
Effects of High-Intensity Intermittent Training Combined with Asparagus officinalis Extract Supplementation on Cardiovascular and Pulmonary Function Parameters in Obese and Overweight Individuals: A Randomized Control Trial



Abstract

1. Introduction
2. Materials and Methods
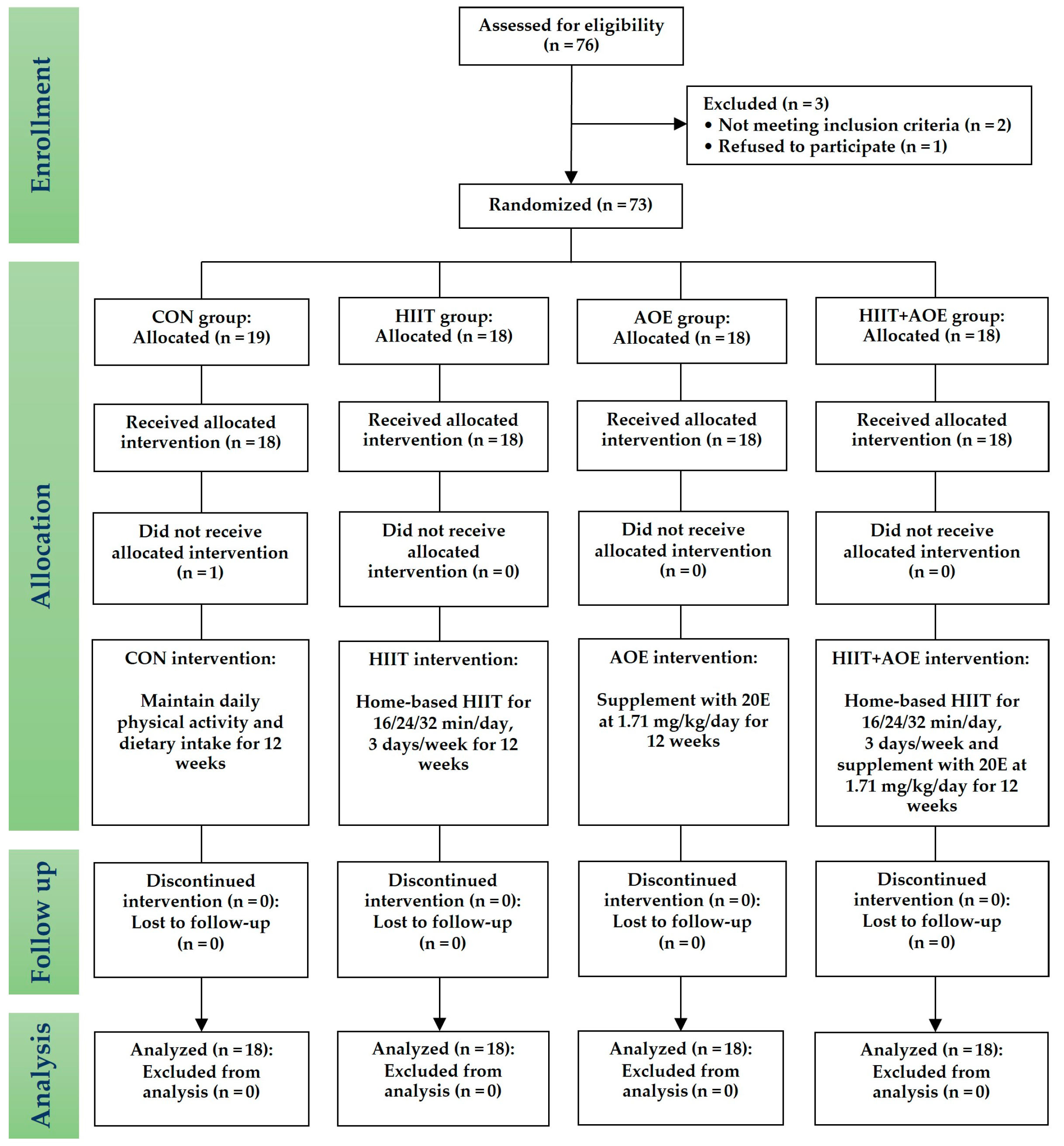
2.1. Study Design
2.2. Screening of Participants
2.3. Sample Size
2.4. HIIT
2.5. Supplement
2.6. Experiments
- Participants in the CON group maintained their daily physical activity and dietary intake.
- Participants in the HIIT group performed a home-based HIIT program for 3 days/week.
