
New-Born Screening for Spinal Muscular Atrophy: Results of a Latvian Pilot Study

 , ,
, ,
Abstract
1. Introduction
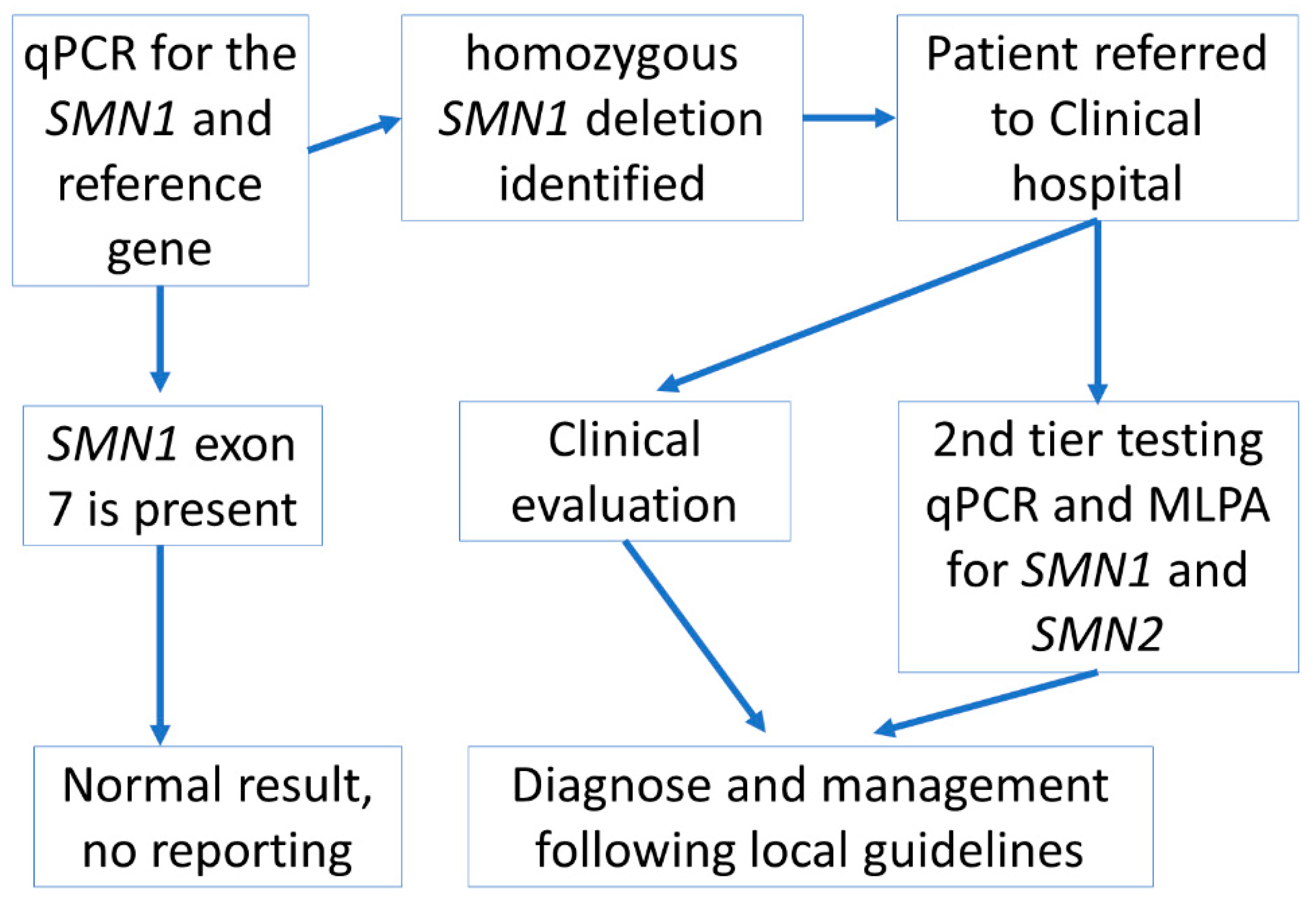
2. Subjects and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lally, C.; Jones, C.; Farwell, W.; Reyna, S.P.; Cook, S.F.; Flanders, W.D. Indirect Estimation of the Prevalence of Spinal Muscular Atrophy Type I, II, and III in the United States. Orphanet J. Rare Dis. 2017, 12, 175. [Google Scholar] [CrossRef]
- D’Amico, A.; Mercuri, E.; Tiziano, F.D.; Bertini, E. Spinal Muscular Atrophy. Orphanet J. Rare Dis. 2011, 6, 71. [Google Scholar] [CrossRef]
- Verhaart, I.E.C.; Robertson, A.; Wilson, I.J.; Aartsma-Rus, A.; Cameron, S.; Jones, C.C.; Cook, S.F.; Lochmüller, H. Prevalence, Incidence and Carrier Frequency of 5q-Linked Spinal Muscular Atrophy–A Literature Review. Orphanet J. Rare Dis. 2017, 12, 124. [Google Scholar] [CrossRef]
- Šetlere, S.; Strautmanis, J.; Rozentāls, G.; Ozolina, G.; Berķe, L.; Mičule, I. Spinālās Muskuļu Atrofijas Klīniski Epidemioloģiskais Raksturojums Latvijā. In Riga Stradins University Scientific Conference Abstract Book; Riga Stradins University: Riga, Latvia, 2018; p. 51. [Google Scholar]
- Finkel, R.S.; De Vivo, D.C.; Swoboda, K.J.; Bertini, E.; Hwu, W.-L.; Foster, R.; Bhan, I.; Fradette, S.; Farwell, W. Nusinersen in Infants Who Initiate Treatment in a Presymptomatic Stage of Spinal Muscular Atrophy (SMA): Interim Results from the Phase 2 NURTURE Study (993). Neurology 2020, 94 (Suppl. 15). Available online: https://n.neurology.org/content/94/15_Supplement/993 (accessed on 30 July 2021).
- De Vivo, D.C.; Bertini, E.; Swoboda, K.J.; Hwu, W.L.; Crawford, T.O.; Finkel, R.S.; Kirschner, J.; Kuntz, N.L.; Parsons, J.A.; Ryan, M.M.; et al. Nusinersen Initiated in Infants during the Presymptomatic Stage of Spinal Muscular Atrophy: Interim Efficacy and Safety Results from the Phase 2 NURTURE Study. Neuromuscul. Disord. 2019, 29, 842–856. [Google Scholar] [CrossRef]
- Dangouloff, T.; Vrščaj, E.; Servais, L.; Osredkar, D. Newborn Screening Programs for Spinal Muscular Atrophy Worldwide: Where We Stand and Where to Go. Neuromuscul. Disord. 2021, 31, 574–582. [Google Scholar] [CrossRef]
- Vill, K.; Kölbel, H.; Schwartz, O.; Blaschek, A.; Olgemöller, B.; Harms, E.; Burggraf, S.; Röschinger, W.; Durner, J.; Gläser, D.; et al. One Year of Newborn Screening for SMA–Results of a German Pilot Project. J. Neuromuscul. Dis. 2019, 6, 503–515. [Google Scholar] [CrossRef]
