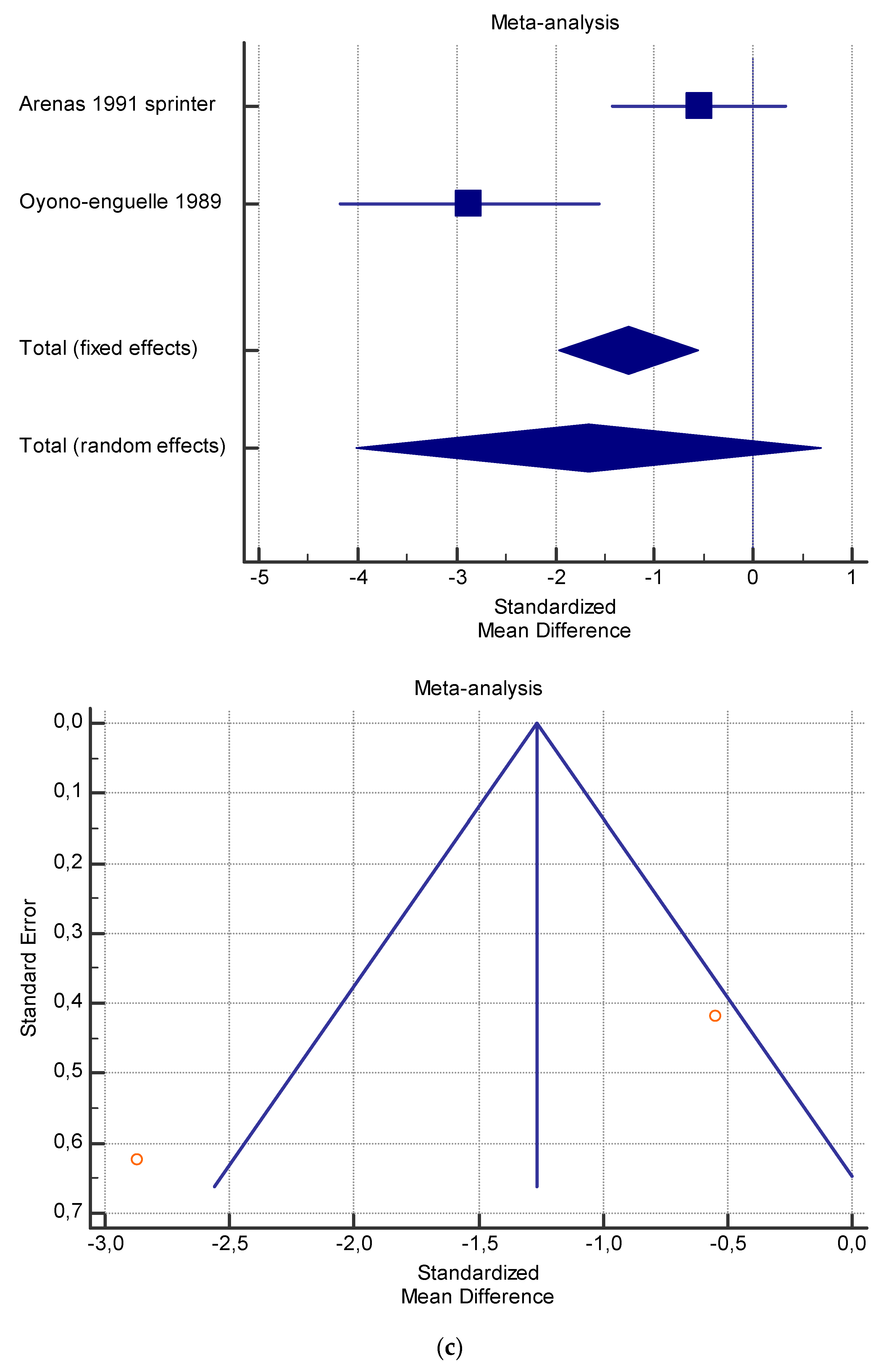
| Authors | Carnitine Dosage | N1 | N2 | Mean 1 | SD 1 | Mean 2 | SD 2 | SMD | SE | 95% CI | t | p | Weight (%) | Test for Heterogeneity | |||
| Fixed | Random | ||||||||||||||||
| Arenas 1991 sprinter | 2 g/d, 3 w | 11 | 11 | 34.0 | 4 | 36.0 | 3 | −0.544 | 0.418 | −1.417 to 0.328 | 69.01 | 51.98 | Q | 9.5950 | |||
| Oyono-Enguelle 1989 | 2 g/d, 3 w | 10 | 10 | 49.8 | 2.3 | 59.4 | 3.9 | −2.872 | 0.624 | −4.183 to −1.560 | 30.99 | 48.02 | DF | 1 | |||
| Total fixed effects | 21 | 21 | −1.266 | 0.347 | −1.968 to −0.563 | −3.642 | 0.001 | 100.00 | 100.00 | Significance level | p = 0.0020 | ||||||
| Total random effects | 21 | 21 | −1.662 | 1.163 | −4.012 to 0.688 | −1.429 | 0.161 | 100.00 | 100.00 | I2 | 89.58% | ||||||
| 95% CI for I2 | 61.34 to 97.19 | ||||||||||||||||
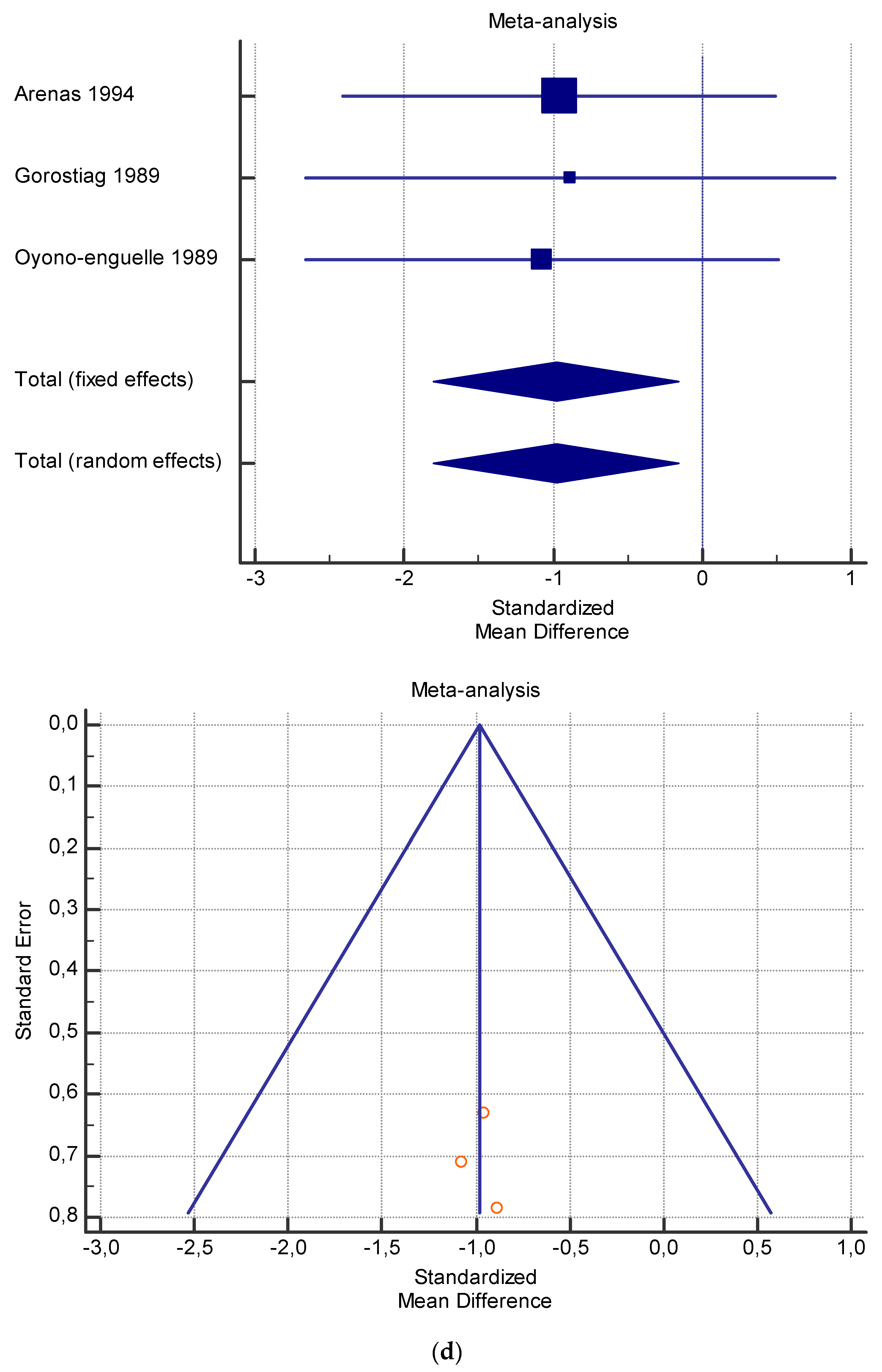
| Arenas 1994 | 2 g/d, 4 w | 7 | 7 | 27.8 | 3.5 | 31.7 | 2.9 | −0.959 | 0.631 | −2.413 to 0.495 | 41.10 | 41.10 | Q | 0.03256 | |||
