Building a Newborn Screening Information Management System from Theory to Practice

Abstract
1. Introduction
2. Theory
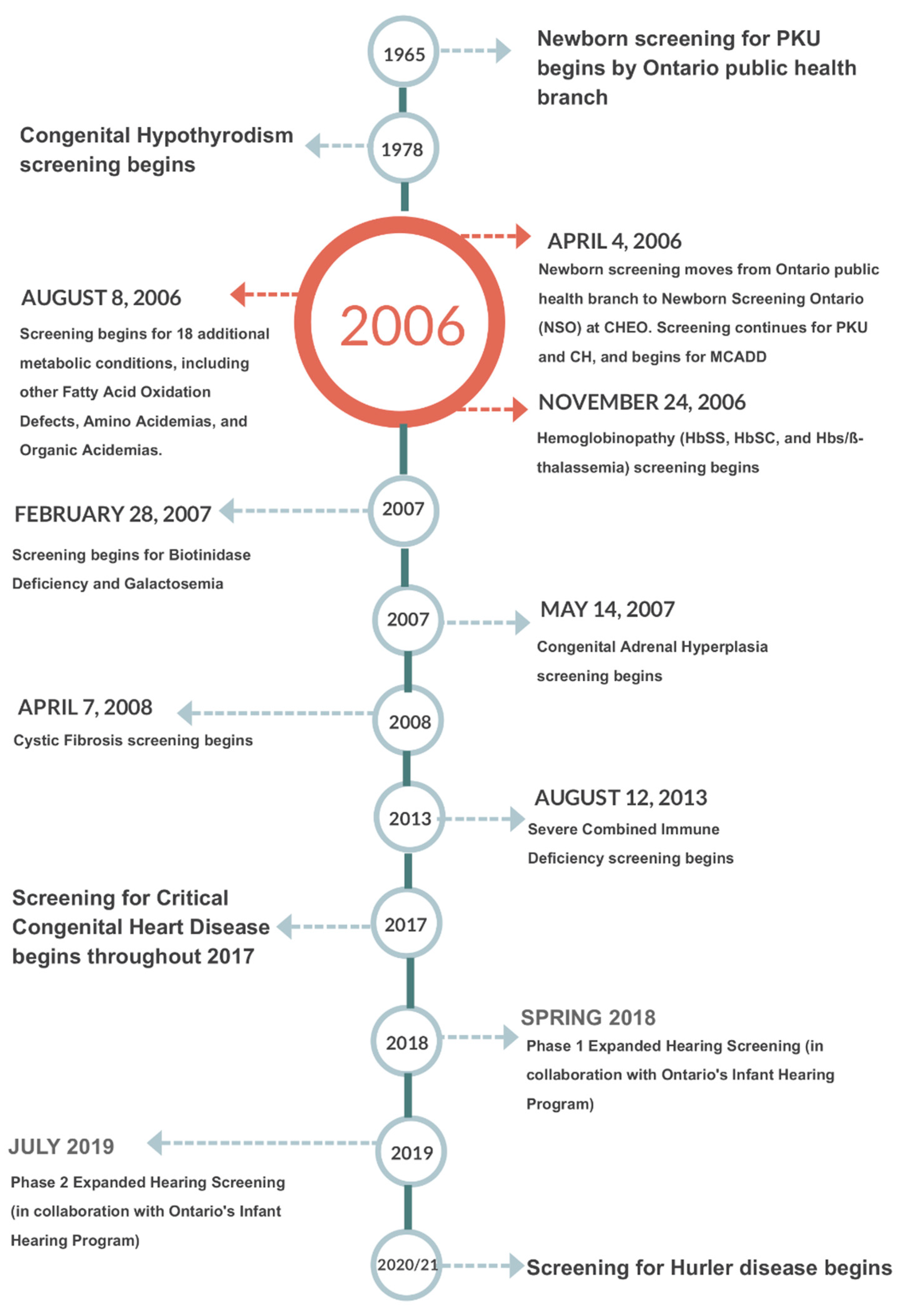
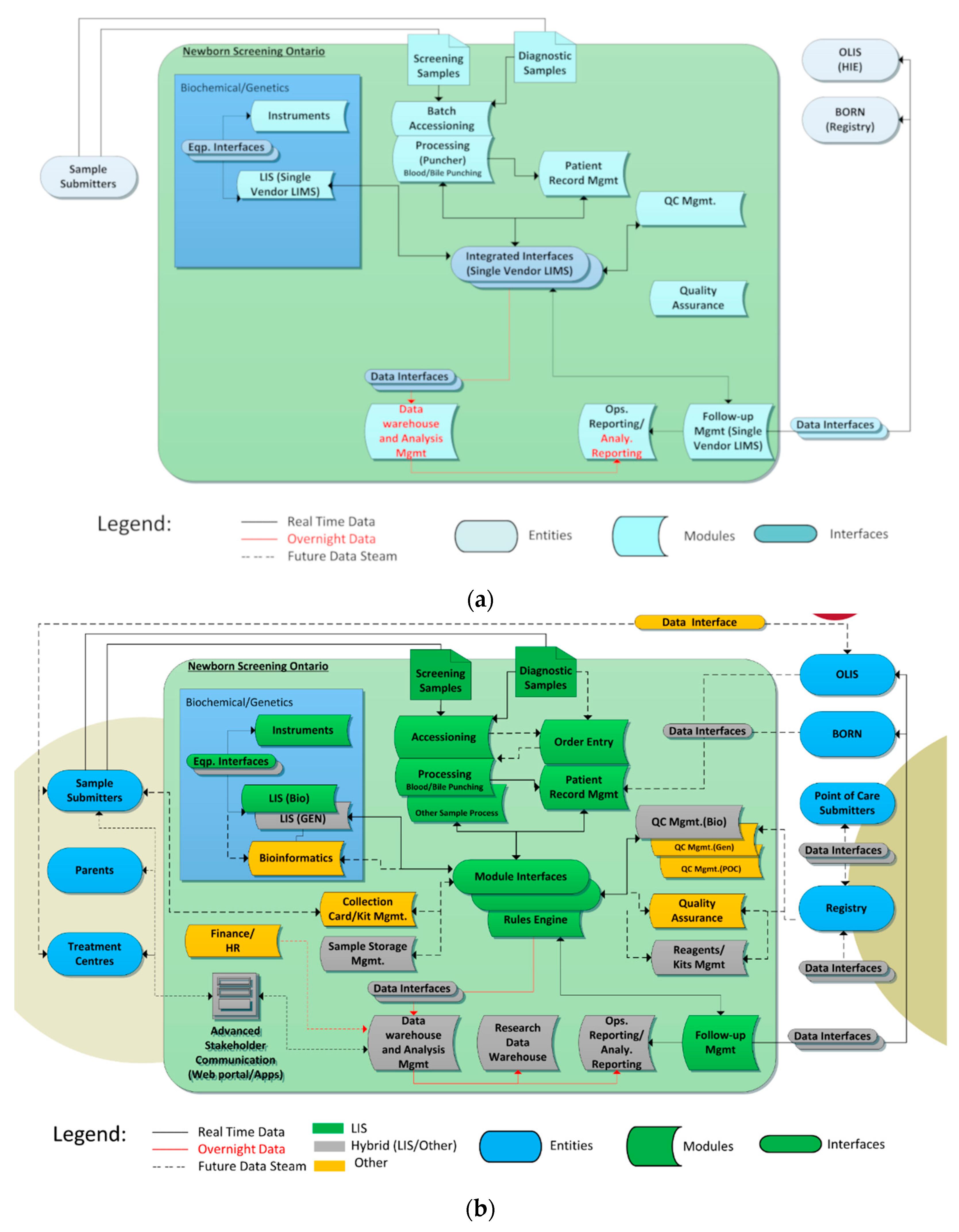
2.1. Outgrowing NSO’s Current SIMS
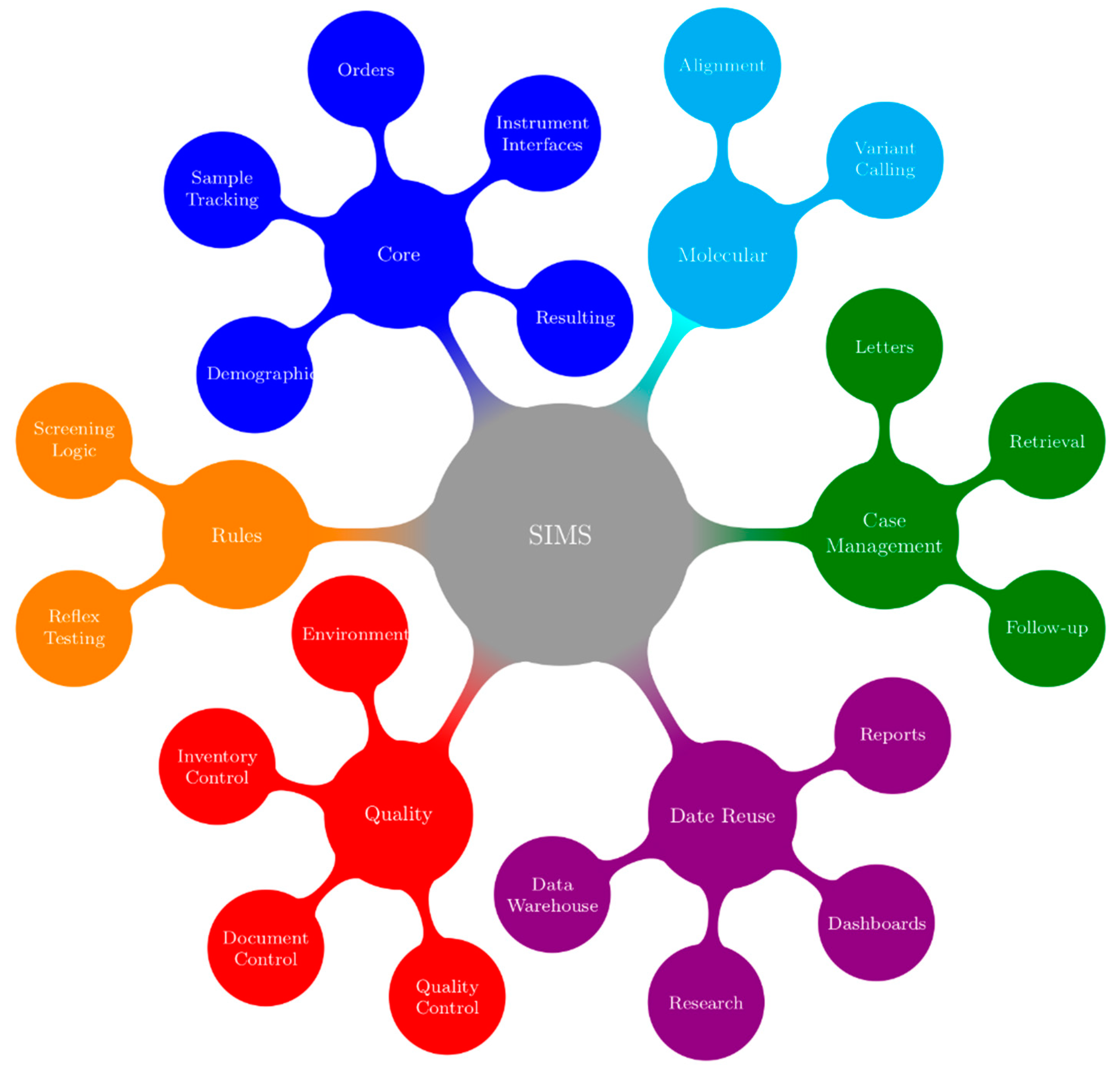
2.2. Designing an “IDEAL” SIMS for NSO