- Chien, Y.-H.; Chiang, S.-C.; Weng, W.-C.; Lee, N.-C.; Lin, C.-J.; Hsieh, W.-S.; Lee, W.-T.; Jong, Y.-J.; Ko, T.-M.; Hwu, W.-L. Presymptomatic Diagnosis of Spinal Muscular Atrophy through Newborn Screening. J. Pediatr. 2017, 190, 124–129. [Google Scholar] [CrossRef]
- Lin, Y.; Lin, C.-H.; Yin, X.; Zhu, L.; Yang, J.; Shen, Y.; Yang, C.; Chen, X.; Hu, H.; Ma, Q.; et al. Newborn Screening for Spinal Muscular Atrophy in China Using DNA Mass Spectrometry. Front. Genet. 2019, 10, 1255. [Google Scholar] [CrossRef]
- Boemer, F.; Caberg, J.H.; Dideberg, V.; Dardenne, D.; Bours, V.; Hiligsmann, M.; Dangouloff, T.; Servais, L. Newborn Screening for SMA in Southern Belgium. Neuromuscul. Disord. 2019, 29, 343–349. [Google Scholar] [CrossRef]
- Scheffer, H.; Maarten Cobben, J.; Matthijs, G.; Wirth, B. Best Practice Guidelines for Molecular Analysis in Spinal Muscular Atrophy. Eur. J. Hum. Genet. 2001, 9, 484–491. [Google Scholar] [CrossRef]
- Mercuri, E.; Finkel, R.S.; Muntoni, F.; Wirth, B.; Montes, J.; Main, M.; Mazzone, E.; Vitale, M.; Snyder, B.; Quijano-Roy, S.; et al. Diagnosis and Management of Spinal Muscular Atrophy: Part 1: Recommendations for Diagnosis, Rehabilitation, Orthopedic and Nutritional Care. Neuromuscul. Disord. 2018, 28, 103–115. [Google Scholar] [CrossRef]
- Calucho, M.; Bernal, S.; Alías, L.; March, F.; Venceslá, A.; Rodríguez-Álvarez, F.J.; Aller, E.; Fernández, R.M.; Borrego, S.; Millán, J.M.; et al. Correlation between SMA Type and SMN2 Copy Number Revisited: An Analysis of 625 Unrelated Spanish Patients and a Compilation of 2834 Reported Cases. Neuromuscul. Disord. 2018, 28, 208–215. [Google Scholar] [CrossRef]
- Cuscó, I.; Bernal, S.; Blasco-Pérez, L.; Calucho, M.; Alias, L.; Fuentes-Prior, P.; Tizzano, E.F. Practical guidelines to manage discordant situations of SMN2 copy number in patients with spinal muscular atrophy. Neurol. Genet. 2020, 6, e530. [Google Scholar] [CrossRef]
- Lāce, B.; Grīnblate, S.; Kornejeva, L.; Švābe, V.; Grauduma, I.; Vēvere, P.; Lugovska, R.; Krams, A.; Martinsons, A. Neonatal Cystic Fibrosis Screening in Latvia: A Pilot Project. Proc. Latv. Acad. Sci. Sect. 2009, 63, 147–150. [Google Scholar] [CrossRef]
- Czibere, L.; Burggraf, S.; Fleige, T.; Glück, B.; Keitel, L.M.; Landt, O.; Durner, J.; Röschinger, W.; Hohenfellner, K.; Wirth, B.; et al. High-Throughput Genetic Newborn Screening for Spinal Muscular Atrophy by Rapid Nucleic Acid Extraction from Dried Blood Spots and 384-Well QPCR. Eur. J. Hum. Genet. 2020, 28, 23–30. [Google Scholar] [CrossRef]
