
Effectiveness of Physical Exercise on Indicators of Metabolic Syndrome in Adults: A Systematic Review with Meta-Analysis of Clinical Trials

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Selection Criteria
2.3. Data Extraction
2.4. Methodological Quality
2.5. Statistical Analysis
3. Results
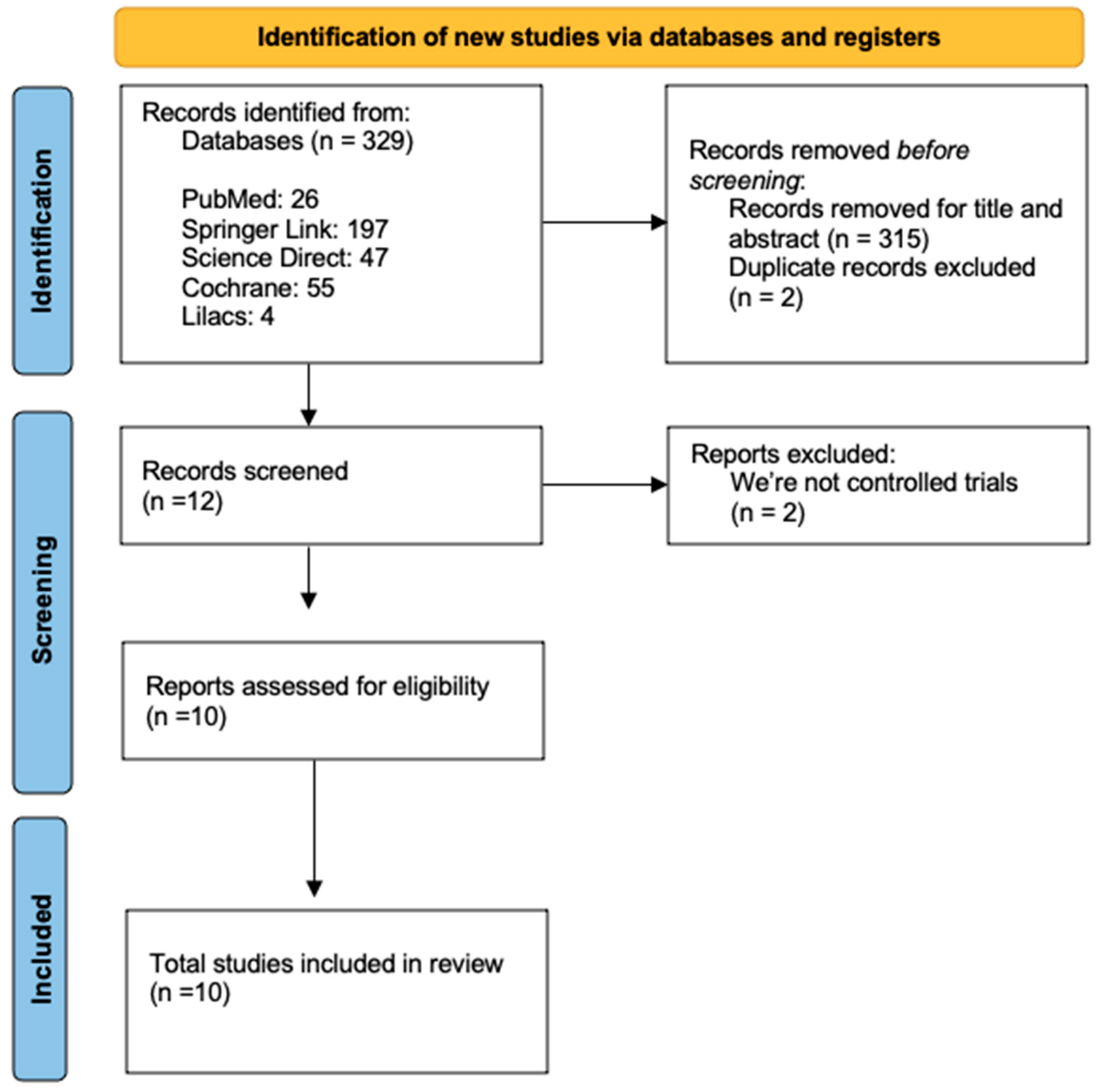
3.1. Search Results
3.2. Characteristics of the Selected Studies
3.2.1. Results of Methodological Quality
3.2.2. Characteristics of the Included Studies
3.2.3. Characteristics of Exercise Programs
3.3. Effects of Exercise on Indicators of Metabolic Syndrome
- Total cholesterol
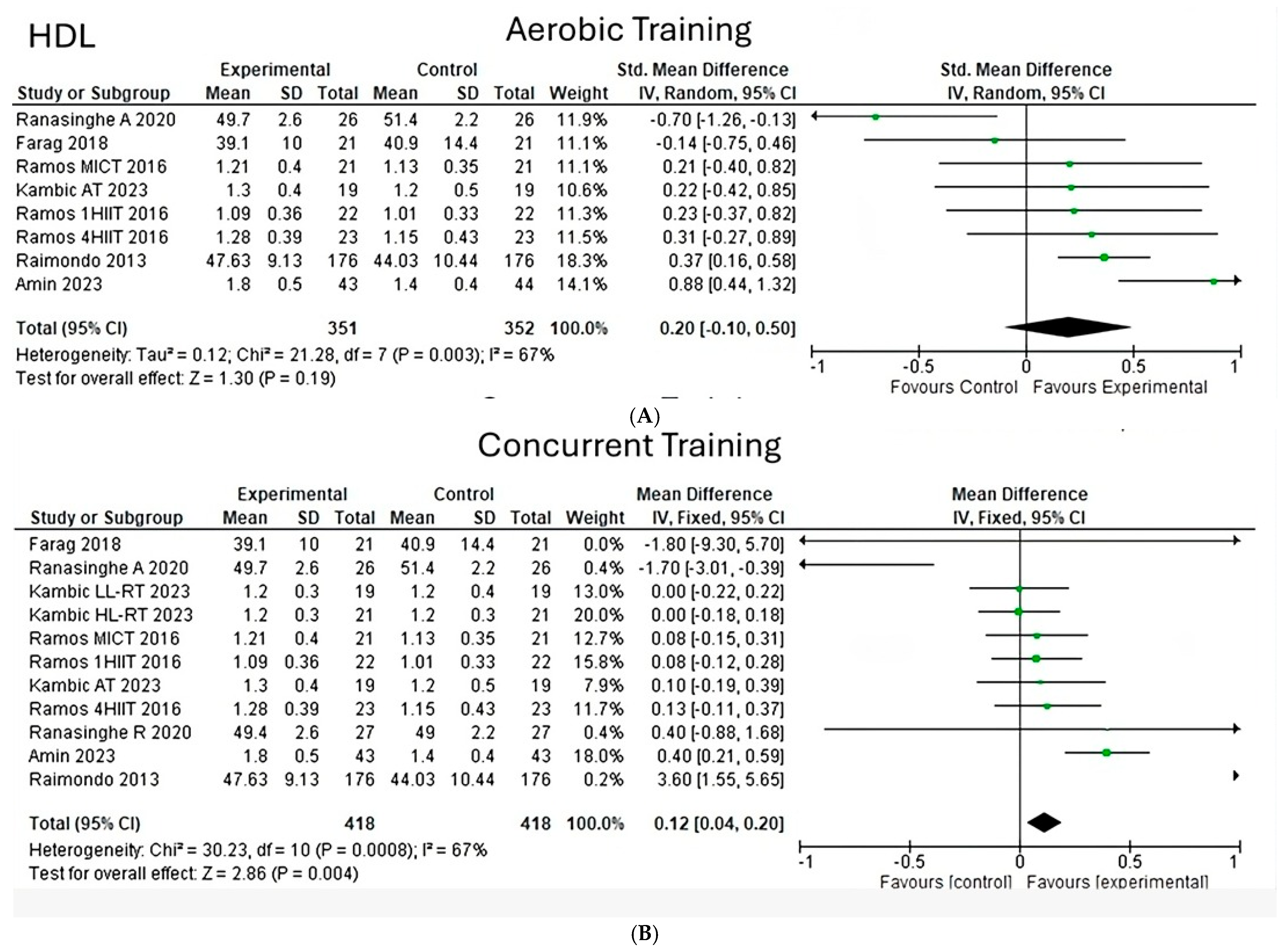
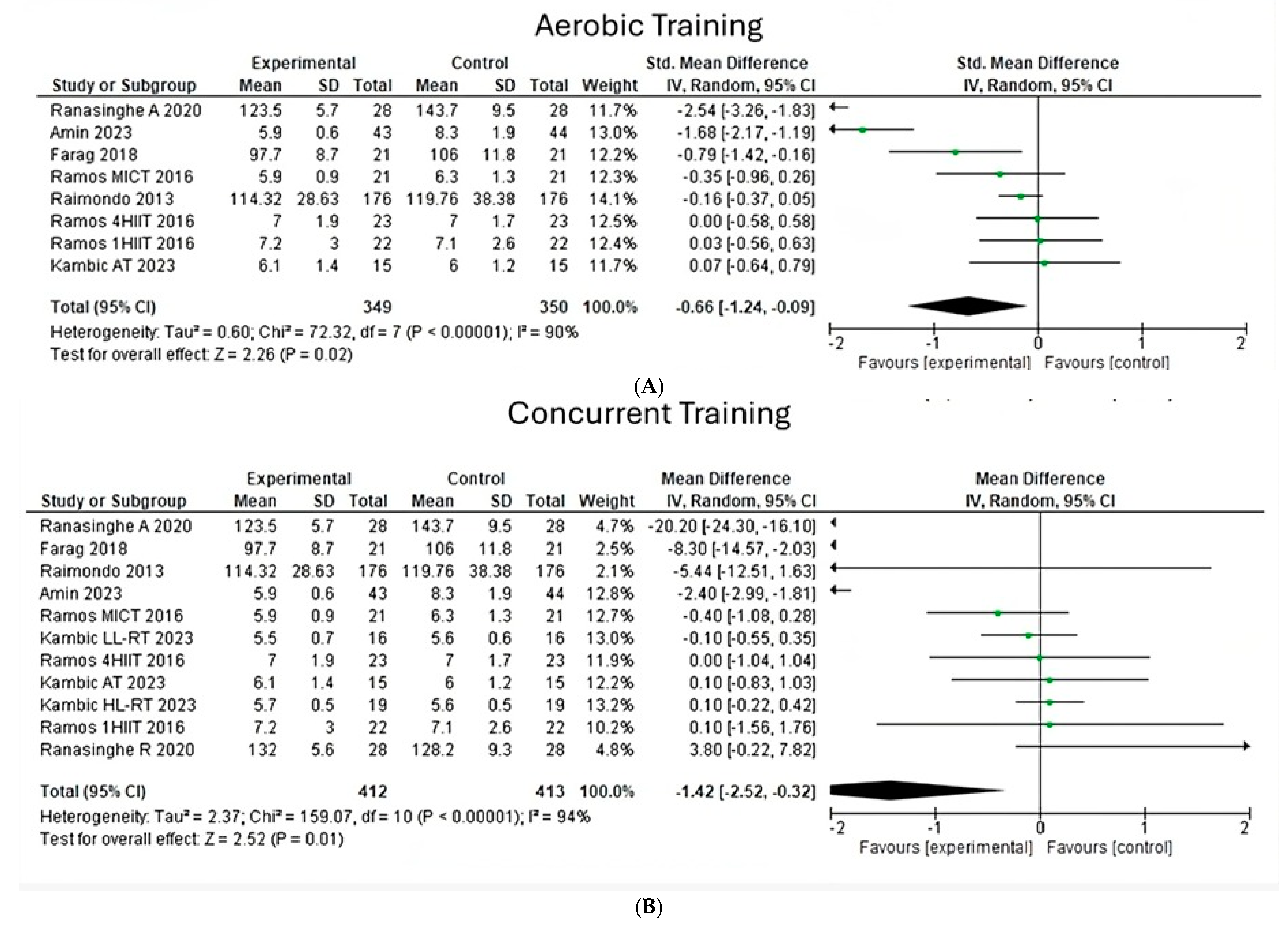
- Low- and high-density lipoprotein
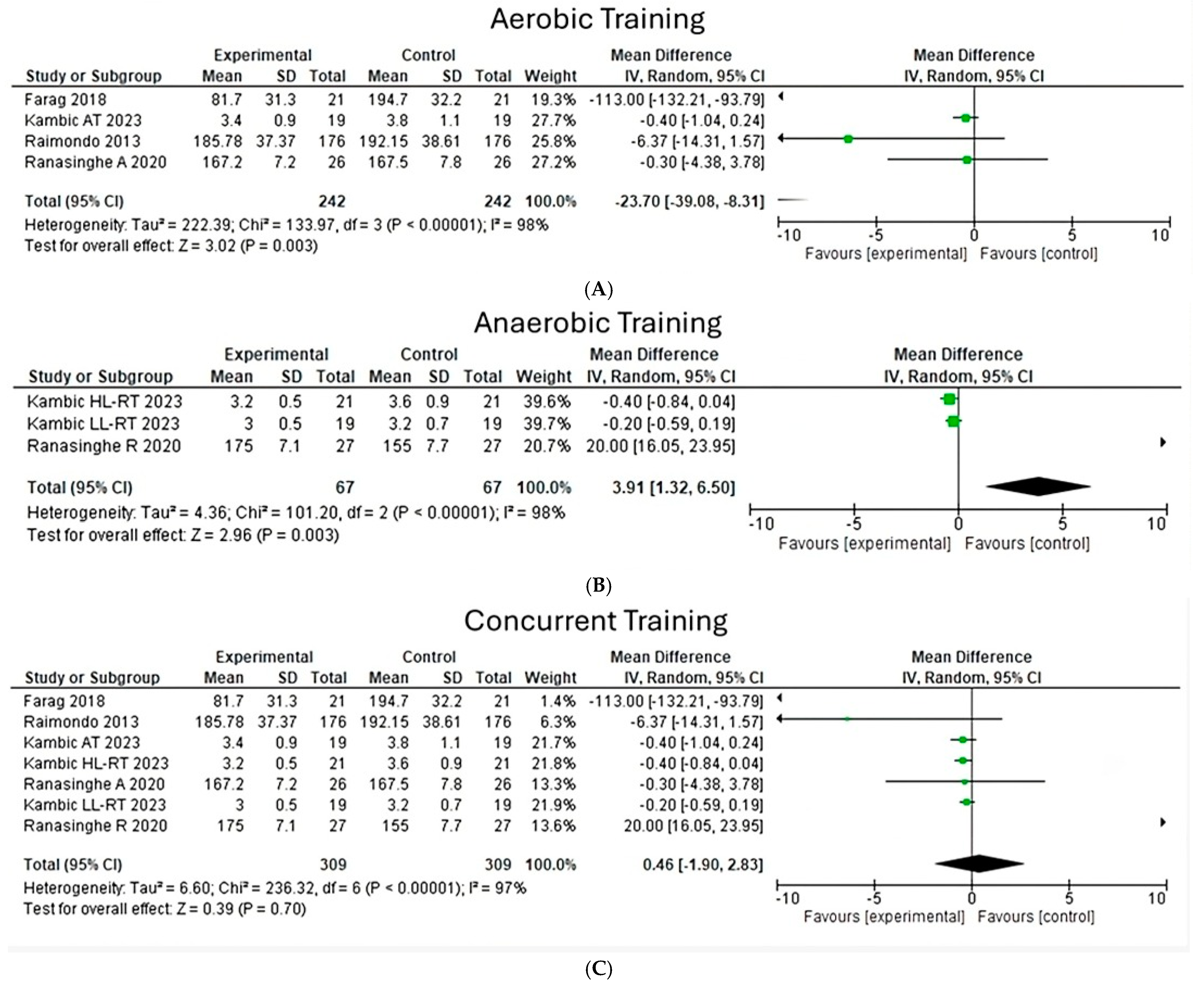
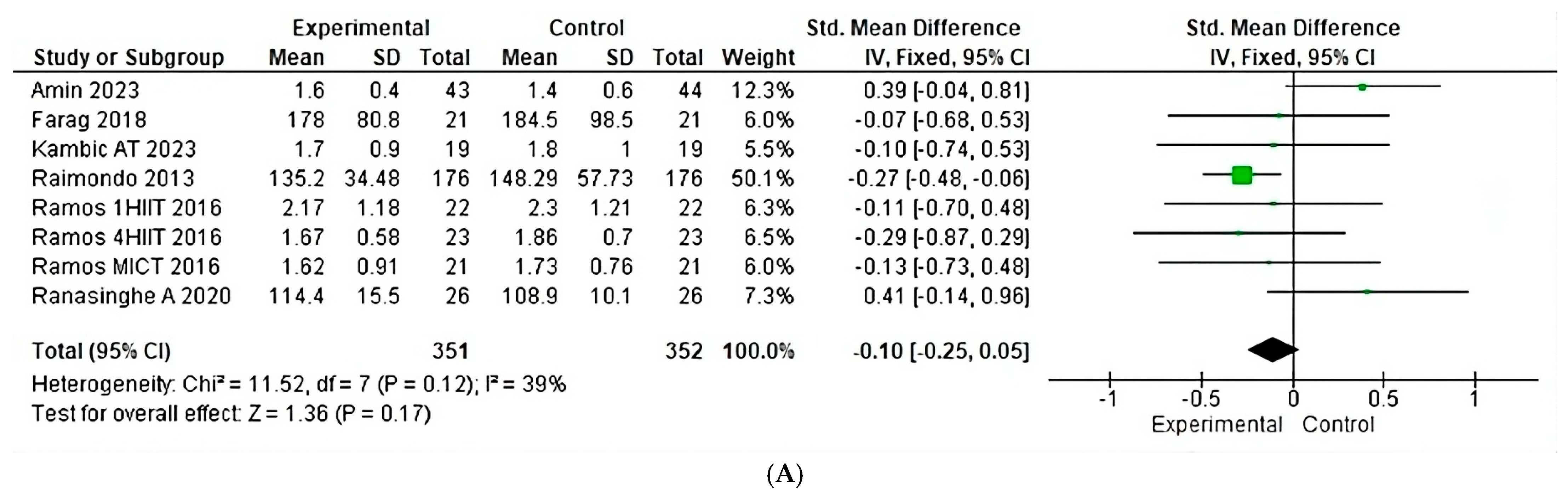
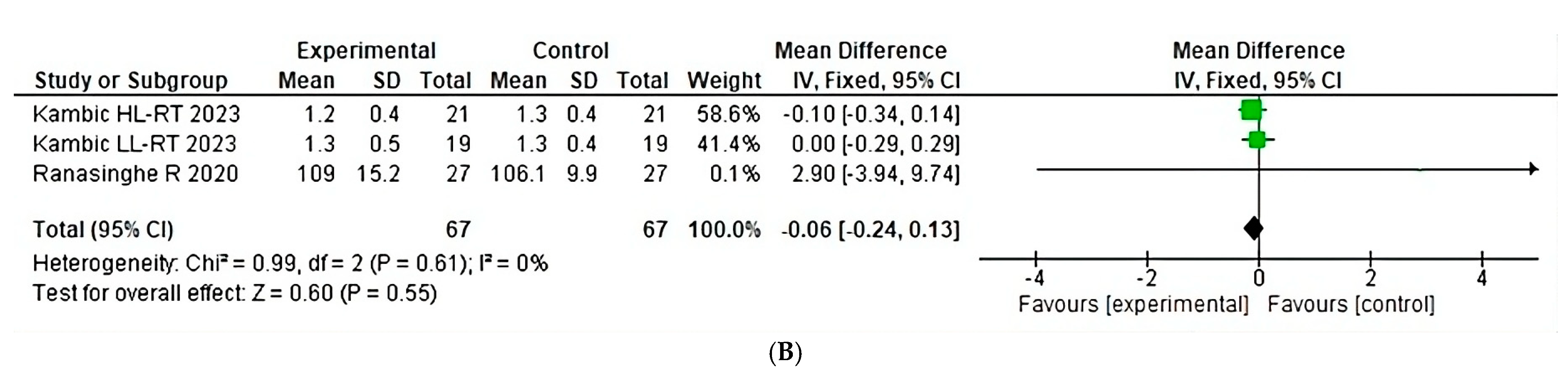
- Fasting blood glucose
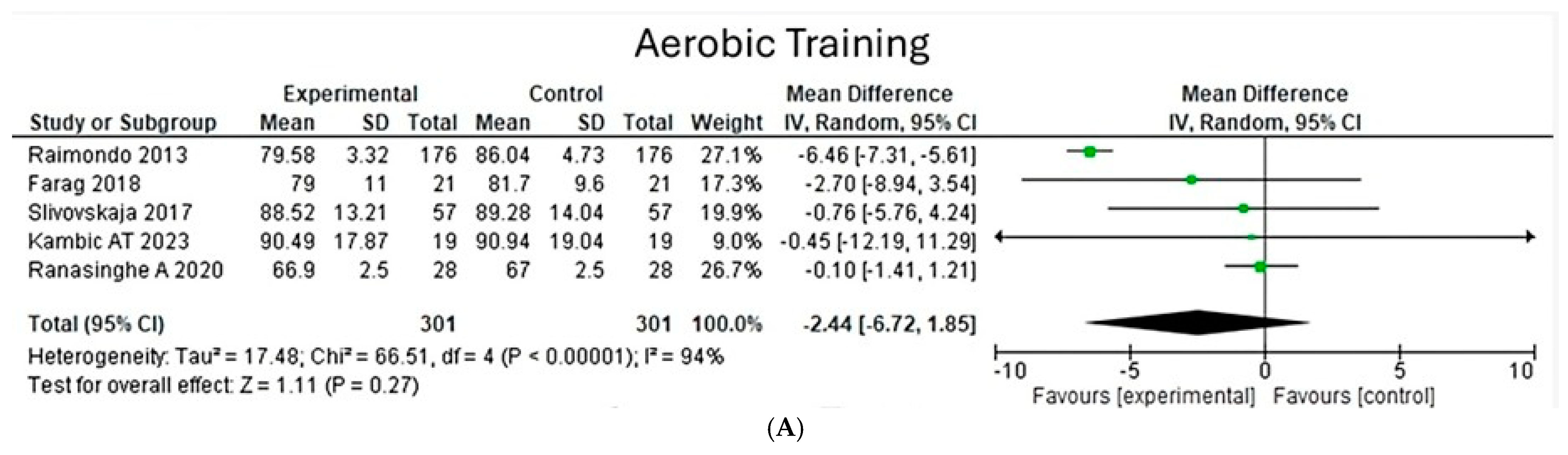
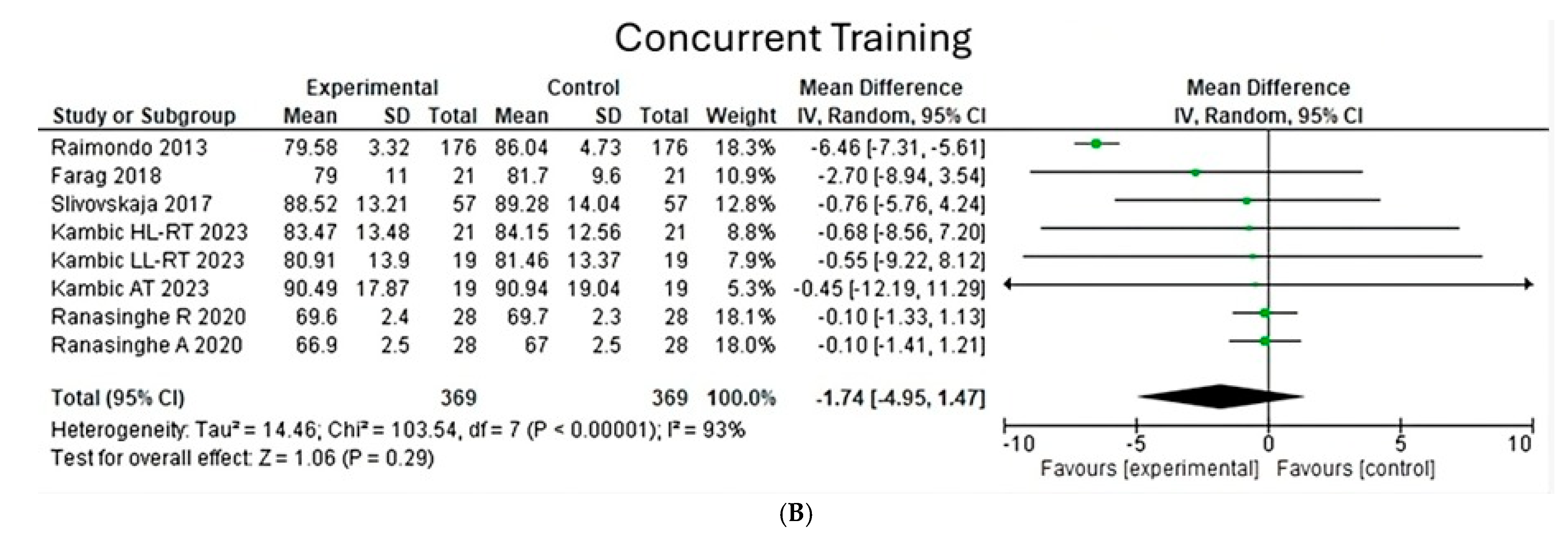
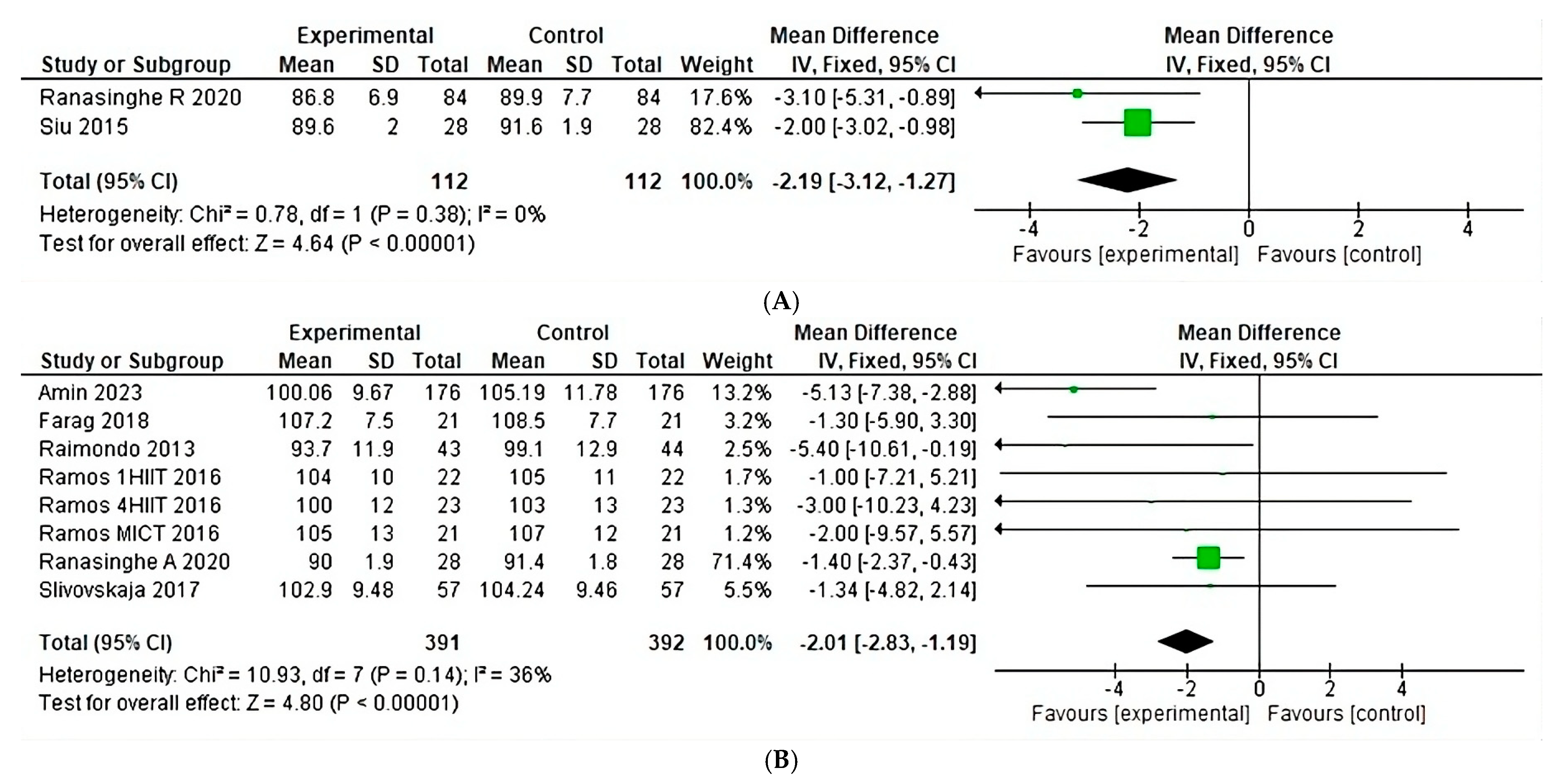
- Diastolic blood pressure
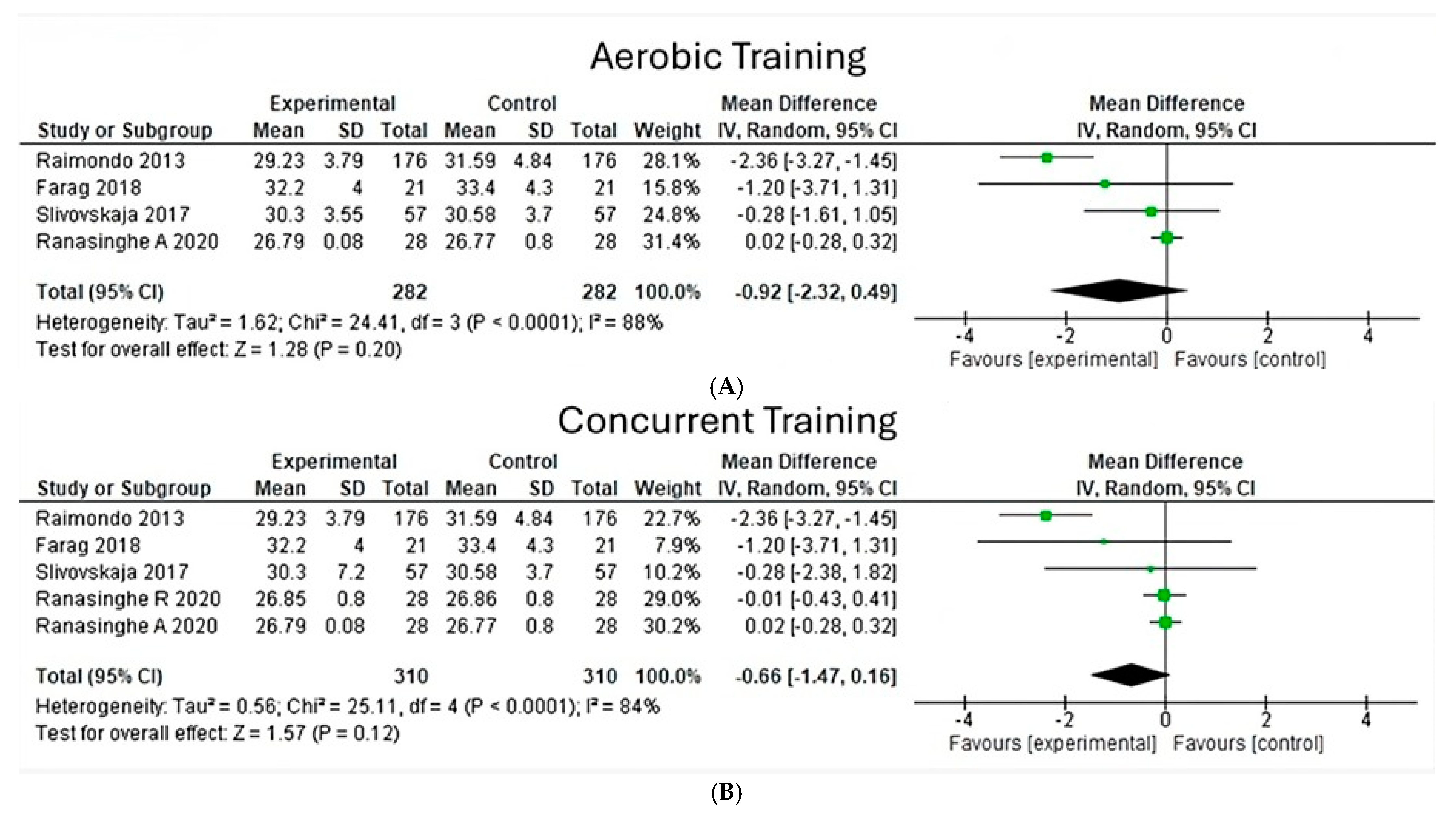
- Body mass index
- Total body weight
- Indicators unchanged
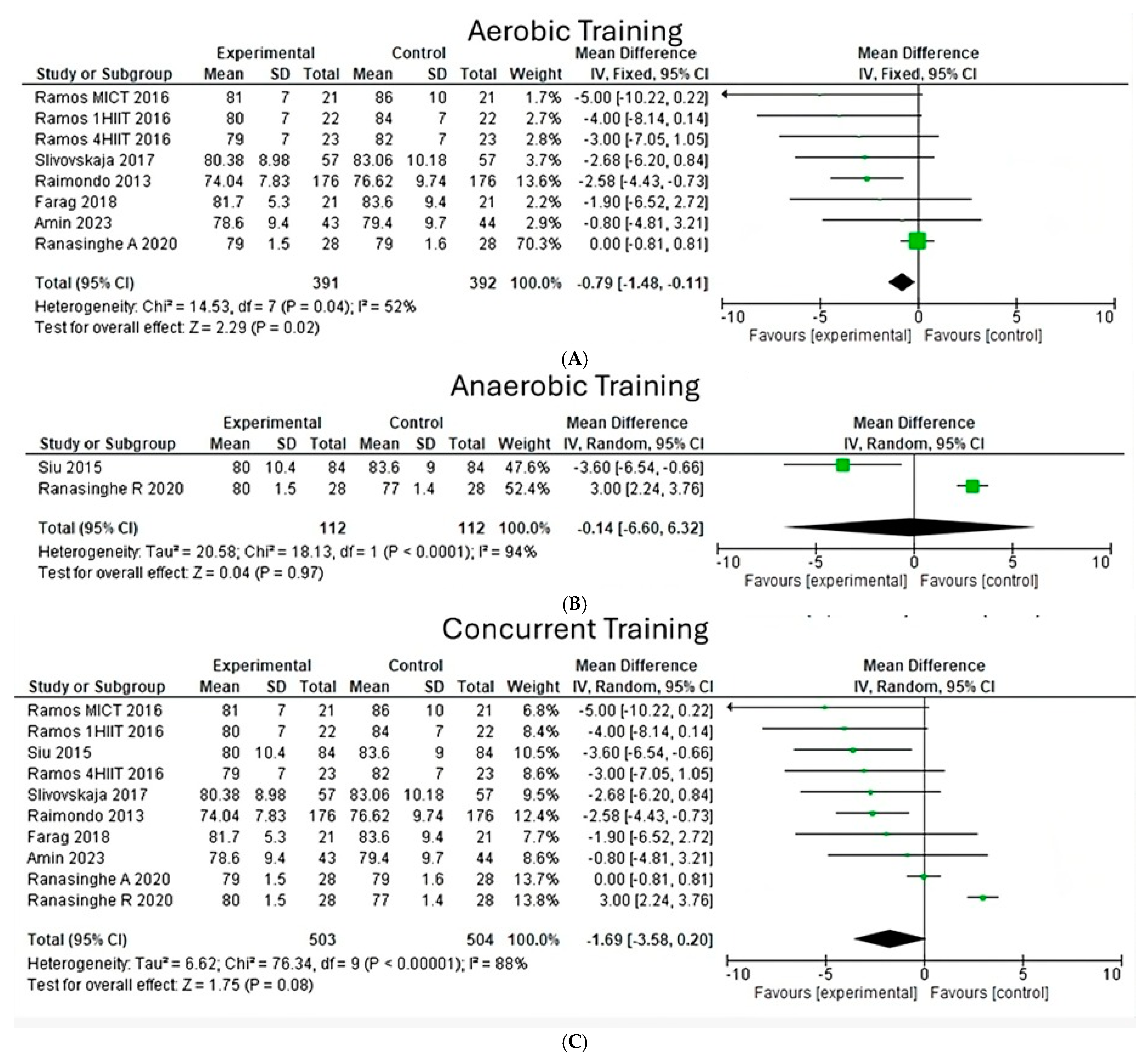
- Systolic blood pressure
- Waist circumference
- Triglycerides
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MetS | Metabolic syndrome |
| T2DM | Type 2 diabetes mellitus |
| HDL | High-density lipoprotein |
| LDL | Low-density lipoprotein |
| CVD | Cardiovascular disease |
| GDP | Gross domestic product |
| PEDro | Physiotherapy evidence database |
| WMD | Weighted mean difference |
| CI | Confidence interval |
| FITT | Frequency, intensity, type, time |
| HIIT | High-intensity interval training |
| HRpeak | High-rate peak |
| CAD | Coronary artery disease |
| BW | Body weight |
| BM | Body mass |
| BMI | Body mass index |
| WC | Waist circumference |
| SBP | Systolic blood pressure |
| DBP | Diastolic blood pressure |
| BP | Blood pressure |
| TG | Triglycerides |
| FBS | Fasting blood sugar |
References
- Carvajal Carvajal, C. Síndrome metabólico: Definiciones, epidemiología, etiología, componentes y tratamiento. Med. Leg. Costa Rica 2017, 34, 175–193. [Google Scholar]
- WHO. Definition, Diagnosis, and Classification of Diabetes Mellitus and Its Complications; WHO: Geneva, Switzerland, 1999. [Google Scholar]
- Carson, C.; Lawson, H.A. Epigenetics of metabolic syndrome. Physiol. Genom. 2018, 50, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, P.M.; Tuomilehto, J.; Rydén, L. The metabolic syndrome–What is it and how should it be managed? Eur. J. Prev. Cardiol. 2019, 26 (Suppl. 2), 33–46. [Google Scholar] [CrossRef]
