We All Have a Role to Play: Redressing Inequities for Children Living with CAH and Other Chronic Health Conditions of Childhood in Resource-Poor Settings

 ,
,  ,
,  and
and 
Abstract
1. Introduction
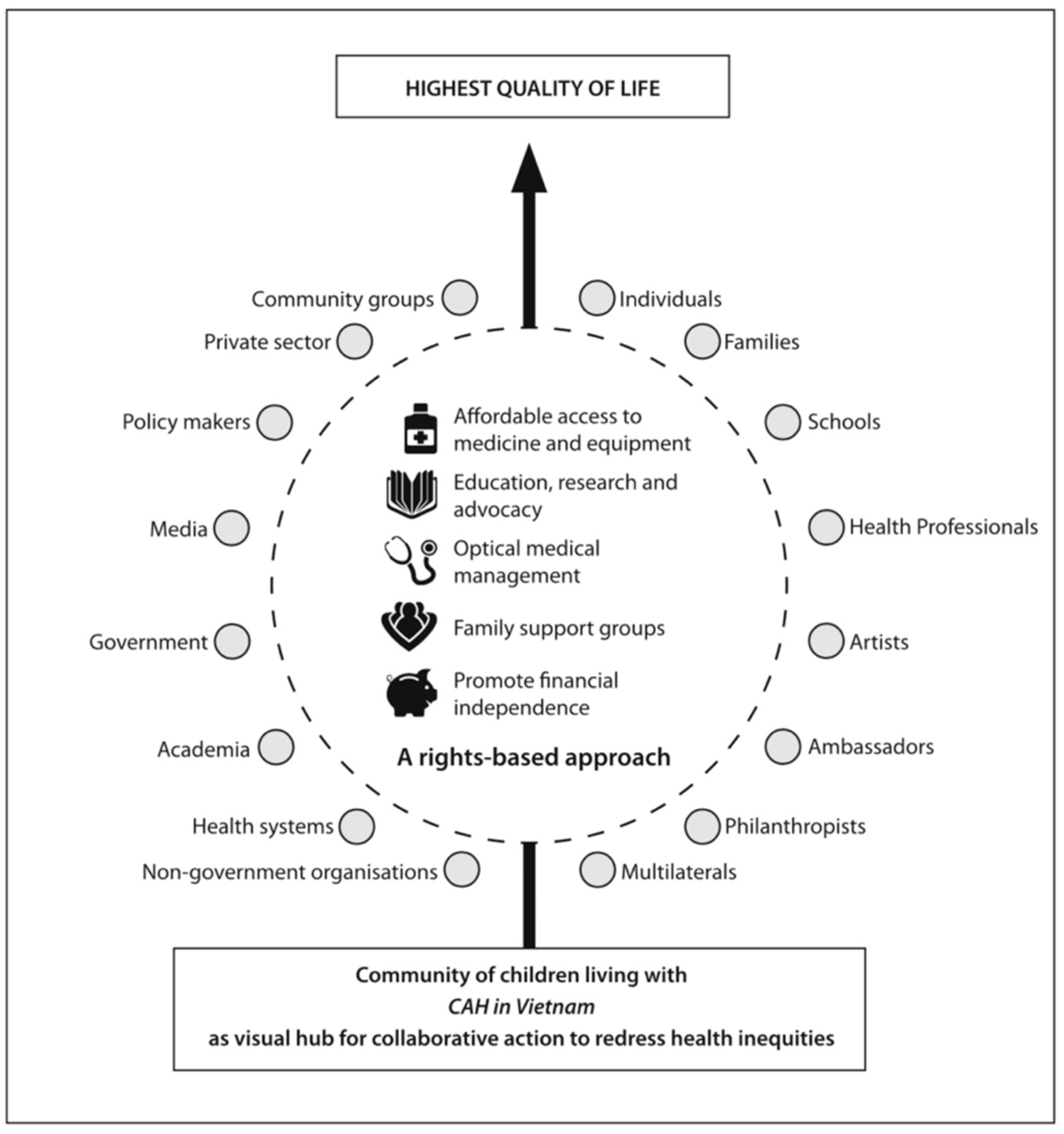
What Is Caring and Living as Neighbours (CLAN)?
- Affordable access to essential medicines and equipment;
- Education, research and advocacy;
- Optimisation of medical management (with a focus on primary, secondary and tertiary prevention);
- Encouragement of family support groups; and
- Reducing financial burdens and promoting financial independence.
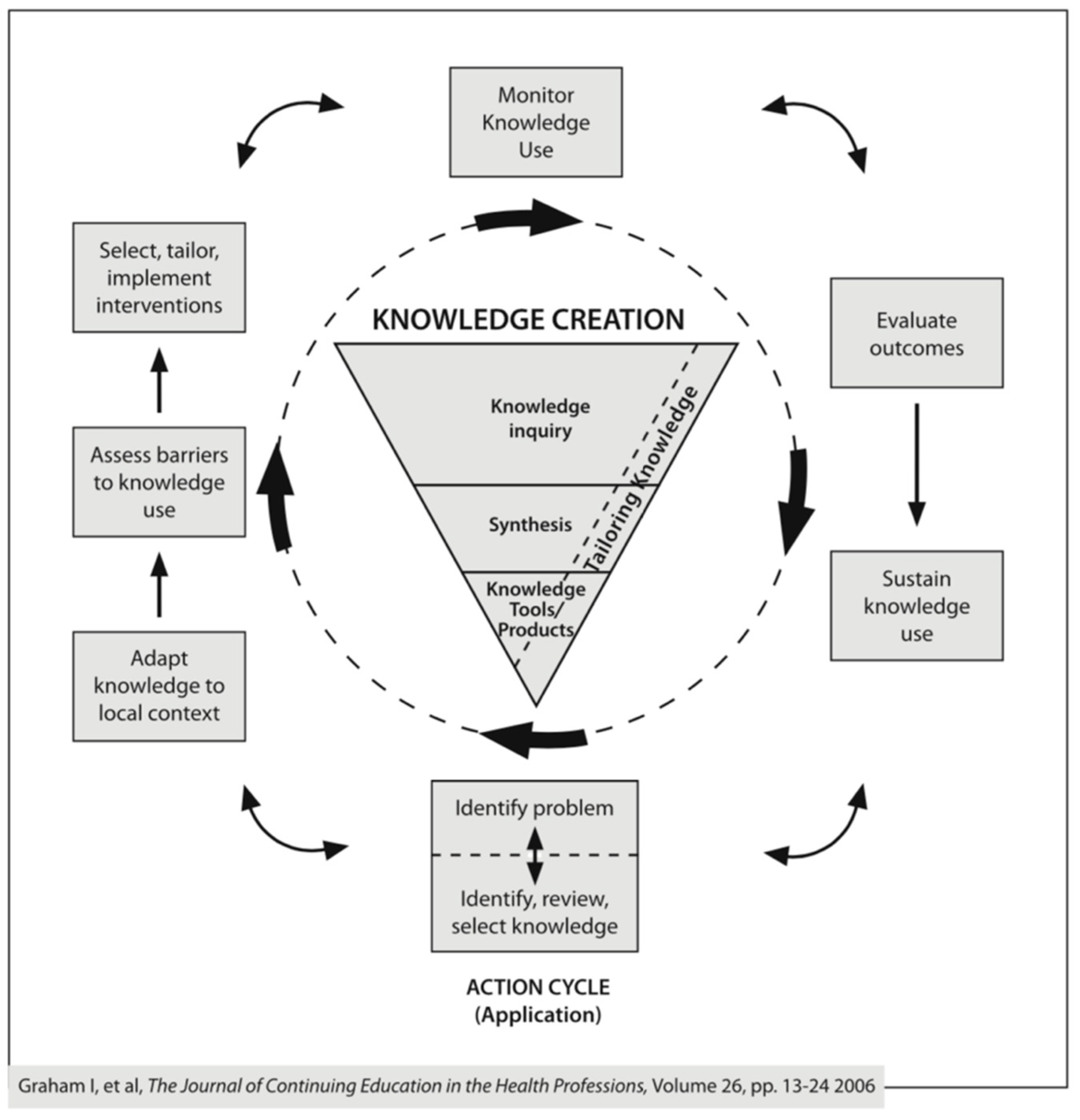
2. Materials and Methods
- Identify the problem—identify, review and select knowledge;
- Adapt knowledge to local context;
- Assess barriers to knowledge use;
- Select, tailor and implement interventions;
- Monitor knowledge use;
- Evaluate outcomes;
- Sustain knowledge use.
3. Results
3.1. Identify the Problem—Identify, Review and Select Knowledge
3.2. Adapt Knowledge to Local Context
- demographic profiles;
- medication use and purchase;
- routine management of CAH;
- management of adrenal crises;
- health and quality of life;
- specific challenges experienced by girls living with CAH;
- understanding other burdens or questions families might have.
3.3. Assess Barriers to Knowledge Use
- Unaffordable and unreliable access to essential medicines—overwhelmingly identified as the most urgent priority.
- Poverty—low incomes (particularly for remote and rural families) were exacerbated by the high cost of medicines and ongoing expenditure and loss of income associated with accessing quality care at tertiary and quaternary centres far from home (few families would trust any health professionals outside of NHP).
- Knowledge and skills gaps—there was an expressed need for education and training on CAH for children, youth, families and health professionals (especially local doctors, who were not considered knowledgeable enough about CAH to manage adrenal crises). Specific queries around genetic counselling and prenatal diagnosis of CAH were also common.
- Language barriers—despite the availability of information on CAH in English, almost all families could only speak Vietnamese, and online translation was not yet readily available.
- Isolation and lack of networks—for both individuals and health professionals.
- Misinformation and myths—were clearly dominant where there was an absence of accurate information.
- Social stigma, beliefs and attitudes—notably cultural considerations, such as fears for children around future marriage and procreation prospects.
- Virilisation—particularly surgical and psycho-social concerns for girls living with CAH when access to medicine had been compromised.
- Health-system challenges for children living with chronic health conditions—such as the complex referral processes, and gaps in existing universal health insurance systems with regards outpatient care for NCDs of childhood.
- Travel and transportation challenges for those living some distance from NHP.
