Newborn Screening for Primary T- and B-Cell Immune Deficiencies—A Prospective Study in Andalucía

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Data
3.2. TREC/KREC/ACTB Assay Performance
3.3. TREC and KREC Levels According to GA and BW
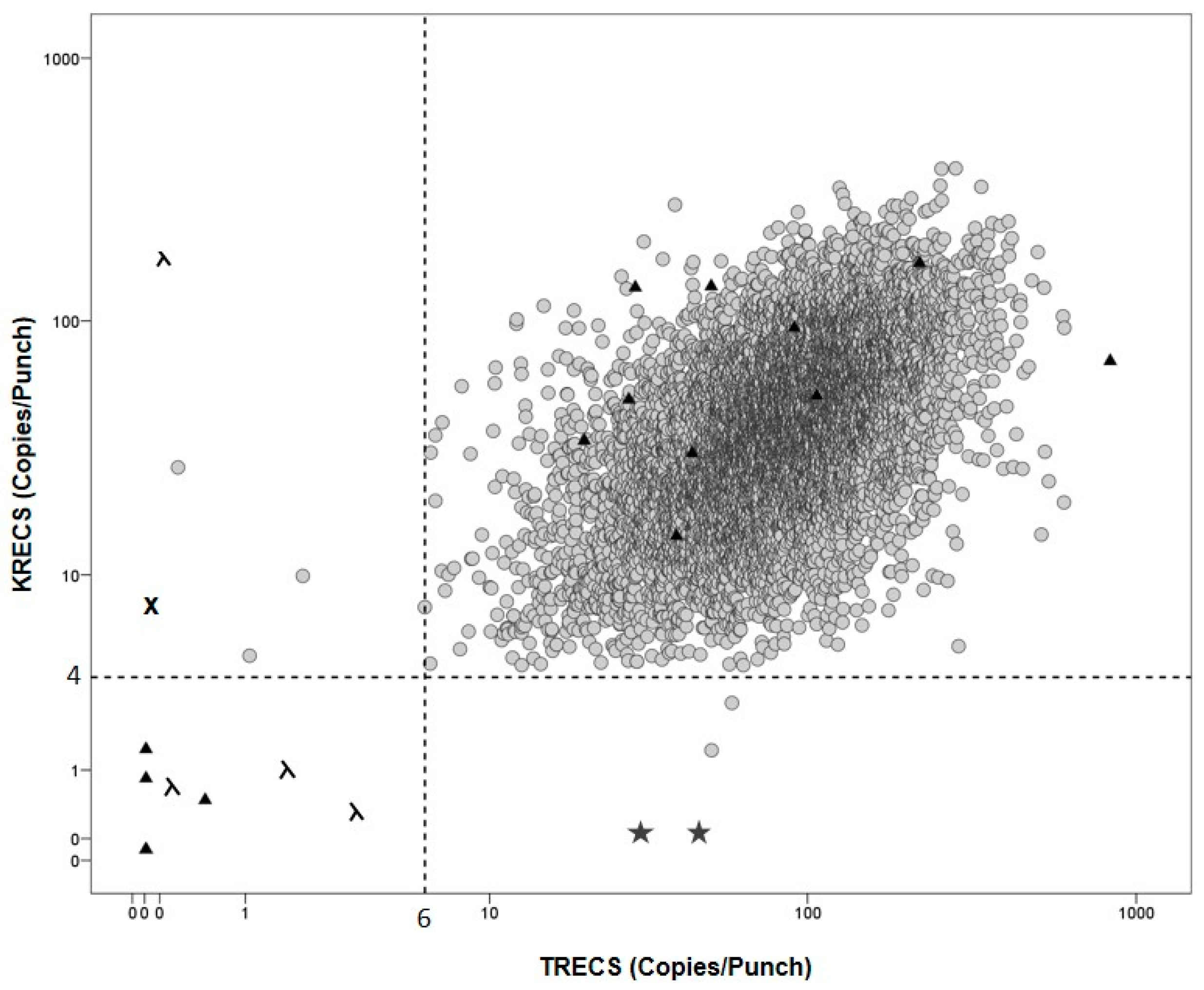
3.4. Positive Results
3.5. External Control Samples
3.6. Internal Control Samples
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Borte, S.; von Döbeln, U.; Hammarström, L. Guidelines for newborn screening of primary immunodeficiency diseases. Curr. Opin. Hematol. 2013, 20, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Modell, V.; Knaus, M.; Modell, F. An analysis and decision tool to measure cost benefit of newborn screening for severe combined immunodeficiency (SCID) and related T-cell lymphopenia. Immunol. Res. 2014, 60, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Van der Spek, J.; Groenwold, R.H.; van der Burg, M.; van Montfrans, J.M. TREC based Newborn Screening for Severe Combined Immunodeficiency Disease: A Systematic Review. J. Clin. Immunol. 2015, 35, 416–430. [Google Scholar] [CrossRef] [PubMed]
- Clément, M.C.; Mahlaoui, N.; Mignot, C.; Le Bihan, C.; Rabetrano, H.; Hoang, L.; Neven, B.; Moshous, D.; Cavazzana, M.; Blanche, S.; et al. Systematic neonatal screening for severe combined immunodeficiency and severe T-cell lymphopenia: Analysis of cost-effectiveness based on French real field data. J. Allergy Clin. Immunol. 2015, 135, 1589–1593. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Thompson, J.D.; Kobrynski, L.; Ojodu, J.; Zarbalian, G.; Grosse, S.D. Cost-Effectiveness/Cost-Benefit Analysis of Newborn Screening for Severe Combined Immune Deficiency in Washington State. J. Pediatr. 2016, 172, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Subbarayan, A.; Colarusso, G.; Hughes, S.M.; Gennery, A.R.; Slatter, M.; Cant, A.J. Clinical features that identify children with primary immunodeficiency. Pediatrics 2011, 127, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.; Xu-Bayford, J.; Allwood, Z.; Slatter, M.; Cant, A.; Davies, E.G. Neonatal diagnosis of severe combined immunodeficiency leads to significantly improved survival outcome: The case of newborn screening. Blood 2011, 17, 2443–2446. [Google Scholar]