2.7. Study End Points
2.7.1. HR Variability
2.7.2. Endothelial Function
2.7.3. BP and BP Variability
2.7.4. Static and Dynamic Lung Volume and Capacity
2.7.5. Respiratory Muscle Strength
2.7.6. Chest Wall Expansion
2.7.7. Body Composition
2.7.8. Physical Activity
2.7.9. Feasibility
2.8. Statistical Analysis
3. Results
3.1. Participant Characteristics and Feasibility
3.2. Effects on HR and HR Variability
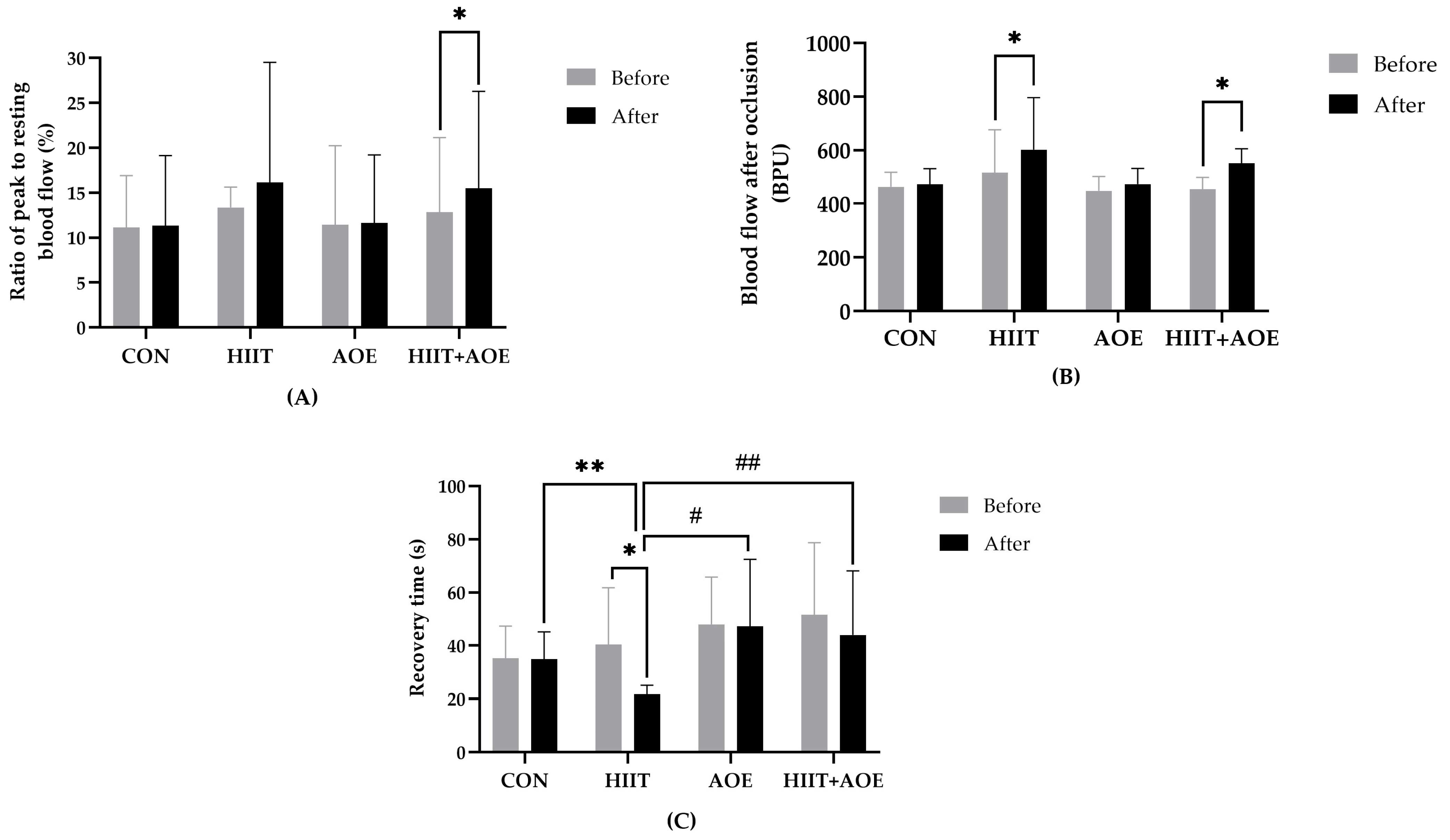
3.3. Effects on Endothelial Function
3.4. Effects on BP and BP Variability
3.5. Effects on Pulmonary Function
3.6. Effects on Respiratory Muscle Strength
3.7. Effects on Chest Wall Expansion and Pulmonary Volume
3.8. Effects on Body Composition
4. Discussion
4.1. Effects of HIIT Combined with A. officinalis Extract Supplementation on Cardiovascular Function Parameters
4.2. Effects of HIIT Combined with A. officinalis Extract Supplementation on Pulmonary Function Parameters
4.3. Effects of HIIT Combined with A. officinalis Extract Supplementation on Body Composition Parameters
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 20E | 20-Hydroxyecdysone |
| AOE | A. officinalis extract group |
| BMI | Body mass index |
| BP | Blood pressure |
| BPV | Blood pressure variability |
| COM | Combined group |
| CON | Control group |
| CV | Coefficient of variation |
| DBP | Diastolic blood pressure |
| ERV | Expiratory reserve volume |
| ES | Effect size |
| FET | Forced expiratory time |
| FEV1 | Forced expiratory volume in one second |
| FRC | Functional residual capacity |
| FVC | Forced vital capacity |
| HF | High frequency |
| HIIT | High-intensity intermittent training |
| HPLC | High-performance liquid chromatography |
| HR | Heart rate |
| HRV | Heart rate variability |
| ICC | Intra-class correlation coefficient |
| IRV | Inspiratory reserve volume |
| LF | Low frequency |
| MAP | Mean arterial pressure |
| MEP | Maximum expiratory mouth pressure |
| MIP | Maximum inspiratory mouth pressure |
| MVV | Maximal voluntary ventilation |
| PEF | Peak expiratory flow rate |
| PIF | Peak inspiratory flow rate |
| PP | Pulse pressure |
| RMSSD | Root mean square of successive RR interval |
| RPE | Rating of perceived exertion |
| RPP | Rate–pressure product |
| SD | Standard deviation |
| SDNN | Standard deviation of normal beat-to-beat |
| TP | Total power |
| TV | Tidal volume |
| UV | Ultraviolet |
| VC | Vital capacity |
| VLF | Very low frequency |
References
- Collaborators, G.F. Burden of disease scenarios for 204 countries and territories, 2022–2050: A forecasting analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2204–2256. [Google Scholar] [CrossRef]
- Ansari, S.; Haboubi, H.; Haboubi, N. Adult obesity complications: Challenges and clinical impact. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820934955. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, C.L.; Kaiser, D.R.; Steinberger, J.; Kelly, A.S.; Dengel, D.R. Relationships of cardiac autonomic function with metabolic abnormalities in childhood obesity. Obesity 2007, 15, 1164–1171. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Cuspidi, C.; Vukomanovic, V.; Kocijancic, V.; Celic, V.; Stanisavljevic, D. The Association between Obesity, Blood Pressure Variability, and Right Ventricular Function and Mechanics in Hypertensive Patients. J. Am. Soc. Echocardiogr. 2016, 29, 802–811. [Google Scholar] [CrossRef]
- Yadav, R.L.; Yadav, P.K.; Yadav, L.K.; Agrawal, K.; Sah, S.K.; Islam, M.N. Association between obesity and heart rate variability indices: An intuition toward cardiac autonomic alteration–a risk of CVD. Diabetes Metab. Syndr. Obes. 2017, 10, 57–64. [Google Scholar] [CrossRef]