- Incorporation as an NGO with the New South Wales (NSW) Department of Fair Trade;
- Fundraising certification with the Office of Liquor and Gaming, NSW;
- Registration with and annual compliance reporting to the Australian Charities and Not-for-Profits Commission (ACNC);
- Signatory to the Code of Conduct and annual Compliance Self Assessment (CSA) audits of the Australian Council For International Development (ACFID) [47];
- Annual reports submitted to the National Library of Australia;
- Tax deductibility status (TDS) and overseas aid gift deductibility status (OAGDS) with the Australian Taxation Office (ATO) and Department of Foreign Affairs and Trade (DFAT);
- Formal association with the United Nations Department of Public Information for NGOs (UNDPI/NGO);
- Special Consultative Status with the UN’s Economic and Social Council (ECOSOC); and
- Community of Practice (COP) member status with the World Health Organisation’s Non-Communicable Disease Global Coordinating Mechanism (WHO NCD/GCM).
3.4. Select, Tailor and Implement Interventions
3.5. Monitor Knowledge Use
- Conceptual knowledge use—this includes changes in levels of knowledge, understanding or attitudes. Examples of indicators used to monitor knowledge use included: the CAH PepTalk Tool [53], developed to evaluate parental knowledge of CAH and its management; numbers of families and health professionals attending Club meetings and training sessions (reflected degree of engagement); nature of questions posed by families at Club meetings (a useful barometer of the general understanding of the community and tool for identifying widely held myths and misunderstandings); engagement of external partners and stakeholders; and requests to CLAN to scale CAH activities to other hospitals (in Vietnam and beyond) and health conditions.
- Instrumental knowledge use—monitors changes in behavior or practice (and most importantly, changes that translate into improved health outcomes). Examples of indicators used included: availability and registration of drugs (reflecting the broader health system); use of injection kits on sick days at home by families; patient registers tracking incidence, prevalence, mortality and loss to follow-up; use of growth charts (introduced for routine use in outpatient clinics); availability and quality of educational resources in local language for families and health professionals; availability and analysis of 17OHP and renin testing; use of genetic analysis; and establishment of NBS for CAH.
- Strategic knowledge use—is the manipulation of knowledge to attain specific power or profit goals (sometimes referred to as “research as ammunition”). Examples of indicators included: publication of results and presentations at international conferences; collaborative engagement in civil society networks; engagement with multilaterals and member state governments; participation of media at Club meetings; requests received to translate CLAN’s model to other conditions and countries; and the number and types of communities established internationally.
