Abstract
Skeletal muscle has multiple functions and is a key component of the locomotor system. It consists of carbohydrates and amino acids for different tissues such as skin, heart and brain. It contributes to the maintenance of blood glucose levels during periods of starvation. Skeletal muscle health is particularly important for the prevention of various diseases. This review discusses various aspects of skeletal muscle tissue including its development, structure, function and morphology, including the guidelines for histology methods. We have also discussed, sarcopenia, age-related muscle diseases and exercise. We hope this review will benefit readers of a clinical and non-clinical background.
1. Introduction
Muscle tissue includes skeletal muscle, myocardium and smooth muscle. Skeletal muscle forms the vast majority of our muscle tissue. It constitutes of 40% of the body weight and contains 50%–75% of the body’s proteins. Skeletal muscle has multiple functions. It is a key component of the locomotor system. It has the ability to convert the chemical energy into mechanical energy therefore generating movement. Therefore, a subject can be independent and able to carry out daily activities. Skeletal muscle is also a reserve of carbohydrates and amino acids for different tissues such as skin, heart and brain [1].
Skeletal muscle contributes to the maintenance of blood glucose levels during periods of starvation [2]. The secondary disability to impaired skeletal muscle is particularly debilitating. The good maintenance of skeletal muscle health is crucial for the prevention of various diseases and the psychological stress due to the disability. Our review discusses skeletal muscle development, structure, function, and morphology as well as guidelines for histology, exercise and sarcopenia and age-related muscle diseases.
2. Development of Skeletal Muscle Fibers
Skeletal muscle originates mainly from paraxial mesoderm arranged in somites, responsible for metameric organization of the body, in many animal species including humans. The somites are arranged in pairs along the longitudinal axis of the embryo. Although they are transitory structures, they are extremely important for organization of the segmental plan of vertebrates [3,4,5]. They originate at regular and cyclic species-specific intervals. The temporal periodicity is regulated by expression of the “oscillating genes” and by gradients of signal molecules responsible for a wave motion, including fibroblast growth factor 8 (FGF-8), WNTA3 protein and retinoic acid (RA) [3,6]. In every somite, it is possible to identify an internal mesenchymal mass and an epithelial lining, which is formed in consequence of the mesenchymal-epithelial transition (MET) regulated by fibronectin, N-cadherin and a small GTPase (Rac1) [7,8]. The somites are detached from one another and subsequently due to local molecular signals, they differentiate into three portions: sclerotome, myotome and dermatome. The differentiation process depends on interactions with the surrounding tissues and is regulated by signal molecules from ectoderm, notochord and neural tube [9]. With regard to the development of skeletal muscle, the myotome cells separate, migrate in the appropriate areas and generate myoblasts. Some progenitor cells do not differentiate in order to give rise to satellite cells located at the periphery of the muscle cells. This is responsible for both postnatal growth of skeletal muscle and possible repair processes [10]. Myogenesis is the muscle differentiation process that involves the proliferation of myoblasts, followed by their mutual fusion in order to form polynuclear syncytia, expressing the characteristic proteins of muscle tissue. The complex mechanism of myogenesis is regulated by the MyoD family, belonging to the class of basic helix loop helix (bHLH) transcription factors, and by hormones and growth factors such as arginine, vasopressin (AVP) and insulin-like growth factor-I (IGF-I) [11,12]. Myogenesis involves several stages: specification, determination and differentiation. Specification is characterized by intra- and extracellular processes that cause mesodermal cells to respond to molecular signals by which the myoblasts are generated. Differentiation includes the synthesis of the myofibrillar proteins (actin, myosin and tropomyosin), the increased activity of intracellular enzymes (creatine phosphokinase and glycogen phosphorylase) and the synthesis of acetylcholinesterase and acetylcholine receptor (AchR). Once differentiated, myoblasts do not proliferate more, but secrete fibronectin in the extracellular matrix and then bind it [13,14]. The link between myoblasts and fibronectin allows the formation of myoblast chains [14,15,16]. Now myoblasts can fuse together to form myotubes, set to become skeletal muscle fibers. Fusion of myoblasts includes the production of myoblast-myoblast pre-fusion complexes, characterized by fragmentation of cell membrane and rearrangement of cytoskeleton. This is followed by pores formation in the membrane cells that allow the exchange of cytoplasmic materials [14]. Both side-to-side and end-to-end interactions are important in fusion, because if lateral movement is inhibited, fusion is significantly reduced. Lastly, closing of the juxtaposed membranes occurs because of the proteins myoferlin and dysferlin [15,16] (Figure 1).
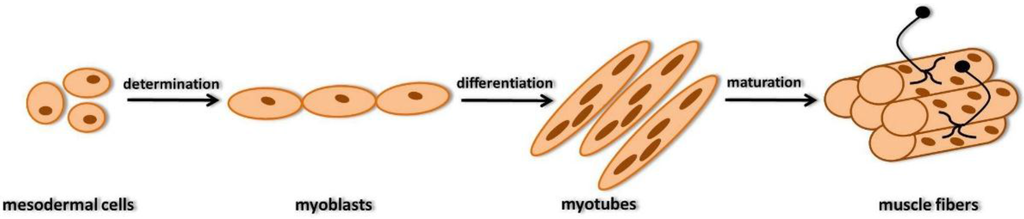
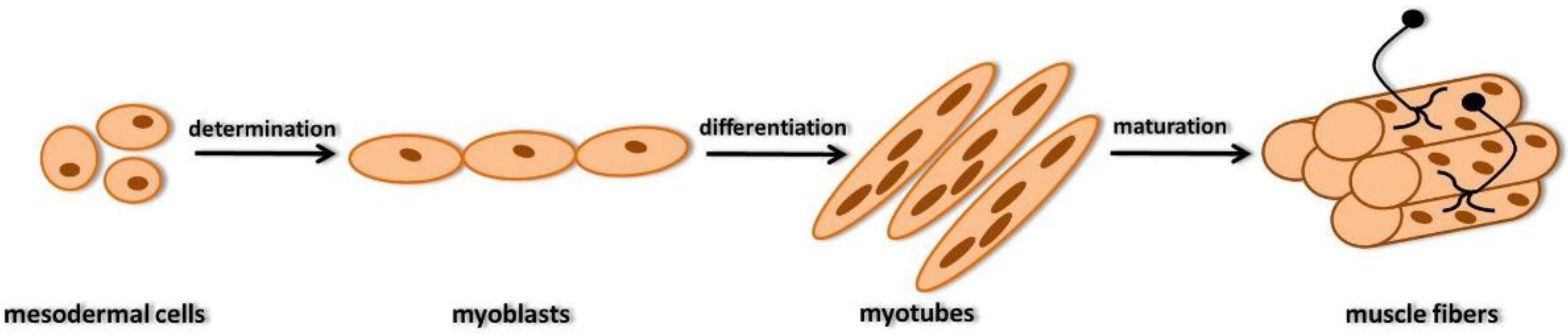
Figure 1.
Scheme of myogenesis: determination gives the competence to mesodermal cells to differentiate myoblasts; differentiation includes molecular processes such as synthesis of actin, myosin, tropomyosin and secretion of fibronectin, causing myoblasts chains to form, through end-to-end and side-to-side interactions, in order to fuse each other to form myotubes; maturation in which transverse banding and sarcomeres appear and become excitable and able to contract.
The further growth of myotubes is because of the ulterior synthesis of contractile proteins, in particular myosin, but also other proteins such as creatine kinase and troponin. The final stage of myogenesis is the maturation of muscle fiber, namely the appearance of transverse banding and sarcomeres that after a few days become excitable and able to contract. In humans, at the end of the 8th week of pregnancy most of the myotubes are differentiated into muscle fiber [17,18]. Moreover, in developing myotubes, the sarcoplasmic reticulum develops and the sarcoplasmic membrane invaginates to produce transverse tubules. Lastly, the synapses develop due to the presence of AchR on the surface of myotubes. In the early stages of embryonic development, each skeletal muscle fiber is innervated by at least two motor neurons. As the multiple innervation disappears, every fiber receives a single motor neuron with the selection based on competition between axons [19].