- Pelosi, P.; Croci, M.; Ravagnan, I.; Tredici, S.; Pedoto, A.; Lissoni, A.; Gattinoni, L. The effects of body mass on lung volumes, respiratory mechanics, and gas exchange during general anesthesia. Anesth. Analg. 1998, 87, 654–660. [Google Scholar] [CrossRef]
- Hedenstierna, G.; Santesson, J. Breathing mechanics, dead space and gas exchange in the extremely obese, breathing spontaneously and during anaesthesia with intermittent positive pressure ventilation. Acta Anaesthesiol. Scand. 1976, 20, 248–254. [Google Scholar] [CrossRef]
- Sharp, J.T.; Henry, J.P.; Sweany, S.K.; Meadows, W.R.; Pietras, R.J. The total work of breathing in normal and obese men. J. Clin. Investig. 1964, 43, 728–739. [Google Scholar] [CrossRef]
- Naimark, A.; Cherniack, R.M. Compliance of the respiratory system and its components in health and obesity. J. Appl. Physiol. 1960, 15, 377–382. [Google Scholar] [CrossRef]
- Schachter, L.M.; Salome, C.M.; Peat, J.K.; Woolcock, A.J. Obesity is a risk for asthma and wheeze but not airway hyperresponsiveness. Thorax 2001, 56, 4–8. [Google Scholar] [CrossRef]
- Jones, R.L.; Nzekwu, M.M. The effects of body mass index on lung volumes. Chest 2006, 130, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Sin, D.D.; Jones, R.L.; Man, S.F. Obesity is a risk factor for dyspnea but not for airflow obstruction. Arch. Intern. Med. 2002, 162, 1477–1481. [Google Scholar] [CrossRef] [PubMed]
- Zerah, F.; Harf, A.; Perlemuter, L.; Lorino, H.; Lorino, A.M.; Atlan, G. Effects of obesity on respiratory resistance. Chest 1993, 103, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.; Sparrow, D.; Weiss, S.T. Effects of obesity and fat distribution on ventilatory function: The normative aging study. Chest 1997, 111, 891–898. [Google Scholar] [CrossRef]
- Biring, M.S.; Lewis, M.I.; Liu, J.T.; Mohsenifar, Z. Pulmonary physiologic changes of morbid obesity. Am. J. Med. Sci. 1999, 318, 293–297. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- American College of Sports, M.; Liguori, G.; Feito, Y.; Fountaine, C.; Roy, B.A. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2022. [Google Scholar]
- Tschakert, G.; Hofmann, P. High-Intensity Intermittent Exercise: Methodological and Physiological Aspects. Int. J. Sports Physiol. Perform. 2013, 8, 600–610. [Google Scholar] [CrossRef]
- Boutcher, S.H. High-intensity intermittent exercise and fat loss. J. Obes. 2011, 2011, 868305. [Google Scholar] [CrossRef]
- Tabata, I.; Irisawa, K.; Kouzaki, M.; Nishimura, K.; Ogita, F.; Miyachi, M. Metabolic profile of high intensity intermittent exercises. Med. Sci. Sports Exerc. 1997, 29, 390–395. [Google Scholar] [CrossRef]
- Tabata, I. Tabata training: One of the most energetically effective high-intensity intermittent training methods. J. Physiol. Sci. 2019, 69, 559–572. [Google Scholar] [CrossRef]
- Padkao, T.; Prasertsri, P. The Impact of Modified Tabata Training on Segmental Fat Accumulation, Muscle Mass, Muscle Thickness, and Physical and Cardiorespiratory Fitness in Overweight and Obese Participants: A Randomized Control Trial. Sports 2025, 13, 99. [Google Scholar] [CrossRef] [PubMed]
- Lafont, R.; Balducci, C.; Dinan, L. Ecdysteroids. Encyclopedia 2021, 1, 1267–1302. [Google Scholar] [CrossRef]
- Dinan, L.; Dioh, W.; Veillet, S.; Lafont, R. 20-Hydroxyecdysone, from Plant Extracts to Clinical Use: Therapeutic Potential for the Treatment of Neuromuscular, Cardio-Metabolic and Respiratory Diseases. Biomedicines 2021, 9, 492. [Google Scholar] [CrossRef] [PubMed]
