Exercise Prescription in Renal Transplant Recipients: From Sports Medicine Toward Multidisciplinary Aspects: A Pilot Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Therapeutic Plan of Intervention: Moderate Individualized Combined Physical Activity and Nutritional Record
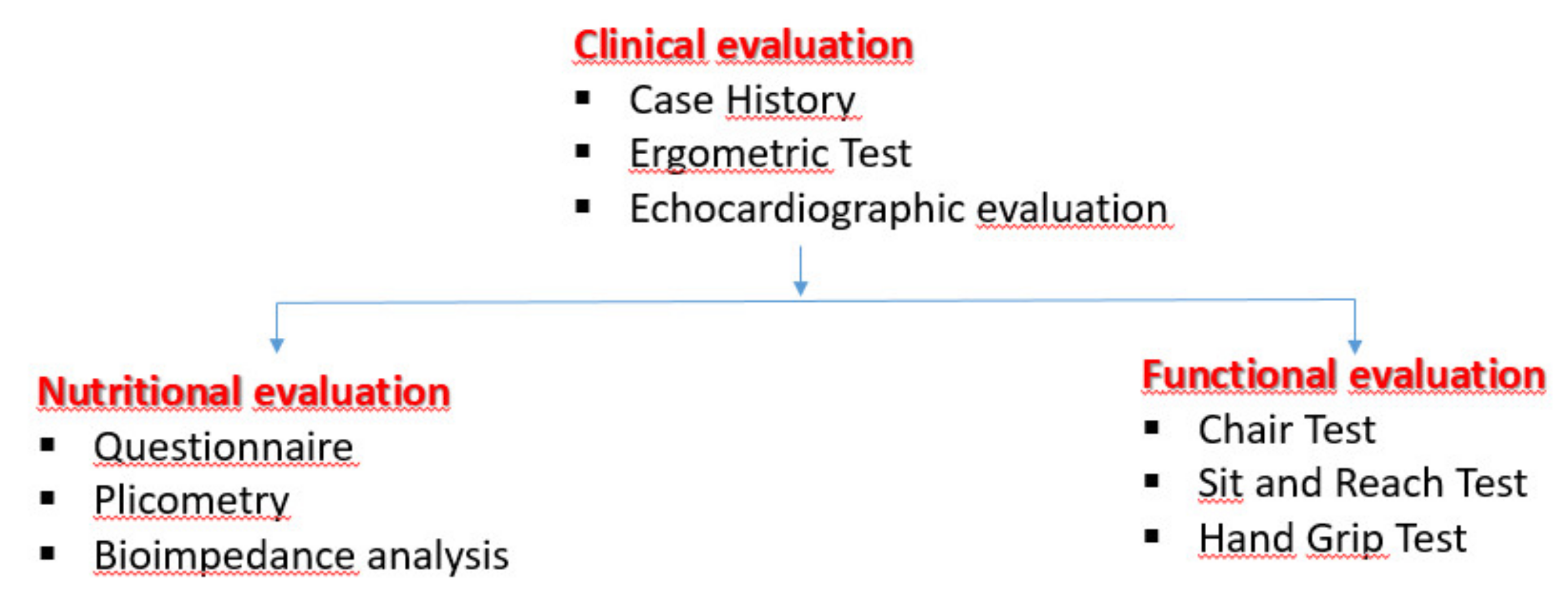
2.2. Flow-chart of the Exercise Program Evaluation and Echocardiographic Evaluation.
2.3. Echocardiographic Evaluation
2.4. Adherence to the Mediterranean Diet
3. Statistical Analysis
4. Results
4.1. Population Studied
4.2. Primary Outcomes: Anthropometric Parameters
4.3. Secondary Outcomes
5. Discussion
6. Conclusions
7. Limitations of the Study
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Oterdoom, L.H.; de Vries, A.P.; van Ree, R.M.; Gansevoort, R.T.; van Son, W.J.; van der Heide, J.J.; Navis, G.; de Jong, P.E.; Gans, R.O.; Bakker, S.J. N-terminal pro-B-type natriuretic peptide and mortality in renal transplant recipients versus the general population. Transplantation 2009, 87, 1562–1570. [Google Scholar] [CrossRef]
- Hewing, B.; Dehn, A.M.; Staeck, O.; Knebel, F.; Spethmann, S.; Stangl, K.; Baumann, G.; Dreger, H.; Budde, K.; Halleck, F. Improved left ventricular structure and function after successful kidney transplantation. Kidney Blood Press Res. 2016, 41, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, L.; Pisani, A.; Capuano, I.; Morgillo, M.; Memoli, A.; Riccio, E.; Guida, B. Nutritional management in renal transplant recipients: A transplant team opportunity to improve graft survival. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 319–324. [Google Scholar] [CrossRef]
- Bernardi, A.; Biasia., F.; Pati, T.; Piva, M.; Scaramuzzo, P.; Stoppa, F.; Bucciante, G. Factors affecting nutritional status, response to exercise, and progression of chronic rejection in kidney transplant recipients. J. Ren. Nutr. 2005, 15, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Neale, J.; Smith, A.C. Cardiovascular risk factors following renal transplant. World J. Transpl. 2015, 5, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Stefani, L.; Galanti, G.; Klika, K. Clinical Implementation of Exercise Guidelines for Cancer Patients: Adaptation of ACSM’s Guidelines to the Italian Model. Funct. Morphol. Kinesiol. 2017, 2, 4. [Google Scholar] [CrossRef]
- Stefani, L.; Galanti, G. Physical Exercise Prescription in Metabolic Chronic Disease. Adv. Exp. Med. Biol. 2017, 1005, 123–141. [Google Scholar] [CrossRef]
- Galanti, G.; Stefani, L.; Mascherini, G.; Petri, C.; Corsani, I.; Francini, L.; Cattozzo, A.; Gianassi, M.; Minetti, E.; Pacini, A.; et al. Short-term prospective study of prescribed physical activity in kidney transplant recipients. Intern. Emerg. Med. 2016, 1, 61–67. [Google Scholar] [CrossRef]
