
Intra-Session Reliability and Predictive Value of Maximum Voluntary Isometric Contraction for Estimating One-Repetition Maximum in Older Women: A Randomised Split-Sample Study

 , , ,
, , ,  , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
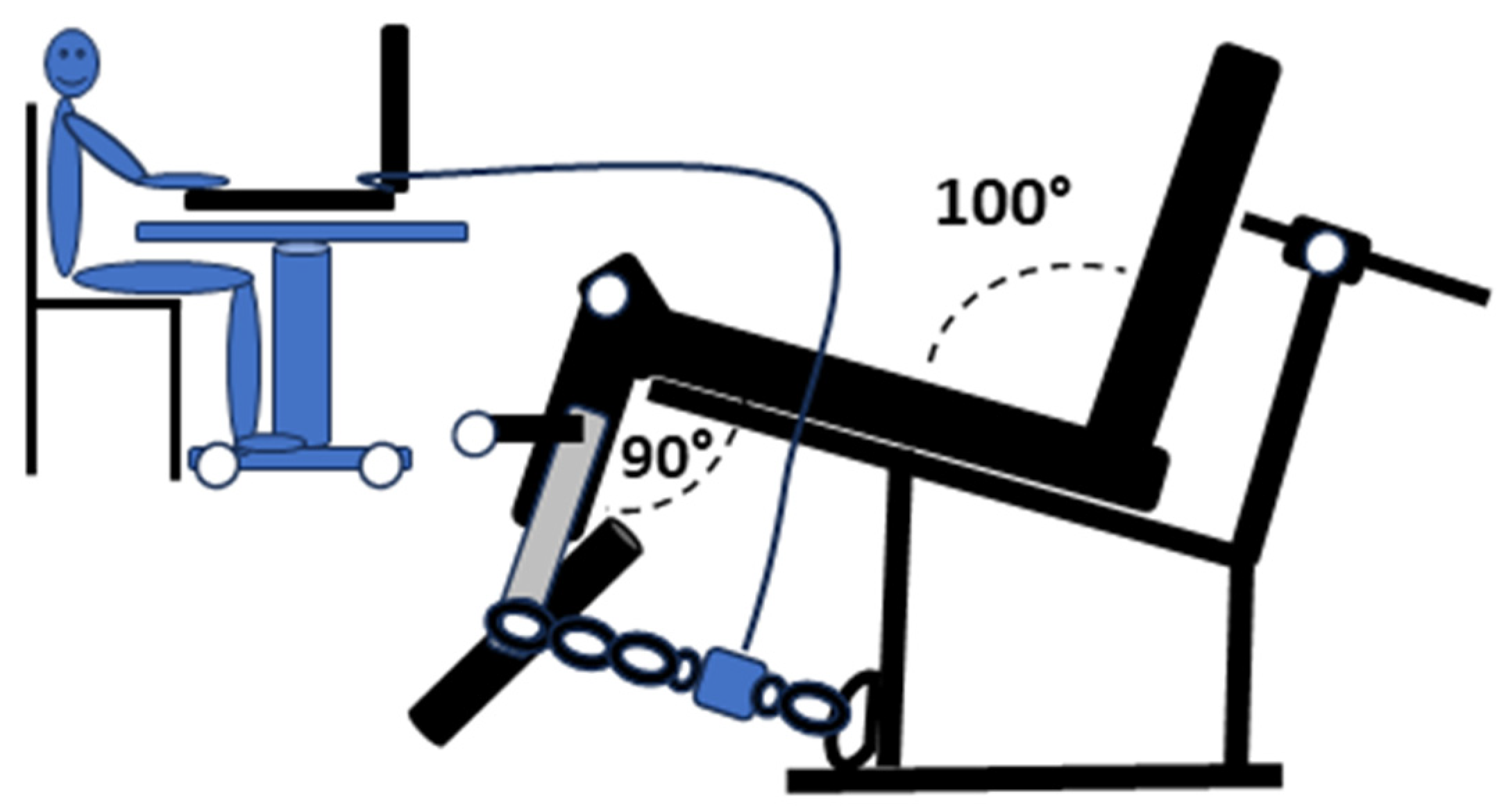
2.3. Determination of Maximum Voluntary Isometric Contraction (MVIC)
2.4. One-Repetition Maximum (1RM) Assessment
2.5. Statistical Analysis
- (a)
- To estimate the correlation between MVIC and 1RM, an exact test for a two-tailed bivariate correlation was selected, with an effect size (ρ) of 0.5, α = 0.05, and 1-β = 0.8, yielding a minimum sample size of 46 participants.