- Denben, B.; Sripinyowanich, S.; Ruangthai, R.; Phoemsapthawee, J. Beneficial Effects of Asparagus officinalis Extract Supplementation on Muscle Mass and Strength following Resistance Training and Detraining in Healthy Males. Sports 2023, 11, 175. [Google Scholar] [CrossRef]
- Seidlova-Wuttke, D.; Wuttke, W. In a placebo-controlled study ß-Ecdysone (ECD) prevented the development of the metabolic syndrome. Planta Medica 2012, 78, CL37. [Google Scholar] [CrossRef]
- Wuttke, W.; Seidlova-Wuttke, D. Beta-ecdysone (Ecd) prevents visceral, bone marrow and joint fat accumulation and has positive effects on serum lipids, bone and joint cartilage. Planta Medica 2012, 78, PD68. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [CrossRef]
- Sripinyowanich, S.; Petchsri, S.; Tongyoo, P.; Lee, T.K.; Lee, S.; Cho, W.K. Comparative Transcriptomic Analysis of Genes in the 20-Hydroxyecdysone Biosynthesis in the Fern Microsorum scolopendria towards Challenges with Foliar Application of Chitosan. Int. J. Mol. Sci. 2023, 24, PD68. [Google Scholar] [CrossRef]
- Matsuda, H.; Kawaba, T.; Yamamoto, Y. Pharmacological studies of insect metamorphotic steroids. Nihon Yakurigaku Zasshi 1970, 66, 551–563. [Google Scholar]
- Vierra, J.; Boonla, O.; Prasertsri, P. Effects of sleep deprivation and 4-7-8 breathing control on heart rate variability, blood pressure, blood glucose, and endothelial function in healthy young adults. Physiol. Rep. 2022, 10, e15389. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Hall, J.; Larsson, A.; Annuk, M.; Fellstrom, B.; Lithell, H. Evaluation of endothelium-dependent vasodilation in the human peripheral circulation. Clin. Physiol. 2000, 20, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [CrossRef]
- Debouche, S.; Pitance, L.; Robert, A.; Liistro, G.; Reychler, G. Reliability and Reproducibility of Chest Wall Expansion Measurement in Young Healthy Adults. J. Manipulative Physiol. Ther. 2016, 39, 443–449. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Jalayondeja, C.; Jalayondeja, W.; Vachalathiti, R.; Bovonsunthonchai, S.; Sakulsriprasert, P.; Kaewkhuntee, W.; Bunprajun, T.; Upiriyasakul, R. Cross-Cultural Adaptation of the Compendium of Physical Activity: Thai Translation and Content Validity. J. Med. Assoc. Thai 2015, 98, S53–S59. [Google Scholar]
- Baecke, J.A.; Burema, J.; Frijters, J.E. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 1982, 36, 936–942. [Google Scholar] [CrossRef]
- Cocks, M.; Shaw, C.S.; Shepherd, S.O.; Fisher, J.P.; Ranasinghe, A.; Barker, T.A.; Wagenmakers, A.J. Sprint interval and moderate-intensity continuous training have equal benefits on aerobic capacity, insulin sensitivity, muscle capillarisation and endothelial eNOS/NAD(P)Hoxidase protein ratio in obese men. J. Physiol. 2016, 594, 2307–2321. [Google Scholar] [CrossRef]
- Hasegawa, N.; Fujie, S.; Horii, N.; Miyamoto-Mikami, E.; Tsuji, K.; Uchida, M.; Hamaoka, T.; Tabata, I.; Iemitsu, M. Effects of Different Exercise Modes on Arterial Stiffness and Nitric Oxide Synthesis. Med. Sci. Sports Exerc. 2018, 50, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Zador, E. Molecular Targets of 20-Hydroxyecdysone in Mammals, Mechanism of Action: Is It a Calorie Restriction Mimetic and Anti-Aging Compound? Cells 2025, 14, 431. [Google Scholar] [CrossRef] [PubMed]
- Orie, N.N.; Raees, A.; Aljaber, M.Y.; Mohamed-Ali, N.; Bensmail, H.; Hamza, M.M.; Al-Ansari, N.; Beotra, A.; Mohamed-Ali, V.; Almaadheed, M. 20-hydroxyecdysone dilates muscle arterioles in a nitric oxide-dependent, estrogen ER-β receptor-independent manner. Phytomedicine Plus 2021, 1, 100078. [Google Scholar] [CrossRef]