- Chan, A.; Scalchunes, C.; Boyle, M.; Puck, J.M. Early vs. delayed diagnosis of severe combined immunodeficiency: A family perspective survey. Clin. Immunol. 2011, 138, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Olbrich, P.; de Felipe, B.; Delgado-Pecellin, C.; Rodero, R.; Rojas, P.; Aguayo, J.; Marquez, J.; Casanovas, J.; Sanchez, B.; Lucena, J.M.; et al. A first pilot study on the neonatal screening of primary immunodeficiencies in Spain: TRECS and KRECS identify severe T- and B-cell lymphopenia. An. Pediatr. 2014, 81, 310–317. [Google Scholar] [CrossRef] [PubMed]
- De Felipe, B.; Olbrich, P.; Lucenas, J.M.; Delgado-Pecellin, C.; Pavon-Delgado, A.; Marquez, J.; Salamanca, C.; Soler-Palacin, P.; Gonzalez-Granado, L.I.; Antolin, L.F.; et al. Prospective neonatal screening for severe T- and B-lymphocyte deficiencies in Seville. Pediatr. Allergy Immunol. 2016, 27, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Borte, S.; von Döbeln, U.; Fasth, A.; Wang, N.; Janzi, M.; Winiarski, J.; Sack, U.; Pan-Hammarström, Q.; Borte, M.; Hammarström, L. Neonatal screening for severe primary immunodeficiency diseases using high-throughput triplex real-time PCR. Blood 2012, 119, 2552–2555. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.; Ohlsson, A.; Borte, S.; Jonsson, S.; Zetterström, R.H.; King, J.; Winiarski, J.; von Döbeln, U.; Hammarström, L. Newborn Screening for Severe Primary Immunodeficiency Diseases in Sweden-a 2-Year Pilot TREC and KREC Screening Study. J. Clin. Immunol. 2017, 37, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Audrain, M.; Thomas, C.; Mirallie, S.; Bourgeois, N.; Sebille, V.; Rabetrano, H.; Durand-Zaleski, I.; Boisson, R.; Persyn, M.; Pierres, C.; et al. Evaluation of the T-cell receptor excision circle assay performances for severe combined immunodeficiency neonatal screening on Guthrie cards in a French single centre study. Clin. Immunol. 2014, 150, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.P.; Rashid, S.; Premachandra, T.; Harvey, K.; Ifederu, A.; Wilson, M.C.; Gaspar, H.B. Screening of neonatal UK dried blood spots using a duplex TREC screening assay. J. Clin. Immunol. 2014, 34, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Kwan, A.; Abraham, R.S.; Currier, R.; Brower, A.; Andruszewski, K.; Abbott, J.K.; Baker, M.; Ballow, M.; Bartoshesky, L.E.; Bonilla, F.A.; et al. Newborn screening for severe combined immunodeficiency in 11 screening programs in the United States. JAMA 2014, 312, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Rechavi, E.; Lev, A.; Lee, Y.N.; Simon, A.J.; Yinon, Y.; Lipitz, S.; Amariglio, N.; Weisz, B.; Notarangelo, L.D.; Somech, R. Timely and spatially regulated maturation of B and T cell repertoire during human fetal development. Sci. Transl. Med. 2015, 7, 276ra25. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, M.J.; Dvorak, C.C.; Cowan, M.J.; Puck, J.M. Treatment of infants identified as having severe combined immunodeficiency by means of newborn screening. J. Allergy Clin. Immunol. 2017, 139, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Inborn Errors Working Party (IEWP). Available online: https://esid.org/layout/set/print/Working-Parties/Inborn-Errors-Working-Party-IEWP/Resources/UPDATED!-EBMT-ESID-GUIDELINES-FOR-HAEMATOPOIETIC-STEM-CELL-TRANSPLANTATION-FOR-PI (accessed on 25 September 2017).


{kind=link}
| Gestational Age (Weeks) | N | (%) | TREC Median [IQR] | p | KREC Median [IQR] | p |
| ≤28 | 58 | 0.7 | 42 [28–72] | <0.001 | 28 [16–44] | <0.001 |
| 29–31 | 105 | 1.2 | 54 [36–77] | <0.001 | 26 [16–44] | <0.001 |
| 32–36 | 801 | 9.1 | 74 [36–81] | <0.001 | 32 [1–56] | <0.001 |
| ≥37 | 6453 | 73.2 | 86 [57–129] | 1 | 40 [23–67] | 1 |
| Unknown | 1397 | 15.8 | 85 [56–126] | 0.2 | 40 [23–66] | 0.9 |
| Birth Weight (g) | N | (%) | TREC | p | KREC | |
| <1000 | 52 | 0.6 | 34 [18–55] | <0.001 | 25 [14–39] | <0.001 |
| 1000–1499 | 113 | 1.3 | 56 [28–87] | <0.001 | 25 [12–45] | <0.001 |
| 1500–2499 | 867 | 9.8 | 73 [46–113] | <0.001 | 31 [17–53] | <0.001 |
| ≥2500 | 6872 | 78.0 | 86 [57–129] | 1 | 40 [23–68] | 1 |
| Unknown | 910 | 10.3 | 87 [57–134] | 0.45 | 39 [23–70] | 0.8 |
| TOTAL (8814) | 8814 | 100 | 86 [56–129] | 40 [23–67] |
| Patient | GA/GENDER | 1st TREC (Copies/µL) | 1st KREC (Copies/µL) | 1st ACTB (Copies/µL) | 2nd TREC (Copies/µL) | 2nd KREC (Copies/µL) | 2nd ACTB (Copies/µL) | 1st LSS (Cells/µL) | 2nd LSS (Cells/µL) | Observations Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|
| P1 | 32/female | 1 | 4 | 1852 | NA | NA | NA | Total 500 CD3 + NA (%) CD19 + NA (%) | NA | Died age 1 month Trisomy, Monosomy (46,XX,der(7)t(7;15)(p22;q22)mat), Hydrops fetalis, Ebstein anomaly |
| P2 | 25/male | 0 | 0 | 4 | 4 | 8 | 7199 | Total 2184 CD3 + 1366 (63%) CD19 + 367 (17%) | NA | Extreme preterm Blood product dependent |
| P3 | 26/male | 1 | 20 | 356 | 0 | 27 | 2592 | Total 2424 CD3 + 1484 (60%) CD19 + 498 (20%) | Total 7493 CD3 + 2454 (35%) CD19 + 4500 (57%) | Extreme preterm Blood product dependent TOF IVIG dependent FU |
| P4 | Term/female | 92 | 1 | 2953 | NA | NA | NA | NA | NA | Azathioprine during pregnancy * |
| P5 | Term/male | 154 | 3 | 3589 | 61 | 1 | 863 | Total 1700 CD3 + NA (%) CD19 + NA (%) | NA | Azathioprine during pregnancy ** |
