
Optimizing Recovery Strategies in Elite Speedskating: A Comparative Analysis of Different Modalities

 , , , ,
, , , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.2.1. Measurements
2.2.2. Exercise Procedure
2.2.3. Recovery Procedures
2.3. Statistical Analysis
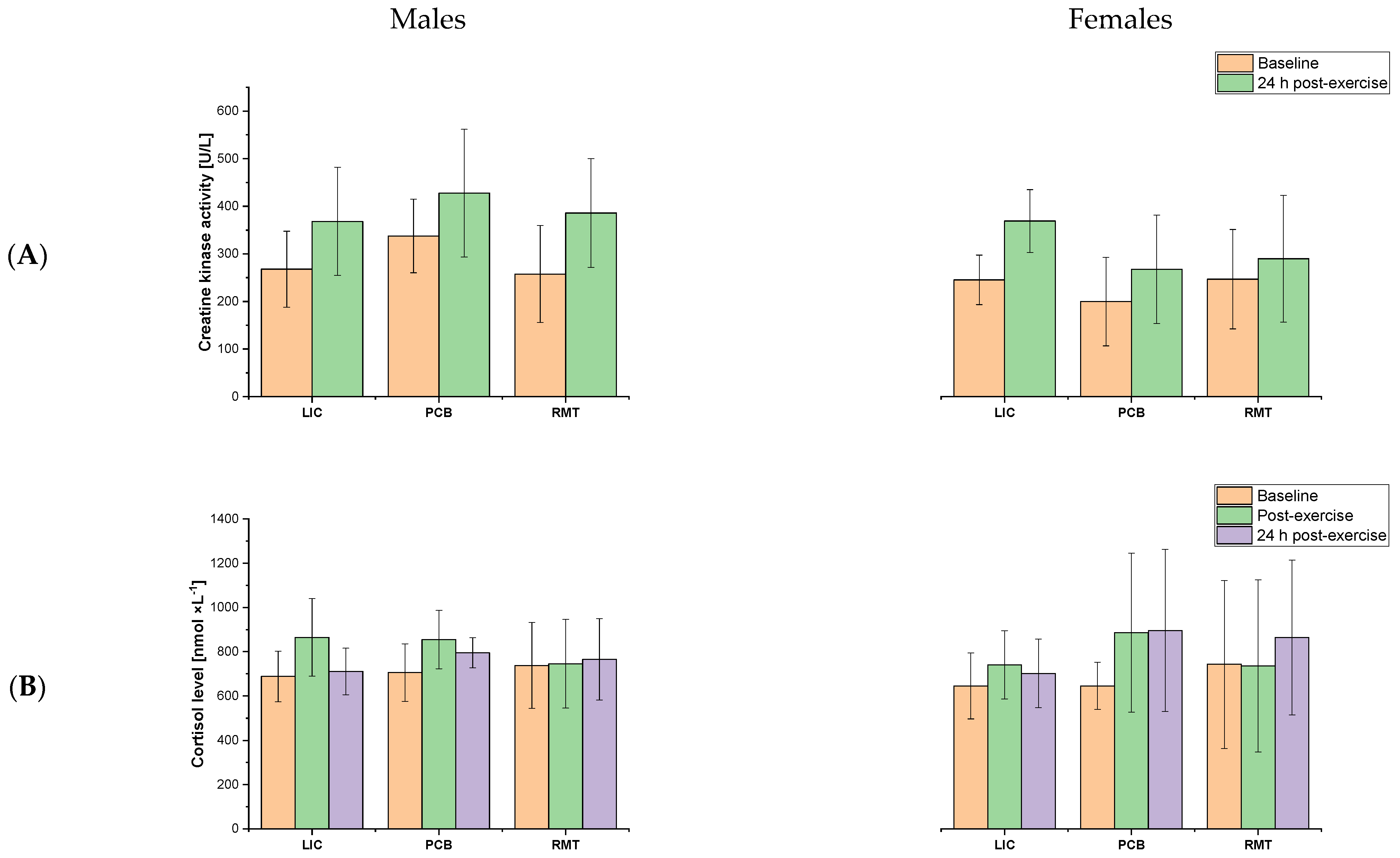
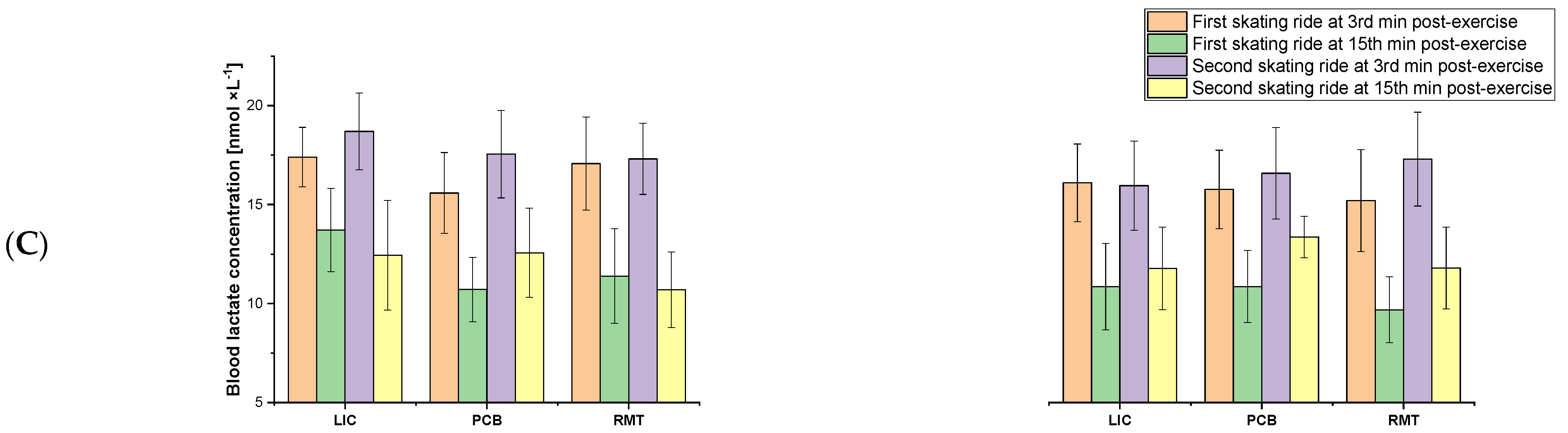
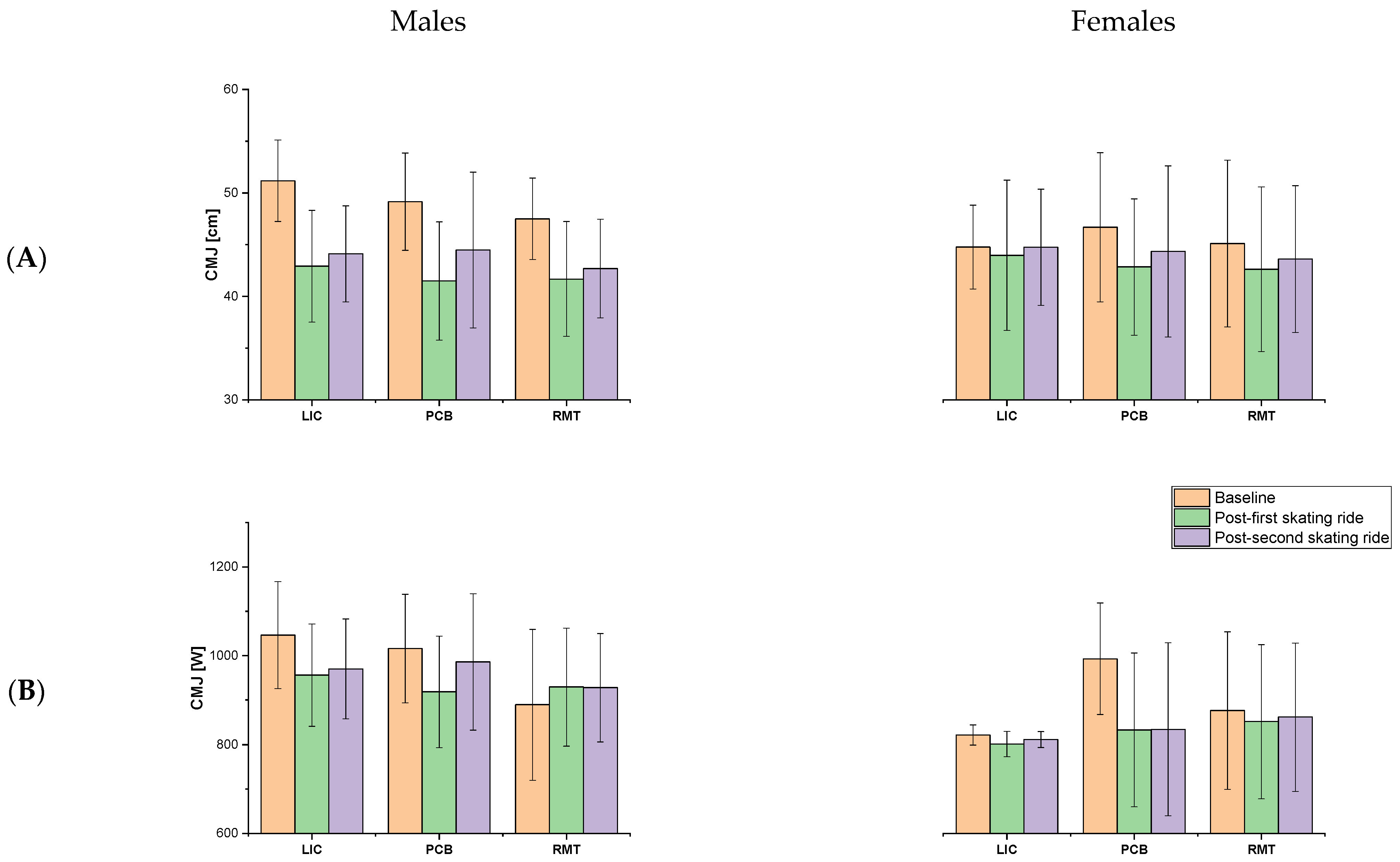
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bullock, N.; Martin, T.D.; Zhang, A. Performance analysis of world class short track speed skating: What does it take to win? Int. J. Perform. Anal. Sport 2008, 8, 9–18. [Google Scholar] [CrossRef]
- Hettinga, F.J.; Konings, M.J.; Cooper, C.E. Differences in Muscle Oxygenation, Perceived Fatigue and Recovery between Long-Track and Short-Track Speed Skating. Front. Physiol. 2016, 7, 619. [Google Scholar] [CrossRef]
- Rundell, K.W. Compromised oxygen uptake in speed skaters during treadmill in-line skating. Med. Sci. Sports Exerc. 1996, 28, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.C.; Fragala, M.S.; Kavouras, S.A.; Queen, R.M.; Pryor, J.L.; Casa, D.J. Biomarkers in Sports and Exercise: Tracking Health, Performance, and Recovery in Athletes. J. Strength Cond. Res. 2017, 31, 2920–2937. [Google Scholar] [CrossRef]
- Mika, A.; Mika, P.; Fernhall, B.; Unnithan, V.B. Comparison of recovery strategies on muscle performance after fatiguing exercise. Am. J. Phys. Med. Rehabil. 2007, 86, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Koizumi, K.; Sukeno, S.; Manabe, M.; Nomura, J. Active recovery effects by previously inactive muscles on 40-s exhaustive cycling. J. Sports Sci. 2009, 27, 1145–1151. [Google Scholar] [CrossRef]
- Koizumi, K.; Fujita, Y.; Muramatsu, S.; Manabe, M.; Ito, M.; Nomura, J. Active recovery effects on local oxygenation level during intensive cycling bouts. J. Sports Sci. 2011, 29, 919–926. [Google Scholar] [CrossRef]