3.6. Evaluate Outcomes—Impact of Using the Knowledge
3.6.1. Vietnam
3.6.2. The Philippines
3.6.3. Indonesia
3.6.4. Pakistan
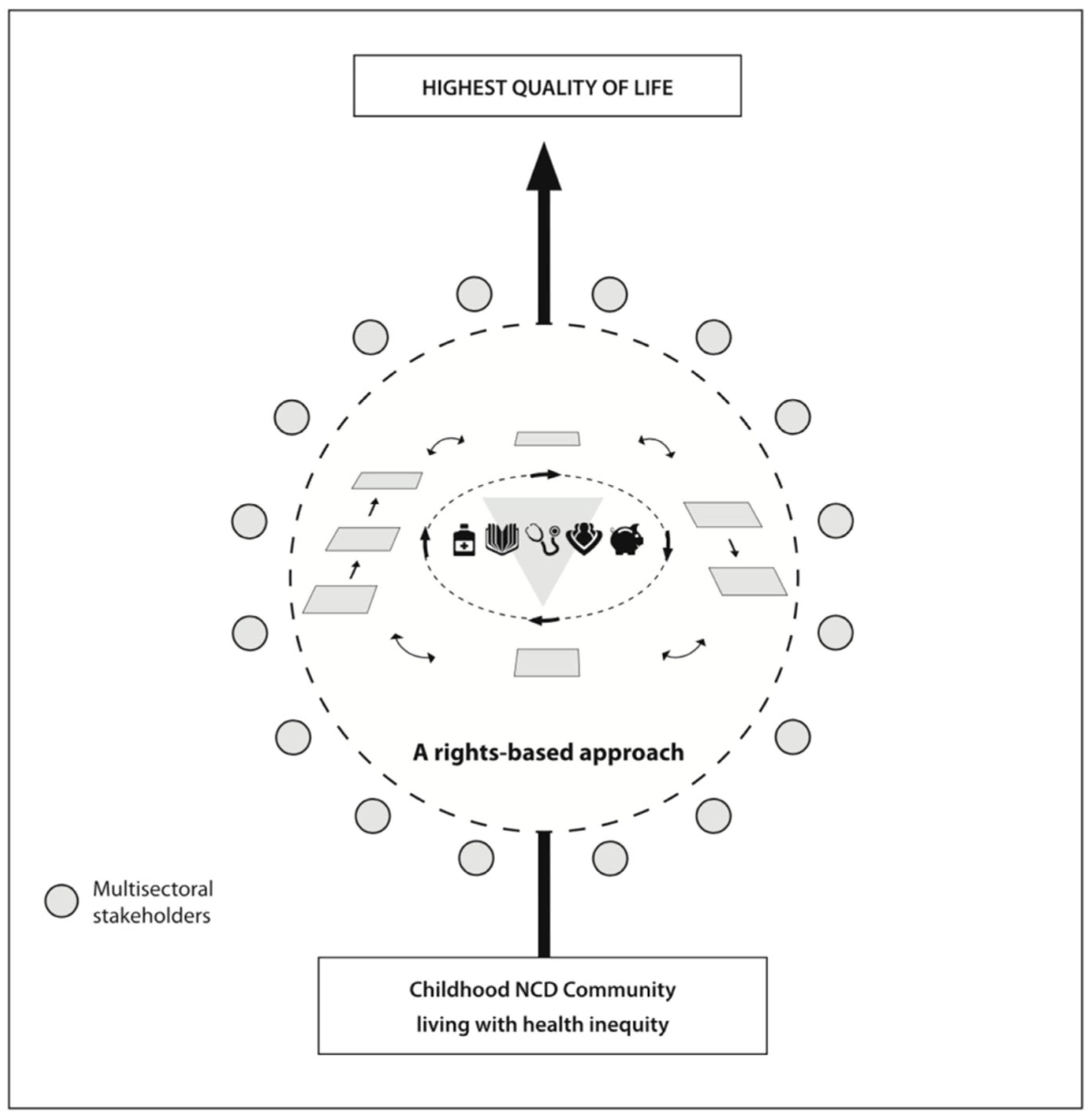
- Human rights-based approach—acknowledging rights and responsibilities as outlined in the United Nations’ Convention on the Rights of the Child [80].
- Equity—a commitment to strive for excellence for all, and ensuring the rights of children in high- and low-income countries to the highest quality of life possible are respected, promoted and protected.
- Community development—all children living with the same chronic health condition in a country are members of a community; these NCD Communities are considered as interconnected and united at the local, regional, national and international level.
- Community control—people living with chronic conditions are experts and must be consulted at all stages when decisions are made around appropriate approaches and actions to drive change.
- Person- and family-centred care—acknowledges the pivotal role children, young people and families play in all activities. Indeed, a number of parents of children with chronic health conditions have stayed engaged with CLAN over a decade, and have been champions in their country for change.
- Sustainable, ethical and transparent approaches to project management—CLAN is committed to the highest standards of accountability and reporting required of NGOs (by ACFID) in Australia and to the United Nations (through UNDPI/NGO and ECOSOC); as a not-for-profit CLAN is committed to sustainable approaches and responsible action in the face of climate change.
- Multisectoral collaboration and partnerships—are key to sustainability and success.
- Above all do no harm—is an overarching guiding principle and informs all actions.
- Type 1 diabetes—Vietnam (2007), Pakistan (2007) and Indonesia (2020);
- Osteogenesis imperfecta (OI)—Vietnam (2011), Indonesia (2013), Pakistan (2014) and Fiji (2016);
- Duchenne muscular dystrophy (DMD)—Vietnam (2012);
- Nephrotic syndrome (NS)—Vietnam (2010);
- Rheumatic heart disease (RHD)—Kenya (2013);
- Nodding syndrome and epilepsy—Uganda (2017);
- Thalassaemia—India (2020);
- Asthma, cancer, autism and cerebral palsy (amongst others)—collaborative advocacy efforts in multiple countries.