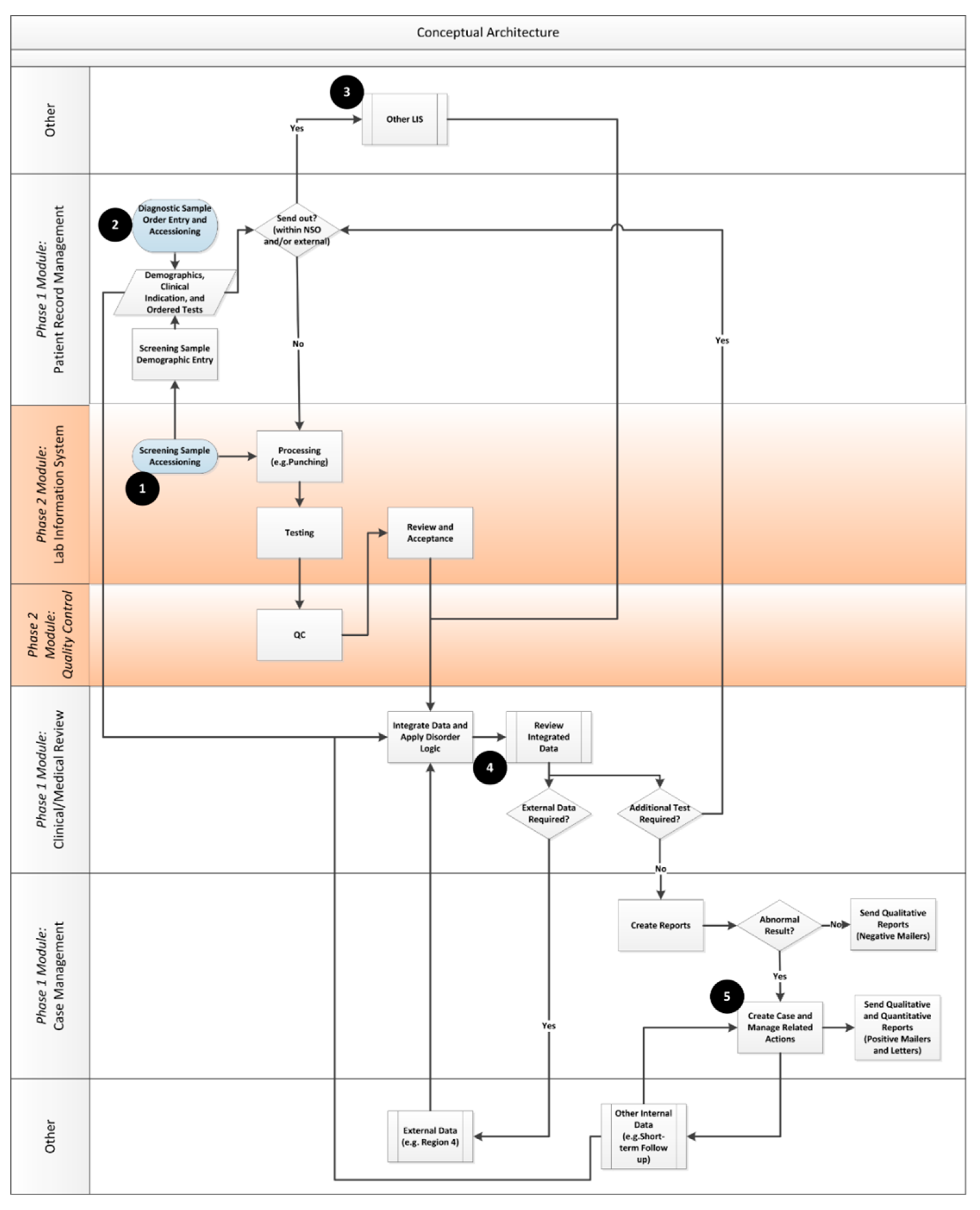
- Patient Record Management: This module is expected to handle most of the pre-analytical aspects of NSO. The module will be used to receive samples in the laboratory and to enter demographic data for these samples. It consists of a number of processes including, however not limited to: Receiving samples; demographic/clinical indication data entry and validation; test ordering (batch and custom); linking multiple samples to a patient; triggering work-flows for samples that are unsatisfactory for testing and ensuring electronic transmission receipt of key information (e.g., demographics in, results out) via HL7 and related protocols.
- Laboratory Information System (LIS)/Quality Control (QC): These modules will be expected to handle most of the analytical and QC data including work-flows and dataflows within the NSO laboratory environment.