3. Structure and Function
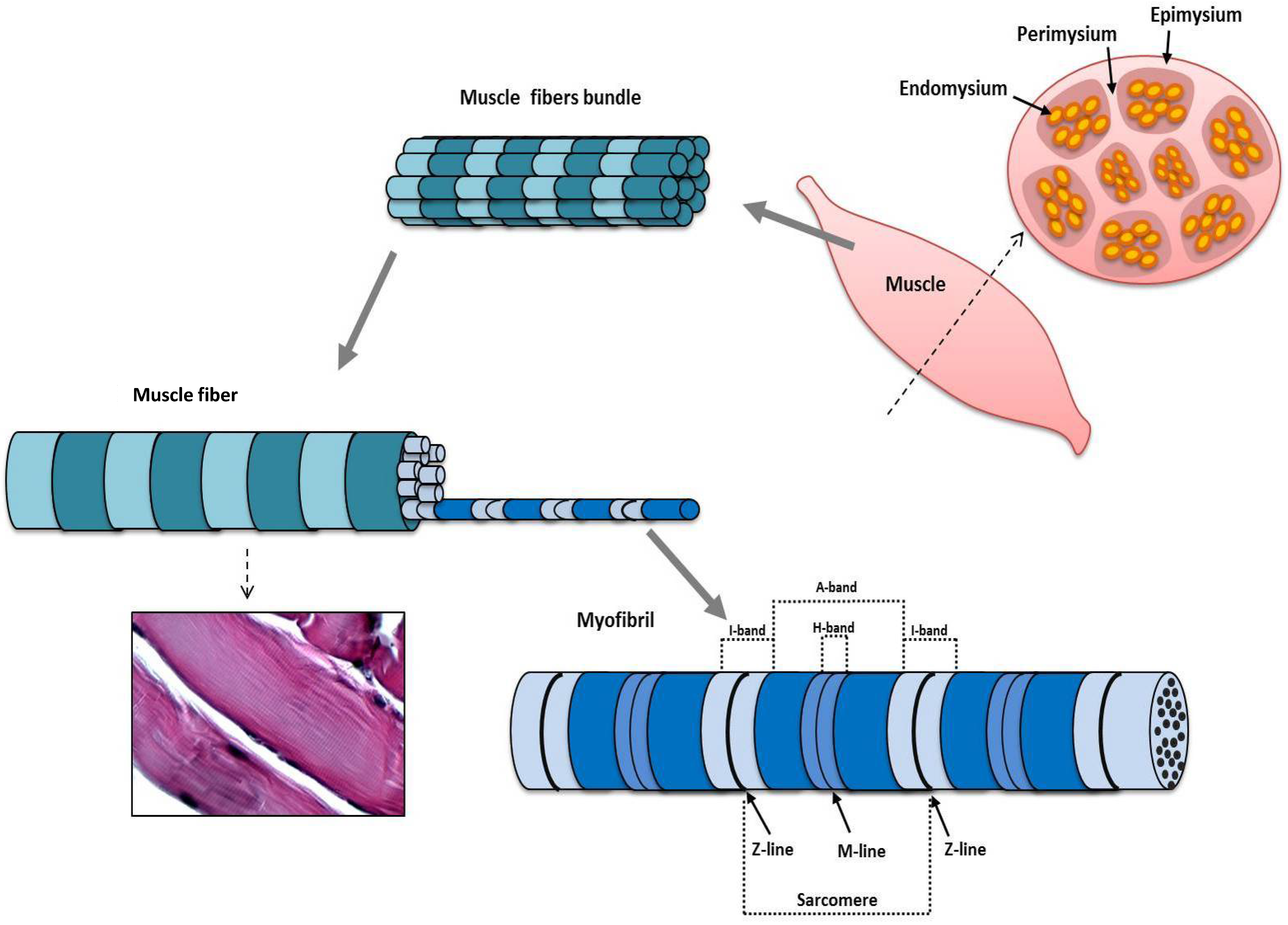
Skeletal muscle is composed of a variable number of muscle fibers and is surrounded by connective tissue, the epimysium, which is connected to the tendon, the structure responsible for the insertion of the muscle to the bone segment. Connective tissue septa originate from epimysium and surround groups of muscle fibers, forming the perimysium. Each muscle fiber (approximate dimensions of 100 μm in diameter and 1 cm in length) is surrounded by reticular connective tissue, which constitutes the endomysium [20]. The epimysium, perimysium and endomysium vascularize and innerve the muscle. The single muscle fiber originates from the fusion of a large number of myoblasts to form a polynuclear syncytium. Satellite cells are adherent to the sarcolemma of muscle fibers, contributing to muscle growth, repair, and regeneration [2]. The sarcoplasm has all cytoplasmic organelles, but consists mostly of myofibrils that, occupying most of the available space, push the numerous nuclei at the periphery of the muscle fiber [21]. The myofibrils are aligned along the longitudinal axis of the muscle fiber and are linked to each other, with the sarcolemma and other cytoplasmic organelles due to several cytoskeletal proteins such as plectin, filamin and dystrophin. Alterations in the seproteins are linked to neuromuscular disorders such as Duchenne and Becker muscular dystrophies [22]. The muscle fiber is characterized by a typical cross-banding that is the result of a well-defined arrangement of myofibrils in the sarcoplasm. Myofibrils consist of myofilaments that are arranged in a well-defined order responding functionally to the contractile function. There are two types of myofilaments, thick and thin, arranged in a well-defined order responsible for the typical cross-banding. The thick myofilaments, consisting of bundles of myosin molecules, are arranged parallel to each other and constitute the A-band, which contains the entire length of a single thick filament. Its central part is called the H-band, which indicates the zone of the thick filaments that is not superimposed by the thin filaments. Myosin is a hexameric protein and is characterized by the ability to bind actin to form actomyosin complex, and is an ATPase able, and therefore able to provide the energy required for contraction. The thin myofilaments are structurally composed of actin filaments (F-actin), which are arranged parallel to each other and determine the I-band, where the thin filaments are not superimposed by thick filaments, and the A-emibands. Moreover, they are regulatory proteins associated with thin filaments, such as tropomyosin and troponin, which have a fundamental regulatory role in the contraction mechanism. Overall, the myofibril consists of an alternation of A-I bands, with the H-band in the middle of A-band, in which only thick myofilaments are present; the A-emibands in which both myosin and actin are present to form actomyosin complex; the M line in the middle of H-band where tails of myosin molecules are connected each other; the Z line in the middle of I-band, in which the thin myofilaments of adjacent sarcomeres (see down) are linked among them. The fragment of myofibril delimited by two Z lines is called sarcomere, which is the functional unit of the muscle fiber, and is able to contract through the sliding of the thin filaments on thick ones (Figure 2).
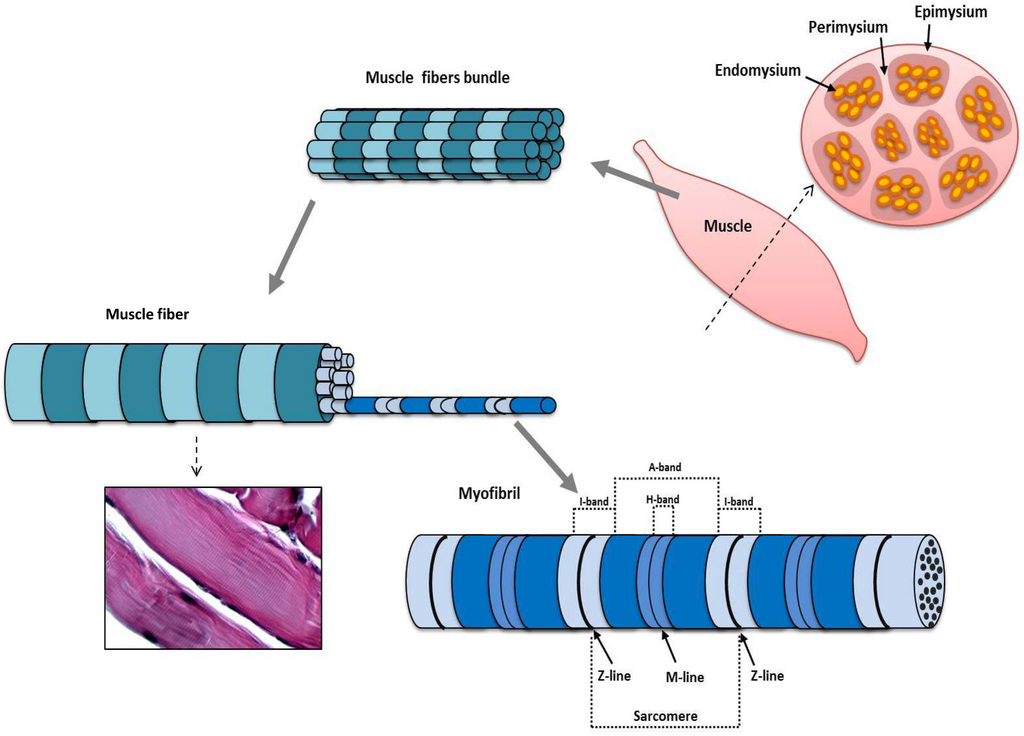
Figure 2.