- (b)
- For the intra-session reliability and MDC determination, a two-tailed paired t-test was chosen, with Cohen’s d = 0.5, α = 0.05, and 1-β = 0.80, resulting in a minimum sample size of 34 participants.
- (c)
- To assess the predictive value of MVIC for 1RM, an F-test for multiple linear regression (fixed model, R2 increase) was selected, with an effect size (f2) of 1.77 (80% variance explained), a single predictor (MVIC), α = 0.05, and 1-β = 0.80, yielding a minimum sample size of 47 participants. All statistical analyses were performed using SPSS 25.0 (IBM Inc., Chicago, IL, USA).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MVIC | Maximum Voluntary Isometric Contraction |
| 1RM | One-Repetition Maximum |
| ICC | Intraclass Correlation Coefficient |
| SEM | Standard Error of Measurement |
| MDC | Minimal Detectable Change |
| R2 | Coefficient of Determination |
| p | p-value |
| SG | Study Group |
| VG | Validation Group |
| BMI | Body Mass Index |
| Min | Minimum |
| Max | Maximum |
| CV | Coefficient of Variation |
| SEE | Standard Error of Estimate |
| Δ | Absolute Percentage Error |
| d | Cohen’s d |
References
- Finni, T.; de Brito Fontana, H.; Maas, H. Force Transmission and Interactions between Synergistic Muscles. J. Biomech. 2023, 152, 111575. [Google Scholar] [CrossRef] [PubMed]
- Suwa, M.; Imoto, T.; Kida, A.; Iwase, M.; Yokochi, T. Age-Related Reduction and Independent Predictors of Toe Flexor Strength in Middle-Aged Men. J. Foot Ankle Res. 2017, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Pabla, P.; Jones, E.J.; Piasecki, M.; Phillips, B.E. Skeletal Muscle Dysfunction with Advancing Age. Clin. Sci. 2024, 138, 863–882. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.; Engelhardt, M. Strength and Muscle Mass Loss with Aging Process. Age and Strength Loss. Muscles Ligaments Tendons J. 2013, 3, 346–350. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Shailendra, P.; Baldock, K.L.; Li, L.S.K.; Bennie, J.A.; Boyle, T. Resistance Training and Mortality Risk: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2022, 63, 277–285. [Google Scholar] [CrossRef]
- Paluch, A.E.; Boyer, W.R.; Franklin, B.A.; Laddu, D.; Lobelo, F.; Lee, D.C.; Mcdermott, M.M.; Swift, D.L.; Webel, A.R.; Lane, A. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation 2024, 149, E217–E231. [Google Scholar] [CrossRef]
- Marques, D.L.; Neiva, H.P.; Marinho, D.A.; Nunes, C.; Marques, M.C. Load-Velocity Relationship in the Horizontal Leg-Press Exercise in Older Women and Men. Exp. Gerontol. 2021, 151, 111391. [Google Scholar] [CrossRef]
- Huang, C.C.; Wang, H.H.; Chen, K.C.; Yang, K.J.; Chang, L.Y.; Shiang, T.Y.; Lin, T.C. Effects of a Dynamic Combined Training on Impulse Response for Middle-Aged and Elderly Patients with Osteoporosis and Knee Osteoarthritis: A Randomized Control Trial. Aging Clin. Exp. Res. 2021, 33, 115–123. [Google Scholar] [CrossRef]
- Mayhew, J.L.; Johnson, B.D.; Lamonte, M.J.; Lauber, D.; Kemmler, W. Accuracy of Prediction Equations for Determining One Repetition Maximum Bench Press in Women before and after Resistance Training. J. Strength. Cond. Res. 2008, 22, 1570–1577. [Google Scholar] [CrossRef]