- Turnbull, F. Effects of different blood-pressure-lowering regimens on major cardiovascular events: Results of prospectively-designed overviews of randomised trials. Lancet 2003, 362, 1527–1535. [Google Scholar] [CrossRef]
- The Blood Pressure Lowering Treatment Trialists’ Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis. Lancet 2021, 397, 1625–1636. [Google Scholar] [CrossRef]
- Lu, Y.; Wiltshire, H.D.; Baker, J.S.; Wang, Q.; Ying, S. The effect of Tabata-style functional high-intensity interval training on cardiometabolic health and physical activity in female university students. Front. Physiol. 2023, 14, 1095315. [Google Scholar] [CrossRef]
- Buniam, J.; Chukijrungroat, N.; Rattanavichit, Y.; Surapongchai, J.; Weerachayaphorn, J.; Bupha-Intr, T.; Saengsirisuwan, V. 20-Hydroxyecdysone ameliorates metabolic and cardiovascular dysfunction in high-fat-high-fructose-fed ovariectomized rats. BMC Complement. Med. Ther. 2020, 20, 140. [Google Scholar] [CrossRef]
- Tsai, S.Y.; Hsu, J.Y.; Lin, C.H.; Kuo, Y.C.; Chen, C.H.; Chen, H.Y.; Liu, S.J.; Chien, K.L. Association of stress hormones and the risk of cardiovascular diseases systematic review and meta-analysis. Int. J. Cardiol. Cardiovasc. Risk Prev. 2024, 23, 200305. [Google Scholar] [CrossRef]
- Songsorn, P.; Somnarin, K.; Jaitan, S.; Kupradit, A. The effect of whole-body high-intensity interval training on heart rate variability in insufficiently active adults. J. Exerc. Sci. Fit. 2022, 20, 48–53. [Google Scholar] [CrossRef]
- Heydari, M.; Boutcher, Y.N.; Boutcher, S.H. High-intensity intermittent exercise and cardiovascular and autonomic function. Clin. Auton. Res. 2013, 23, 57–65. [Google Scholar] [CrossRef]
- Phungphong, S.; Kijtawornrat, A.; Chaiduang, S.; Saengsirisuwan, V.; Bupha-Intr, T. 20-Hydroxyecdysone attenuates cardiac remodeling in spontaneously hypertensive rats. Steroids 2017, 126, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Zaroni, R.S.; Brigatto, F.A.; Schoenfeld, B.J.; Braz, T.V.; Benvenutti, J.C.; Germano, M.D.; Marchetti, P.H.; Aoki, M.S.; Lopes, C.R. High Resistance-Training Frequency Enhances Muscle Thickness in Resistance-Trained Men. J. Strength Cond. Res. 2019, 33 Suppl. 1, S140–S151. [Google Scholar] [CrossRef]
- Heydari, M.; Freund, J.; Boutcher, S.H. The effect of high-intensity intermittent exercise on body composition of overweight young males. J. Obes. 2012, 2012, 480467. [Google Scholar] [CrossRef] [PubMed]
- Sieck, G.C.; Ferreira, L.F.; Reid, M.B.; Mantilla, C.B. Mechanical properties of respiratory muscles. Compr. Physiol. 2013, 3, 1553–1567. [Google Scholar] [CrossRef] [PubMed]
- Dioh, W.; Chabane, M.; Tourette, C.; Azbekyan, A.; Morelot-Panzini, C.; Hajjar, L.A.; Lins, M.; Nair, G.B.; Whitehouse, T.; Mariani, J.; et al. Testing the efficacy and safety of BIO101, for the prevention of respiratory deterioration, in patients with COVID-19 pneumonia (COVA study): A structured summary of a study protocol for a randomised controlled trial. Trials 2021, 22, 42. [Google Scholar] [CrossRef]
- Burgomaster, K.A.; Howarth, K.R.; Phillips, S.M.; Rakobowchuk, M.; Macdonald, M.J.; McGee, S.L.; Gibala, M.J. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J. Physiol. 2008, 586, 151–160. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, L.; Xiao, C.; Li, J.; Hu, T.; Li, L. Association between waist-to-hip ratio and risk of myocardial infarction: A systematic evaluation and meta-analysis. Front. Cardiovasc. Med. 2024, 11, 1438817. [Google Scholar] [CrossRef]