- Rodríguez, A.V.; Luján, R.C.; del Castillo, L.A.E.; López, S.A.R.; Legleu, C.E.C. Efecto del ejercicio físico sobre la concentración de adipocinas en adultos con obesidad. Una revisión sistemática. Mov. Científico 2019, 13, 27–36. [Google Scholar]
- Gutiérrez-Solis, A.L.; Datta Banik, S.; Méndez-González, R.M. Prevalence of metabolic syndrome in Mexico: A systematic review and meta-analysis. Metab. Syndr. Relat. Disord. 2018, 16, 395–405. [Google Scholar] [CrossRef]
- Baxriddinovna, R.D. Metabolic Syndrome and Pharmacoeconomy. Eur. J. Innov. Non-Formal Educ. 2023, 3, 69–74. [Google Scholar]
- Saklayen, M.G. The global epidemic of the metabolic syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Ortiz-Rodríguez, M.A.; Bautista-Ortiz, L.F.; Villa, A.R.; Antúnez-Bautista, P.K.; Aldaz-Rodríguez, M.V.; Estrada-Luna, D.; Denova-Gutierrez, E.; Camacho-Diaz, B.H.; Martinez-Salazar, M.F. Prevalence of metabolic syndrome among Mexican adults. Metab. Syndr. Relat. Disord. 2022, 20, 264–272. [Google Scholar]
- Babaei, P.; Hoseini, R. Exercise training modulates adipokine dysregulations in metabolic syndrome. Sports Med. Health Sci. 2022, 4, 18–28. [Google Scholar] [CrossRef]
- Vechin, F.C.; Conceição, M.S.; Telles, G.D.; Libardi, C.A.; Ugrinowitsch, C. Interference phenomenon with concurrent strength and high-intensity interval training-based aerobic training: An updated model. Sports Med. 2021, 51, 599–605. [Google Scholar] [CrossRef]
- Oh, S.; So, R.; Shida, T.; Matsuo, T.; Kim, B.; Akiyama, K.; Isobe, T.; Okamoto, Y.; Tanaka, K.; Shoda, J. High-intensity aerobic exercise improves both hepatic fat content and stiffness in sedentary obese men with nonalcoholic fatty liver disease. Sci. Rep. 2017, 7, 43029. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.A.; Thom, J.M.; Rye, K.A.; Parmenter, B.J. Aerobic, resistance or combined training: A systematic review and meta-analysis of exercise to reduce cardiovascular risk in adults with metabolic syndrome. Atherosclerosis 2018, 274, 162–171. [Google Scholar] [CrossRef]
- Liang, M.; Pan, Y.; Zhong, T.; Zeng, Y.; Cheng, A.S. Effects of aerobic, resistance, and combined exercise on metabolic syndrome parameters and cardiovascular risk factors: A systematic review and network meta-analysis. Rev. Cardiovasc. Med. 2021, 22, 1523–1533. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Lozano, D.L.; Camarillo-Nava, V.M.; Juárez-Zepeda, T.E.; Andrade-Pineda, J.E.; Pérez-López, D.; Reyes-Pacheco, J.A.; Lucho-Gutiérrez, Z.M.; Carmona-Aparicio, L. Costo-efectividad del tratamiento de la diabetes mellitus tipo 2 en México. Rev. Méd. Inst. Mex. Seguro Soc. 2023, 61, 172. [Google Scholar]