- Hill, J.; Howatson, G.; van Someren, K.; Leeder, J.; Pedlar, C. Compression garments and recovery from exercise-induced muscle damage: A meta-analysis. Br. J. Sports Med. 2014, 48, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, S.; Driller, M.W. The effect of intermittent sequential pneumatic compression on recovery between exercise bouts in well-trained triathletes. J. Sci. Cycl. 2015, 4, 19–23. [Google Scholar]
- Overmayer, R.G.; Driller, M.W. Pneumatic Compression Fails to Improve Performance Recovery in Trained Cyclists. Int. J. Sports Physiol. Perform. 2018, 13, 490–495. [Google Scholar] [CrossRef]
- Wisniowski, P.; Cieslinski, M.; Jarocka, M.; Kasiak, P.S.; Makaruk, B.; Pawliczek, W.; Wiecha, S. The Effect of Pressotherapy on Performance and Recovery in the Management of Delayed Onset Muscle Soreness: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2077. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Xu, Y.; Yang, Y.; Xiao, S.; Fu, W. Effectiveness of Using Compression Garments in Winter Racing Sports: A Narrative Review. Front. Physiol. 2020, 11, 970. [Google Scholar] [CrossRef]
- Konieczny, M.; Matuska, J.; Pakosz, P.; Domaszewski, P.; Skulska, M.; Herrero, P.; Skorupska, E. Resting muscle tension and trigger points in elite junior short-track athletes and healthy non-athletes: A cross-sectional examination. Front. Sports Act. Living 2024, 6, 1412412. [Google Scholar] [CrossRef]
- Chleboun, G.S.; Howell, J.N.; Baker, H.L.; Ballard, T.N.; Graham, J.L.; Hallman, H.L.; Perkins, L.E.; Schauss, J.H.; Conatser, R.R. Intermittent pneumatic compression effect on eccentric exercise-induced swelling, stiffness, and strength loss. Arch. Phys. Med. Rehabil. 1995, 76, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, T.; Granda, D.; Klusiewicz, A. Practical Application of Respiratory Muscle Training in Endurance Sports. Strength Cond. J. 2024, 46, 686–695. [Google Scholar] [CrossRef]
