Landscape of Congenital Adrenal Hyperplasia Newborn Screening in the United States


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. NewSTEPs State Profiles
2.2. CAH Data Request
2.3. CAH Data Query and Analytics
3. Results
3.1. State Profile Data
3.2. Methodology for Screening
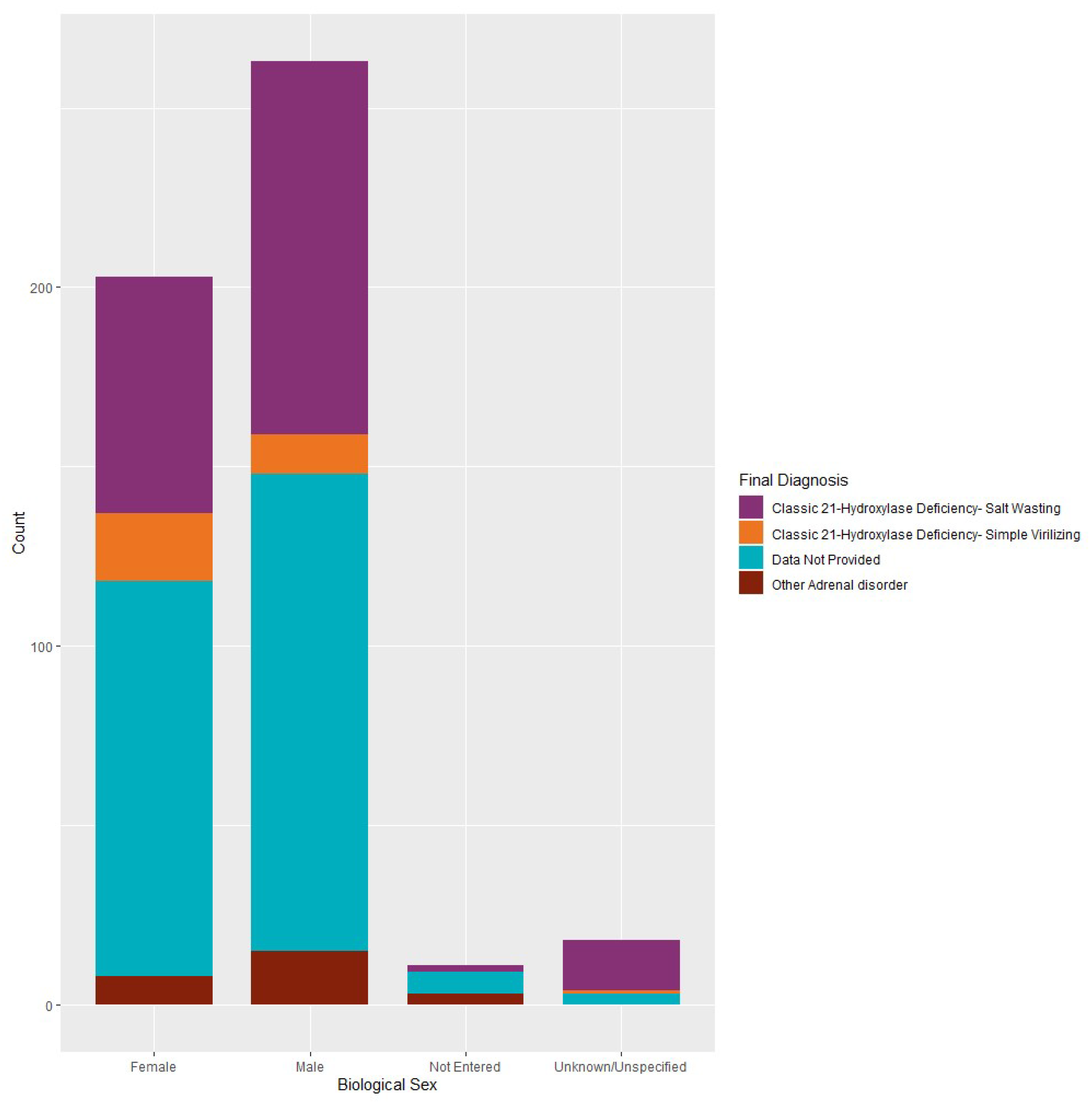
3.3. Confirmed Case Data
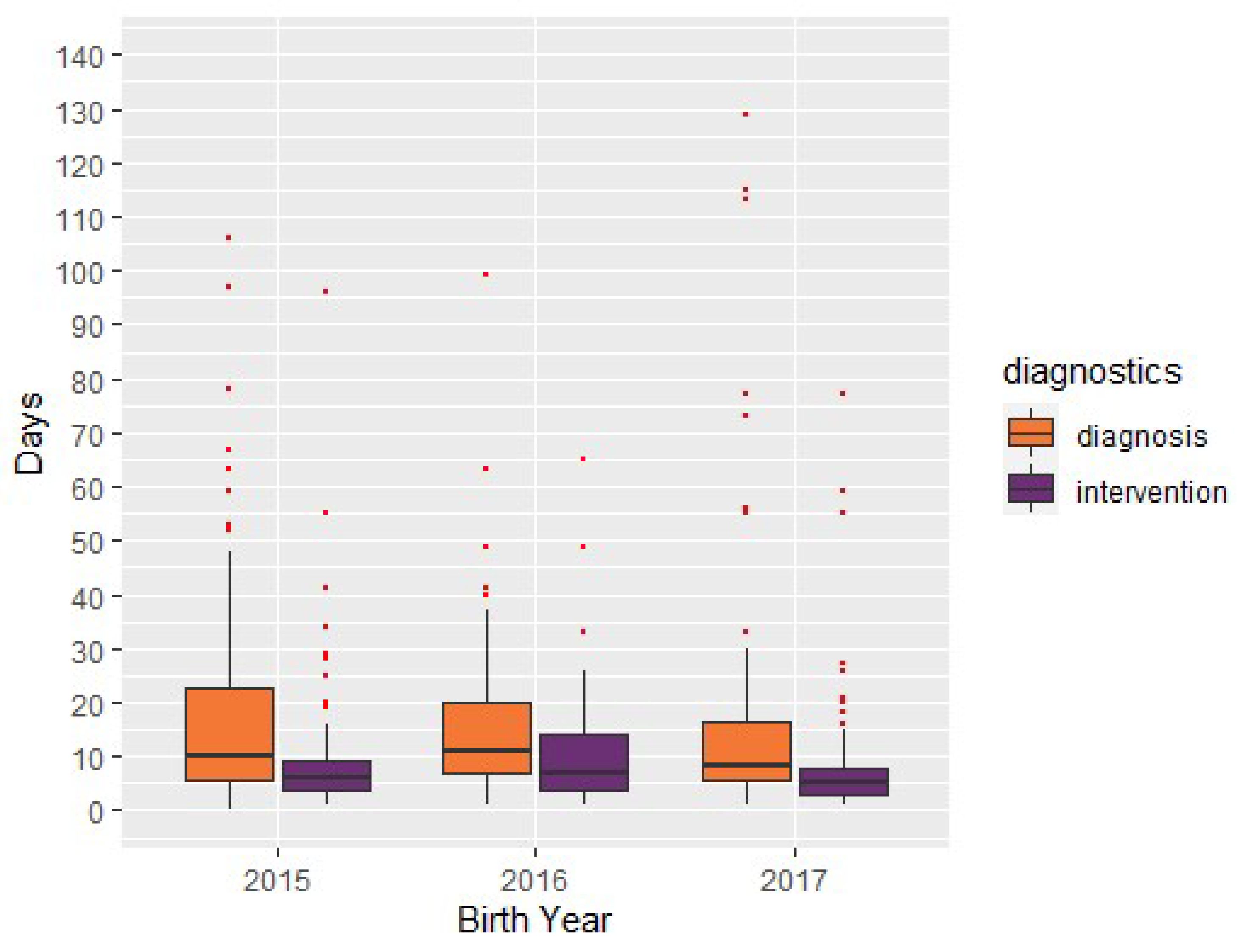
3.4. Diagnostic Workup Data
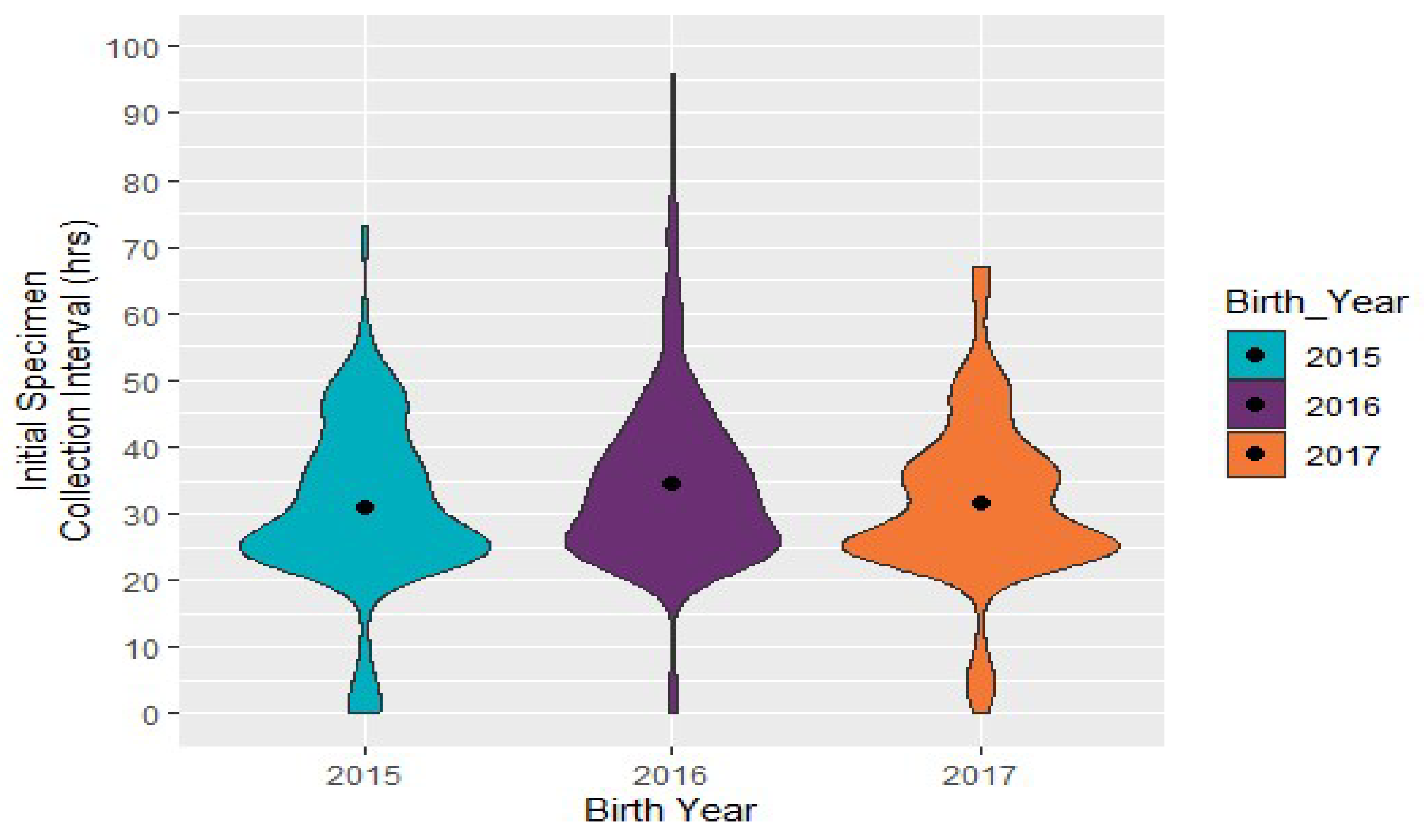