- Roi, G.S.; Mosconi, G.; Totti, T.; Angelini, M.L.; Brugin, E.; Sarto, P.; Merlo, L.; Sgarzi, S.; Stancari, M.; Todeschini, P.; et al. Renal function and physical fitness after 12-mo supervised training in kidney transplant recipients. World J. Transpl. 2018, 8, 13–22. [Google Scholar] [CrossRef]
- ACSM. Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; Available online: http://www.acsm.org (accessed on 1 July 2013).
- Płonek, T.; Pupka, A.; Marczak, J.; Skóra, J.; Blocher, D. The influence of regular exercise training on kidney transplant recipients’ health and fitness condition. Adv. Clin. Exp. Med. 2013, 22, 2203–2208. [Google Scholar]
- Stefani, L.; Riggs, K.; Mascherini, G.; Mazzoni, F.; Lunghi, A.; Petri, C.; Petreni, P.; Di Costanzo, F.; Maffulli, N.; Galanti, G. Effects of a home-based exercise rehabilitation program for cancersurvivors. J. Sports Med. Phys. Fit. 2019, 59, 846–852. [Google Scholar] [CrossRef]
- Thompson, P.D.; Arena, R.; Riebe, D.; Pescatello, L.S. American College of Sports Medicine. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription, ninth edition. Curr. Sports Med. Rep 2013, 12, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.D.S.; Barreto Silva, M.I.; da Costa, M.S.; Pontes, K.S.D.S.; Castro, F.G.; Antunes, V.P.; Rosina, K.T.C.; Menna Barreto, A.P.M.; Souza, E.; Klein, M.R.S.T. High abdominal adiposity and low phase angle in overweight renal transplant recipients. Clin. Transplant. 2019, 33, e13654. [Google Scholar] [CrossRef]
- Douglas, P.S.; Garcia, M.J.; Haines, D.E.; Lai, W.W.; Manning, W.J.; Patel, A.R.; Picard, M.H.; Polk, D.M.; Ragosta, M.; Ward, R.P.; et al. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 appropriate use criteria for echocardiography. J. Am. Coll. Cardiol. 2011, 57, 1126–1166. [Google Scholar] [CrossRef]
- Minetti, E.; Riggs, K.; Ingletto, C.; Mascherini, G.; Pedrizzetti, G.; Stefani, L. Changes in global longitudinal strain in renal transplant recipients following 12 months of exercise. Intern. Emerg. Med. 2018, 805–809. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D Speckle tracking echocardiography: Consensus document of the EACVI/ASE/industry task force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef]
- Sofi, F.; Dinu, M.; Pagliai, G.; Marcucci, R.; Casini, A. Validation of a literature-based adherence score to Mediterranean diet: The MEDI-LITE score. Int. J. Food Sci. Nutr. 2017, 68, 757–762. [Google Scholar] [CrossRef]