- Robledo-Millan, C.R.; Diaz-Dominguez, M.R.; Castaneda-Ramirez, A.E.; Quinones-Lara, E.; Valencia-Marin, S.; Suarez-Garcia, R.X.; Lopez-Desiderio, N.G.; Ramos-Cortes, C.A.; Gaytan Gomez, A.M.; Bello-Lopez, J.M.; et al. A Novel Metabolic Risk Classification System Incorporating Body Fat, Waist Circumference, and Muscle Strength. J. Funct. Morphol. Kinesiol. 2025, 10, 72. [Google Scholar] [CrossRef]
- Liu, J.; Xu, H.; Cupples, L.A.; GT, O.C.; Liu, C.T. The impact of obesity on lung function measurements and respiratory disease: A Mendelian randomization study. Ann. Hum. Genet. 2023, 87, 174–183. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CON Group | HIIT Group | AOE Group | HIIT + AOE Group | |
|---|---|---|---|---|
| Number | 18 | 18 | 18 | 18 |
| Sex (n, male–female) | 5:13 | 5:13 | 2:16 | 2:16 |
| Age (years) | 21.61 ± 2.06 | 20.72 ± 1.32 | 20.22 ± 1.93 | 20.06 ± 2.01 |
| WHO BMI classification (n, obese–overweight) | 16:2 | 13:5 | 13:5 | 13:5 |
| Physical activity level | ||||
| Sedentary (n, %) | 3 (17%) | 3 (17%) | 3 (17%) | 1 (6%) |
| Active (n, %) | 11 (61%) | 12 (66%) | 9 (55%) | 14 (78%) |
| Athletic (n, %) | 4 (22%) | 3 (17%) | 6 (33%) | 3 (17%) |
| Physical activity score | ||||
| Before | 7.01 ± 1.07 | 7.04 ± 0.99 | 7.46 ± 1.19 | 6.86 ± 0.85 |
| After | 6.96 ± 0.79 | 7.31 ± 1.22 | 7.27 ± 0.99 | 7.37 ± 1.20 |
| CON Group (n = 18) | HIIT Group (n = 18) | AOE Group (n = 18) | HIIT + AOE Group (n = 18) | |||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | |
| HR (beats/min) | 76.53 ± 10.56 | 73.55 ± 11.04 | 77.95 ± 10.82 | 76.04 ± 10.03 | 75.03 ± 15.69 | 78.07 ± 9.94 | 74.09 ± 9.98 | 72.00 ± 8.25 |
| NN interval (ms) | 795.97 ± 93.24 | 831.07 ± 110.27 | 783.90 ± 110.24 | 803.33 ± 116.17 | 830.61 ± 161.17 | 781.56 ± 110.01 | 823.12 ± 106.74 | 844.26 ± 102.25 |
| SDNN (ms) | 56.42 ± 23.76 | 57.83 ± 21.09 | 48.79 ± 25.81 | 52.67 ± 20.47 | 62.02 ± 35.66 | 66.09 ± 45.50 | 62.77 ± 26.12 | 64.09 ± 26.12 |
| RMSSD (ms) | 48.36 ± 32.78 | 48.86 ± 22.86 | 39.32 ± 29.86 | 42.11 ± 25.69 | 64.15 ± 57.77 | 60.56 ± 65.05 | 56.22 ± 34.57 | 57.99 ± 35.70 |
| Total power (ms2) | 3536.15 ± 2982.59 | 3274.70 ± 2221.98 | 2965.62 ± 3132.98 | 2987.58 ± 2328.17 | 4895.11 ± 3803.14 | 6562.20 ± 4461.31 | 4397.41 ± 3847.59 | 4616.22 ± 4457.35 |
| VLF power (ms2) | 1377.50 ± 895.81 | 1564.83 ± 1024.58 | 1139.12 ± 1542.15 | 1182.67 ± 899.51 | 1366.86 ± 1100.79 | 2437.27 ± 2623.72 | 1678.00 ± 1474.66 | 1929.49 ± 1743.83 |
| LF power (ms2) | 799.42 ± 842.98 | 924.37 ± 448.48 | 715.01 ± 542.55 | 652.06 ± 462.84 | 953.64 ± 839.18 | 922.38 ± 3586.96 | 1170.22 ± 1492.73 | 963.91 ± 973.55 |
| LF power (nu) | 44.82 ± 18.09 | 49.09 ± 19.98 | 53.14 ± 13.72 | 40.80 ± 16.33 * | 44.04 ± 21.70 | 40.23 ± 23.03 | 40.53 ± 16.38 | 33.99 ± 11.74 * |
| HF power (ms2) | 1044.01 ± 1429.90 | 609.39 ± 478.49 | 1035.46 ± 1690.28 | 1168.29 ± 1165.66 | 2293.36 ± 3511.80 | 2467.31 ± 4393.79 | 1226.39 ± 985.26 | 1396.06 ± 1532.63 |
| HF power (nu) | 40.89 ± 17.65 | 39.06 ± 15.97 | 43.59 ± 17.03 | 49.54 ± 19.45 | 48.00 ± 21.62 | 50.75 ± 21.47 | 50.18 ± 15.37 | 55.47 ± 11.10 ** |
| LF/HF ratio | 1.65 ± 1.90 | 1.66 ± 1.31 | 1.58 ± 1.14 | 1.06 ± 0.81 * | 1.63 ± 2.11 | 1.30 ± 1.39 | 1.00 ± 0.78 | 0.67 ± 0.36 *,** |
| CON Group (n = 18) | HIIT Group (n = 18) | AOE Group (n = 18) | HIIT + AOE Group (n = 18) | |||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | |
| SBP (mmHg) | 118.64 ± 16.15 | 112.42 ± 12.28 | 118.31 ± 11.77 | 114.12 ± 12.27 * | 112.33 ± 13.24 | 112.46 ± 12.56 | 110.70 ± 8.08 | 111.01 ± 9.17 |