3.7. Sustain Knowledge Use
4. Discussion
4.1. Limitations and Challenges
4.2. Recommendations
4.3. Affordable Access to Essential Medicines and Equipment Is Pillar 1 for a Reason
4.4. Share the Wheel—Don’t Reinvent It
4.5. Community Is Core to Sustainability
4.6. Knowledge Is Power
4.7. Two-Way Learning Strengthens Us All
4.8. Prioritise Children and Families Experiencing the Greatest Inequities
4.9. Embrace Imperfection amongst Complexity
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Approach to Monitoring | Individuals & Families | Health Practitioners | Health System |
|---|---|---|---|
| Conceptual knowledge use (changes in levels of knowledge, understanding or attitudes) |
|
|
|
| Instrumental knowledge use (changes in behavior or practice—translates into improved health outcomes) |
|
|
|
| Strategic knowledge use (manipulation of knowledge to attain specific power or profit goals—research as ammunition) |
|
|
|
| KTA Stages | CLAN Milestone/Activities | Knowledge Creation | Products/Tools Developed |
|---|---|---|---|
| Identify the problem | International Congenital Adrenal Hyperplasia (CAH) newsletters describe situation in Vietnam Short-term humanitarian donation of essential medicines obtained for every child with CAH in Vietnam CLAN founded as Non-Government Organisation (NGO) in 2004 and incorporated as NGO with Department of Fair Trade in 2007 | Access to medicine is a life-threatening problem for children living with CAH in Vietnam when essential medicines are not registered nor affordably available. National CAH Communities need to be acknowledged and supported to connect globally with one another. | CLAN constitution and policy handbook CLAN website CLAN Newsletters |
| Adapt knowledge to local use | Health needs assessment (HNA) conducted in Hanoi, Vietnam to learn more about challenges facing families. | Consultation with people living with CAH is essential to a comprehensive understanding of “the problem” facing families and children living with CAH in resource-poor settings | CAH HNA survey template (since translated to rheumatic heart disease (RHD), nephrotic syndrome and epilepsy) |
| Assess barriers to knowledge use | Analysis of responses to HNA of families, and interviews with health professionals and other stakeholders, with results published in peer-review literature. Insights informed development of CLAN’s model | Power of publication of results. Development of CLAN’s Strategic Framework for Action and identification of CLAN’s five pillars | Publications (see references) CLAN Strategic Framework for Action |
| Select, tailor and implement interventions | Findings from HNA informed the development of a strategic plan to improve quality of life for every child living with CAH in Vietnam. The plan was shared with a broad range of stakeholders to promote multisectoral collaborative action and affordable/achievable/urgent actions prioritized for immediate action across the five pillars (specific examples outlined in Table A1). | Families and children must be the visual hub of all action; community development is key to sustainability. Collaboration with a broad range of multisectoral stakeholders is essential to scaling activities; communication is key to ensuring all stakeholders are aware of one another’s contributions and commitments (reduces duplication and strengthens engagement. CLAN’s model able to be replicated across multiple locations nationally. | Plan for CLAN—a strategic work plan, capturing activities to redress inequities according to the five pillars Successful application to the World Health Organisation’s Essential Medicines List for Children (WHO EMLc) for hydrocortisone and fludrocortisone tablets Translated educational resources (booklets, books, videos, mobile phone apps etc.) Social media platforms (Whats App, Facebook, Twitter, Instagram) |
| Monitor knowledge use | Evaluation of all events and activities informed a continuous quality improvement approach, and ensures priorities of people living with CAH are addressed Health outcomes were monitored by local professionals (e.g., mortality; loss to follow-up, incidence, prevalence) Close collaboration with hospital executive ensured appropriate alignment with Ministry of Health and media | Transparent and ethical project management is vital. Activities must address conceptual, instrumental and strategic knowledge use. | APPES (Asia Pacific Pediatric Endocrinology Society)—CLAN Equity (ACE) Snapshot Survey—facilitates rapid landscape analysis to identify inequities associated with paediatric endocrine conditions CLAN NGO reports:
|
| Evaluate outcomes | RE-AIM framework informs evaluation Expansion of activities to support new Communities for CAH and other chronic conditions of childhood Support and promote professional societies and networks for health workers Development of patient registers and other systems for monitoring health outcomes, incidence and prevalence | CLAN’s model is scalable and replicable across countries and health conditions. Health professionals play essential role in supporting childhood NCD communities. | CLAN Club meeting checklist CLAN Club Grant Application form Patient registers Google analytics APPES-CLAN Declaration |
| Sustain knowledge use | Many communities now operating independently, with own social media platforms and strategic agendas Founding of NCD Child and IndigenousNCDs facilitates broader synergies, networks and sustainability of the movement | Community development and involvement of PLW NCDs is key to sustainability of movement. There is commonality across NCDs. CLAN’s work is relevant to broader NCD movement and other communities (e.g., Indigenous persons globally). | Links with individual and independent grassroots NCD communities and collaborations:
|
References
- Speiser, P.W.; Arlt, W.; Auchus, R.J.; Baskin, L.S.; Conway, G.S.; Merke, D.P.; Meyer-Bahlburg, H.F.; Miller, W.L.; Murad, M.H.; Oberfield, S.E.; et al. Congenital Adrenal Hyperplasia due to steroid 21-Hydroxylase deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2018, 103, 4043–4088. [Google Scholar] [CrossRef] [PubMed]
- Brener, A.; Segev-Becker, A.; Weintrob, N.; Stein, R.; Interator, H.; Schachter-Davidov, A.; Israeli, G.; Elkon-Tamir, E.; Lebenthal, Y.; Eyal, O.; et al. Health-related quality of life in children and adolescents with Nonclassic Congenital Adrenal Hyperplasia. Endocr. Pract. 2019, 25, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Halper, A.; Hooke, M.C.; Gonzalez-Bolanos, M.T.; Vanderburg, N.; Tran, T.N.; Torkelson, J.; Sarafoglou, K. Health-related quality of life in children with congenital adrenal hyperplasia. Health Qual. Life Outcomes 2017, 15, 194. [Google Scholar] [CrossRef] [PubMed]
- Piane, L.D.; Rinaudo, P.; Miller, W.L. 150 Years of Congenital Adrenal Hyperplasia: Translation and Commentary of De Crecchio’s Classic Paper from 1865. Endocrinology 2015, 156, 1210–1217. [Google Scholar] [CrossRef]
- Padilla, C.D.; Therrell, B.L. Newborn screening in the Asia Pacific region. J. Inherit. Metab. Dis. 2007, 30, 490–506. [Google Scholar] [CrossRef]
- Alfadhel, M.; Al Othaim, A.; Al Saif, S.; Al Mutairi, F.; Alsayed, M.; Rahbeeni, Z.; Alzaidan, H.; Alowain, M.; Al-Hassnan, Z.; Saeedi, M.; et al. Expanded Newborn Screening Program in Saudi Arabia: Incidence of screened disorders. J. Paediatr. Child Health 2017, 53, 585–591. [Google Scholar] [CrossRef]
- Australian Health Ministers Advisory Council (AHMAC). CAH Condition Assessment Summary for NBS in Australia—March 2019. Available online: http://www.cancerscreening.gov.au/internet/screening/publishing.nsf/Content/C79A7D94CB73C56CCA257CEE0000EF35/$File/Congenital%20adrenal%20hyperplasia%20(CAH)%20condition%20assessment%20summary%20-%20March%202019.pdf (accessed on 30 July 2020).