- Kurobe, Y.; Momose, K. Use of Force–Velocity Relationship to Estimate the One-Repetition Maximum Leg Press Exercise among Young Females. J. Phys. Ther. Sci. 2023, 35, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Burgess, L.C.; Taylor, P.; Wainwright, T.W.; Swain, I.D. Strength and Endurance Deficits in Adults with Moderate-to-Severe Hip Osteoarthritis, Compared to Healthy, Older Adults. Disabil. Rehabil. 2022, 44, 5563–5570. [Google Scholar] [CrossRef] [PubMed]
- Hansford, H.J.; Parmenter, B.J.; McLeod, K.A.; Wewege, M.A.; Smart, N.A.; Schutte, A.E.; Jones, M.D. The Effectiveness and Safety of Isometric Resistance Training for Adults with High Blood Pressure: A Systematic Review and Meta-Analysis. Hypertens. Res. 2021, 44, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Portilla-Cueto, K.; Medina-Pérez, C.; Romero-Pérez, E.M.; Núñez-Othón, G.; Horta-Gim, M.A.; de Paz, J.A. Muscle Quality of Knee Extensors Based on Several Types of Force in Multiple Sclerosis Patients with Varying Degrees of Disability. Medicina 2022, 58, 316. [Google Scholar] [CrossRef]
- Vona, M.; Codeluppi, G.M.; Iannino, T.; Ferrari, E.; Bogousslavsky, J.; Von Segesser, L.K. Effects of Different Types of Exercise Training Followed by Detraining on Endothelium-Dependent Dilation in Patients with Recent Myocardial Infarction. Circulation 2009, 119, 1601–1608. [Google Scholar] [CrossRef]
- Medina-Perez, C.; de Souza-Teixeira, F.; Fernandez-Gonzalo, R.; Hernandez-Murua, J.A.; de Paz-Fernandez, J.A. Effects of High-Speed Power Training on Muscle Strength and Power in Patients with Multiple Sclerosis. J. Rehabil. Res. Dev. 2016, 53, 359–368. [Google Scholar] [CrossRef]
- Warneke, K.; Wagner, C.M.; Keiner, M.; Hillebrecht, M.; Schiemann, S.; Behm, D.G.; Wallot, S.; Wirth, K. Maximal Strength Measurement: A Critical Evaluation of Common Methods—A Narrative Review. Front. Sports Act. Living 2023, 5, 1105201. [Google Scholar] [CrossRef]
- Sung, K.S.; Yi, Y.G.; Shin, H.I. Reliability and Validity of Knee Extensor Strength Measurements Using a Portable Dynamometer Anchoring System in a Supine Position. BMC Musculoskelet. Disord. 2019, 20, 320. [Google Scholar] [CrossRef]
- Hartog, J.; Dijkstra, S.; Fleer, J.; van der Harst, P.; Mariani, M.A.; van der Woude, L.H.V. A Portable Isometric Knee Extensor Strength Testing Device: Test-Retest Reliability and Minimal Detectable Change Scores of the Q-Force II in Healthy Adults. BMC Musculoskelet. Disord. 2021, 22, 966. [Google Scholar] [CrossRef]
- Grootswagers, P.; Vaes, A.M.M.; Hangelbroek, R.; Tieland, M.; van Loon, L.J.C.; de Groot, L.C.P.G.M. Relative Validity and Reliability of Isometric Lower Extremity Strength Assessment in Older Adults by Using a Handheld Dynamometer. Sports Health 2022, 14, 899–905. [Google Scholar] [CrossRef]
- Tan, A.E.L.; Grisbrook, T.L.; Minaee, N.; Williams, S.A. Predicting 1 Repetition Maximum Using Handheld Dynamometry. PM R 2018, 10, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.T.; Quach, P.T.M.; McGraw, M.; Preus, R.I.; Barefoot, R.C.; Lancaster, W.C.; Ponder, J.; Singh, H. Using Isometric Squat Strength to Predict Concentric and Eccentric Squat Strength in Young and Older Adults. Physiother. Res. Int. 2025, 30, e70034. [Google Scholar] [CrossRef] [PubMed]