- Lee, F.; Cahhana, M.; Comeau, A.M.; Logerquist, K.; Jones, D.E.; Rohrwasser, A.; Baker, M. Spinal Muscular Atrophy: Overview of Available Screening Methods. Available online: https://www.newsteps.org/sites/default/files/resources/download/aphl_sma_webinar_slides_webinarslides_june2018_kh.pdf (accessed on 30 July 2021).
- Mercer, K. ORISE Fellow Newborn Screening Translational Research Initiative Newborn Screening and Molecular Biology Branch Newborn Screening for Spinal Muscular Atrophy. Available online: https://www.aphl.org/conferences/proceedings/Documents/Mercer.pdf (accessed on 7 July 2021).
- Emery, S.L.; Erdman, D.D.; Bowen, M.D.; Newton, B.R.; Winchell, J.M.; Meyer, R.F.; Tong, S.; Cook, B.T.; Holloway, B.P.; McCaustland, K.A.; et al. Real-Time Reverse Transcription-Polymerase Chain Reaction Assay for SARS-Associated Coronavirus. Emerg. Infect. Dis. 2004, 10, 311–316. [Google Scholar] [CrossRef]
- Strom, C.M.; Anderson, B.; Peng, M.; Patel, U.; Braastad, C.D.; Sun, W. 1000 Sample Comparison of MLPA and RT-PCR for Carrier Detection and Diagnostic Testing for Spinal Muscular Atrophy Type 1. Open J. Genet. 2013, 3, 111–114. [Google Scholar] [CrossRef]
- Lee, T.-M.; Kim, S.-W.; Lee, K.-S.; Jin, H.-S.; Koo, S.K.; Jo, I.; Kang, S.; Jung, S.-C. Quantitative Analysis of SMN1 Gene and Estimation of SMN1 Deletion Carrier Frequency in Korean Population Based on Real-Time PCR. J. Korean Med. Sci. 2004, 19, 870–873. [Google Scholar] [CrossRef][Green Version]
- Dangouloff, T.; Burghes, A.; Tizzano, E.F.; Servais, L. 244th ENMC International Workshop: Newborn Screening in Spinal Muscular Atrophy 10–12 May 2019, Hoofdorp, The Netherlands. Neuromuscul. Disord. 2020, 30, 93–103. [Google Scholar] [CrossRef]
- Romanelli Tavares, V.L.; Monfardini, F.; Lourenço, N.C.; da Rocha, K.M.; Weinmann, K.; Pavanello, R.; Zatz, M. Newborn Screening for 5q Spinal Muscular Atrophy: Comparisons between Real-Time PCR Methodologies and Cost Estimations for Future Implementation Programs. Int. J. Neonatal Screen. 2021, 7, 53. [Google Scholar] [CrossRef] [PubMed]
- Kariyawasam, D.S.T.; Russell, J.S.; Wiley, V.; Alexander, I.E.; Farrar, M.A. The Implementation of Newborn Screening for Spinal Muscular Atrophy: The Australian Experience. Genet. Med. 2020, 22, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Strautmanis, J.; Kenina, V.; Setlere, S.; Diriks, M.; Millere, E.; Micule, I.; Lace, B.; Kristapsone, G.; Grantina, I.; Auzenbaha, M.; et al. Spinal Muscular Atrophy Expert Paper “Diagnosis of Spinal Muscular Atrophy and Treatment Approach in Latvia”. Clinical Guidelines of Latvian National Health Service. 2022. Available online: https://www.vmnvd.gov.lv/lv/media/14120/download (accessed on 1 February 2022).