- Warne, G.L.; Armstrong, K.L.; Faunce, T.A.; Wilcken, B.; Boneh, A.; Geelhoed, E.; Craig, M.E. The case for newborn screening for congenital adrenal hyperplasia in Australia. Med. J. Aust. 2010, 192, 107. [Google Scholar] [CrossRef]
- Gleeson, H.K.; Wiley, V.; Wilcken, B.; Elliott, E.J.; Cowell, C.; Thonsett, M.; Byrne, G.; Ambler, G. Two-year pilot study of newborn screening for congenital adrenal hyperlasia in New South Wales compared with nationwide case surveillance in Australia. J. Paediatr. Child Health 2008, 44, 554–559. [Google Scholar] [CrossRef]
- Wu, J.Y.; Sudeep; Cowley, D.M.; Harris, M.; McGown, I.N.; Cotterill, A.M. Is it time to commence newborn screening for congenital adrenal hyperplasia in Australia? Med. J. Aust. 2011, 195, 260–262. [Google Scholar] [CrossRef]
- CAHSGA (Congenital Adrenal Hyperplasia Support Group Australia) Incorporated. Available online: http://www.cah.org.au (accessed on 30 July 2020).
- CARES Foundation. Available online: https://caresfoundation.org (accessed on 30 July 2020).
- CLAN (Caring & Living As Neighbours) Incorporated. Available online: www.clanchildhealth.org (accessed on 30 July 2020).
- Armstrong, K.; Henderson, C.; Hoan, N.; Warne, G.L. Living with Congenital Adrenal Hyperplasia in Vietnam: A Survey of Parents. J. Pediatr. Endocrinol. Metab. 2006, 19, 1207–1224. [Google Scholar] [CrossRef]
- Armstrong, K.L. Working together so we #LeaveNoChildBehind. In Proceedings of the 9th Biennial Scientific Meeting of APPES (Asia Pacific Pediatric Endocrinology Society), Tokyo, Japan, 17–20 November 2016. [Google Scholar]
- Roe, M.T.; Mahaffey, K.W.; Ezekowitz, J.A.; Alexander, J.H.; Goodman, S.G.; Hernandez, A.F.; Temple, T.; Berdan, L.; Califf, R.M.; Harrington, R.A.; et al. The future of cardiovascular clinical research in North America and beyond—Addressing challenges and leveraging opportunities through unique academic and grassroots collaborations. Am. Heart J. 2015, 169, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, K.L.; Nguyen, H.T.; Nguyen, L.T.; Le, V.H.; Thoai, L.H.; Binh, T.; Hoang, T.T.D.; Mac, Y.T.; Tong, A.; Hodson, E. Understanding the challenges facing children and families living with Nephrotic Syndrome in Vietnam: A survey of families. In Pediatric Nephrology; Springer: New York, NY, USA, 2013. [Google Scholar]
- Merriam, S.B.; Johnson-Bailey, J.; Lee, M.-Y.; Kee, Y.; Ntseane, G.; Muhamad, M. Power and positionality: Negotiating insider/outsider status within and across cultures. Int. J. Lifelong Educ. 2001, 20, 405–416. [Google Scholar] [CrossRef]
- Ozano, K.; Khatri, R. Reflexivity, positionality and power in cross-cultural participatory action research with research assistants in rural Cambodia. Educ. Action Res. 2017, 26, 190–204. [Google Scholar] [CrossRef]
- Bhaskar, R. A Realist Theory of Science; Taylor and Francis Group, Routledge: London, UK; New York, NY, USA, 1978. [Google Scholar]
- Easton, G. Critical realism in case study research. Ind. Mark. Manag. 2010, 39, 118–128. [Google Scholar] [CrossRef]
- Fletcher, A.J. Applying critical realism in qualitative research: Methodology meets method. Int. J. Soc. Res. Methodol. 2016, 20, 181–194. [Google Scholar] [CrossRef]
- McEvoy, P.; Richards, D.A. A critical realist rationale for using a combination of quantitative and qualitative methods. J. Res. Nurs. 2006, 11, 66–78. [Google Scholar] [CrossRef]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef]
- NCD Alliance—“Our Views, Our Voices”. Available online: https://ncdalliance.org/what-we-do/capacity-development/our-views-our-voices (accessed on 27 August 2020).
- Harrison, H.; Birks, M.; Franklin, R.; Mills, J. Case Study Research: Foundations and Methodological Orientations. Forum Qual. Soc. Res. 2017, 18. [Google Scholar] [CrossRef]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef]
- World Health Organisation (WHO)—Knowledge-to-Action (KTA) Framework. Available online: https://www.who.int/reproductivehealth/topics/best_practices/greatproject_KTAframework/en/ (accessed on 30 July 2020).
- Yin, R. Case Study Research: Design and Methods, 5th ed.; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Warne, G. The state of children and teenagers with CAH in Vietnam. In CARES Foundation Fall Newsletter; CARES Foundation: Union, NJ, USA, 2004; p. 12. [Google Scholar]
- Konheiser, M. My Vietnam Experience, in CARES Foundation Fall Newsletter; CARES Foundation: Union, NJ, USA, 2004; pp. 10–11. [Google Scholar]
- Australian Government, Department of Health—Medicare. Available online: https://www.health.gov.au/health-topics/medicare (accessed on 30 July 2020).
- Mylan Australia. Available online: https://www.mylan.com.au (accessed on 30 July 2020).
- Bristol Myers Squibb. Available online: https://www.bms.com/about-us/our-company/new-bristol-myers-squibb.html (accessed on 30 July 2020).
- CLAN (Caring & Living As Neighbours) Annual Report 2005. Available online: https://www.clanchildhealth.org/uploads/8/3/3/6/83366650/clan_2005_annual_report.pdf (accessed on 30 August 2020).
- CLAN (Caring & Living As Neighbours) Annual Report 2006. Available online: https://www.clanchildhealth.org/uploads/8/3/3/6/83366650/clan_2006_-_annual_report.pdf (accessed on 30 August 2020).
- CLAN (Caring & Living As Neighbours) Annual Report 2007. Available online: https://www.clanchildhealth.org/uploads/8/3/3/6/83366650/clan_2007_annual_report.pdf (accessed on 30 August 2020).
- Consensus Statement on 21-Hydroxylase Deficiency from The European Society for Paediatric Endocrinology and The Lawson Wilkins Pediatric Endocrine Society. Horm. Res. Paediatr. 2002, 58, 188–195. [CrossRef]
- CLAN (Caring & Living As Neighbours) Annual Report 2008. Available online: https://www.clanchildhealth.org/uploads/8/3/3/6/83366650/2008-clan-annual-report.pdf (accessed on 30 August 2020).