| DBP (mmHg) | 74.40 ± 12.53 | 70.64 ± 8,14 | 73.94 ± 8.54 | 70.57 ± 8.72 * | 70.81 ± 11.46 | 71.72 ± 10.35 | 69.77 ± 7.16 | 69.24 ± 6.58 |
| MAP (mmHg) | 89.15 ± 13.03 | 84.57 ± 8.74 | 88.73 ± 8.99 | 85.09 ± 9.05 * | 84.65 ± 11.34 | 85.30 ± 10.57 | 83.42 ± 7.16 | 83.16 ± 7.10 |
| PP (mmHg) | 44.24 ± 9.91 | 41.77 ± 9.00 | 44.37 ± 7.89 | 43.55 ± 9.25 | 41.51 ± 8.85 | 40.74 ± 7.44 | 40.92 ± 4.61 | 41.77 ± 5.41 |
| RPP (mmHg/min) | 9156.46 ± 1604.82 | 8170.73 ± 1372.36 | 9147.75 ± 1704.77 | 8374.79 ± 1358.85 * | 8433.38 ± 2621.42 | 8043.40 ± 1408.16 | 8647.23 ± 1093.37 | 8179.88 ± 1589.57 |
| CON Group (n = 18) | HIIT Group (n = 18) | AOE Group (n = 18) | HIIT + AOE Group (n = 18) | |||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | |
| Forced expiratory volume in one second (FEV1) | ||||||||
| FEV1 (L) | 2.89 ± 0.52 | 2.87 ± 0.50 | 3.02 ± 0.87 | 3.06 ± 0.85 | 2.92 ± 0.59 | 3.00 ± 0.52 | 2.88 ± 0.54 | 2.94 ± 0.50 |
| FEV1 (%predicted) | 95.72 ± 9.81 | 95.44 ± 10.01 | 98.88 ± 11.58 | 100.44 ± 11.50 | 99.61 ± 15.95 | 101.11 ± 13.23 | 99.16 ± 14.27 | 101.44 ± 10.52 |
| Forced vital capacity (FVC) | ||||||||
| FVC (L) | 3.19 ± 0.65 | 3.21 ± 0.63 | 3.39 ± 1.08 | 3.44 ± 1.04 | 3.28 ± 0.64 | 3.34 ± 0.58 | 3.26 ± 0.58 | 3.26 ± 0.66 |
| FVC (%predicted) | 93.55 ± 8.16 | 94.22 ± 9.34 | 98.50 ± 13.09 | 100.11 ± 12.41 | 99.83 ± 14.68 | 100.00 ± 13.55 | 100.77 ± 11.55 | 100.67 ± 12.46 |
| Peak expiratory flow (PEF) | ||||||||
| PEF (L/min) | 6.95 ± 1.64 | 6.98 ± 1.62 | 6.49 ± 1.39 | 7.20 ± 1.41 * | 6.44 ± 1.79 | 7.15 ± 1.53 * | 6.24 ± 1.18 | 6.74 ± 1.12 * |
| PEF (%predicted) | 97.27 ± 25.16 | 97.50 ± 23.90 | 91.50 ± 15.45 | 101.56 ± 15.06 * | 92.27 ± 19.14 | 101.33 ± 16.78 * | 92.11 ± 12.87 | 99.83 ± 14.72 * |
| Forced expiratory volume in one second per forced vital capacity (FEV1/FVC) | ||||||||
| FEV1/FVC (%) | 90.77 ± 5.63 | 89.77 ± 5.57 * | 89.72 ± 5.54 | 89.61 ± 4.85 | 89.38 ± 6.89 | 90.33 ± 6.53 * | 88.72 ± 9.28 | 91.17 ± 5.34 *,** |
| FEV1/FVC (%predicted) | 101.05 ± 5.57 | 99.94 ± 5.59 * | 99.55 ± 5.92 | 99.50 ± 5.03 | 98.83 ± 7.48 | 100.22 ± 7.22 | 97.77 ± 10.14 | 100.61 ± 6.00 *,** |
| Forced expiratory flow at 25–75% of FVC (FEF25-75) | ||||||||
| FEF25-75 (L) | 3.71 ± 0.96 | 3.58 ± 0.89 | 3.67 ± 0.98 | 3.56 ± 0.76 | 3.61 ± 1.03 | 3.76 ± 0.95 | 3.46 ± 0.99 | 3.73 ± 0.60 |
| FEF25-75 (%predicted) | 98.00 ± 25.95 | 94.61 ± 24.24 | 96.00 ± 18.58 | 95.22 ± 17.82 | 97.1 ± 26.30 | 100.56 ± 24.68 | 94.11 ± 27.456 | 101.94 ± 18.35 |
| Maximal voluntary ventilation (MVV) (L/min) | 108.43 ± 19.59 | 107.85 ± 18.89 | 113.46 ± 32.73 | 114.92 ± 31.86 | 109.84 ± 22.43 | 112.88 ± 110.60 | 108.14 ± 20.25 | 110.60 ± 18.80 |
| Peak inspiratory flow (PIF) (L/min) | 4.71 ± 1.36 | 5.03 ± 1.31 | 4.22 ± 1.50 | 5.49 ± 1.61 * | 4.17 ± 1.41 | 5.17 ± 1.41 * | 4.11 ± 0.70 | 4.89 ± 1.21 * |
| Forced expiratory time (s) | 2.40 ± 0.61 | 2.51 ± 0.65 | 2.72 ± 0.65 | 2.82 ± 0.64 | 2.58 ± 0.73 | 2.50 ± 0.79 | 2.88 ± 0.90 | 2.61 ± 0.85 |
| CON Group (n = 18) | HIIT Group (n = 18) | AOE Group (n = 18) | HIIT + AOE Group (n = 18) | |||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | |
| Chest expansion | ||||||||
| Upper chest (cm) | 2.94 ± 1.49 | 3.02 ± 1.26 | 2.71 ± 1.11 | 3.54 ± 1.50 * | 2.83 ± 0.79 | 3.30 ± 0.84 | 3.40 ± 0.83 | 3.62 ± 1.39 |
| Middle chest (cm) | 2.07 ± 1.45 | 2.21 ± 1.46 | 2.36 ± 1.36 | 2.88 ± 2.00 | 2.37 ± 1.02 | 2.98 ± 1.36 | 2.97 ± 1.10 | 3.22 ± 1.36 |
| Lower chest (cm) | 2.89 ± 1.52 | 2.88 ± 1.56 | 3.41 ± 1.30 | 3.85 ± 1.75 | 3.85 ± 1.46 | 3.71 ± 0.92 | 3.81 ± 0.97 | 4.79 ± 1.49 *,** |
| Pulmonary volume | ||||||||