- Painter, P.; Roshanravan, B. The association of physical activity and physical function with clinical outcomes in adults with chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2013, 22, 615–623. [Google Scholar] [CrossRef]
- Lin, S.Y.; Fetzer, S.J.; Lee, P.C.; Chen, C.H. Predicting adherence to health care recommendations using health promotion behaviors in kidney transplant recipient within 1–5 years post-transplant. J. Clin. Nurs. 2011, 20, 23–24. [Google Scholar] [CrossRef]
- Neale, J.; Smith, A.C.; Bishop, N.C.; Am, J. Effects of Exercise and Sport in Solid Organ Transplant Recipients: A Review. Phys. Med. Rehabil. 2017, 96, 273–288. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, T.; Hathaway, D. An Integrative Literature Review of Physical Activity Recommendations for Adult Renal Transplant Recipients. Prog. Transpl. 2016, 26, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Svensson, M.; Jardine, A.; Fellström, B.; Holdaas, H. Prevention of cardiovascular disease after renal transplantation. Organ. Transplant. 2012, 17, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, F.; Mallamaci, F.; D’Arrigo, G.; Baggetta, R.; Bolignano, D.; Torino, C.; Lamberti, N.; Bertoli, S.; Ciurlino, D.; Rocca-Rey, L.; et al. Exercise in Patients on Dialysis: A Multicenter, Randomized Clinical Trial. J. Am. Soc. Nephrol. 2017, 28, 1259–1268. [Google Scholar] [CrossRef]
- Calella, P.; Hernández-Sánchez, S.; Garofalo, C.; Ruiz, J.R.; Carrero, J.; Bellizzi, V.J. Exercise training in kidney transplant recipients: A systematic review. J. Nephrol. 2019, 32, 567–579. [Google Scholar] [CrossRef]
- Raymond, J.; Johnson, S.T.; Diehl-Jones, W.; Vallance, J.K. Walking, Sedentary Time and Health-Related Quality of Life Among Kidney Transplant Recipients: An Exploratory Study. Transpl. Proceed. 2016, 48, 59e64. [Google Scholar] [CrossRef]
- Gordon, E.J.; Prohaska, T.R.; Gallant, M.; Sminoff, L.A. Self-care strategies and barriers among kidney transplant recipients: A qualitative study. Chronic Illn. 2009, 5, 75–91. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| T0 | T6 | T12 | ΔT0-T6 | ΔT6–T12 | ANOVA | |
|---|---|---|---|---|---|---|
| Weight (kg) | 71.8 ± 14.8 | 70.8 ± 14.3 | 70.6 ± 14.7 * | 1.0 (95% CI: −8.0, 6.0) | −0.2 (95% CI: −6.6, 7.0) | <0.05 |
| Waist Circumference (cm) | 89.4 ± 12.5 | 89.1 ± 12.5 | 88.6 ± 11.4 * | −0.3 (95% CI: 6.3, 5.7) | −0.5 (95% CI: −6.7, 4.7) | <0.05 |
| Biceps Skinfold (mm) | 8.2 ± 3.9 | 6.9 ± 3.5 * | 6.9 ± 3.3 | 1.3 (95% CI: −05.0, 3.1) | 0.0 (95% CI: −0.1, 0.1) | <0.05 |
| Triceps Skinfold (mm) | 13.5 ± 3.7 | 13.6 ± 5.8 | 11.8 ± 5.1 * | 0.1 (95% CI: −2.2, 2.4) | 2.0 (95% CI: −0.6, 6.0) | <0.05 |