- Portilla-Cueto, K.; Medina-Pérez, C.; Romero-Pérez, E.M.; Hernández-Murúa, J.A.; Vila-Chã, C.; de Paz, J.A. Reliability of Isometric Muscle Strength Measurement and Its Accuracy Prediction of Maximal Dynamic Force in People with Multiple Sclerosis. Medicina 2022, 58, 948. [Google Scholar] [CrossRef] [PubMed]
- Kassiano, W.; Costa, B.; Nunes, J.P.; Cyrino, L.T.; Nascimento, M.A.; Tomeleri, C.; Antunes, M.; Gobbo, L.A.; Ribeiro, A.S.; Coelho-e-Silva, M.J.; et al. Muscular Strength and Skeletal Muscle Mass in 511 Physically Independent Older Women Aged 60–88 Years. Exp. Gerontol. 2022, 166, 111867. [Google Scholar] [CrossRef]
- Neugarten, B.L. Dynamics of Transition of Middle Age to Old Age. Adaptation and the Life Cycle. J. Geriatr. Psychiatry 1970, 4, 71–100. [Google Scholar]
- Campos-Nonato, I.; Galván-Valencia, Ó.; Hernández-Barrera, L.; Oviedo-Solís, C.; Barquera, S. Prevalencia de Obesidad y Factores de Riesgo Asociados En Adultos Mexicanos: Resultados de La Ensanut 2022. Salud Publica Mex. 2023, 65, s238–s247. [Google Scholar] [CrossRef]
- Hartmann, A.; Knols, R.; Murer, K.; De Bruin, E.D. Reproducibility of an Isokinetic Strength-Testing Protocol of the Knee and Ankle in Older Adults. Gerontology 2009, 55, 259–268. [Google Scholar] [CrossRef]
- Jenkins, N.D.M.; Buckner, S.L.; Bergstrom, H.C.; Cochrane, K.C.; Goldsmith, J.A.; Housh, T.J.; Johnson, G.O.; Schmidt, R.J.; Cramer, J.T. Reliability and Relationships among Handgrip Strength, Leg Extensor Strength and Power, and Balance in Older Men. Exp. Gerontol. 2014, 58, 47–50. [Google Scholar] [CrossRef]
- Ordway, N.R.; Hand, N.; Briggs, G.; Ploutz-Snyder, L.L. Reliability of Knee and Ankle Strength Measures in an Older Adult Population. J. Strength. Cond. Res. 2006, 20, 82–87. [Google Scholar] [CrossRef]
- Parraca, J.A.; Adsuar, J.C.; Domínguez-Muñoz, F.J.; Barrios-Fernandez, S.; Tomas-Carus, P. Test-Retest Reliability of Isokinetic Strength Measurements in Lower Limbs in Elderly. Biology 2022, 11, 802. [Google Scholar] [CrossRef]
- Swales, B.; Ryde, G.C.; Fletcher, I.; Whittaker, A.C. The Reliability and Suitability of Strength Assessments in Frail and Pre-Frail Older Adults: Recommendations for Strength Testing in Older Populations. BMC Geriatr. 2023, 23, 820. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kamide, N.; Kitai, Y.; Ando, M.; Sato, H.; Yoshitaka, S.; Sakamoto, M. Absolute Reliability of Measurements of Muscle Strength and Physical Performance Measures in Older People with High Functional Capacities. Eur. Geriatr. Med. 2019, 10, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful Change and Responsiveness in Common Physical Performance Measures in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Godi, M.; Franchignoni, F.; Caligari, M.; Giordano, A.; Turcato, A.M.; Nardone, A. Comparison of Reliability, Validity, and Responsiveness of the Mini- BESTest and Berg Balance Scale in Patients with Balance Disorders. Phys. Ther. 2013, 93, 158–167. [Google Scholar] [CrossRef]
- de Oliveira, M.P.B.; Calixtre, L.B.; da Silva Serrão, P.R.M.; de Oliveira Sato, T.; de Medeiros Takahashi, A.C.; de Andrade, L.P. Reproducibility of Isokinetic Measures of the Knee and Ankle Muscle Strength in Community-Dwelling Older Adults without and with Alzheimer’s Disease. BMC Geriatr. 2022, 22, 940. [Google Scholar] [CrossRef]