- Gasca-Pineda, R.; Osorio-Hernández, M.; Mehta, R.; Escobedo-de-la-Peña, J.; Narváez-Oriani, C.A. Carga económica de la hipercolesterolemia en población con alto riesgo cardiovascular en México. Arch. Cardiol. Mex. 2023, 93, 328–335. [Google Scholar] [CrossRef]
- INEGI. Comunicado de Prensa. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/boletines/2024/MOPRADEF/MOPRADEF2023.pdf (accessed on 25 January 2024).
- Murillo-Bonilla, L.M. México Rumbo al 2050 en Salud. Rev. Med. Clín. 2022, 6, e15092206019. [Google Scholar]
- Gómez-Conesa, A. Escala PEDro-Español; Asociación Española de Fisioterapeutas y Unidad de Metaanálisis de la Universidad de Murcia Actualizado: Murcia, Spain, 2012. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2021. [Google Scholar]
- Moravcová, K.; Karbanová, M.; Bretschneider, M.P.; Sovová, M.; Ožana, J.; Sovová, E. Comparing digital therapeutic intervention with an intensive obesity management program: Randomized controlled trial. Nutrients 2022, 14, 2005. [Google Scholar] [CrossRef]
- Slivovskaja, I.; Buzinskaitė, J.; Ryliškytė, L.; Balsytė, J.; Navickas, R.; Puronaitė, R.; Jucevičienė, A.; Juocevičius, A.; Laucevičius, A. Positive impact of a 4-week duration supervised aerobic training on anthropometric, metabolic, hemodynamic and arterial wall parameters in metabolic syndrome subjects. Semin. Cardiovasc. Med. 2017, 23, 11–16. [Google Scholar] [CrossRef]
- Siu, P.M.; Yu, A.P.; Benzie, I.F.; Woo, J. Effects of 1-year yoga on cardiovascular risk factors in middle-aged and older adults with metabolic syndrome: A randomized trial. Diabetol. Metab. Syndr. 2015, 7, 40. [Google Scholar] [CrossRef]
- Ranasinghe, C.; Devage, S.; Constantine, G.R.; Katulanda, P.; Hills, A.P.; King, N.A. Glycemic and cardiometabolic effects of exercise in South Asian Sri Lankans with type 2 diabetes mellitus: A randomized controlled trial Sri Lanka diabetes aerobic and resistance training study (SL-DARTS). Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 77–85. [Google Scholar] [CrossRef]
- Ramos, J.S.; Dalleck, L.C.; Borrani, F.; Mallard, A.R.; Clark, B.; Keating, S.E.; Fassett, R.G.; Coombes, J.S. The effect of different volumes of high-intensity interval training on proinsulin in participants with the metabolic syndrome: A randomized trial. Diabetologia 2016, 59, 2308–2320. [Google Scholar] [CrossRef]