| Gorostiaga 1989 | 2 g/d, 4 w | 10 | 10 | 31.4 | 1.7 | 39.2 | 3.3 | −0.888 | 0.785 | −2.664 to 0.888 | 26.51 | 26.51 | DF | 2 | |||
| Oyono-Enguelle 1989 | 2 g/d, 4 w | 10 | 10 | 49.8 | 2.3 | 64.1 | 3.7 | −1.075 | 0.710 | −2.657 to 0.508 | 32.39 | 32.39 | Significance level | p = 0.9839 | |||
| Total fixed effects | 27 | 27 | −0.978 | 0.404 | −1.801 to −0.154 | −2.418 | 0.021 | 100.00 | 100.00 | I2 | 0.00% | ||||||
| Total random effects | 27 | 27 | −0.978 | 0.404 | −1.801 to −0.154 | −2.418 | 0.021 | 100.00 | 100.00 | 95% CI for I2 | 0.00 to 0.00 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vecchio, M.; Chiaramonte, R.; Testa, G.; Pavone, V. Clinical Effects of L-Carnitine Supplementation on Physical Performance in Healthy Subjects, the Key to Success in Rehabilitation: A Systematic Review and Meta-Analysis from the Rehabilitation Point of View. J. Funct. Morphol. Kinesiol. 2021, 6, 93. https://doi.org/10.3390/jfmk6040093