- Romer, L.M.; McConnell, A.K.; Jones, D.A. Effects of inspiratory muscle training upon recovery time during high intensity, repetitive sprint activity. Int. J. Sports Med. 2002, 23, 353–360. [Google Scholar] [CrossRef]
- Brown, P.I.; Sharpe, G.R.; Johnson, M.A. Inspiratory muscle training reduces blood lactate concentration during volitional hyperpnoea. Eur. J. Appl. Physiol. 2008, 104, 111–117. [Google Scholar] [CrossRef]
- Kowalski, T.; Wilk, A.; Rebis, K.; Lohse, K.M.; Sadowska, D.; Klusiewicz, A. Influence of voluntary isocapnic hyperpnoea on recovery after high-intensity exercise in elite short-track speedskaters—Randomized controlled trial. BMC Sports Sci. Med. Rehabil. 2024, 16, 137. [Google Scholar] [CrossRef]
- Spengler, C.M.; Roos, M.; Laube, S.M.; Boutellier, U. Decreased exercise blood lactate concentrations after respiratory endurance training in humans. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 79, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Fregosi, R.F.; Dempsey, J.A. Effects of exercise in normoxia and acute hypoxia on respiratory muscle metabolites. J. Appl. Physiol. 1986, 60, 1274–1283. [Google Scholar] [CrossRef] [PubMed]
- Hopper, S.I.; Murray, S.L.; Ferrara, L.R.; Singleton, J.K. Effectiveness of diaphragmatic breathing for reducing physiological and psychological stress in adults: A quantitative systematic review. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 1855–1876. [Google Scholar] [CrossRef] [PubMed]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, P. Convenience sampling. BMJ 2013, 347, f6304. [Google Scholar] [CrossRef]
- Tesch, P.A.; Wright, J.E. Recovery from short term intense exercise: Its relation to capillary supply and blood lactate concentration. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 52, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Claudino, J.G.; Cronin, J.; Mezencio, B.; McMaster, D.T.; McGuigan, M.; Tricoli, V.; Amadio, A.C.; Serrao, J.C. The countermovement jump to monitor neuromuscular status: A meta-analysis. J. Sci. Med. Sport 2017, 20, 397–402. [Google Scholar] [CrossRef]