- Hsu, C.Y.; Rivkees, S.A. Congenital Adrenal Hyperplasia: A Parent’s Guide; AuthorHouse: Bloomington, IN, USA, 2005; p. 290. [Google Scholar]
- Hsu, C.Y.; Rivkees, S.A. Tăng Sản thượng thận Bẩm Sinh; Nhà Xuất Bản Y Học.: Hanoi, Vietnam, 2011; p. 323. [Google Scholar]
- CLAN (Caring & Living As Neighbours) Annual Report 2011–2012. Available online: https://www.clanchildhealth.org/uploads/8/3/3/6/83366650/fy10-11_clan_annual_report_[email]-1.pdf (accessed on 30 August 2020).
- Sayer, A. Realism and Social Science; Sage: London, UK, 2000. [Google Scholar]
- Serrat, O. The Five Whys Technique. 2009. Available online: https://www.adb.org/sites/default/files/publication/27641/five-whys-technique.pdf (accessed on 30 July 2020).
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organisation Model List of Essential Medicines for Children, 7th ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- ACFID (Australian Council For International Development). Available online: https://acfid.asn.au (accessed on 30 August 2020).
- International Insulin Foundation (IIF) Project in Vietnam. Available online: http://www.access2insulin.org/iifs-project-in-vietnam.html (accessed on 30 July 2020).
- CLAN (Caring & Living As Neighbours). Child-Friendly CAH Rights Flyer; CLAN Inc.: Sydney, Australia, 2017; Available online: https://www.clanchildhealth.org/cah.html (accessed on 30 August 2020).
- VIDEO—July 2012 CAH Club Hanoi, Vietnam. Available online: https://www.youtube.com/watch?v=QcynUyhzhV4 (accessed on 30 August 2020).
- APPES. The Tokyo Declaration of the 9th Biennial Scientific Meeting of the Asia Pacific Pediatric Endocrinology Society (APPES). In Proceedings of the APPES Conference, Tokyo, Japan, 17–20 November 2016. [Google Scholar]
- Zainuddin, A.A.; Grover, S.R.; Shamsuddin, K.; Mahdy, Z.A. Research on Quality of Life in Female Patients with Congenital Adrenal Hyperplasia and Issues in Developing Nations. J. Pediatric Adolesc. Gynaecol. 2013, 26, 296–304. [Google Scholar] [CrossRef]
- Mitchelhill, I.; Armstrong, K.; Craig, M.; Dung, V.C.; Thao, B.P.; Khanh, N.N.; Ngoc, T.B.; Hoang, T.T.D.; Quynh, H.; Tran, D.T.P.; et al. Evaluation of parental knowledge after establishing CAH clubs in Vietnam & Indonesia. Int. J. Pediatric Endocrinol. 2015, 2015 (Suppl. 1), P53. [Google Scholar]
- APPES (Asia Pacific Pediatric Endocrinology Society). Available online: https://www.appes.org (accessed on 30 July 2020).
- CLAN (Caring & Living As Neighbours) Annual Report 2016–2017. Available online: https://www.clanchildhealth.org/uploads/8/3/3/6/83366650/clan_2016-2017_annual_report__1_.pdf (accessed on 30 August 2020).
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef]
- Dung, V.C.; Thao, B.P.; Ngoc, C.T.B.; Khanh, N.N.; Dat, N.P.; Hoan, N.T.; Mai, D.T.; Craig, M. Updated registry of congenital adrenal hyperplasia at the north pediatric referral centre of Vietnam. Int. J. Pediatr. Endocrinol. 2015, 2015, P49. [Google Scholar] [CrossRef][Green Version]
- Huynh, Q.T.; Thuy, H.; Armstrong, K.; Craig, M. Effectiveness of diabetes and congenital adrenal hyperplasia meeting clubs. Int. J. Pediatr. Endocrinol. 2013, 2013, P134. [Google Scholar] [CrossRef][Green Version]
- Ngoc, C.T.B.; Dung, V.C.; Thao, B.P.; Khanh, N.N.; Dat, N.P.; Craig, M.; Ellard, S.; Hoan, N.T. Phenotype, genotype of neonatal diabetes mellitus due to insulin gene mutation. Int. J. Pediatr. Endocrinol. 2015, 2015, P12. [Google Scholar] [CrossRef][Green Version]
- Can, T.B.N.; Dung, V.C.; Bui, T.P.; Nguyen, K.N.; Flanagan, S.E.; Ellard, S.; Craig, M.; Nguyen, D.P.; Nguyen, H.T. Neonatal diabetes mellitus: Genotype, phenotype and outcome. Ann. Transl. Med. 2015. [Google Scholar] [CrossRef]
- Can, T.B.N.; Dung, V.C.; Thao, B.P.; Khanh, N.N.; Dat, N.P.; Sian, E.; Thi, H.N. The Result of Sulphonylureas Treatment in Patients with Neonatal Diabetes Mellitus due to kcnj11/abcc8 Gene Mutations in Vietnam. In Proceedings of the ESPE Dublin (European Society for Paediatric Endocrinology Conference), Hormone Research in Paediatrics (82), Dublin, Ireland, 18–22 September 2014. [Google Scholar]
- Chi, D.V.; Tran, T.H.; Nguyen, D.H.; Luong, L.H.; Le, P.T.; Ta, M.H.; Ngo, H.T.T.; Nguyen, M.P.; Le-Anh, T.P.; Nguyen, D.P.; et al. Novel variants of CYP21A2 in Vietnamese patients with congenital adrenal hyperplasia. Mol. Genet. Genom. Med. 2019, 7, e623. [Google Scholar] [CrossRef]
- Chi, D.V.; (National Hospital of Pediatrics, Hanoi, Vietnam). Personal communication, 2020.
- Chi, D.V.; Nguyen, N.L.; Nguyen, H.H.; Nguyen, T.K.L.; Tran, T.H.; Ta, T.V.; Tran, V.K. A novel nonsense mutation in the CYP21A2 gene of a Vietnamese patient with congenital adrenal hyperplasia. In Proceedings of the Biomedical Research and Therapy—Abstract Proceeding: International Conference “Innovations in Cancer Research and Regenerative Medicine 2017”, Ho Chi Minh City, Vietnam, 10–13 September 2017. [Google Scholar]
- Armstrong, K.L.; Ditchfield, S.; Henderson, C.; Nguyen, H.T.; Bui, T.P.; Warne, G. Young people living with CAH in Vietnam: A survivor’s cohort (Poster presentation). In Proceedings of the 2008 State Population Health Conference: Public Health Research for the Real World, Hindmarsh, South Australia, 18 October 2008. [Google Scholar]
- Varni, J.W. The PedsQL TM Measurement Model for the Pediatric Quality of Life Inventory. Available online: https://www.pedsql.org/index.html (accessed on 20 September 2020).