- Di Raimondo, D.; Tuttolomondo, A.; Buttà, C.; Casuccio, A.; Giarrusso, L.; Miceli, G.; Licata, G.; Pinto, A. Metabolic and anti-inflammatory effects of a home-based programme of aerobic physical exercise. Int. J. Clin. Pr. 2013, 67, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Kambic, T.; Božič Mijovski, M.; Jug, B.; Hadžić, V.; Lainscak, M. Insulin resistance, lipids and body composition in patients with coronary artery disease after combined aerobic training and resistance training: A randomized, controlled trial. Diabetol. Metab. Syndr. 2023, 15, 47. [Google Scholar] [CrossRef]
- Farag, H.A.M.; Hosseinzadeh-Attar, M.J.; Muhammad, B.A.; Esmaillzadeh, A.; Bilbeisi, A.H.E. Comparative effects of vitamin D and vitamin C supplementations with and without endurance physical activity on metabolic syndrome patients: A randomized controlled trial. Diabetol. Metab. Syndr. 2018, 10, 80. [Google Scholar] [CrossRef] [PubMed]
- Bönhof, G.J.; Strom, A.; Apostolopoulou, M.; Karusheva, Y.; Sarabhai, T.; Pesta, D.; Roden, M.; Ziegler, D. High-intensity interval training for 12 weeks improves cardiovascular autonomic function but not somatosensory nerve function and structure in overweight men with type 2 diabetes. Diabetologia 2022, 65, 1048–1057. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Kerr, D.; Atiase, Y.; Samir, M.M.; Driscoll, A. Improving metabolic syndrome in Ghanaian adults with type 2 diabetes through a home-based physical activity program: A feasibility randomized controlled trial. Int. J. Environ. Res. Public Health 2023, 20, 5518. [Google Scholar] [CrossRef]
- Balducci, S.; Zanuso, S.; Massarini, M.; Corigliano, G.; Nicolucci, A.; Missori, S.; Italian Diabetes Exercise Study (IDES) Group. The Italian Diabetes and Exercise Study (IDES): Design and methods for a prospective Italian multicentre trial of intensive lifestyle intervention in people with type 2 diabetes and the metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 585–595. [Google Scholar] [CrossRef]
- Smith, J.A.; Murach, K.A.; Dyar, K.A.; Zierath, J.R. Exercise metabolism and adaptation in skeletal muscle. Nat. Rev. Mol. Cell Biol. 2023, 24, 607–632. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cite | Item 1 | Item 2 | Item 4 | Item 8 | Item 9 | Item 10 | Item 11 | Total |
|---|---|---|---|---|---|---|---|---|
| Raimondo et al. (2013) [26] | X | X | X | X | X | 5 | ||
| Sui el al. (2015) [23] | X | X | X | X | X | X | X | 7 |
| Ramos et al. (2016) [25] | X | X | X | X | X | X | 6 | |
| Slivovskaja et al. (2017) [22] | X | X | X | X | 4 | |||
| Farag et al. (2018) [28] | X | X | X | X | X | X | 6 | |
| Ranasinghe et al. (2020) [24] | X | X | X | X | X | X | X | 7 |
| Bönhof et al. (2022) [29] | X | X | X | X | X | 6 | ||