- Clinical/medical review: The review and releasing of results is a critical component of laboratory information work-flow between the technologists and medical/scientific staff. This module is designed to apply pre-programmed logic to distill critical lab information in order to produce actionable results in an efficient manner. The Clinical/medical review module will consist of a configurable rules-based system that integrates information from multiple data sources, applies disorder logic and streamlines work-flows to drive decisions. It will also include a rules-based expert system including a web-based graphical user interface (GUI) to support the review and reporting functions, an administrative interface for creating and managing rules and a user configurable knowledge base that is “human readable”. In its first iteration, this functionality will be imbedded in the core SIMS. The possibility of using an independent rules engine service that can be made available to multiple systems in the longer term will also be explored.
- Case management: This module will be expected to handle most of the post-analytical aspects of NSO including follow up with submitters and treatment centres.
- Sample Lifecycle Management: The need to track blood collection cards throughout their lifecycle from distribution through transport to storage is a key and sometimes overlooked process within newborn screening program management. A local vendor has worked with NSO to develop a system that helps manage sample card inventory management, track the transport of samples and card usage, monitor expiry dates for filter paper and is working towards tracking in lab samples, off-site storage and destruction.
- Reporting and Analytics: In order to support the data intensive nature of newborn screening results, NSO has developed a data warehouse to enable user controlled data access and to manage automated and ad-hoc reporting on all types of NSO data.
- Decision support—Third party products can be linked in to provide decision support to key decision makers to assist in timely, effective decision making.
3. Practice
3.1. Technical Considerations
3.2. User Considerations
3.3. Procurement Considerations
3.4. Implementation Considerations
3.5. Organizational and Jurisdictional Considerations
3.6. Project Benefits and Impacts
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- CLIR—Collaborative Laboratory Integrated Reports—About CLIR. Available online: https://clir.mayo.edu/Home/About (accessed on 26 November 2018).
- Pantanowitz, L.; Henricks, W.H.; Beckwith, B.A. Medical Laboratory Informatics. Clin. Lab. Med. 2007, 27, 823–843. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, J.L.; Young, D.S. The Ideal Laboratory Information System. Arch. Pathol. Lab. Med. 2013, 137, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Newborn Screening Ontario CCHD Screening. Available online: https://www.newbornscreening.on.ca/en/health-care-providers/submitters/cchd-screening-implementation (accessed on 26 November 2018).
- Newborn Screening Ontario Expanded Hearing Screening. Available online: https://www.newbornscreening.on.ca/en/page/overview (accessed on 26 November 2018).
- Federal Advisory Committees—Recommended Uniform Screening Panel. Available online: https://www.hrsa.gov/advisory-committees/heritable-disorders/rusp/index.html (accessed on 26 November 2018).
- Secretary’s Advisory Committee on Heritable Disorders in Newborns and Children; 2011 Annual Report to Congress. (PDF-871 KB). Available online: http://www.hrsa.gov/advisorycommittees/mchbadvisory/heritabledisorders/reportsrecommendations/reports/sachdnc2011report.pdf (accessed on 20 February 2018).
- McCudden, C.R.; Henderson, M.P.A. Laboratory Information Systems. In Contemporary Practice in Clinical Chemistry, 3rd ed.; Clarke, W., Ed.; AACC: Washington, DC, USA, 2016; pp. 263–276. ISBN 9781594251894. [Google Scholar]
- Huhns, M.N.; Singh, M.P. Service-oriented computing: Key concepts and principles. IEEE Internet Comput. 2005, 9, 75–81. [Google Scholar]
- Hermann, S.A. Best-of-breed versus integrated systems. Am. J. Health-Syst. Pharm. 2010, 67, 1406–1410. [Google Scholar] [CrossRef] [PubMed]
- Mulder, P. Decision Matrix Analysis. From ToolsHero. 2018. Available online: https://www.toolshero.com/decision-making/decision-matrix-analysis/ (accessed on 27 November 2018).
- Newborn Screening Ontario—Newborn Screening Advisory Council. Available online: https://www.newbornscreening.on.ca/en/advisory-council (accessed on 26 November 2018).