Morphology of skeletal muscle. Epimysium is the connective tissue surrounding the entire skeletal muscle. Perimysium consists of connective septa from epimysium surrounding bundles of muscle fibers. Endomysium is reticular connective tissue surrounding each muscle fiber. The sarcoplasm of the single muscle fiber is filled with myofibrils aligned along the longitudinal axis of the muscle fiber. Myofibrils consist of myofilaments arranged in a well-defined order responsible for the typical cross-banding consisting of A-band, with the central H-band consisting of only thick myofilaments, and I-band, composed by thin myofilaments, incorporating the Z line. The sarcomere is the fragment of myofibril delimited by two Z lines, and it is the functional unit of the muscle fiber that is able to contract. In the Hematoxylin & Eosin (H&E) longitudinal section (20×) the cross-banding, consisting of alternated A-bands (dark) and I-bands (light), is slightly evident.
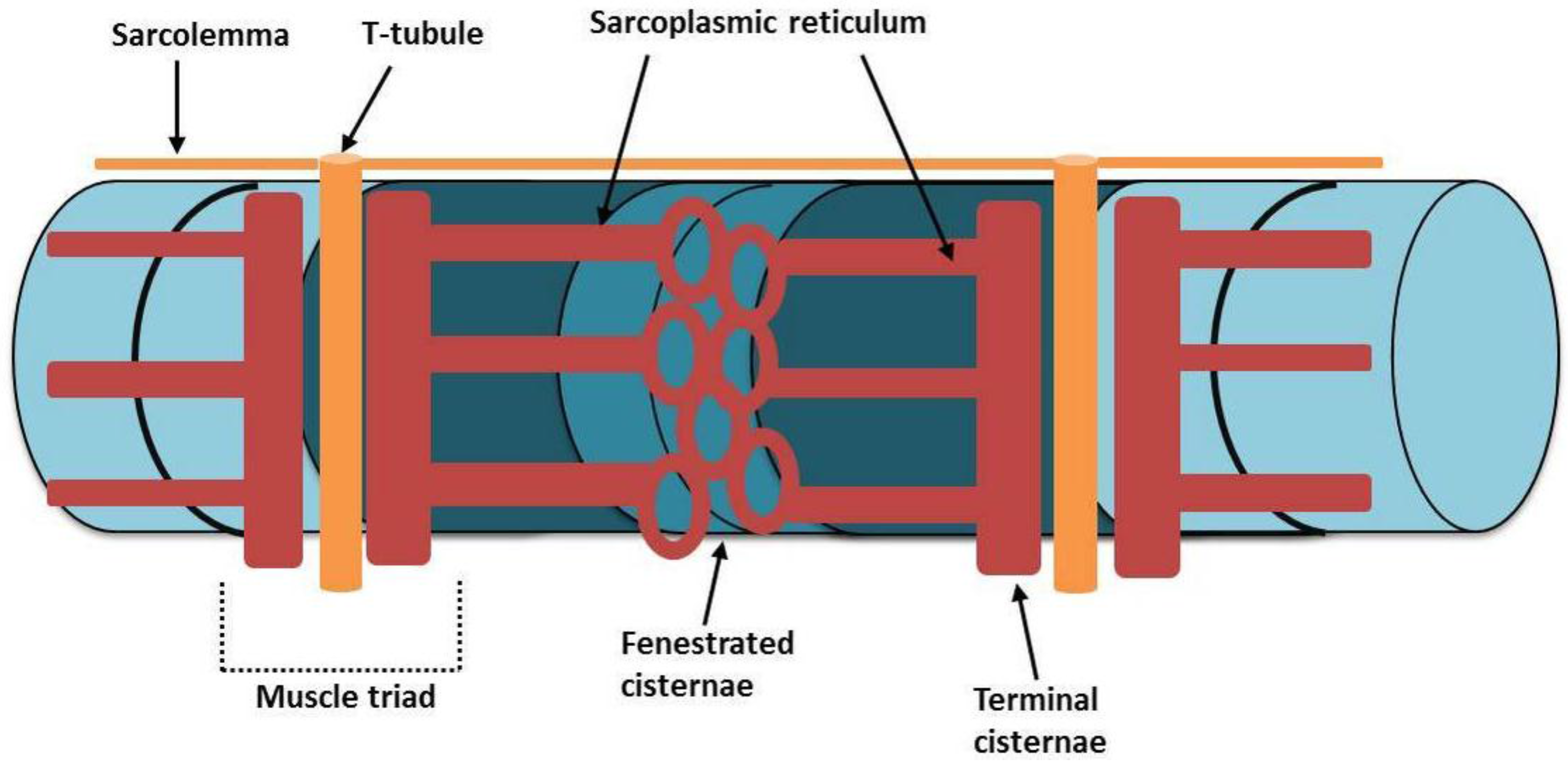
Thanks to the bond of the thin filaments of adjacent sarcomeres at the level of the Z line, the simultaneous contraction of individual sarcomeres results in the contraction of the entire muscle fiber [23]. The well-defined arrangement of the myofilaments is supported by the presence of several cytoskeletal proteins such as titin and nebulin that contribute to the stability and integrity of the sarcomere [23,24]. The contraction of the myofibrils is possible by the presence of sarcolemmal and sarcoplasmic structures that allow the excitation-contraction coupling. In fact, the mechanism of contraction is triggered by Ca++ ions that bind to troponin, and in particular to C sub-unit, allowing the sliding of thin myofilaments on thick ones. The muscle fiber is rich in Ca++ ions, collected and stored in the sarcoplasmic reticulum. This is a modified smooth endoplasmic reticulum, arranged in tubules enveloping the myofibrils. In particular, the sarcoplasmic reticulum is divided into fenestrated cisternae and terminal cisternae; the latter have a horizontal pattern and retain the Ca++ ions that will be released when a nerve impulse comes, making them available to binding to C troponin, thus triggering the mechanism of contraction [25]. The release of Ca++ ions from the terminal cisternae is allowed by sarcolemmal structures, namely the transverse tubule (T-tubule) that is an invagination of the sarcolemma, whose role is the conduction of the nerve action potential to the interior of the cell. The T-tubules are associated with the terminal cisternae, so that the action potential from the nerve fiber associated, can be transmitted to the terminal cisternae, which, thus, release the Ca++ ions. The association between one T-tubule and two terminal cisternae constitute the so-called muscles triad [26] (Figure 3).

Figure 3.
The sarcoplasmic reticulum is a modified smooth endoplasmic reticulum, arranged in tubules enveloping the myofibrils, divided into fenestrated cisternae and terminal cisternae. In the latter, the Ca++ ions are stored and released when a nerve impulse comes. Transverse tubules (T-tubules) are invaginations of the sarcolemma having the role of the nerve action potential conduction in order to permit the release of Ca++ ions from the terminal cisternae. Muscles triad is the association between one T-tubule and two terminal cisternae.
Lastly, the mitochondria allow concretely the sliding of thin myofilaments on thick ones and, therefore, the contraction of the sarcomeres. Indeed, the mitochondria form a three-dimensional network throughout the cell, generating the required chemical energy (ATP), subsequently transformed into mechanical energy by the ATPase activity of myosin [27]. In Humans, skeletal muscles are heterogeneous depending on the predominance of the various fiber types. These latter can be distinguished: type I, rich in mitochondria and myoglobin (slow, oxidative, and fatigue-resistant); IIA, rich in mitochondria and myoglobin, but also in glycogen and therefore also capable of anaerobic glycolysis (fast, oxidative, and intermediate metabolic properties); and IIB, rich in glycogen and poor in mitochondria and myoglobin (fastest, glycolytic, and fatigable) [28]. The heterogeneity of human skeletal muscle could reflect an adaptation to different stimuli from the motor neurons [2].