| Moravcová et al. (2022) [21] | X | X | X | X | X | X | 6 | |
| Amin et al. (2023) [30] | X | X | X | X | X | X | 6 | |
| Kambic et al. (2023) [27] | X | X | X | X | X | X | 6 |
| Cite and Location | ID | Objective | Population Characteristics | Exercise Characteristics | Results |
|---|---|---|---|---|---|
| Amin et al., 2023, Ghana [30] | A1 | To determine the effect of a 12-week culturally appropriate home-based physical activity program on metabolic syndrome markers and quality of life in Ghanaian adults with T2DM. | n = 44 Age: 56.5 ± 8.5 years Sex: both genders Pathology: MetS | Program: resistance band Frequency: 3 sessions/week Intensity: brisk pace, 5.2–5.6 km/h Type: aerobic Time: 45 min | =TG -FBG * =HDL -SBP * -DBP -WC * |
| Moravcová et al., 2022, Czech Republic [21] | A2 | This is to evaluate whether the effect of using Vitadio is comparable to that of participating in an intensive individualized weight reduction program administered in person at a specialized clinic. | n = 29 Age: 43 ± 9.5 years Sex: both genders Pathology: obesity, T2DM | Program: Vitadio app Frequency: daily Intensity: 3 months intensive, 3 months sustaining Type: not specified Time: 60 min | -BW * -BMI * -WC * -FBS * -TG * +HDL * =LDL |
| Ramos et al., 2016, Australia [25] | A3 | To investigate the impact of moderate-intensity continuous training and different volumes of HIIT on circulating intact proinsulin concentration. | n = 23 Age: 57 ± 9 years Sex: both genders Pathology: MetS | Program: 1HIIT (16 weeks) Frequency: 3 times/week Intensity: 85–95% HRpeak Type: aerobic Time: 17 min/session | -BW -BMI -WC * =FBS +HDL * -TG -SBP * -DBP |
| Ramos et al., 2016, Australia [25] | A4 | To investigate the impact of moderate-intensity continuous training and different volumes of HIIT on circulating intact proinsulin concentration. | n = 22 Age: 56 ± 10 years Sex: both genders Pathology: MetS | Program: 4HIIT (16 weeks) Frequency: 3 times/week Intensity: 85–95% HRpeak Type: aerobic Time: 38 min/session | -BW -BMI -WC +FBS +HDL -TG -SBP -DBP * |
| Ramos et al., 2016, Australia [25] | A5 | To investigate the impact of moderate-intensity continuous training and different volumes of HIIT on circulating intact proinsulin concentration. | n = 21 Age: 58 ± 7 years Sex: both genders Pathology: MetS | Program: MICT (16 weeks) Frequency: 5 times/week Intensity: 60–70% HRpeak Type: aerobic Time: 30 min/session | -BW =BMI -WC * -FBS +HDL -TG -SBP * -DBP * |