{kind=link}
| Number of Parents Recruited | Median Result Report Time (Days) after DBS Sample Receipt to Molecular Laboratory | SD | Median Result Report Time (Days) after Birth of Newborn | SD | |
|---|---|---|---|---|---|
| Month1 * | 83 | 12 | 2.42 | 30 | 4.22 |
| Month2 | 680 | 5 | 2.11 | 11 | 4.51 |
| Month3 | 1051 | 4 | 1.71 | 11 | 2.97 |
| Month4 | 1330 | 5 | 2.02 | 12 | 3.56 |
| Month5 | 1183 | 3 | 2.07 | 11 | 5.65 |
| Month6 | 1317 | 2 | 1.31 | 11 | 2.98 |
| Month7 | 1247 | 2 | 1.34 | 11 | 2.88 |
| Month8 | 1443 | 3 | 1.41 | 11 | 3.11 |
| Month9 | 1023 | 2 | 1.33 | 10 | 2.96 |
| Month10 | 1054 | 3 | 1.32 | 11 | 2.50 |
| Method Using Methanol [16] | Method Using Thesit® [17] | |
|---|---|---|
| Isolation volume | 1.5 mL tube | 0.2 mL tube |
| Isolation time | ~2 h for 96 samples | ~1 h for 96 samples |
| Initial material | One 3 mm blood punch | One 3 mm blood punch |
| Isolated median DNA concentration (measured by NanoDrop) | 26.6 ± 9.68 ng/μL | 43.0 ± 10.3 ng/μL |
| Final volume | 100 μL | 50 μL |
| DNA quality for qPCR | satisfactory | satisfactory |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gailite, L.; Sterna, O.; Konika, M.; Isakovs, A.; Isakova, J.; Micule, I.; Setlere, S.; Diriks, M.; Auzenbaha, M. New-Born Screening for Spinal Muscular Atrophy: Results of a Latvian Pilot Study. Int. J. Neonatal Screen. 2022, 8, 15. https://doi.org/10.3390/ijns8010015
Gailite L, Sterna O, Konika M, Isakovs A, Isakova J, Micule I, Setlere S, Diriks M, Auzenbaha M. New-Born Screening for Spinal Muscular Atrophy: Results of a Latvian Pilot Study. International Journal of Neonatal Screening. 2022; 8(1):15. https://doi.org/10.3390/ijns8010015
Chicago/Turabian StyleGailite, Linda, Olga Sterna, Maija Konika, Aleksejs Isakovs, Jekaterina Isakova, Ieva Micule, Signe Setlere, Mikus Diriks, and Madara Auzenbaha. 2022. "New-Born Screening for Spinal Muscular Atrophy: Results of a Latvian Pilot Study" International Journal of Neonatal Screening 8, no. 1: 15. https://doi.org/10.3390/ijns8010015
APA StyleGailite, L., Sterna, O., Konika, M., Isakovs, A., Isakova, J., Micule, I., Setlere, S., Diriks, M., & Auzenbaha, M. (2022). New-Born Screening for Spinal Muscular Atrophy: Results of a Latvian Pilot Study. International Journal of Neonatal Screening, 8(1), 15. https://doi.org/10.3390/ijns8010015