4. Guidelines for Histology
In the histopathological analysis of skeletal muscle, different qualitative parameters such as shape and type of the muscle fiber; number and location of nuclei; any cellular infiltration; presence of fibrosis; and, even, necrosis are considered fundamental for the detection of morphological alterations. Equally important are the quantitative parameters such as the number of fibers. An increase in the number of fibers is a sign of hyperplasia. An increase in the size of single fibers is a sign of hypertrophy. Both qualitative and quantitative evaluations are usually carried out on muscle samples embedded in paraffin according to routine methods and are subsequently analyzed by light microscopy. The frozen sections, although easily perishable, may also be used and, in some cases, are preferred, as occurs in immunohistochemistry, when an antibody does not work well in paraffin. In the research field, electron microscopy is definitely the most effective technique for morphological investigation but it requires more complex procedures and equipment, which is not always available.
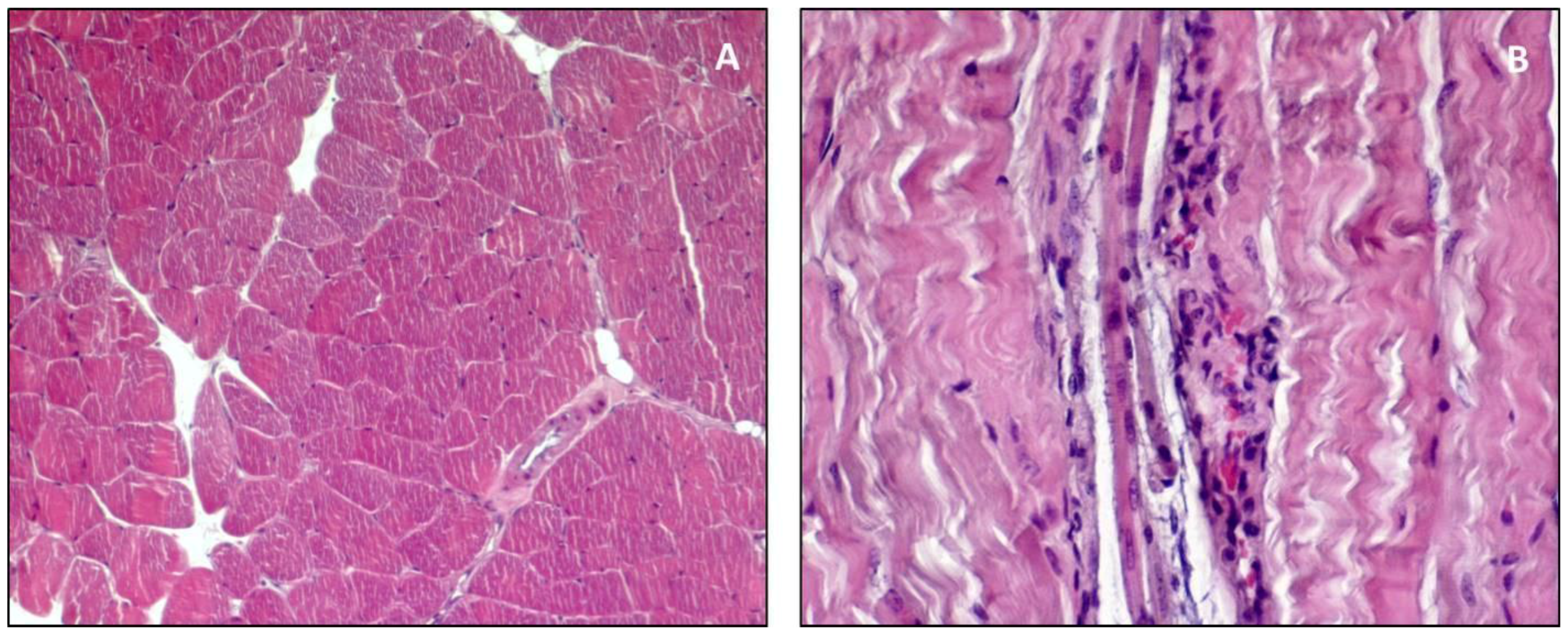
A first consideration is about the orientation of the paraffin-embedded muscle fiber sample. The cross sections are preferred because they allow the qualitative assessments, and they are necessary for the quantitative ones [29,30]. In the research field, the choice of the muscle to be analyzed is a basic step, thus the anterior tibialis is widely used because it is easily accessible, the muscle fibers have a fairly uniform orientation and also it is rich in fast fibers. The soleus is appropriate if needing to analyze slow fibers. The cross sections, about 5 μm, are stained choosing a wide range of histochemical staining. The routine histological staining is Hematoxylin & Eosin (H&E) that stains the cytoplasm in pink and the nuclei in dark purple. H&E gives general information on the morphology of the analyzed muscle tissue sufficient to detect any alterations, both qualitative and quantitative. In an H&E stained cross section, the muscle fibers of a health sample have similar size, are gathered in bundles, the nuclei are peripheral and the sarcoplasm appears uniform and unfragmented (Figure 4A); signs of necrosis are eventually evidenced by inflammatory cells infiltration (Figure 4B), hyper-contracted or degenerated myofibrils, and fragmented sarcoplasm [31]. It is possible to detect regeneration phenomena due to the presence of muscle fibers with central nuclei rather than peripheral, which demonstrate the maturation of newer myotubes.

Figure 4.
(A) H&E cross section (10×): Muscle fibers with similar size, gathered in bundles surrounded by endomysium. Peripheral nuclei stained in dark purple, sarcoplasm uniformly stained in pink. (B) H&E longitudinal section (20×): Signs of necrosis evidenced by inflammatory cells infiltration and hyper-contracted or degenerated myofibrils. Nuclei of both inflammatory cells and muscle fibers stained in dark purple, sarcoplasm stained in pink.
The H&E staining is also useful for the detection of fibrosis, even if different stainings, such as Van Gieson’s or Masson’s Trichrome, are more suitable to show fibrous connective tissue. To demonstrate the endomysium, the argentic impregnation staining, according to Gomori for reticulin, is particularly effective. The endomysium appears as thin branches of reticular connective tissue encapsulating the blood capillaries, while the muscle fibers do not appear stained. Other histochemical stainings are specific for molecules such as glycogen and lipids that are the energy source for contraction. The periodic acid-Schiff staining (PAS) is appropriate for the detection of glycogen; in this case, the sarcoplasm is diffusely stained in fuchsia. Oil Red Orcein staining highlights the neutral lipids, collected in sarcoplasmic vacuoles. In a muscle, the intensity of these stainings can vary, indicating that single muscle fibers can use different energy sources [32]. Some enzymatic stainings also need to be considered, such as that for the ATPase at pH 9.6, highlighting adenosine triphosphatase activity, which allows a more marked distinction between the type I fibers (myofibers with slow contraction and fatigue resistant) faintly stained, and the type II fibers (fast-twitch myofibers and not very resistant to fatigue) intensely stained in black. The enzymatic stainings for DPNH-diaphorase, is used for the detection of enzymatic activities related to the mitochondria and it darkly stains type I fibers, as it contains a great number of mitochondria, and faintly type II fibers, which contain a reduced number of mitochondria.
