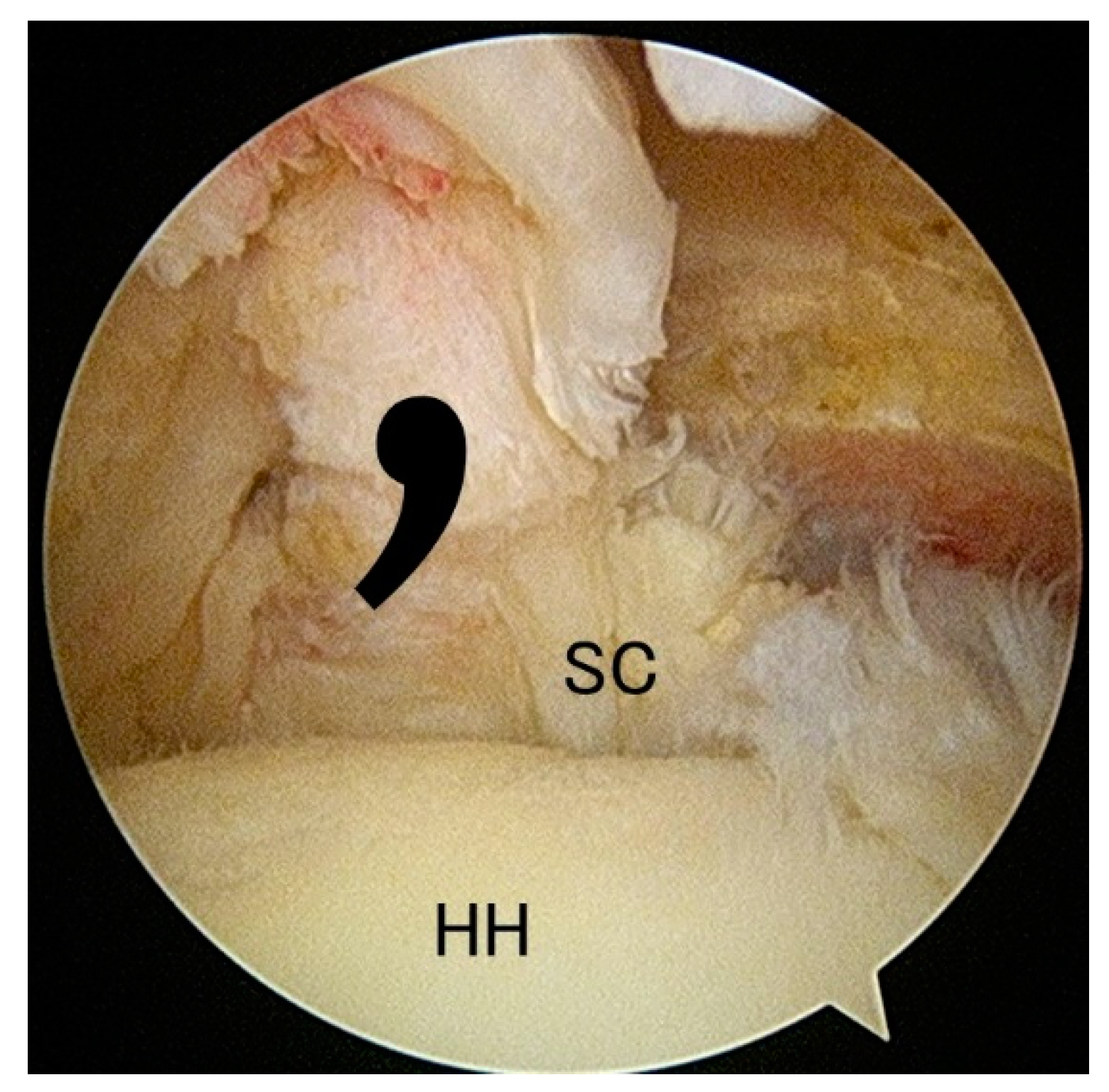
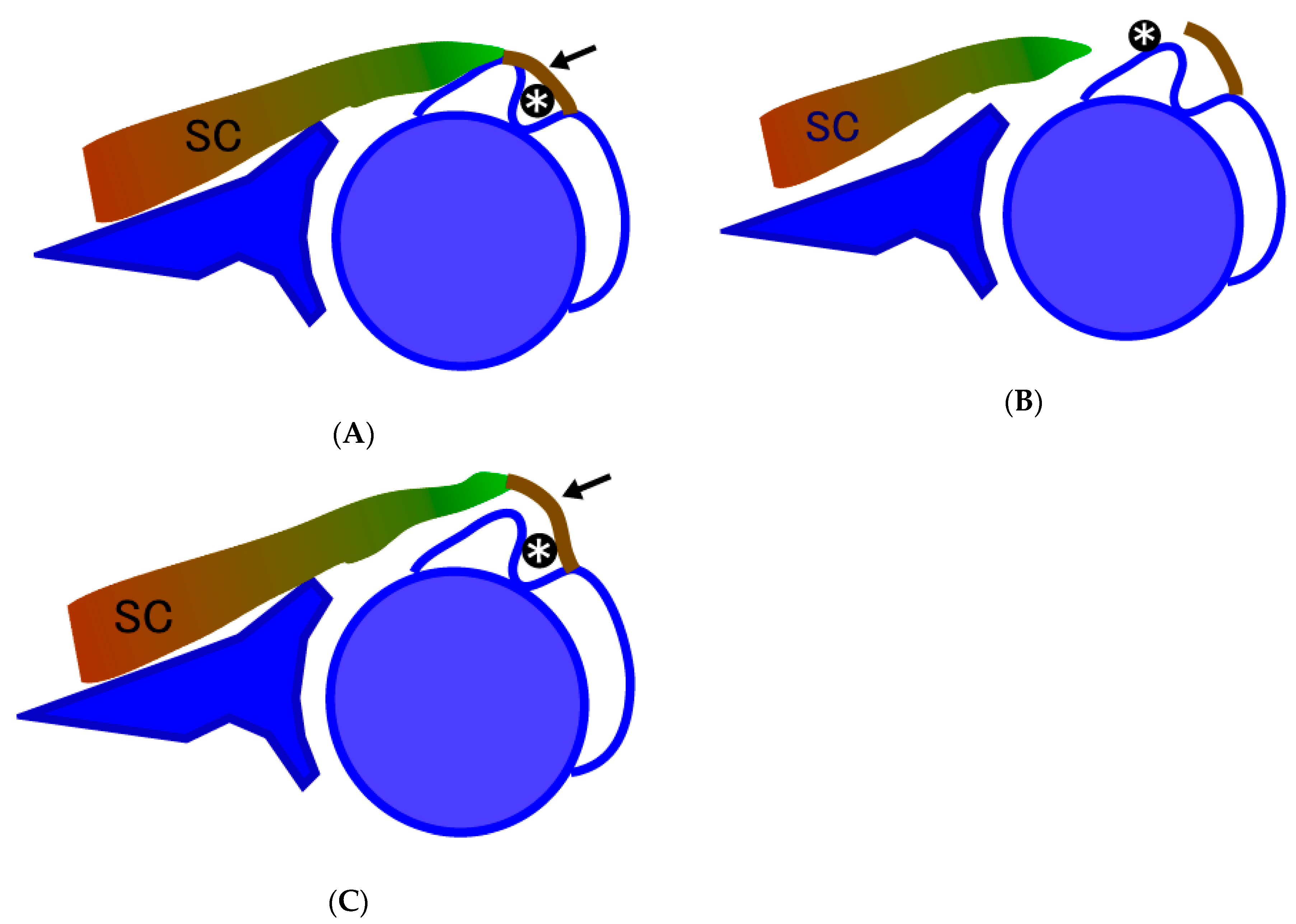
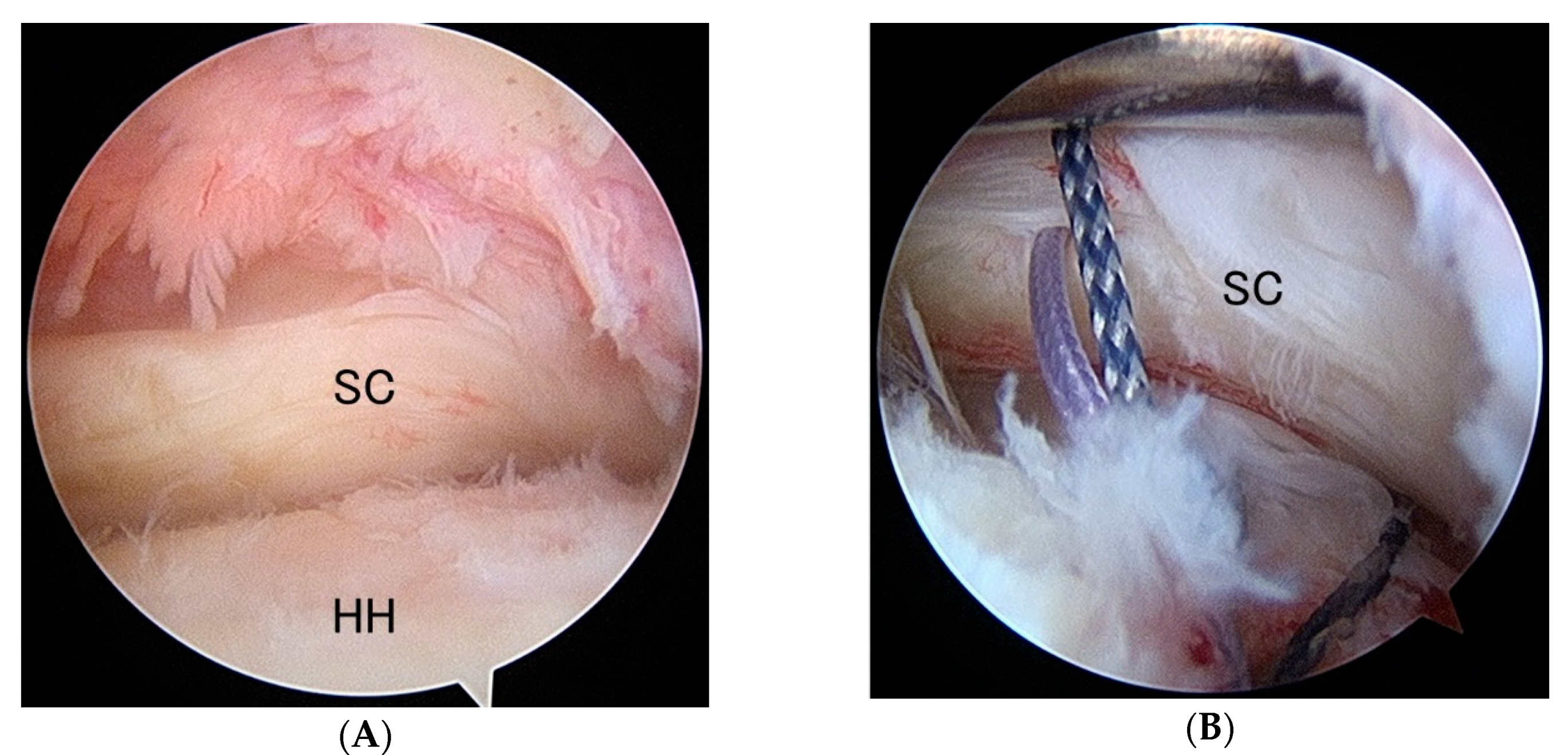
Floating Subscapularis Tear: A Variation of the Partial Subscapularis Tear


Abstract
1. Introduction
2. Materials and Methods
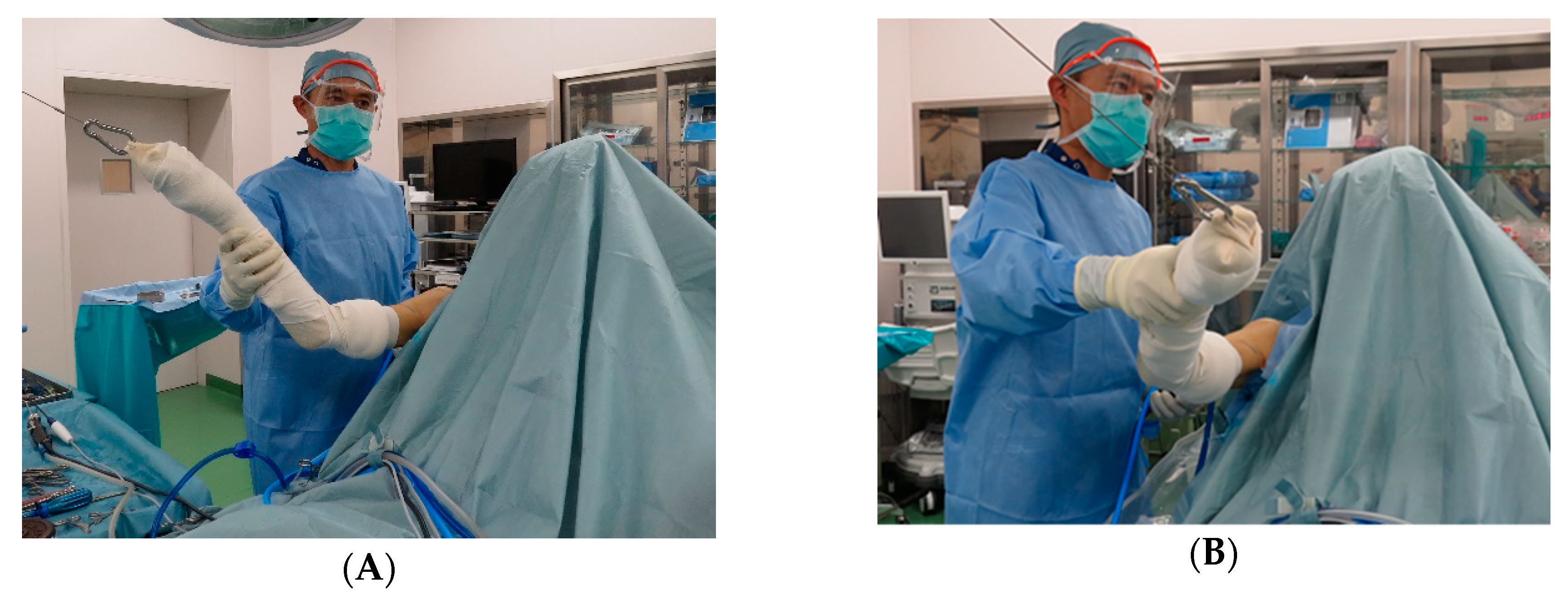
Surgical Technique
3. Results
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Clark, J.M.; Harryman, D.T. Tendons, ligaments, and capsule of the rotator cuff. Gross and microscopic anatomy. J. Bone Joint Surg. 1992, 74, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Richards, D.P.; Burkhart, S.S.; Tehrany, A.M.; Wirth, M.A. The subscapularis footprint: An anatomic description of its insertion site. Arthroscopy 2007, 23, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Arai, R.; Sugaya, H.; Mochizuki, T.; Nimura, A.; Moriishi, J.; Akita, K. Subscapularis tendon tear: an anatomic and clinical investigation. Arthroscopy 2008, 24, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Bennett, W.F. Subscapularis, medial, and