- CLAN (Caring & Living As Neighbours), VIDEO—Happy and Healthy with CAH. 2012. Available online: https://www.youtube.com/watch?v=83b05k7MGQ4 (accessed on 30 August 2020).
- Proceedings of the the Second Meeting of the Subcommittee of the Expert Committee on the Selection and Use of Essential Medicines, Geneva, Switzerland, 29 September–3 October 2008; Available online: https://www.who.int/selection_medicines/committees/subcommittee/2/Fludrocortisone_MAIN.pdf (accessed on 30 August 2020).
- Facebook Group for CAHSAPI (the Philippines CAH Support Group). Available online: https://www.facebook.com/groups/170268589670584 (accessed on 30 July 2020).
- Republic of the Philippines Department of Health, Newborn Screening Program. Available online: https://www.doh.gov.ph/newborn-screening (accessed on 10 August 2020).
- Utari, A.; Ariani, M.D.; Ediati, A.; Juniarto, A.Z.; Faradz, S.M.H. Mortality Problems of Congenital Adrenal Hyperplasia in Central Java-Indonesia: 12 years experiences. In Proceedings of the 9th Biannual Meeting of the Asia Pacific Pediatric Endocrine Society (APPES)—50th Scientific Meeting of Japanese Society for Pediatric Endocrinology (JSPE), Tokyo, Japan, 16–20 November 2016. [Google Scholar]
- VIDEO—Tatap Masa Depan dengan Optimis—Look to the Future with Optimism. A CAH Resource for Families in Bahasa Indonesia. Available online: https://m.youtube.com/watch?index=3&list=UUOYPyehX3HOgmluHNFEP00A&t=0s&v=Rt7kaTQDrSQ#menu (accessed on 30 August 2020).
- Utari, A.; Ediati, A. Bacaan Untuk Remaja Putri Dengan Hiperplasia Adrenal Kongenital—Readings for Young Women with Congenital Adrenal Hyperplasia. Available online: https://www.clanchildhealth.org/uploads/8/3/3/6/83366650/cah_book_for_adolescent_girls_bahasa_indonesia.pdf (accessed on 30 August 2020).
- Warne, G.; Sung, V.; Raza, S.R.; Khan, Y.N.; Armstrong, K.L. Application for inclusion of Hydrocortisone tablets in the WHO Model List of Essential Medicines for Children. In Proceedings of the the Expert Committee on the Selection and Use of Essential Medicines, Children’s Essential Medicines List, World Health Organization, Geneva, Switzerland, 29 September–3 October 2008. [Google Scholar]
- Warne, G.; Raza, S.R.; Khan, Y.N.; Armstrong, K.L. Application for inclusion of Fludrocortisone tablets in the WHO Model List of Essential Medicines for Children. In Proceedings of the the Second Meeting of the Subcommittee of the Expert Committee on the Selection and Use of Essential Medicines, Geneva, Switzerland, 29 September–3 October 2008. [Google Scholar]
- SPED. Society of Paediatric Endocrinology and Diabetes—Pakistan. Available online: http://sped.org.pk (accessed on 30 August 2020).
- Pfizer Australia. Available online: https://www.pfizer.com.au (accessed on 27 August 2020).
- CLAN Inc. Video: Working together for the CAH Community in Pakistan (CLAN and NICH), November 2016. Available online: https://www.youtube.com/watch?v=begn3hQ6pNg&index=8&list=UUOYPyehX3HOgmluHNFEP00A&t=0s (accessed on 30 August 2020).
- World Health Organisation. World Health Organisation Constitution (adopted by the International Health Conference in New York, USA on 22 July 1946, and Came into Force on 7 April 1948). Available online: https://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf?ua=1 (accessed on 30 August 2020).
- United Nations Convention on the Rights of the Child. Adopted and Opened for Signature, Ratification and Accession by General Assembly Resolution 44/25 of 20 November 1989, with Entry into Force 2 September 1990 in Accordance with Article 49. Available online: https://www.ohchr.org/en/professionalinterest/pages/crc.aspx (accessed on 30 August 2020).
- Wishbone Day. Available online: http://www.wishboneday.com/p/about.html (accessed on 30 August 2020).
- NCD Child. Available online: http://www.ncdchild.org (accessed on 30 August 2020).
- United Nations General Assembly. Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases. In proceedings of the 66th session (agenda item 117) of the United Nations General Assembly in 2011. Available online: https://www.who.int/nmh/events/un_ncd_summit2011/political_declaration_en.pdf?ua (accessed on 30 August 2020).
- World Health Organisation. Omnibus Resolution—Follow-Up to the Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-communicable Diseases; Agenda item 13.1 and 13.2; WHA66.10.; World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- IndigenousNCDs. Available online: www.indigenousncds.org (accessed on 30 July 2020).
- Bukhman, G.; Mocumbi, A.O.; Atun, R.; Becker, A.E.; Bhutta, Z.; Binagwaho, A.; Clinton, C.; Coates, M.M.; Dain, K.; Ezzati, M.; et al. The Lancet NCDI Poverty Commission: Bridging a gap in universal health coverage for the poorest billion. Lancet 2020. [Google Scholar] [CrossRef]
- Maslow, A.H. A theory of human motivation. Psychol. Rev. 1943, 50, 370–396. [Google Scholar] [CrossRef]
- World Health Organisation. WHO Launches First-Ever Insulin Prequalification Programme to Expand Access to Life-Saving Treatment for Diabetes. Available online: https://www.who.int/news-room/detail/13-11-2019-who-launches-first-ever-insulin-prequalification-programme-to-expand-access-to-life-saving-treatment-for-diabetes (accessed on 27 August 2020).
- Finlay, S.M.; Armstrong, K.L. Indigenous languages must play a role in tackling noncommunicable diseases. 2019 BMJ Collection “Solutions for Non-Communicable Disease Prevention and Control”. Available online: https://www.bmj.com/NCD-solutions (accessed on 30 August 2020).
- Utari, A.; Ediati, A.; Dhaliwal, R.; Freeman, J.; Armstrong, K. Girl power! How a novel booklet developed to provide psychological support for teenage girls living with CAH in Indonesia is helping to redress health inequities regionally in Poster. In Proceedings of the (P02.18) at the November 2018 APPES (Asia Pacific Pediatric Endocrinology Society) Conference, Chiang Mai, Thailand, 7–10 November 2018. [Google Scholar]
- United Nations Sustainable Development Goals (SDGs). Available online: https://www.un.org/sustainabledevelopment/sustainable-development-goals/ (accessed on 27 August 2020).