| Raimondo et al., 2013, Italy [26] | A6 | The study was to assess the metabolic and anti-inflammatory effects of a home-based program of fast walking in patients affected by metabolic syndrome. | n = 95 Age: 59.1 ±13.6 years Sex: both genders Pathology: MetS | Program: fast walking Frequency: 5 times/week Intensity: higher than comfortable Type: aerobic Time: 60 min/session | -BW * -WC * -BMI * -FBS * +HDL * -TC * -TG * -SBP * -DBP * |
| Balducci et al., 2008, Italy [31] | A7 | To evaluate the efficacy of an intensive lifestyle intervention on modifiable cardiovascular disease (CVD) risk factors in a large cohort of people with type 2 diabetes and metabolic syndrome | n = 303 Age: 60 ± 6 years Sex: both genders Pathology: MetS, T2DM, CVD | Program: training program (12 months) LI Frequency: 2 times/week Intensity: 55% (HRpeak); 60% (2 sets, 15 rep) Type: aerobic, resistance Time: 75 min | -TG * -LDL * +HDL * -SBP -DBP -BMI -WC * |
| Balducci et al., 2008, Italy [31] | A8 | To evaluate the efficacy of an intensive lifestyle intervention on modifiable cardiovascular disease (CVD) risk factors in a large cohort of people with type 2 diabetes and metabolic syndrome | n = 303 Age: 60 ± 6 years Sex: both genders Pathology: MetS, T2DM, CVD | Program: training program (12 months) HI Frequency: 2 times/week Intensity: 70% (HRpeak); 80% (3 sets, eight rep) Type: aerobic, resistance Time: 75 min | -TG * -LDL * +HDL * -SBP -DBP -BMI -WC * |
| Kambic et al., 2023, Slovenia [27] | A9 | To examine whether the addition of high-load (HL) or low-load (LL) RT has any effect on the levels of insulin resistance and lipids versus aerobic training (AT) alone in patients with coronary artery disease (CAD). | n = 26 Age: 61 ± 8 years Sex: both genders Pathology: coronary artery disease (CAD) | Program: cycling, HL-RT (12 weeks) Frequency: 3 times/week Intensity: 50–80% HRpeak, 3 sets 70% of 1RM (6–11 rep/set) to 80% of 1RM (12–16 rep/set) Type: aerobic, anaerobic Time: 50 min/session | -BW -BMI * -LDL * -TG +FBG -TC * =HDL |
| Kambic et al., 2023, Slovenia [27] | A10 | To examine whether the addition of high-load (HL) or low-load (LL) RT has any effect on the levels of insulin resistance and lipids versus aerobic training (AT) alone in patients with coronary artery disease (CAD). | n = 28 Age: 61 ± 8 years Sex: both genders Pathology: coronary artery disease (CAD) | Program: cycling, LL-RT (12 weeks) Frequency: 3 times/week Intensity: 50–80% HRpeak, 3 sets 35% of 1RM (6–11 rep/set) to 40% of 1RM (12–16 rep/set) Type: aerobic, anaerobic Time: 50 min/session | -BW -BMI * -LDL =TG -FBG -TC =HDL |