Vecchio M, Chiaramonte R, Testa G, Pavone V. Clinical Effects of L-Carnitine Supplementation on Physical Performance in Healthy Subjects, the Key to Success in Rehabilitation: A Systematic Review and Meta-Analysis from the Rehabilitation Point of View. Journal of Functional Morphology and Kinesiology. 2021; 6(4):93. https://doi.org/10.3390/jfmk6040093
Chicago/Turabian StyleVecchio, Michele, Rita Chiaramonte, Gianluca Testa, and Vito Pavone. 2021. "Clinical Effects of L-Carnitine Supplementation on Physical Performance in Healthy Subjects, the Key to Success in Rehabilitation: A Systematic Review and Meta-Analysis from the Rehabilitation Point of View" Journal of Functional Morphology and Kinesiology 6, no. 4: 93. https://doi.org/10.3390/jfmk6040093
APA StyleVecchio, M., Chiaramonte, R., Testa, G., & Pavone, V. (2021). Clinical Effects of L-Carnitine Supplementation on Physical Performance in Healthy Subjects, the Key to Success in Rehabilitation: A Systematic Review and Meta-Analysis from the Rehabilitation Point of View. Journal of Functional Morphology and Kinesiology, 6(4), 93. https://doi.org/10.3390/jfmk6040093