- Laurent, C.M.; Green, J.M.; Bishop, P.A.; Sjokvist, J.; Schumacker, R.E.; Richardson, M.T.; Curtner-Smith, M. A practical approach to monitoring recovery: Development of a perceived recovery status scale. J. Strength Cond. Res. 2011, 25, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Williams, N. The Borg Rating of Perceived Exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Hicks, A.L.; Kent-Braun, J.; Ditor, D.S. Sex Differences in Human Skeletal Muscle Fatigue. Exerc. Sport Sci. Rev. 2001, 29, 109–112. [Google Scholar] [CrossRef]
- Billaut, F.; Bishop, D. Muscle fatigue in males and females during multiple-sprint exercise. Sports Med. 2009, 39, 257–278. [Google Scholar] [CrossRef]
- Spencer, M.; Bishop, D.; Dawson, B.; Goodman, C. Physiological and metabolic responses of repeated-sprint activities:specific to field-based team sports. Sports Med. 2005, 35, 1025–1044. [Google Scholar] [CrossRef]
- Hinzpeter, J.; Zamorano, A.; Cuzmar, D.; Lopez, M.; Burboa, J. Effect of active versus passive recovery on performance during intrameet swimming competition. Sports Health 2014, 6, 119–121. [Google Scholar] [CrossRef]
- Milia, R.; Roberto, S.; Pinna, M.; Palazzolo, G.; Sanna, I.; Omeri, M.; Piredda, S.; Migliaccio, G.; Concu, A.; Crisafulli, A. Physiological responses and energy expenditure during competitive fencing. Appl. Physiol. Nutr. Metab. 2014, 39, 324–328. [Google Scholar] [CrossRef]
- Meline, T.; Solsona, R.; Antonietti, J.P.; Borrani, F.; Candau, R.; Sanchez, A.M. Influence of post-exercise hot-water therapy on adaptations to training over 4 weeks in elite short-track speed skaters. J. Exerc. Sci. Fit. 2021, 19, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Chiappa, G.R.; Roseguini, B.T.; Alves, C.N.; Ferlin, E.L.; Neder, J.A.; Ribeiro, J.P. Blood lactate during recovery from intense exercise: Impact of inspiratory loading. Med. Sci. Sports Exerc. 2008, 40, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Stanley, W.C. Myocardial lactate metabolism during exercise. Med. Sci. Sports Exerc. 1991, 23, 920–924. [Google Scholar] [CrossRef]