- Keshavarzi, F.; Azadinia, F.; Talebian, S.; Rasouli, O. Test-Retest Reliability of a Load Cell Setup, Ito, and Timed Loaded Standing Tests for Measuring Muscle Strength and Endurance in Older Adults with and without Hyperkyphosis. Musculoskelet. Sci. Pract. 2022, 58, 102475. [Google Scholar] [CrossRef]
- Jenkins, N.D.M.; Cramer, J.T. Reliability and Minimum Detectable Change for Common Clinical Physical Function Tests in Sarcopenic Men and Women. J. Am. Geriatr. Soc. 2017, 65, 839–846. [Google Scholar] [CrossRef]
- Dos’Santos, T.; Thomas, C.; Comfort, P.; McMahon, J.J.; Jones, P.A.; Oakley, N.P.; Young, A.L. Between-Session Reliability of Isometric Midthigh Pull Kinetics and Maximal Power Clean Performance in Male Youth Soccer Players. J. Strength. Cond. Res. 2018, 32, 3364–3372. [Google Scholar] [CrossRef]
- Sahu, P.K.; Goodstadt, N.; Ramakrishnan, A.; Silfies, S.P. Test-Retest Reliability and Concurrent Validity of Knee Extensor Strength Measured by a Novel Device Incorporated into a Weight Stack Machine vs. Handheld and Isokinetic Dynamometry. PLoS ONE 2024, 19, e0301872. [Google Scholar] [CrossRef]
- Wang, C.Y.; Olson, S.L.; Protas, E.J. Test-Retest Strength Reliability: Hand-Held Dynamometry in Community-Dwelling Elderly Fallers. Arch. Phys. Med. Rehabil. 2002, 83, 811–815. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement from the National Strength and Conditioning Association. J. Strength. Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Fetherstonhaugh, D.; Winbolt, M. Perceived Barriers and Enablers to Conducting Nursing Assessments in Residential Aged Care Facilities in Victoria, Australia. Aust. J. Adv. Nurs. 2019, 36, 14–22. [Google Scholar] [CrossRef]
- Bertani, R.F.; Bonardi, J.M.; De Campos, G.; Lima, L.G.; Ferriolli, E.; Moriguti, J.C.; Da Costa Lima, N.K. One Repetition Maximum Test in Octogenarian: Evaluation of Blood Pressure. J. Sports Med. Phys. Fit. 2017, 57, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Lovell, D.I.; Cuneo, R.; Gass, G.C. The Blood Pressure Response of Older Men to Maximum and Sub-Maximum Strength Testing. J. Sci. Med. Sport. 2011, 14, 254–258. [Google Scholar] [CrossRef]
- Boraczyński, M.; Boraczyński, T.; Podstawski, R.; Wójcik, Z.; Gronek, P. Relationships between Measures of Functional and Isometric Lower Body Strength, Aerobic Capacity, Anaerobic Power, Sprint and Countermovement Jump Performance in Professional Soccer Players. J. Hum. Kinet. 2020, 75, 161–175. [Google Scholar] [CrossRef]
- McGuigan, M.R.; Newton, M.J.; Winchester, J.B.; Nelson, A.G. Relationship between Isometric and Dynamic Strength in Recreationally Trained Men. J. Strength. Cond. Res. 2010, 24, 2570–2573. [Google Scholar] [CrossRef]
- McGuigan, M.R.; Winchester, J.B. The Relationship between Isometric and Dynamic Strength in College Football Players. J. Sports Sci. Med. 2008, 7, 101–105. [Google Scholar] [CrossRef]

{kind=link}
| Variable | All (n = 82) | Study Group (n = 41) | Validation Group (n = 41) | p | d | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Min | Max | Mean | ± | SD | Min | Max | Mean | ± | SD | Min | Max | ||||
| Age (years) | 66.9 | ± | 4.1 | 60.0 | 75.0 | 66.9 | ± | 4.2 | 60.0 | 75.0 | 67.0 | ± | 4.0 | 60.0 | 74.0 | 0.98 | 0.01 | |