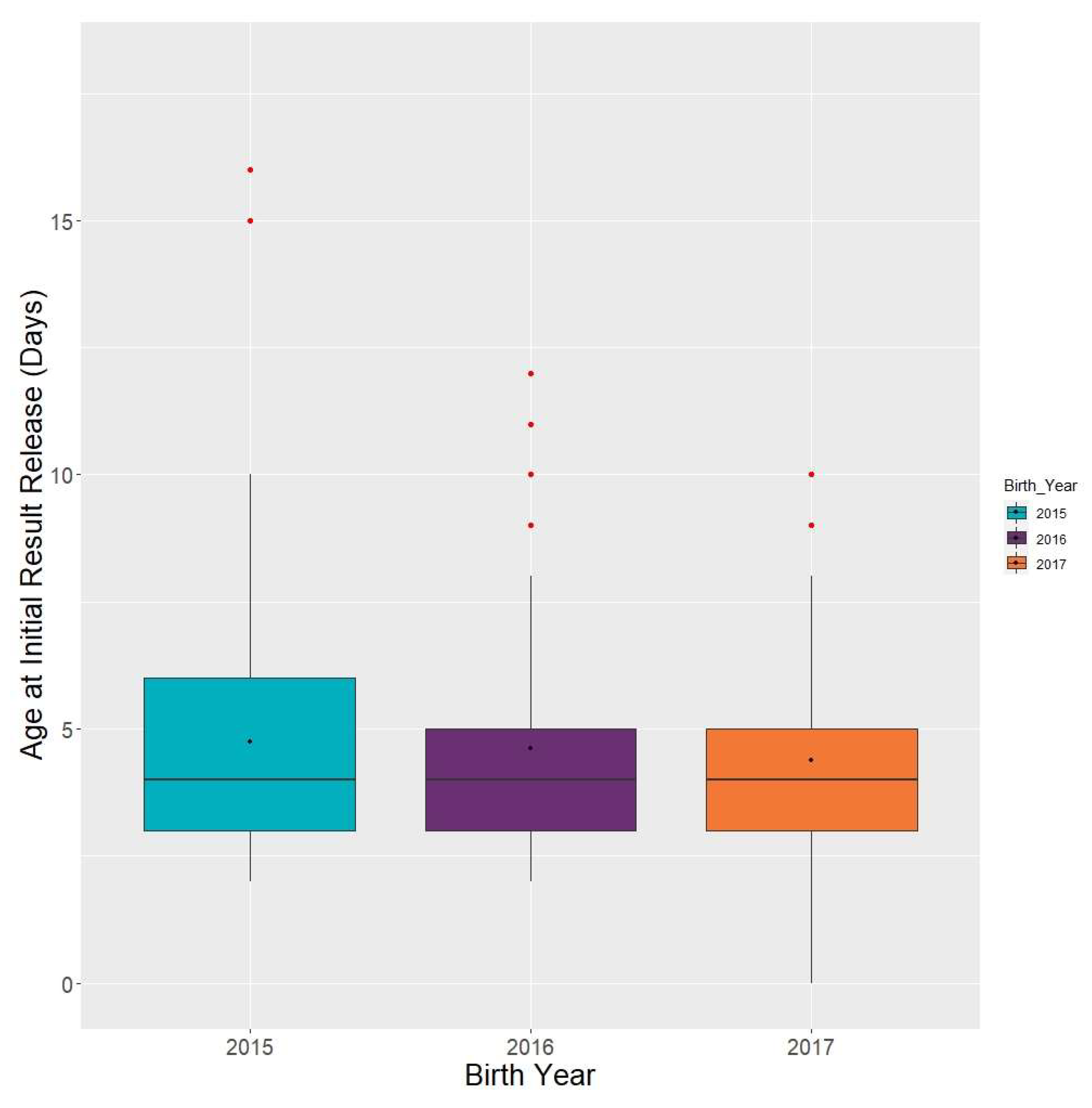
3.5. Timeliness Data
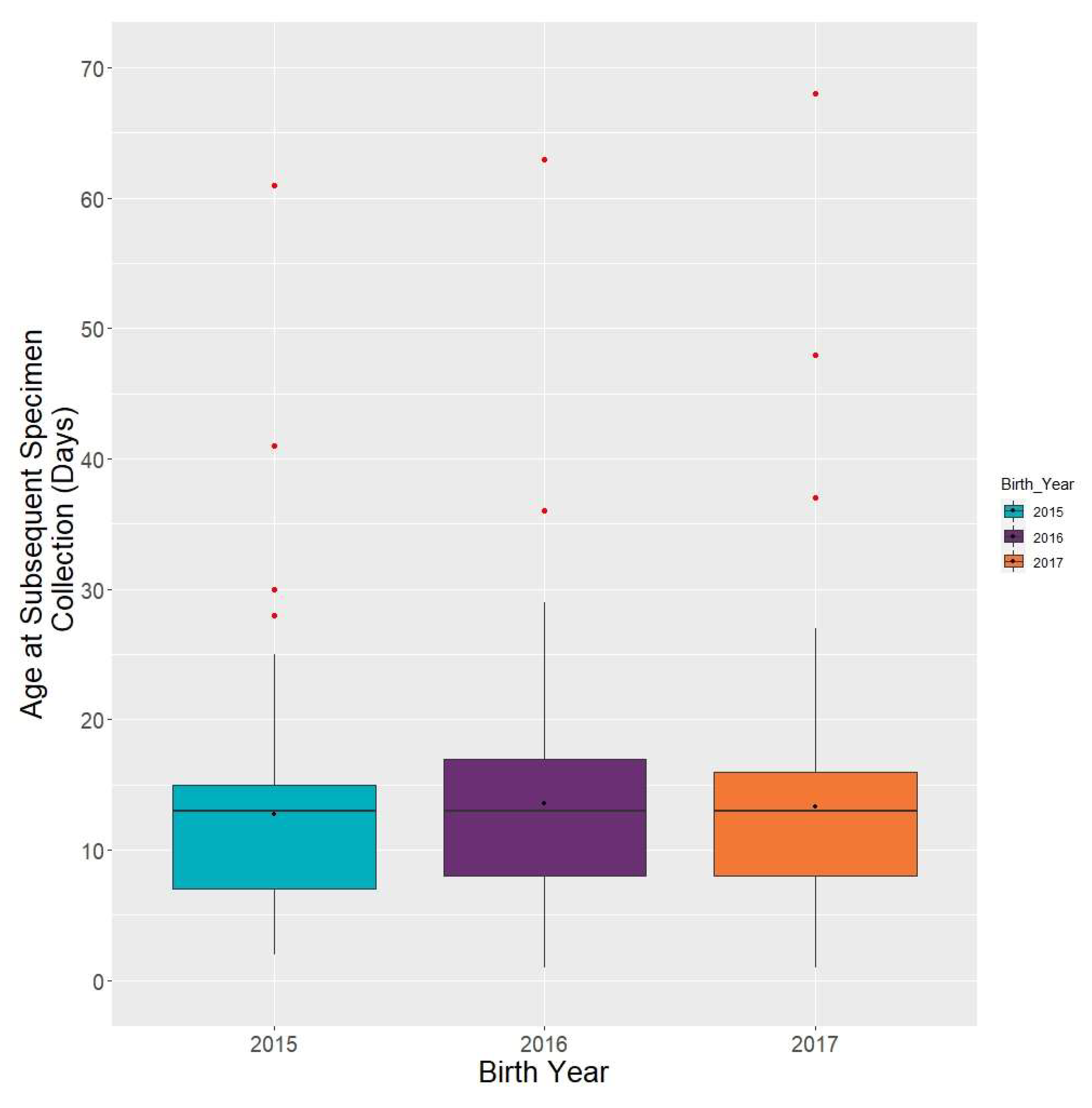
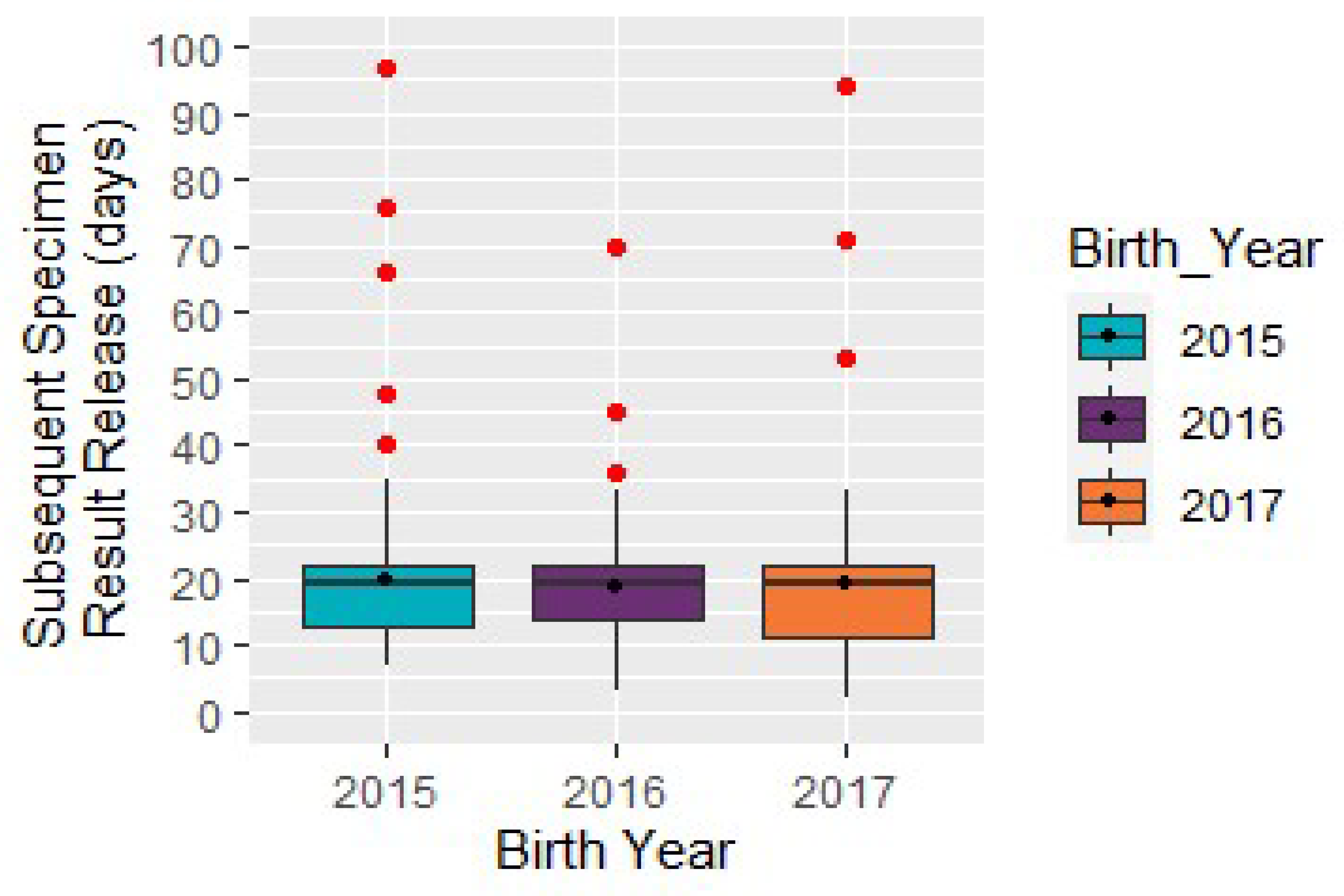
3.6. Subsequent Specimen Collection
4. Discussion
4.1. State Profile Data
4.2. Confirmed Case Data
4.3. Timeliness Data
- Standard confirmatory testing: Clinician draws electrolytes and 17-OHP;
- Electrolytes may or may not indicate need for urgent intervention, however a decision is rendered based on laboratory results and the clinical presentation of the infant;