- Rodgers, R. Do-Re-Mi, in The Sound of Music; Rodgers and Hammerstein: New York, NY, USA, 1959. [Google Scholar]
- Kluge, H.H.P.; Wickramasinghe, K.; Rippin, H.L.; Mendes, R.; Peters, D.H.; Kontsevaya, A.; Breda, J. Prevention and control of non-communicable diseases in the COVID-19 response. Lancet 2020, 395, 1678–1680. [Google Scholar] [CrossRef]
- World Bank. Profiles of the New Poor Due to the COVID-19 Pandemic. Available online: https://www.worldbank.org/en/topic/poverty/brief/Profiles-of-the-new-poor-due-to-the-COVID-19-pandemic (accessed on 30 August 2020).
- World Health Organisation. COVAX: Working for Global Equitable Access to COVID-19 Vaccines. Available online: https://www.who.int/initiatives/act-accelerator/covax (accessed on 21 September 2020).
- United Nations, The Sustainable Development Goals Report. 2016. Available online: https://unstats.un.org/sdgs/report/2016/leaving-no-one-behind (accessed on 30 August 2020).



| Priorities | CLAN Activities |
|---|---|
| Pillar 1. Access to medicines and equipment | Short-term initiatives Three year donation of hydrocortisone and fludrocortisone tablets secured; use of hydrocortisone for injection promoted and injection kits shared |
| Medium term Hydrocortisone and fludrocortisone tablets registered in Vietnam; rapid assessment protocol completed with the International Insulin Foundation [48] to analyse access to medicines in Vietnam; collaborative application to have hydrocortisone and fludrocortisone tablets included in the World Health Organisation Essential Medicines List for Children (WHO EMLc). | |
| Long term Essential medicines for CAH included within national insurance scheme | |
| Pillar 2. Education, research and advocacy | Education Translation of educational resources into Vietnamese language; educational sessions for health care professionals (HCPs) prior to Club meetings; educational sessions for families/youth at Club meetings (led by local HCPs); training for HCPs both onsite (Australian nurse educator spent 6 months in Vietnam) and in Australia (endocrinologist training in Australia with APPES (the Asia Pacific Pediatric Endocrinology Society)). |
| Research Health needs assessment completed and published in journal; RAPIA adapted for CAH and completed in Vietnam [48]; CLAN-APPES Snapshot Survey developed to rapidly identify inequities [15]. | |
| Advocacy Presentation on CAH activities at APPES Conference; Child-friendly CAH Rights Flyers (raise awareness of the United Nations (UN) Convention on the Rights of the Child using five pillars) [49]; Club newsletters in Vietnamese (include FAQs; latest information on CAH; messages of support from international community) and videos to raise awareness [50]; Club reports (English) shared with all key partners internationally; success stories/videos shared internationally (CLAN website/social media); CLAN panel at 2010 UN Department of Public Information for Non-Government Organisations (UNDPI/NGO) Conference in Melbourne; APPES Declaration 2018 [51]. | |
| Pillar 3. Optimisation of medical management | Primary prevention Genetic counselling education and training |
| Secondary prevention Staff training and education to promote early diagnosis; availability of 17 Hydroxyprogesterone (17OHP) testing for diagnosis and monitoring; newborn screening (NBS) pilot scaled to national program. | |
| Tertiary prevention Staff and family education and training; educational resources and clinical guidelines available in Vietnamese; affordable access to essential monitoring and equipment (such as 17OHP, renin, genetic testing and injection kits); support for gynaecology and surgical teams to exchange internationally [52]; and promotion of growth charts for routine monitoring. | |
| Holistic care Strengthened focus on patient and family centred care; training in psychological support; information about pregnancy for people living with CAH. | |
| Pillar 4. Encourage Support Groups | Support of annual Club meetings; CAH Club executive nominated; communication networks established (Facebook, Whats App, Twitter, Instagram); connections with international CAH support networks facilitated; training sessions facilitated for families and health professionals; success stories from international CAH Communities shared to inspire. |
| Pillar 5. Reduce financial burdens | Children encouraged to attend school; awards for school performance; education on emergency management/injection kits reduce need to travel; medicine affordably available (on national insurance scheme) and facilitation of international supply chains to optimise pricing; systematic outpatient care (reduce travel and unapproved expenses). |
| Pillar 6. Ethical & transparent management | CLAN incorporated as non-governmental organisation in Australia [13]; fundraising certification; ethical governance and accountability processes; multilateral engagement, reporting and accountability. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armstrong, K.; Benedict Yap, A.; Chan-Cua, S.; Craig, M.E.; Cole, C.; Chi Dung, V.; Hansen, J.; Ibrahim, M.; Nadeem, H.; Pulungan, A.; et al. We All Have a Role to Play: Redressing Inequities for Children Living with CAH and Other Chronic Health Conditions of Childhood in Resource-Poor Settings. Int. J. Neonatal Screen. 2020, 6, 76. https://doi.org/10.3390/ijns6040076
Armstrong K, Benedict Yap A, Chan-Cua S, Craig ME, Cole C, Chi Dung V, Hansen J, Ibrahim M, Nadeem H, Pulungan A, et al. We All Have a Role to Play: Redressing Inequities for Children Living with CAH and Other Chronic Health Conditions of Childhood in Resource-Poor Settings. International Journal of Neonatal Screening. 2020; 6(4):76. https://doi.org/10.3390/ijns6040076
Chicago/Turabian StyleArmstrong, Kate, Alain Benedict Yap, Sioksoan Chan-Cua, Maria E. Craig, Catherine Cole, Vu Chi Dung, Joseph Hansen, Mohsina Ibrahim, Hassana Nadeem, Aman Pulungan, and et al. 2020. "We All Have a Role to Play: Redressing Inequities for Children Living with CAH and Other Chronic Health Conditions of Childhood in Resource-Poor Settings" International Journal of Neonatal Screening 6, no. 4: 76. https://doi.org/10.3390/ijns6040076
APA StyleArmstrong, K., Benedict Yap, A., Chan-Cua, S., Craig, M. E., Cole, C., Chi Dung, V., Hansen, J., Ibrahim, M., Nadeem, H., Pulungan, A., Raza, J., Utari, A., & Ward, P. (2020). We All Have a Role to Play: Redressing Inequities for Children Living with CAH and Other Chronic Health Conditions of Childhood in Resource-Poor Settings. International Journal of Neonatal Screening, 6(4), 76. https://doi.org/10.3390/ijns6040076