lateral head coracohumeral ligament insertion anatomy. Arthroscopic appearance and incidence of "hidden" rotator interval lesions. Arthroscopy 2001, 17, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Barth, J.R.; Burkhart, S.S.; De Beer, J.F. The bear-hug test: A new and sensitive test for diagnosing a subscapularis tear. Arthroscopy 2006, 22, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Lenart, B.A.; Ticker, J.B. Subscapularis tendon tears: Management and arthroscopic repair. EFORT Open Rev. 2017, 2, 484–495. [Google Scholar] [CrossRef] [PubMed]
- Lo, I.K.; Burkhart, S.S. The comma sign: An arthroscopic guide to the torn subscapularis tendon. Arthroscopy 2003, 19, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Lafosse, L.; Jost, B.; Reiland, Y.; Audebert, S.; Toussaint, B.; Gobezie, R. Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears. J. Bone Joint Surg. Am. 2007, 89, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Garavaglia, G.; Ufenast, H.; Taverna, E. The frequency of subscapularis tears in arthroscopic rotator cuff repairs: A retrospective study comparing magnetic resonance imaging and arthroscopic findings. Int. J. Shoulder Surg. 2011, 5, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Walch, G.; Nove-Josserand, L.; Levigne, C.; Renaud, E. Tears of the supraspinatus tendon associated with “hidden” lesions of the rotator interval. J. Shoulder Elbow Surg. 1994, 3, 353–360. [Google Scholar] [CrossRef]
- Yoo, J.C.; Rhee, Y.G.; Shin, S.J.; Park, Y.B.; McGarry, M.H.; Jun, B.J.; Lee, T.Q. Subscapularis tendon tear classification based on 3-dimensional anatomic footprint: a cadaveric and prospective clinical observational study. Arthroscopy. 2015, 31, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Neyton, L.; Daggett, M.; Kruse, K.; Walch, G. The Hidden Lesion of the Subscapularis: Arthroscopically Revisited. Arthrosc Tech. 2016, 5, e877–e881. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Singh, R.; Singla, M.; Tubbs, R.S. Macro/micro observational studies of fibres maintaining the biceps brachii tendon in the bicipital groove: application to surgery, pathology and kinesiology. Folia Morphol (Warsz). 2015, 74, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Tebaa, E.; Tantot, J.; Isaac-Pinet, S.; Nové-Josserand, L. Histologic characteristics of the subscapularis tendon from muscle to bone: reference to subscapularis lesions. J. Shoulder. Elbow. Surg. 2019, 28, 959–965. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable * | |||
|---|---|---|---|
| Age, y | 66.3 (7.6) | ||
| Gender | |||
| Male | 22 | ||
| Female | 11 | ||
| Dominant side | 59% | ||
| ROM (active) | |||
| Forward flexion, ° | 122 (43) | 0 to 170 | |
| ER at side, ° | 49 (21) | 10 to 80 | |
| UCLA score | 17.3 (4.8) | 5 to 25 | |
| VAS (pain), mm | 65 (19) | ||
| Associated cuff tears | |||
| Partial tear of the supraspinatus | 4 | ||
| Full-thickness tear of surpaspinatus | 11 | ||
| Full-thickness tear of surpaspinatus and infraspinatus | 10 | ||
| Status of the long head of biceps tendon | |||
| normal | 3 | ||
| hypertrophy | 2 | ||
| Partial tear | 6 | ||
| full tear | 9 | ||
| subluxation | 7 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamakado, K. Floating Subscapularis Tear: A Variation of the Partial Subscapularis Tear. J. Funct. Morphol. Kinesiol. 2020, 5, 11. https://doi.org/10.3390/jfmk5010011
Yamakado K. Floating Subscapularis Tear: A Variation of the Partial Subscapularis Tear. Journal of Functional Morphology and Kinesiology. 2020; 5(1):11. https://doi.org/10.3390/jfmk5010011
Chicago/Turabian StyleYamakado, Kotaro. 2020. "Floating Subscapularis Tear: A Variation of the Partial Subscapularis Tear" Journal of Functional Morphology and Kinesiology 5, no. 1: 11. https://doi.org/10.3390/jfmk5010011
APA StyleYamakado, K. (2020). Floating Subscapularis Tear: A Variation of the Partial Subscapularis Tear. Journal of Functional Morphology and Kinesiology, 5(1), 11. https://doi.org/10.3390/jfmk5010011