| VC (L) | 3.01 ± 0.73 | 3.10 ± 0.71 | 3.22 ± 1.16 | 3.34 ± 1.13 * | 3.02 ± 0.62 | 3.21 ± 0.58 * | 3.13 ± 0.69 | 3.17 ± 0.67 |
| IC (L) | 1.93 ± 0.05 | 2.00 ± 0.59 | 2.02 ± 0.64 | 2.17 ± 0.63 | 1.77 ± 0.64 | 2.08 ± 0.60 * | 1.91 ± 0.30 | 1.96 ± 0.44 |
| TV (L) | 0.96 ± 0.38 | 0.86 ± 0.54 | 0.94 ± 0.47 | 0.99 ± 0.39 | 0.84 ± 0.35 | 0.88 ± 0.43 | 0.99 ± 0.41 | 0.95 ± 0.47 |
| ERV (L) | 1.12 ± 0.56 | 1.11 ± 0.51 | 1.19 ± 0.62 | 1.17 ± 0.58 | 1.25 ± 0.41 | 1.13 ± 0.38 | 1.22 ± 0.50 | 1.21 ± 0.42 |
| IRV (L) | 0.96 ± 0.47 | 1.15 ± 0.59 | 1.07 ± 0.52 | 1.19 ± 0.52 | 0.93 ± 0.60 | 1.20 ± 0.41 * | 0.92 ± 0.31 | 1.01 ± 0.51 |
| CON Group (n = 18) | HIIT Group (n = 18) | AOE Group (n = 18) | HIIT + AOE Group (n = 18) | |||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | |
| Body mass (kg) | 77.40 ± 15.25 | 77.36 ± 14.49 | 77.64 ± 16.60 | 78.89 ± 16.75 | 71.43 ± 13.05 | 72.71 ± 13.54 | 70.47 ± 7.60 | 71.19 ± 7.67 |
| Body mass index (kg/m2) | 29.10 ± 5.11 | 29.11 ± 4.87 | 29.13 ± 5.48 | 29.59 ± 5.65 | 26.98 ± 2.97 | 27.44 ± 3.04 | 26.92 ± 2.50 | 27.19 ± 2.32 |
| Skeletal muscle mass (kg) | 25.37 ± 5.52 | 25.25 ± 5.55 | 25.88 ± 6.08 | 26.14 ± 6.27 | 24.60 ± 5.79 | 24.79 ± 6.09 | 24.14 ± 3.97 | 23.96 ± 3.84 |
| Fat-free mass (kg) | 46.04 ± 9.06 | 45.82 ± 9.06 | 46.85 ± 9.84 | 47.24 ± 10.20 | 44.73 ± 9.60 | 45.11 ± 10.12 | 44.12 ± 6.50 | 43.77 ± 6.28 |
| Fat mass (kg) | 31.36 ± 10.23 | 31.53 ± 9.62 | 30.79 ± 11.64 | 31.65 ± 11.85 | 26.70 ± 6.21 | 27.60 ± 6.52 | 26.34 ± 5.26 | 27.42 ± 4.84 |
| Percent body fat (%) | 40.07 ± 7.38 | 40.44 ± 7.14 | 39.02 ± 8.98 | 39.54 ± 9.21 | 37.44 ± 5.53 | 38.04 ± 5.64 | 37.37 ± 5.79 | 38.52 ± 5.10 |
| Waist circumference (cm) | 95.13 ± 9.53 | 95.41 ± 11.75 | 95.31 ± 12.97 | 94.38 ± 12.99 | 87.73 ± 9.92 | 89.28 ± 9.44 | 85.04 ± 8.13 | 86.96 ± 6.99 |
| Waist–hip ratio | 0.92 ± 0.06 | 0.94 ± 0.06 * | 0.91 ± 0.06 | 0.91 ± 0.06 | 0.91 ± 0.15 | 0.93 ± 0.81 | 0.87 ± 0.04 | 0.88 ± 0.05 ** |
| Basal metabolic rate (kcal) | 1364 ± 195 | 1359 ± 196 | 1382 ± 212 | 1390 ± 220 | 1336 ± 207 | 1344 ± 218 | 1323 ± 140 | 1315 ± 135 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padkao, T.; Prasertsri, P. Effects of High-Intensity Intermittent Training Combined with Asparagus officinalis Extract Supplementation on Cardiovascular and Pulmonary Function Parameters in Obese and Overweight Individuals: A Randomized Control Trial. J. Funct. Morphol. Kinesiol. 2025, 10, 202. https://doi.org/10.3390/jfmk10020202
Padkao T, Prasertsri P. Effects of High-Intensity Intermittent Training Combined with Asparagus officinalis Extract Supplementation on Cardiovascular and Pulmonary Function Parameters in Obese and Overweight Individuals: A Randomized Control Trial. Journal of Functional Morphology and Kinesiology. 2025; 10(2):202. https://doi.org/10.3390/jfmk10020202
Chicago/Turabian StylePadkao, Tadsawiya, and Piyapong Prasertsri. 2025. "Effects of High-Intensity Intermittent Training Combined with Asparagus officinalis Extract Supplementation on Cardiovascular and Pulmonary Function Parameters in Obese and Overweight Individuals: A Randomized Control Trial" Journal of Functional Morphology and Kinesiology 10, no. 2: 202. https://doi.org/10.3390/jfmk10020202
APA StylePadkao, T., & Prasertsri, P. (2025). Effects of High-Intensity Intermittent Training Combined with Asparagus officinalis Extract Supplementation on Cardiovascular and Pulmonary Function Parameters in Obese and Overweight Individuals: A Randomized Control Trial. Journal of Functional Morphology and Kinesiology, 10(2), 202. https://doi.org/10.3390/jfmk10020202