- Advanced confirmatory testing: In cases in which exam or presentation strongly suggests diagnosis of CAH, additional adrenal testing may be warranted in consultation with endocrinologist.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- NewSTEPs 2019 Annual Report. Available online: https://www.newsteps.org/sites/default/files/nbs-newsteps-2019-annual-report.pdf (accessed on 5 May 2020).
- Merke, D.; Kabbani, M. Congenital adrenal hyperplasia: Epidemiology, management and practical drug treatment. Pediatr. Drugs 2001, 3, 599–611. [Google Scholar] [CrossRef] [PubMed]
- White, P. Neonatal screening for congenital adrenal hyperplasia. Nat. Rev. Endocrinol. 2009, 5, 490–498. [Google Scholar] [CrossRef] [PubMed]
- NewSTEPs. Available online: https://www.newsteps.org/ (accessed on 5 May 2020).
- Ojodu, J.; Singh, S.; Kellar-Guenther, Y.; Yusuf, C.; Jones, E.; Wood, T.; Baker, M.; Sontag, M.K. NewSTEPs: The Establishment of a National Newborn Screening Technical Assistance Resource Center. Int. J. Neonatal Screen. 2018, 4, 1. [Google Scholar] [CrossRef]
- NewSTEPs Data Repository User Guide. Available online: https://www.newsteps.org/sites/default/files/newsteps_general_user_guide_june2018_se.pdf (accessed on 5 May 2020).
- Sontag, M.K.; Sarkar, D.; Comeau, A.M.; Hassell, K.; Botto, L.D.; Parad, R.; Rose, S.R.; Wintergerst, K.A.; Smith-Whitley, K.; Singh, S.; et al. Case Definitions for Conditions Identified by Newborn Screening Public Health Surveillance. Int. J. Neonatal Screen. 2018, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Newborn Screening Follow-up; Approved Guideline—Second Edition; CLSI document NBS02-A2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2013.
- NewSTEPs List of Time-critical Disorders. Available online: https://www.newsteps.org/sites/default/files/case-definitions/qi_source_document_time_critical_disorders_0.pdf (accessed on 5 May 2020).