| BMI kg/m2 | 24.4 ± 2.2 | 24.2 ± 3.3 | 24.2 ± 3.1 | −0.2 (95% CI: −1.5, 1.5) | 0.0 (95% CI: −1.5, 1.5) | 0.88 |
| HG right(kg) | 32.2 ± 9.6 | 33.8 ± 10.9 | 33.9 ±10.8 | −1.6 (95% CI: −6.4, 3.2) | 0.1 (95% CI: −5.0, 5.2) | 0.65 |
| HG left (kg) | 33.1 ± 10.4 | 34.6 ± 11.2 | 35.7 ± 11.3 * | 1.5 (95% CI: −3.6, 6.6) | 1.1 (95% CI: −4.1, 6.3) | <0.05 |
| TBW (%) | 41.1 ± 9.2 | 40.6 ± 2.3 | 40.4 ± 4.2 | −0.5 (95% CI: −2.2, 3.2) | −0.2 (95% CI: −1.3, 1.7) | 0.58 |
| ICW (%) | 20.5 ± 5.0 | 20.3 ± 4.9 | 20.3 ± 5.4 | −0.2 (95% CI: −2.1, 2.5) | 0.0 (95% CI: −2.2, 2.6) | 0.55 |
| ECW (%) | 23.3 ± 2.6 | 20 ± 4.5 | 20.5 ± 5.0 | −2.9 (95% CI: −4.6, −1.2) | −0.5 (95% CI: −7.2, −2.8) | 0.69 |
| T0 | T6 | T12 | Δ T0–T6 | Δ T6–T12 | ANOVA | |
|---|---|---|---|---|---|---|
| LVDD | 50 ± 2.7 | 49.7 ± 2.9 | 50 ± 2.6 | −0.5 (95% CI: −1.5, 0.5) | 0.5 (95% CI: 0.6, 0.4) | 0.74 |
| LVSD | 27.8 ± 2.7 | 28.1 ± 3.9 | 28.2 ± 2.4 | −0.3 (95% CI: −1.8, 1.2) | 0.1 (95% CI: −1.4, 1.6) | 0.57 |
| EF | 63.4 ± 3.4 | 62.2 ± 4.4 | 64.4 ± 4.5 | −1.3 (95% CI: −3.1, 0.5) | −2.2 (95% CI: −4.0, −0.4) | 0.53 |
| E/A | 1.14 ± 0.3 | 1.15 ± 0.5 | 1.12 ± 0.6 | 0.01 (95% CI: −0.2, 0.2) | −0.03 (95% CI: −0.2, 0.3) | 0.57 |
| MEDI- LITE T0 | MEDI- LITE T6 | |
|---|---|---|
| Mean | 11,500 | 11,700 |
| Standard Deviation | 19,003 | 30,569 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlandi, G.; Sofi, F.; Moscarelli, L.; Cirami, L.; Mancini, S.; Stefani, L. Exercise Prescription in Renal Transplant Recipients: From Sports Medicine Toward Multidisciplinary Aspects: A Pilot Study. J. Funct. Morphol. Kinesiol. 2020, 5, 10. https://doi.org/10.3390/jfmk5010010
Orlandi G, Sofi F, Moscarelli L, Cirami L, Mancini S, Stefani L. Exercise Prescription in Renal Transplant Recipients: From Sports Medicine Toward Multidisciplinary Aspects: A Pilot Study. Journal of Functional Morphology and Kinesiology. 2020; 5(1):10. https://doi.org/10.3390/jfmk5010010
Chicago/Turabian StyleOrlandi, Goffredo, Francesco Sofi, Luciano Moscarelli, Lino Cirami, Sabrina Mancini, and Laura Stefani. 2020. "Exercise Prescription in Renal Transplant Recipients: From Sports Medicine Toward Multidisciplinary Aspects: A Pilot Study" Journal of Functional Morphology and Kinesiology 5, no. 1: 10. https://doi.org/10.3390/jfmk5010010
APA StyleOrlandi, G., Sofi, F., Moscarelli, L., Cirami, L., Mancini, S., & Stefani, L. (2020). Exercise Prescription in Renal Transplant Recipients: From Sports Medicine Toward Multidisciplinary Aspects: A Pilot Study. Journal of Functional Morphology and Kinesiology, 5(1), 10. https://doi.org/10.3390/jfmk5010010