- Epic Systems Corporation. Available online: https://www.epic.com/ (accessed on 26 November 2018).
- Cerner Corporation. Available online: https://www.cerner.com/ (accessed on 26 November 2018).
- Ward, J.; Elvin, R. A new framework for managing IT-enabled business change. Inf. Syst. J. 1999, 9, 197–221. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical/Medical Review-BR-001: Solution will Receive Input from Multiple Sources. The Solution must Provide the Ability to Receive and Configure Data from Multiple Sources using Standard Messaging Formats (e.g. HL7, XML), Text Files, and Direct Database Connections. | ||||
|---|---|---|---|---|
| Related Detailed Requirements | ||||
| Name | Description | Mandatory/Desirable | Status—(Mandatory must be 3 or 4) | Description of Functional Solution and Discussion of Status |
| Clinical/Medical Review-FR-001: Configure input for demographic data | The solution will be able to configure and accept input for demographic data, clinical indications and historical patient information including but not limited to linked samples and previous test results. | Mandatory | ||
| Clinical/Medical Review-FR-002: Configure input for lab results | The system will be able to configure and accept input for laboratory tests and assay/sample results at any stage (e.g. pending, preliminary, post QC, final) from any LIS or directly from instruments. The input must include notes and flags relating to quality control at the sample plate or assay level. | Mandatory | ||
| Clinical/Medical Review-FR-003: Configure input for qualitative and quantitative results | The solution will be able to configure and accept input for test results, both quantitative and qualitative ( including but not limited to images such as total ion counts and hemoglobin chromatograms) | Mandatory | ||
| Clinical/Medical Review-FR-004: Configure input for other internal data | The solution will be able to configure and accept input for other internal data such as short term follow-up data including but not limited to diagnostic test results, definitive diagnoses, and courses of treatment. | Mandatory | ||
| Clinical/Medical Review-FR-005: Configure input for external data | The system will be able to configure and accept input from external data sources including but not limited to external knowledge bases or analytical results from external entities (e.g. Region 4) | Mandatory | ||
| Environment Name | Usage | COTS Software Version | NSO Configuration/Rules Version | Data |
|---|---|---|---|---|
| Development | Developing and testing NSO configuration and rule changes Testing new product builds/product upgrades | Latest software build being tested | Production rules as a base with any changes in progress | Test data only |
| Test | Deployment testing (DEV to TEST) Sanity testing of new product build and NSO configuration and rule changes Regression testing UAT Training Troubleshooting production issues (e.g., replicating cases on anonymized production data) End-to-end testing with external interfaces with anonymized production data | Same as production For new releases, updated to be same as DEV once DEV build/configuration passed Lancet testing (i.e., production candidate) and close to moving to PROD release During Software builds/product upgrades, contains updated software When no Software product upgrades in progress, same as production | Production rules when testing Software builds / product upgrades and/or troubleshooting production issues New/updated rules when doing final tests on anonymized production data prior to release | Anonymized production data Test data |
| Production | Production use Sanity testing of new NSO rule changes on production data through the use of test patients | Production | Production | Production data Test data (for test patients only) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pluscauskas, M.; Henderson, M.; Milburn, J.; Chakraborty, P. Building a Newborn Screening Information Management System from Theory to Practice. Int. J. Neonatal Screen. 2019, 5, 9. https://doi.org/10.3390/ijns5010009
Pluscauskas M, Henderson M, Milburn J, Chakraborty P. Building a Newborn Screening Information Management System from Theory to Practice. International Journal of Neonatal Screening. 2019; 5(1):9. https://doi.org/10.3390/ijns5010009
Chicago/Turabian StylePluscauskas, Michael, Matthew Henderson, Jennifer Milburn, and Pranesh Chakraborty. 2019. "Building a Newborn Screening Information Management System from Theory to Practice" International Journal of Neonatal Screening 5, no. 1: 9. https://doi.org/10.3390/ijns5010009
APA StylePluscauskas, M., Henderson, M., Milburn, J., & Chakraborty, P. (2019). Building a Newborn Screening Information Management System from Theory to Practice. International Journal of Neonatal Screening, 5(1), 9. https://doi.org/10.3390/ijns5010009