| Weight (kg) | 71.2 | ± | 11.4 | 49.5 | 96.6 | 71.0 | ± | 11.5 | 49.5 | 96.3 | 71.3 | ± | 11.3 | 52.8 | 96.6 | 0.92 | 0.02 | |
| Height (m) | 1.6 | ± | 0.1 | 1.4 | 1.8 | 1.57 | ± | 0.06 | 1.43 | 1.70 | 1.56 | ± | 0.05 | 1.45 | 1.75 | 0.78 | 0.06 | |
| BMI (kg/m2) | 29.0 | ± | 4.7 | 20.6 | 42.4 | 28.8 | ± | 4.6 | 20.6 | 41.7 | 29.2 | ± | 4.8 | 21.9 | 42.4 | 0.73 | 0.08 | |
| MVIC (kg) | 49.9 | ± | 10.5 | 31.4 | 72.5 | 48.2 | ± | 9.3 | 31.4 | 66.1 | 51.5 | ± | 11.5 | 34.5 | 72.5 | 0.16 | 0.31 | |
| 1RM (kg) | 42.5 | ± | 11.5 | 20.0 | 70.0 | 41.1 | ± | 10.9 | 21.0 | 60.0 | 43.9 | ± | 12.0 | 20.0 | 70.0 | 0.28 | 0.24 | |
| MVIC | Mean (kg) | SD | ICC | Confidence Interval 95% | CV (%) | SEM (kg) | SEM (%) | MDC (kg) | MDC (%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Test 1 | 48.6 | 10.7 | 0.960 | (0.937 | 0.974) | 3.2 | 2.1 | 4.3 | 5.8 | 11.9 | |
| Test 2 | 49.3 | 10.4 | ||||||||||
| Slope | Intercept (Beta) | R | R2 | SEE (kg) | |
|---|---|---|---|---|---|
| Study group | 0.932 | −3.852 | 0.786 | 0.618 | 6.9 |
| Groups | Measured_1RM (kg) | Estimated_1RM (kg) | p-1 | △ (%) | p-2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study group | 41.1 | ± | 10.9 | 41.1 | ± | 8.6 | 0.996 | 14.6 | ± | 17.2 | 0.758 |
| Validation group | 43.9 | ± | 12.0 | 44.2 | ± | 10.7 | 0.791 | 13.4 | ± | 17.3 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Murúa, J.A.; Romero-Pérez, E.M.; Guajardo-Cruztitla, J.L.; Olivares, B.S.M.; Gallego-Selles, Á.; González-Martín, D.; Reyes-Merino, F.; Sánchez-García, N.; de Paz, J.A. Intra-Session Reliability and Predictive Value of Maximum Voluntary Isometric Contraction for Estimating One-Repetition Maximum in Older Women: A Randomised Split-Sample Study. J. Funct. Morphol. Kinesiol. 2025, 10, 160. https://doi.org/10.3390/jfmk10020160
Hernández-Murúa JA, Romero-Pérez EM, Guajardo-Cruztitla JL, Olivares BSM, Gallego-Selles Á, González-Martín D, Reyes-Merino F, Sánchez-García N, de Paz JA. Intra-Session Reliability and Predictive Value of Maximum Voluntary Isometric Contraction for Estimating One-Repetition Maximum in Older Women: A Randomised Split-Sample Study. Journal of Functional Morphology and Kinesiology. 2025; 10(2):160. https://doi.org/10.3390/jfmk10020160
Chicago/Turabian StyleHernández-Murúa, José Aldo, Ena Monserrat Romero-Pérez, Jorge Luis Guajardo-Cruztitla, Blas Sinahí Madrigal Olivares, Ángel Gallego-Selles, Diego González-Martín, Francisca Reyes-Merino, Nidia Sánchez-García, and José Antonio de Paz. 2025. "Intra-Session Reliability and Predictive Value of Maximum Voluntary Isometric Contraction for Estimating One-Repetition Maximum in Older Women: A Randomised Split-Sample Study" Journal of Functional Morphology and Kinesiology 10, no. 2: 160. https://doi.org/10.3390/jfmk10020160
APA StyleHernández-Murúa, J. A., Romero-Pérez, E. M., Guajardo-Cruztitla, J. L., Olivares, B. S. M., Gallego-Selles, Á., González-Martín, D., Reyes-Merino, F., Sánchez-García, N., & de Paz, J. A. (2025). Intra-Session Reliability and Predictive Value of Maximum Voluntary Isometric Contraction for Estimating One-Repetition Maximum in Older Women: A Randomised Split-Sample Study. Journal of Functional Morphology and Kinesiology, 10(2), 160. https://doi.org/10.3390/jfmk10020160