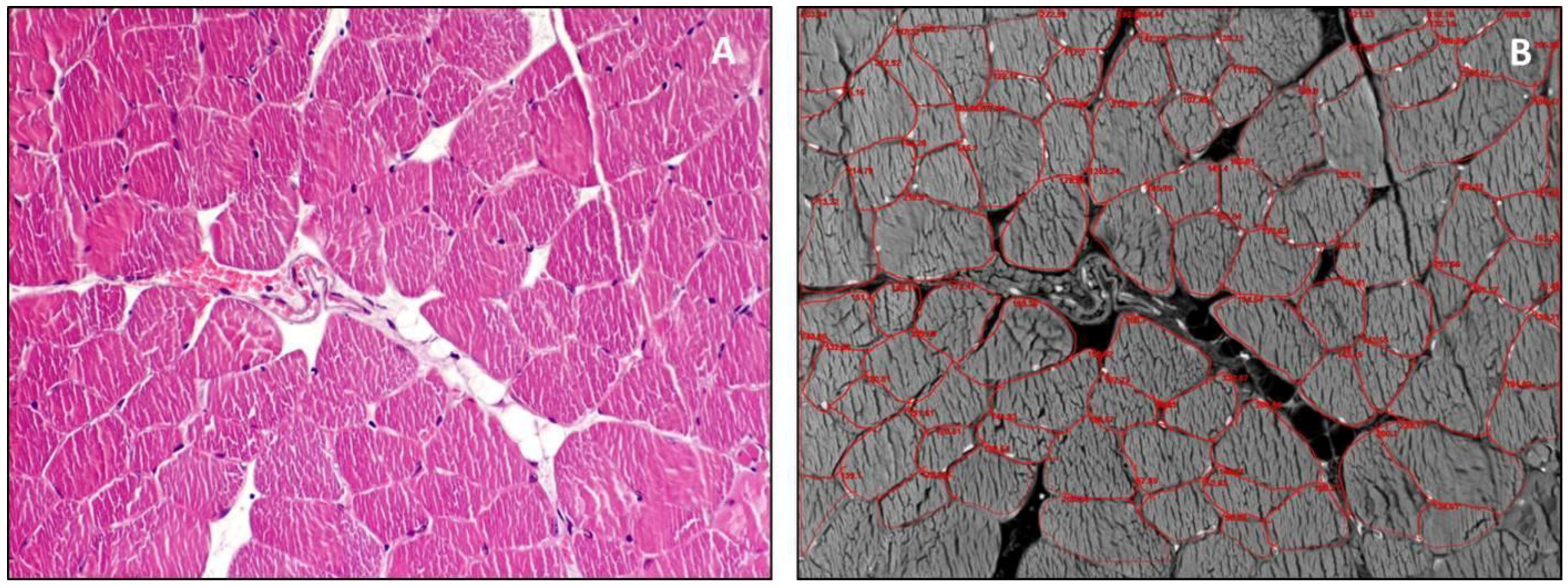
Lastly, it is necessary to consider the histomorphometric analysis that enables the quantitative assessment of a muscle sample. Indeed, this allows counting muscle fibers in a specific area of the analyzed slide, and also the muscle fiber size can be measured. In the morphometric analysis, the parameter to determine the size of the fibers is usually the diameter, the perimeter or the area (Figure 5).
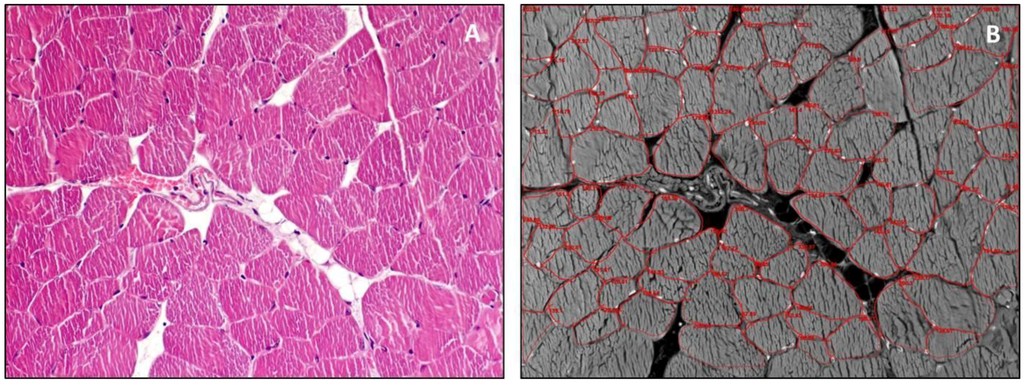
Figure 5.
(A) H&E cross section (20×) of muscle sample used for histomorphometric analysis. Peripheral nuclei stained in dark purple, sarcoplasm uniformly stained in pink; (B) Photo negative of (A) analyzed by AxioVisio software (AxioVision Release 4.8.2 SP2 Software, Carl Zeiss Microscopy GmbH, Jena, Germany) in which perimeter of each fiber is defined through a red line.
The investigator should be very careful in the choice of the section to analyze by selecting the best cross sections and avoid oblique sections, although, in this last case, the problem is avoided by measuring the minimal Feret’s diameter [31]. Currently, the histomorphometric analysis is mainly achieved through the use of software, such as AxioVision (used in our laboratory) and others such as MATLAB Application and Olympus Soft Imaging Solutions [29,30] that allow accurate measurement of parameters, giving a major impact to the scientific investigations.
5. Exercise
Physical activity induces significant structural and metabolic changes in skeletal muscle, according to the type of exercise performed. In relation to the exercise-type specificity, different molecular pathways are activated causing muscle hypertrophy and its adaptation [33]. The endurance exercise (aerobic) involves the work of a large number of muscle bundles and is a type of prolonged physical activity, without developing too much fatigue. Endurance exercise usually includes walking, running, swimming, cycling, and some team sports. Muscles undergoing an endurance training show an increased efficiency in the contraction due to structural adaptations such as a greater development of the sarcoplasmic reticulum, a greater number of mitochondria, a greater activity of the enzymes involved in the Krebs cycle and a higher content in glycogen [34,35]. Endurance exercise enhances protein synthesis, mitochondrial biogenesis and the release of interleukin-6 (IL-6), resulting in inhibition of tumor necrosis factor-α (TNF-α) production and consequent inhibition of muscle fiber apoptosis; it also may mediate anti-inflammatory and anti-atrophy effects [36,37,38,39]. However, endurance training is not associated to hypertrophy [2]. The resistance exercise (anaerobic and strength) is a type of physical activity that generates great muscular strength and induces hypertrophy of skeletal muscle fibers as a result of the confluence of positive muscle protein balance and satellite cell addition to muscle fibers [40]. Hypertrophic muscle fibers have greater dimensions as a result of increased protein synthesis exceeding the protein catabolism. Furthermore, resistance training induces activation of satellite cells, whereby the number of muscle fibers also increases [2,41,42]. Moreover, this kind of training can attenuate both fiber atrophy and pro-apoptotic signaling [36,37,43,44] and, in addition, can increase the activity of mitochondrial enzymes and decrease skeletal muscle TNF-α, thus inhibiting apoptosis of muscle fibers [36,37,43,45].
Lastly, it is important to remember that physical exercise can cause an increase in oxidative stress with production of reactive oxygen species (ROS) that often cause cellular alterations. However, at the same time, it stimulates the adaptive response of the body against oxidative stress [46], increasing the production of heat shock proteins (HSPs) in order to protect against subsequent periods of stress damage and to facilitate a rapid recovery and remodeling when damage occurs [47,48]. Moreover, it seems that when physical exercise is supported with a good quality of nutrition or with supplementation of exogenous antioxidants, it promotes the adaptation of cell antioxidant defense system much better, achieving an optimal level of defense [4,49,50]. A good quality of nutritional status can be achieved thanks to some nutrients having antioxidant properties, such as carotenoids and oleic acid. The latter is a compound of extra-virgin olive oil, a typical nutrient of the Mediterranean diet, which we recently showed its antioxidant properties not only in skeletal muscle but also in myocardium and cartilage [51,52,53].