- Zaccaro, A.; Piarulli, A.; Laurino, M.; Garbella, E.; Menicucci, D.; Neri, B.; Gemignani, A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front. Hum. Neurosci. 2018, 12, 353. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, T.; Obminski, Z.; Walerianczyk, W.; Klusiewicz, A. The acute effect of respiratory muscle training on cortisol, testosterone, and testosterone-to-cortisol ratio in well-trained triathletes—Exploratory study. Respir. Physiol. Neurobiol. 2025, 331, 104353. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalski, T.; Rębiś, K.; Malczewska-Lenczowska, J.; Klusiewicz, A.; Starczewski, M.; Klich, S.; Kasiak, P. Optimizing Recovery Strategies in Elite Speedskating: A Comparative Analysis of Different Modalities. J. Funct. Morphol. Kinesiol. 2025, 10, 34. https://doi.org/10.3390/jfmk10010034
Kowalski T, Rębiś K, Malczewska-Lenczowska J, Klusiewicz A, Starczewski M, Klich S, Kasiak P. Optimizing Recovery Strategies in Elite Speedskating: A Comparative Analysis of Different Modalities. Journal of Functional Morphology and Kinesiology. 2025; 10(1):34. https://doi.org/10.3390/jfmk10010034
Chicago/Turabian StyleKowalski, Tomasz, Kinga Rębiś, Jadwiga Malczewska-Lenczowska, Andrzej Klusiewicz, Michał Starczewski, Sebastian Klich, and Przemysław Kasiak. 2025. "Optimizing Recovery Strategies in Elite Speedskating: A Comparative Analysis of Different Modalities" Journal of Functional Morphology and Kinesiology 10, no. 1: 34. https://doi.org/10.3390/jfmk10010034
APA StyleKowalski, T., Rębiś, K., Malczewska-Lenczowska, J., Klusiewicz, A., Starczewski, M., Klich, S., & Kasiak, P. (2025). Optimizing Recovery Strategies in Elite Speedskating: A Comparative Analysis of Different Modalities. Journal of Functional Morphology and Kinesiology, 10(1), 34. https://doi.org/10.3390/jfmk10010034