| Bönhof et al., 2022, Germany [29] | A11 | To determine which modality of exercise training as a component of lifestyle intervention may exert favourable effects on somatosensory and autonomic nerve tests in people with type 2 diabetes. | n = 23 Age: 30–65 years Sex: men Pathology: T2DM | Program: HIIT (12 weeks) Frequency: 3 times/week Intensity: 4 min 90% HRpeak, 3 min 70% HRpeakType: aerobic Time: 35 min/session | =BMI -SBP * -DBP * -TG +TC +HDL -LDL |
| Farag et al., 2018, Iran [28] | A12 | In the present study, we hypothesized that the intake of vitamin D and/or C with endurance physical activity might reduce the risk of metabolic syndrome. | n = 180 Age: between 30 and 50 years Sex: both genders Pathology: MetS | Program: climbing, running Frequency: 2 times/week each Intensity: not specified Type: aerobic Time: 360 min/week | -BW -BMI +WC -FBS * -TG * -LDL * +HDL * -SBP -DBP -TC * |
| Siu et al., 2015, China [23] | A13 | To examine the effects of 1 year of yoga exercise on the cardiovascular risk factors, including central obesity, hypertension, dyslipidemia and hyperglycemia in middle-aged and older Hong Kong Chinese adults with MetS. | n = 182 Age: 56 ± 9.1 years Sex: not specified Pathology: MetS | Program: yoga (1 year) Frequency: 3 times/week Intensity: not specified Type: aerobic, anaerobic Time: 60 min/session | -WC * -SBP -DBP -FBS -TG =HDL |
| Ranasinghe et al., 2020, Australia [24] | A14 | To examine the effects of aerobic training (AT) and resistance training (RT) compared to standard care on glycemic control in South Asian Sri Lankan adults with type 2 diabetes mellitus (T2DM). | n = 28 Age: 35–65 years Sex: both genders Pathology: T2DM | Program: aerobic training (3 months) Frequency: 2 times/week Intensity: 60–70% HRpeak Type: aerobic Time: 75 min/session | =BW =BMI +WC -HDL -LDL +TG -SBP =DBP -FBS -TC |
| Ranasinghe et al., 2020, Australia [24] | A15 | To examine the effects of aerobic training (AT) and resistance training (RT) compared to standard care on glycemic control in South Asian Sri Lankan adults with type 2 diabetes mellitus (T2DM). | n = 28 Age: 35–65 years Sex: both genders Pathology: T2DM | Program: resistance training (3 months) Frequency: 2 times/week Intensity: 50%-1RM (8 rep/three sets) Type: anaerobic Time: 75 min/session | -BW =BMI +WC +HDL * -LDL * +TG -SBP +DBP +FBS * |
| Farag et al., 2019, Iran [28] | A16 | To determine the effects of vitamin D supplementation along with endurance physical activity on lipid profile among metabolic syndrome patients. | n = 90 Age: 30–50 years Sex: both genders Pathology: MetS | Program: climbing, running Frequency: 2 times/week each Intensity: not specified Type: aerobic Time: 360 min/week | -TG +TC +LDL +HDL |