6. Sarcopenia
Sarcopenia is a condition characterized by the loss of skeletal muscle mass and functions. The most typical symptom of sarcopenia is muscle wasting and atrophy. The muscle progressively reduces in size, and muscle fibers are replaced by fat and fibrous tissue. This causes increased oxidative stress, muscle metabolism changes, and neuromuscular junction degeneration, which causes progressive loss of muscle function and frailty [54,55]. Major study groups such as the European Working Group on Sarcopenia in Older People (EWGSOP), the European Society for Clinical Nutrition and Metabolism Special Interest Groups (ESPEN-SIG) and the International Working Group on Sarcopenia (IWGS) are working together in order to provide a clear definition of sarcopenia. It is considered to be a syndrome characterized by progressive and generalized loss of skeletal muscle mass and strength with a risk of adverse outcomes including physical disability, poor quality of life and, ultimately, death [56]. In particular, the EWGSOP has identified a number of parameters that allow identifying three different degrees of sarcopenia: presarcopenia, stage characterized by low muscle mass without impact on muscle strength or physical performance; sarcopenia, stage characterized by low muscle mass, plus low muscle strength or low physical performance; and severe sarcopenia, the stage in which all three criteria of the definition are met (low muscle mass, low muscle strength and low physical performance) [56]. This distinction in these three levels of sarcopenia can be very useful in the management of patients suffering from sarcopenia, in order to identify the most appropriate treatments to the individual case. It is also important to well identify the selection criteria for patients involved in clinical trials and to establish a core outcome set to be used in all clinical trials of sarcopenia, as reported by some authors [57]. Sarcopenia increases 14% in those aged between 65 and 70 years and 53% after 80 years. It is, therefore, a typical expression of ageing but it is not an exclusive status of the elderly. In fact, it can develop as consequence of conditions such as disuse, malnutrition and cachexia [58,59,60]. Furthermore, sarcopenia can be associated in comorbidity with other diseases such as obesity, osteoporosis, type 2 diabetes, insulin resistance and cirrhosis, and in young patients with inflammatory diseases [59,61,62,63,64]. In clinical practice, identifying the causes of sarcopenia, even if not always evident, is very useful for management and therapy of the disease. Anyway, it is crucial to distinguish sarcopenia in primary (or age-related), in which no other cause save aging itself are found, and secondary, in which one or more other causes are evident [56]. Lastly, sarcopenia needs to be distinguished from cachexia. Cachexia is a multifactorial syndrome characterized by severe body weight, fat and muscle loss and increased protein catabolism due to several diseases. Factors that determine cachexia could be anorexia and metabolic alterations such as increased muscle proteolysis and impaired carbohydrate, protein and lipid metabolism. Increased inflammatory status is also considered. Cachexia is clinically relevant since it increases patients’ morbidity and mortality [65].
7. Ageing
Ageing is characterized by a decline in physical function in daily activities resulting in reduced quality of life. The decline of motor activity is linked to muscle weakness and atrophy. Sarcopenia is one of the main indicators of ageing and, as reported above, is characterized by loss of skeletal muscle mass and strength [2,36]. The decline of muscle strength is due to the progressive decrease in anabolism with an increase in catabolism, as well as to the reduced muscle regeneration capacity [36]. In age-related sarcopenia, a reduced number of satellite cells have been highlighted [66,67]. Furthermore, the activation of satellite cells in response to muscle damage decreases in elderly [68]. In ageing, the muscle fiber is altered in many morphological characteristics as a result of molecular events involving different cytoplasmic organelle. The sarcoplasmic reticulum shows alterations that have an impact in its ability to store Ca++ ions decreasing, and, thus, its effectiveness in excitation-contraction coupling [69]. The unbalanced muscle protein turnover is associated with the quality of myofilaments [70]. For example, the reduction in myosin protein content may be related to abnormal myostatin gene transcription or reductions in translation and protein synthesis leading to a lower myosin concentration [2]. In addition, post-translational modifications of myosin may result in myofilament dysfunction [2]. Oxidative modification of myosin may disrupt the binding of the myosin head to the actin filament, reducing the number of actin-myosin cross-bridges and, thus, limiting strength and power generation [2,71]. Age-related alterations are also associated with a loss of mitochondrial content and function [72]. The unbalanced muscle protein turnover and tissue remodeling are associated with impaired muscle cell recruitment and apoptosis [73]. Apoptosis is a programmed cell death mechanism that may have an important role in aging of skeletal muscle [37,74]. Apoptotic stimuli that can be considered as initiators of the apoptotic signaling in aged skeletal muscle are several and different, among them oxidative stress, Ca++ and TNF-α [73,75]. Increased oxidative stress, typical of aging, alters the balance between degradation and resynthesis of skeletal muscle proteins [76] and also determines mitochondrial dysfunction and apoptosis by activating some major signaling pathways, leading to reduction in muscle mass and strength [37,77]. TNF-α can induce apoptosis in muscle fibers; indeed, increased synthesis of TNF-α in aged skeletal muscle is a molecular signal activating death receptors on the cell surface membrane [37,78]. Lastly, ageing is also associated with increased DNA fragmentation and cleaved caspase-3 in rat skeletal muscle [74]. Data from literature show that sarcopenia, with loss of muscle mass and strength, is higher in men when compared to women [79,80]. Furthermore, the loss of muscle strength in ageing is more evident in older people forced to immobilization; conversely, it can be less evident in relation to the level of daily physical activity [81,82].
8. Conclusions
Skeletal muscle has multiple functions and provides the basic activities of the locomotor system in daily life. Thus, good maintenance and homeostasis of skeletal muscle are fundamental for the prevention of certain diseases and psychological stress caused by possible disability. Particularly, in some pathological conditions and in ageing, physical exercise could improve performance of skeletal muscle, avoiding sarcopenia. The goal of this review is to give an overview of the morphology of skeletal muscle from development to ageing so that both clinical and non-clinical readers can improve their knowledge about skeletal muscle.
Acknowledgments
This study was supported by grants-in-aid from FIR 2014-2016, (cod. 314509), University of Catania, Italy. The funder had no role in the design of the study, collection and analysis of the data, decision to publish, or the preparation of the manuscript.
Author Contributions
Francesca Maria Trovato: Study concept and design; acquisition of data; drafting of the manuscript, critical revision of the manuscript for important intellectual content; Rosa Imbesi: Study concept and design; acquisition of data; interpretation of data; drafting of the manuscript; Nerys Conway: drafting of the manuscript; critical revision of the manuscript for important intellectual content; Paola Castrogiovanni: Study concept and design; acquisition of data; interpretation of data; drafting of the manuscript. All authors approved the final submitted version.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AchR | Acetylcholine Receptor |
| AVP | Vasopressin |
| ESPEN-SIG | European Society for Clinical Nutrition and Metabolism Special Interest Groups |
| EWGSOP | European Working Group on Sarcopenia in Older People |
| F-actin | Actin Filaments |
| FGF-8 | Fibroblast Growth Factor 8 |
| H&E | Hematoxylin & Eosin |
| IGF-I | Insulin-like Growth Factor-I |
| IL-6 | Interleukin 6 |