| Control | AGE at Time of DBS (Months) | Gender | TREC (Copies/µL) | KREC (Copies/µL) | ACTB (Copies/µL) | LSS (Cells/µL) 1st Available Sample | Diagnosis |
|---|---|---|---|---|---|---|---|
| C1 | 9.6 | Male | 0 | 56 | 705 | Total 611 CD3 + 30 (4.7%) CD19 + 428 (67.1%) | T-B+SCID (undefined) |
| C2 | 0.2 | Male | 0.5 | 0 | 1257 | Total 11800 CD3 + 9440 (80%) CD19 + (<1%) | T-B-SCID (RAG) |
| C3 | 0.2 | Female | 4 | 0 | 722 | Total 300 CD3 + 79 (45%) CD19 + 1 (2%) | T-B-SCID (ADA) |
| C4 | 0.2 | Male | 1.9 | 0.6 | 1182 | Total 1740 CD3 + 1087 (78%) CD19 + 1 (0.1%) | TlowB-SCID (Omenn) |
| C5 | 93 | Male | 23 | 0 | 3229 | Total 3400 CD3 + 2598 (76%) CD19 + 2 (0.05%) | XLA |
| C6 | 60 | Male | 42 | 0 | 1980 | Total 5594 CD3 + 5346 (92.9%) CD19 + 4 (0.1%) | XLA |
| C7 | 20 | Male | 0 | 7 | 805 | Total 1678 CD3 + 664 (42.9%) CD19 + 314 (20.2%) | Ataxia telangiectasia |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Felipe, B.; Olbrich, P.; Goycochea-Valdivia, W.; Delgado-Pecellin, C.; Sanchez-Moreno, P.; Sánchez, B.; Lucena, J.M.; Ferrari-Cortes, A.; De Soto, J.S.M.; Marquez, J.; et al. Newborn Screening for Primary T- and B-Cell Immune Deficiencies—A Prospective Study in Andalucía. Int. J. Neonatal Screen. 2017, 3, 27. https://doi.org/10.3390/ijns3040027
De Felipe B, Olbrich P, Goycochea-Valdivia W, Delgado-Pecellin C, Sanchez-Moreno P, Sánchez B, Lucena JM, Ferrari-Cortes A, De Soto JSM, Marquez J, et al. Newborn Screening for Primary T- and B-Cell Immune Deficiencies—A Prospective Study in Andalucía. International Journal of Neonatal Screening. 2017; 3(4):27. https://doi.org/10.3390/ijns3040027
Chicago/Turabian StyleDe Felipe, Beatriz, Peter Olbrich, Walter Goycochea-Valdivia, Carmen Delgado-Pecellin, Paula Sanchez-Moreno, Berta Sánchez, José Manuel Lucena, Araceli Ferrari-Cortes, Joséfa Salguero Martin De Soto, Josefina Marquez, and et al. 2017. "Newborn Screening for Primary T- and B-Cell Immune Deficiencies—A Prospective Study in Andalucía" International Journal of Neonatal Screening 3, no. 4: 27. https://doi.org/10.3390/ijns3040027
APA StyleDe Felipe, B., Olbrich, P., Goycochea-Valdivia, W., Delgado-Pecellin, C., Sanchez-Moreno, P., Sánchez, B., Lucena, J. M., Ferrari-Cortes, A., De Soto, J. S. M., Marquez, J., Salamanca, C., Jimenez Contreras, C., & Neth, O. (2017). Newborn Screening for Primary T- and B-Cell Immune Deficiencies—A Prospective Study in Andalucía. International Journal of Neonatal Screening, 3(4), 27. https://doi.org/10.3390/ijns3040027