| Slivovskaja et al., 2017, Lithuania [22] | A17 | To evaluate if 4-week supervised aerobic training had any impact on anthropometric, metabolic, hemodynamic, and arterial wall parameters in MetS subjects. | n = 57 Age: 52.79 ± 6.65 years Sex: both genders Pathology: MetS | Program: (4 weeks) Frequency: 5 times/week Intensity: gradually increased by 40–60% HRRType: aerobic training Time: 30–40 min/session | -BM -WC * -LDL * -DBP * -BP * |
| Kambic et al., 2023, Slovenia [27] | A18 | Examine whether the addition of high-load (HL) or low-load (LL) RT has any effect on insulin resistance and lipid levels compared to aerobic training (AT) alone in patients with coronary artery disease (CAD). | n = 25 Age: 61 ± 8 years Sex: both genders Pathology: Coronary artery disease (CAD). | Program: Cycling, HL-RT (12 weeks) Frequency: 3 times/week Intensity: 50–80% HRpeak, Type: aerobic Time: 40 min/session | -BW -LDL =TG =FBG -TC =HDL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galván, B.; Enriquez del Castillo, L.A.; Flores, L.A.; Quintana-Mendias, E.; Torres-Rojo, F.I.; Villegas-Balderrama, C.V.; Cervantes-Hernández, N. Effectiveness of Physical Exercise on Indicators of Metabolic Syndrome in Adults: A Systematic Review with Meta-Analysis of Clinical Trials. J. Funct. Morphol. Kinesiol. 2025, 10, 244. https://doi.org/10.3390/jfmk10030244
Galván B, Enriquez del Castillo LA, Flores LA, Quintana-Mendias E, Torres-Rojo FI, Villegas-Balderrama CV, Cervantes-Hernández N. Effectiveness of Physical Exercise on Indicators of Metabolic Syndrome in Adults: A Systematic Review with Meta-Analysis of Clinical Trials. Journal of Functional Morphology and Kinesiology. 2025; 10(3):244. https://doi.org/10.3390/jfmk10030244
Chicago/Turabian StyleGalván, Brandon, Liliana Aracely Enriquez del Castillo, Luis Alberto Flores, Estefania Quintana-Mendias, Flor Isela Torres-Rojo, Cinthia Verónica Villegas-Balderrama, and Natanael Cervantes-Hernández. 2025. "Effectiveness of Physical Exercise on Indicators of Metabolic Syndrome in Adults: A Systematic Review with Meta-Analysis of Clinical Trials" Journal of Functional Morphology and Kinesiology 10, no. 3: 244. https://doi.org/10.3390/jfmk10030244
APA StyleGalván, B., Enriquez del Castillo, L. A., Flores, L. A., Quintana-Mendias, E., Torres-Rojo, F. I., Villegas-Balderrama, C. V., & Cervantes-Hernández, N. (2025). Effectiveness of Physical Exercise on Indicators of Metabolic Syndrome in Adults: A Systematic Review with Meta-Analysis of Clinical Trials. Journal of Functional Morphology and Kinesiology, 10(3), 244. https://doi.org/10.3390/jfmk10030244