| IWGS | International Working Group on Sarcopenia |
| MET | Mesenchymal-Epithelial Transition |
| PAS | Periodic Acid-Schiff staining |
| RA | Retinoic Acid |
| ROS | Reactive Oxygen Species |
| TNF-α | Tumor Necrosis Factor-α |
| T-tubule | Transverse Tubule |
References
- Wolfe, R.R. The underappreciated role of muscle in health and disease. Am. J. Clin. Nutr. 2006, 84, 475–482. [Google Scholar] [PubMed]
- Frontera, W.R.; Ochala, J. Skeletal muscle: A brief review of structure and function. Calcif. Tissue Int. 2015, 96, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Aulehla, A.; Pourquiè, O. Signaling gradients during paraxial mesoderm development. Cold Spring Harb. Perspect. Biol. 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Imbesi, R.; D’Agata, V.; Musumeci, G.; Castogiovanni, P. Skeletal muscle: From development to function. Clin. Ter. 2014, 165, 47–56. [Google Scholar] [PubMed]
- Musumeci, G.; Castrogiovanni, P.; Coleman, R.; Szychlinska, M.A.; Salvatorelli, L.; Parenti, R.; Magro, G.; Imbesi, R. Somitogenesis: From somite to skeletal muscle. Acta Histochem. 2015, 117, 313–328. [Google Scholar] [CrossRef] [PubMed]
- Palmeirim, I.; Rodrigues, S.; Dale, J.K.; Maroto, M. Development on time. Adv. Exp. Med. Biol. 2008, 641, 62–71. [Google Scholar] [PubMed]
- Roy, P.; Bandyopadhyay, A. Spatio-temporally restricted expression of cell adhesion molecules during chicken embryonic development. PLoS ONE 2014, 9, e96837. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.L.; Muerdter, C.P.; Knickerbocker, A.D.; Walsh, R.M.; Zepeda-Rivera, M.A.; Depner, K.H.; Sangesland, M.; Cisneros, T.B.; Kim, J.Y.; Sanchez-Vazquez, P.; et al. Cdc42 GTPase and Rac1 GTPase act downstream of p120 catenin and require GTP exchange during gastrulation of zebrafish mesoderm. Dev. Dyn. 2012, 241, 1545–1561. [Google Scholar] [CrossRef] [PubMed]
- Dockter, J.L. Sclerotome induction and differentiation. Curr. Top. Dev. Biol. 2000, 48, 77–127. [Google Scholar] [PubMed]
- Mitchell, K.J.; Pannerec, A.; Cadot, B.; Parlakian, A.; Besson, V.; Gomes, E.R.; Marazzi, G.; Sassoon, D.A. Identification and characterization of a non-satellite cell muscle resident progenitor during postnatal development. Nat. Cell Biol. 2010, 12, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Gerhart, J.; Elder, J.; Neely, C.; Schure, J.; Kvist, T.; Knudsen, K.; George-Weinstein, M. MyoD-positive epiblast cells regulate skeletal muscle differentiation in the embryo. J. Cell Biol. 2006, 175, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, G.; Trovato, F.M.; Avola, R.; Imbesi, R.; Castrogiovanni, P. Serotonin/growth hormone/insulin-like growth factors axis on pre- and post-natal development: A contemporary review. OA Anat. 2013, 1, 12. [Google Scholar] [CrossRef]
- Yasa, I.C.; Gunduz, N.; Kilinc, M.; Guler, M.O.; Tekinay, A.B. Basal Lamina Mimetic Nanofibrous Peptide Networks for Skeletal Myogenesis. Sci. Rep. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Demonbreun, A.R.; Biersmith, B.H.; McNally, E.M. Membrane fusion in muscle development and repair. Semin. Cell Dev. Biol. 2015, 45, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Posey, A.D., Jr.; Demonbreun, A.; McNally, E.M. Ferlin proteins in myoblast fusion and muscle growth. Curr. Top. Dev. Biol. 2011, 96, 203–230. [Google Scholar] [PubMed]
- Abmayr, S.M.; Zhuang, S.; Geisbrecht, E.R. Myoblast fusion in Drosophila. Methods Mol. Biol. 2008, 475, 75–97. [Google Scholar] [PubMed]
- Walsh, F.S.; Celeste, A.J. Myostatin: A modulator of skeletal-muscle stem cells. Biochem. Soc. Trans. 2005, 33, 1513–1517. [Google Scholar] [CrossRef] [PubMed]
- Tobin, J.F.; Celeste, A.J. Myostatin, a negative regulator of muscle mass: Implications for muscle degenerative diseases. Curr. Opin. Pharmacol. 2005, 5, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, G.; Castrogiovanni, P.; Trovato, F.M.; Parenti, R.; Szychlinska, M.A.; Imbesi, R. Pregnancy, embryo-fetal development and nutrition: Physiology around fetal programming. J. Histol. Histopathol. 2015, 2. [Google Scholar] [CrossRef]
- Fortin, M.; Videman, T.; Gibbons, L.E.; Battiè, M.C. Paraspinal muscle morphology and composition: A 15-yr longitudinal magnetic resonance imaging study. Med. Sci. Sports Exerc. 2014, 46, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Greising, S.M.; Gransee, H.M.; Mantilla, C.B.; Sieck, G.C. Systems biology of skeletal muscle: Fiber type as an organizing principle WIREs. Syst. Biol. Med. 2012, 4, 457–473. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.D. Functional muscle ischemia in Duchenne and Becker muscular dystrophy. Front. Physiol. 2013, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ottenheijm, C.A.C.; Granzier, H. Lifting the nebula: Novel insights into skeletal muscle contractility. Physiology 2010, 25, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Monroy, J.A.; Powers, K.L.; Gilomre, L.A.; Uyeno, T.A.; Lindstedt, S.L.; Nishikawa, K.C. What is the role of titin in active muscle? Exerc. Sports Sci. Rev. 2012, 40, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lamboley, C.R.; Murphy, R.M.; McKenna, M.J.; Lamb, G.D. Sarcoplasmic reticulum Ca2+ uptake and leak properties, and SERCA isoform expression, in type I and type II fibres of human skeletal muscle. J. Physiol. 2014, 592, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Jayasinghe, I.D.; Launikonis, B.S. Three-dimensional reconstruction and analysis of the tubular system of vertebrate skeletal muscle. J. Cell Sci. 2013, 126, 4048–4058. [Google Scholar] [CrossRef] [PubMed]
- Dahl, R.; Larsen, S.; Dohlmann, T.L.; Qvortrup, K.; Helge, J.W.; Dela, F.; Prats, C. Three-dimensional reconstruction of the human skeletal muscle mitochondrial network as a tool to assess mitochondrial content and structural organization. Acta Physiol. 2015, 213, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Schiaffino, S.; Reggiani, C. Fiber types in mammalian skeletal muscles. Physiol. Rev. 2011, 91, 1447–1531. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Mackey, A.L.; Srikuea, R.; Esser, K.A.; Yang, L. Automated image segmentation of haematoxylin and eosin stained skeletal muscle cross-sections. J. Microsc. 2013, 252, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.R.; Barton, E.R. SMASH—Semi-automatic muscle analysis using segmentation of histology: A MATLAB application. Skelet. Muscle 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Briguet, A.; Courdier-Fruh, I.; Foster, M.; Meier, T.; Magyar, J.P. Histological parameters for the quantitative assessment of muscular dystrophy in the mdx-mouse. Neuromuscul. Disord. 2004, 14, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Flisinski, M.; Brymora, A.; Elminowska-Wenda, G.; Bogucka, J.; Walasik, K.; Stefanska, A.; Strozecki, P.; Manitius, J. Morphometric analysis of muscle fibre types in rat locomotor and postural skeletal muscles in different stages of chronic kidney disease. J. Physiol. Pharmacol. 2014, 65, 567–576. [Google Scholar] [PubMed]
- Lamon, S.; Wallace, M.A.; Russell, A.P. The STARS signaling pathway: A key regulator of skeletal muscle function. Pflugers Arch. 2014, 466, 1659–1671. [Google Scholar] [CrossRef] [PubMed]
- Seene, T.; Kaasik, P.; Alev, K. Muscle protein turnover in endurance training: A review. Int. J. Sports Med. 2011, 32, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Lira, V.A.; Greene, N.P. Exercise training-induced regulation of mitochondrial quality. Exerc. Sport Sci. Rev. 2012, 40, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, G.; Imbesi, R.; Szychlinska, M.A.; Castrogiovanni, P. Apoptosis and Skeletal Muscle in Aging. Open J. Apoptosis 2015, 4, 41–46. [Google Scholar] [CrossRef]
- Meng, S.J.; Yu, L.J. Oxidative stress, molecular inflammation and sarcopenia. Int. J. Mol. Sci. 2010, 11, 1509–1526. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Menshikova, E.V.; Ritov, V.B.; Fairfull, L.; Ferrell, R.E.; Kelley, D.E.; Goodpaster, B.H. Effects of exercise on mitochondrial content and function in aging human skeletal muscle. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 6, 1534–1540. [Google Scholar] [CrossRef]
- Phillips, S.M. A brief review of critical processes in exercise-induced muscular hypertrophy. Sports Med. 2014, 44, S71–S77. [Google Scholar] [CrossRef] [PubMed]