- Definition of Term Pregnancy. Available online: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/11/definition-of-term-pregnancy (accessed on 8 July 2020).
- Health Resources and Services Administration Federal Advisory Committees: Newborn Screening Timeliness Goals. Available online: https://www.hrsa.gov/advisory-committees/heritable-disorders/newborn-screening-timeliness.html (accessed on 21 May 2020).
- NewSTEPs Quality Indicator Source Document. Available online: https://www.newsteps.org/sites/default/files/quality-indicators/quality_indicator_source_document_july_17_2018_se.pdf (accessed on 5 May 2020).
- NewSTEPs Definitions for Medical Intervention and Diagnosis by Disorder. Available online: https://www.newsteps.org/sites/default/files/case-definitions/case_definition_overview_summary_feb62017.pdf (accessed on 5 May 2020).
- Held, P.K.; Shapira, S.K.; Hinton, C.F.; Jones, E.; Hannon, W.H.; Ojodu, J. Congenital adrenal hyperplasia cases identified by newborn screening in one- and two-screen states. Mol. Genet. Metab. 2015, 116, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Sontag, M.K.; Miller, J.I.; McKasson, S.; Sheller, R.; Edelman, S.; Yusuf, C.; Singh, S.; Sarkar, D.; Bocchini, J.; Scott, J.; et al. Newborn screening timeliness quality improvement initiative: Impact of national recommendations and data repository. PLoS ONE 2020, 15, e0231050. [Google Scholar] [CrossRef] [PubMed]
- New, M.; Yau, M.; Lekarev, O.; Lin-Su, K.; Parsa, A.; Pina, C.; Yuen, T.; Khattab, A. Congenital Adrenal Hyperplasia. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Dungan, K., Grossman, A., Hershman, J.M., Kaltsas, G., Koch, C., Kopp, P., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK278953/ (accessed on 15 March 2017).
- Speiser, P.W.; Chawla, R.; Chen, M.; Diaz-Thomas, A.; Finlayson, C.; Rutter, M.M.; Sandberg, D.E.; Shimy, K.; Talib, R.; Cerise, J.; et al. Newborn Screening Protocols and Positive Predictive Value for Congenital Adrenal Hyperplasia Vary across the United States. Int. J. Neonatal Screen. 2020, 6, 37. [Google Scholar] [CrossRef]
- NewSTEPs Case Definitions for Newborn Screening. Available online: https://www.newsteps.org/sites/default/files/case-definitions/classificationtablesmaster_12.13.19_se.pdf (accessed on 5 May 2020).
- van der Kamp, H.J.; Oudshoorn, C.G.M.; Elvers, B.H.; van Baarle, M.; Otten, B.J.; Wit, J.M.; Verkerk, P.H. Cutoff Levels of 17-α-Hydroxyprogesterone in Neonatal Screening for Congenital Adrenal Hyperplasia Should Be Based on Gestational Age Rather Than on Birth Weight. J. Clin. Endocrinol. Metab. 2005, 90, 3904–3907. [Google Scholar] [CrossRef] [PubMed]











© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edelman, S.; Desai, H.; Pigg, T.; Yusuf, C.; Ojodu, J. Landscape of Congenital Adrenal Hyperplasia Newborn Screening in the United States. Int. J. Neonatal Screen. 2020, 6, 64. https://doi.org/10.3390/ijns6030064
Edelman S, Desai H, Pigg T, Yusuf C, Ojodu J. Landscape of Congenital Adrenal Hyperplasia Newborn Screening in the United States. International Journal of Neonatal Screening. 2020; 6(3):64. https://doi.org/10.3390/ijns6030064
Chicago/Turabian StyleEdelman, Sari, Hiral Desai, Trey Pigg, Careema Yusuf, and Jelili Ojodu. 2020. "Landscape of Congenital Adrenal Hyperplasia Newborn Screening in the United States" International Journal of Neonatal Screening 6, no. 3: 64. https://doi.org/10.3390/ijns6030064
APA StyleEdelman, S., Desai, H., Pigg, T., Yusuf, C., & Ojodu, J. (2020). Landscape of Congenital Adrenal Hyperplasia Newborn Screening in the United States. International Journal of Neonatal Screening, 6(3), 64. https://doi.org/10.3390/ijns6030064