- Blaauw, B.; Reggiani, C. The role of satellite cells in muscle hypertrophy. J. Muscle Res. Cell Motil. 2014, 35, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Nader, G.A.; von Walden, F.; Liu, C.; Lindvall, J.; Gutmann, L.; Pistilli, E.E.; Gordon, P.M. Resistance exercise training modulates acute gene expression during human skeletal muscle hypertrophy. J. Appl. Physiol. 2014, 116, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Theou, O.; Stathokostas, L.; Roland, K.P.; Jakobi, J.M.; Patterson, C.; Vandervoort, A.A.; Jones, G.R. The effectiveness of exercise interventions for the management of frailty: A systematic review. J. Aging Res. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Kwak, H.B.; Lawler, J.M. Exercise training attenuates age-induced changes in apoptotic signaling in rat skeletal muscle. Antioxid. Redox Signal. 2006, 8, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Melov, S.; Tarnopolsky, M.A.; Beckman, K.; Felkey, K.; Hubbard, A. Resistance exercise reverses aging in human skeletal muscle. PLoS ONE 2007, 2, e465. [Google Scholar] [CrossRef] [PubMed]
- Castrogiovanni, P.; Imbesi, R. Oxidative stress and skeletal muscle in exercise. Ital. J. Anat. Embryol. 2012, 117, 107–117. [Google Scholar] [PubMed]
- Brioche, T.; Pagano, A.F.; Py, G.; Chopard, A. Muscle wasting and aging: Experimental models, fatty infiltrations, and prevention. Mol. Asp. Med. 2016, in press. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.J. Strategies for reducing oxidative damage in ageing skeletal muscle. Adv. Drug Deliv. Rev. 2009, 61, 1363–1368. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Cabrera, M.C.; Viña, J.; Ji, L.L. Interplay of oxidants and antioxidants during exercise: Implications for muscle health. Phys. Sportsmed. 2009, 37, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, G.; Szychlinska, M.A.; Mobasheri, A. Age-related degeneration of articular cartilage in the pathogenesis of osteoarthritis: Molecular markers of senescent chondrocytes. Histol. Histopathol. 2015, 30, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Castrogiovanni, P.; Imbesi, R. Muscle in exercise. Role of different fatty acids in diets. Ital. J. Anat. Embryol. 2006, 111, 199–214. [Google Scholar] [PubMed]
- Musumeci, G.; Trovato, F.M.; Pichler, K.; Weinberg, A.M.; Loreto, C.; Castrogiovanni, P. Extra-virgin olive oil diet and mild physical activity prevent cartilage degeneration in an osteoarthritis model: An in vivo and in vitro study on lubricin expression. J. Nutr. Biochem. 2013, 24, 2064–2075. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, G.; Trovato, F.M.; Imbesi, R.; Castrogiovanni, P. Effects of dietary extra-virgin olive oil on oxidative stress resulting from exhaustive exercise in rat skeletal muscle: A morphological study. Acta Histochem. 2014, 116, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Ryall, J.G.; Schertzer, J.D.; Lynch, G.S. Cellular and molecular mechanisms underlying age-related skeletal muscle wasting and weakness. Biogerontology 2008, 9, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Reginster, J.Y.; Cooper, C.; Rizzoli, R.; Kanis, J.A.; Appelboom, G.; Bautmans, I.; Bischoff-Ferrari, H.A.; Boers, M.; Brandi, M.L.; Bruyère, O.; et al. Recommendations for the conduct of clinical trials for drugs to treat or prevent sarcopenia. Aging Clin. Exp. Res. 2016, 28, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.M.; Al-Jaouni, R.; Filippi, J.; Wiroth, J.B.; Zeanandin, G.; Arab, K.; Hébuterne, X. Sarcopenia is prevalent in patients with Crohn’s disease in clinical remission. Inflamm. Bowel Dis. 2008, 14, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The healthcare costs of sarcopenia in the United States. J. Am. Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Martyn, C.N.; Cooper, C.; Sayer, A.A. Grip strength, body composition, and mortality. Int. J. Epidemiol. 2007, 36, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, C.; di Rosa, M. Modulation of myotilin and fylamin C in various muscle diseases: A microarray analysis. J. Funct. Morphol. Kinesiol. 2016, 1, 90–101. [Google Scholar] [CrossRef]
- Trovato, F.M.; Aiello, F.C.; Larocca, L.; Taylor-Robinson, S.D. The role of physical activity and nutrition in the sarcopenia of cirrhosis. J. Funct. Morphol. Kinesiol. 2016, 1, 118–125. [Google Scholar] [CrossRef]
- Jeejeebhoy, K.N. Malnutrition, fatigue, frailty, vulnerability, sarcopenia and cachexia: Overlap of clinical features. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Miljkovic, N.; Lim, J.Y.; Miljkovic, I.; Frontera, W.R. Aging of skeletal muscle fibers. Ann. Rehabil. Med. 2015, 39, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Hikida, R.S. Aging changes in satellite cells and their functions. Curr. Aging Sci. 2011, 4, 279–297. [Google Scholar] [CrossRef] [PubMed]
- McKay, B.R.; Ogborn, D.I.; Baker, J.M.; Toth, K.G.; Tarnopolsky, M.A.; Parise, G. Elevated SOCS3 and altered IL-6 signaling is associated with age-related human muscle stem cell dysfunction. Am. J. Physiol. Cell Physiol. 2013, 304, C717–C728. [Google Scholar] [CrossRef] [PubMed]
- Weisleder, N.; Brotto, M.; Komazaki, S.; Pan, Z.; Zhao, X.; Nosek, T.; Parness, J.; Takeshima, H.; Ma, J. Muscle aging is associated with compromised Ca2+ spark signaling and segregated intracellular Ca2+ release. J. Cell Biol. 2006, 174, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.S.; Toth, M.J. Myofilament protein alterations promote physical disability in aging and disease. Exerc. Sport Sci. Rev. 2013, 41, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Moen, R.J.; Klein, J.C.; Thomas, D.D. Electron paramagnetic resonance resolves effects of oxidative stress on muscle proteins. Exerc. Sport Sci. Rev. 2014, 42, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Broskey, N.T.; Greggio, C.; Boss, A.; Boutant, M.; Dwyer, A.; Schlueter, L.; Hans, D.; Gremion, G.; Kreis, R.; Boesch, C.; et al. Skeletal muscle mitochondria in the elderly: Effects of physical fitness and exercise training. J. Clin. Endocrinol. Metab. 2014, 99, 1852–1861. [Google Scholar] [CrossRef] [PubMed]
- Tudorascu, I.; Sfredel, V.; Riza, A.L.; Dănciulescu Miulescu, R.; Ianoşi, S.L.; Dănoiu, S. Motor unit changes in normal aging: A brief review. Rom. J. Morphol. Embryol. 2014, 55, 1295–1301. [Google Scholar] [PubMed]
- Leeuwenburgh, C. Role of apoptosis in sarcopenia. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 999–1001. [Google Scholar] [CrossRef] [PubMed]
- Brioche, T.; Lemoine-Morel, S. Oxidative stress, sarcopenia, antioxidant strategies and exercise: Molecular aspects. Curr. Pharm. Des. 2016, 22, 2664–2678. [Google Scholar] [CrossRef] [PubMed]
- Koopman, R.; van Loon, L.J. Aging, exercise, and muscle protein metabolism. J. Appl. Physiol. 2009, 106, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.S.; Hofer, T.; Seo, A.Y.; Leeuwenburgh, C. Molecular mechanisms of life- and health-span extension: Role of calorie restriction and exercise intervention. Appl. Physiol. Nutr. Metab. 2007, 32, 954–966. [Google Scholar] [CrossRef] [PubMed]
- Phillips, T.; Leeuwenburgh, C. Muscle fiber specific apoptosis and TNF-α signaling in sarcopenia are attenuated by life-long calorie restriction. FASEB J. 2005, 19, 668–670. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R.; Hughes, V.A.; Fielding, R.A.; Fiatarone, M.A.; Evans, W.J.; Roubenoff, R. Aging of skeletal muscle: A 12-year longitudinal study. J. Appl. Physiol. 2000, 88, 1321–1326. [Google Scholar] [PubMed]
- Yamada, M.; Moriguch, Y.; Mitani, T.; Aoyama, T.; Arai, H. Age-dependent changes in skeletal muscle mass and visceral fat area in Japanese adults from 40 to 79 years-of-age. Geriatr. Gerontol. Int. 2014, 14, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Reid, K.F.; Pasha, E.; Doros, G.; Clark, D.J.; Patten, C.; Phillips, E.M.; Frontera, W.R.; Fielding, R.A. Longitudinal decline of lower extremity muscle power in healthy and mobility-limited older adults: Influence of muscle mass, strength, composition, neuromuscular activation and single fiber contractile properties. Eur. J. Appl. Physiol. 2014, 114, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Hughes, V.A.; Frontera, W.R.; Wood, M.; Evans, W.J.; Dallal, G.E.; Roubenoff, R.; Fiatarone Singh, M.A. Longitudinal muscle strength changes in older adults: Influence of muscle mass, physical activity, and health. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, B209–B217. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).