
Influence of Season, Storage Temperature and Time of Sample Collection in Pancreatitis-Associated Protein-Based Algorithms for Newborn Screening for Cystic Fibrosis
 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
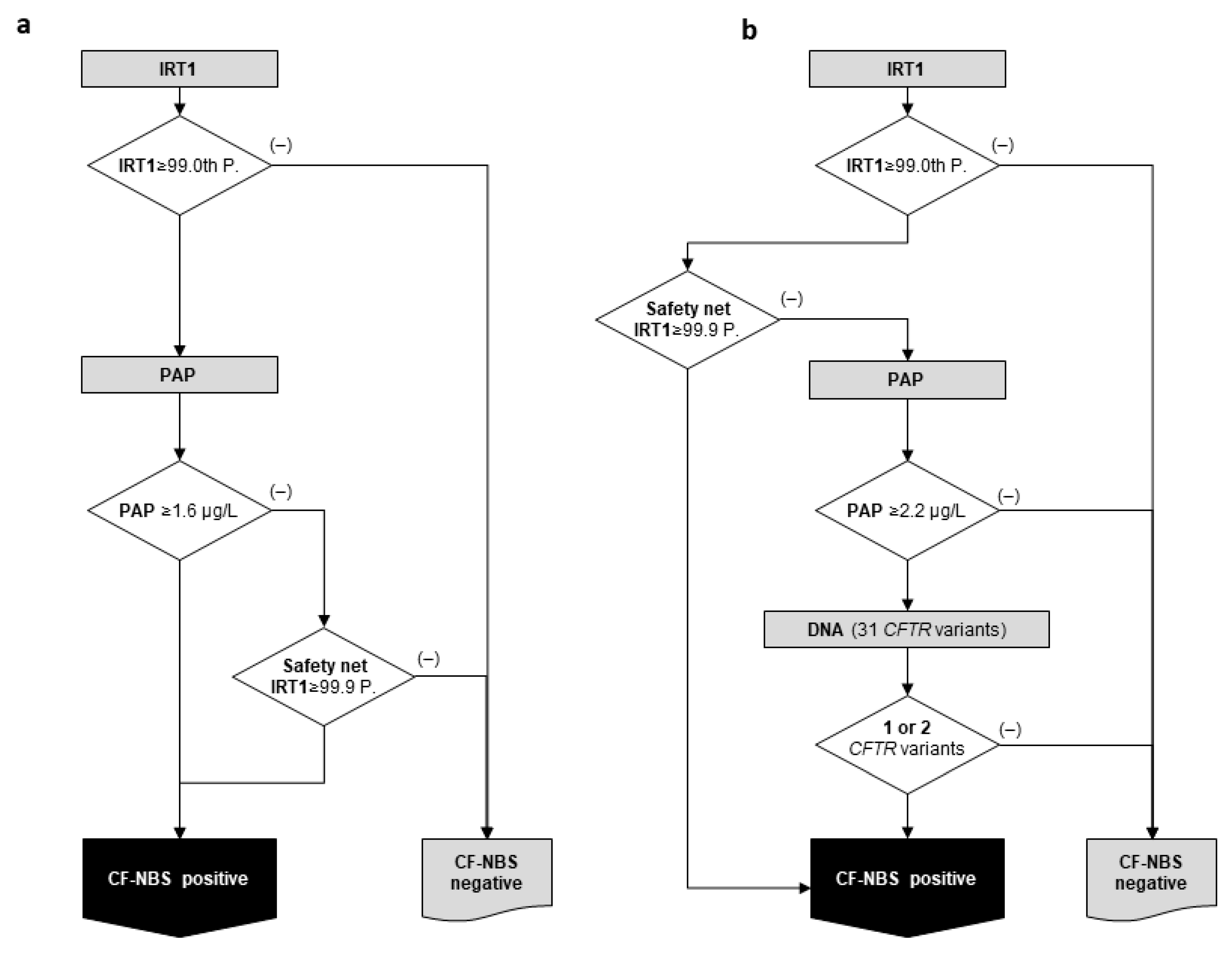
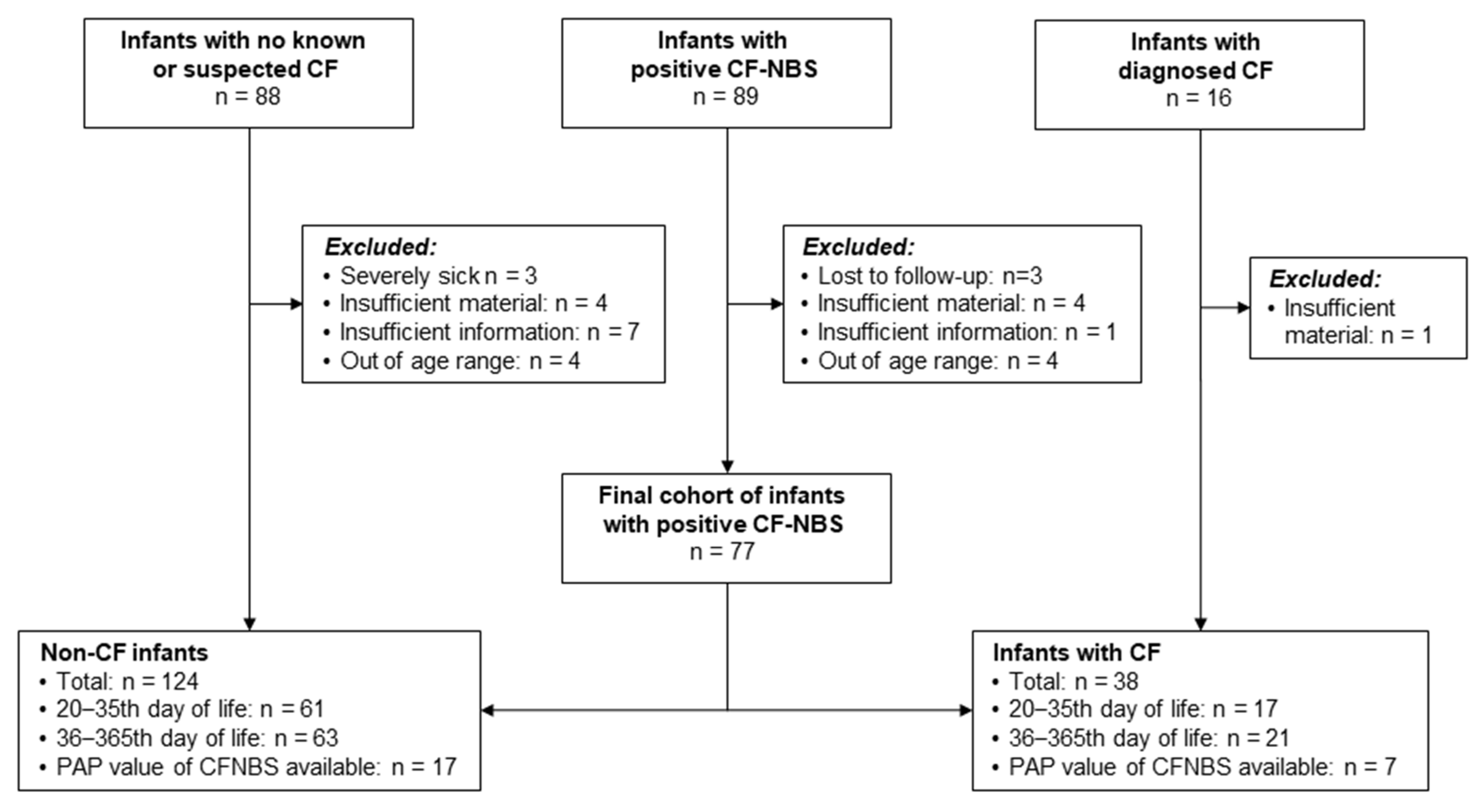
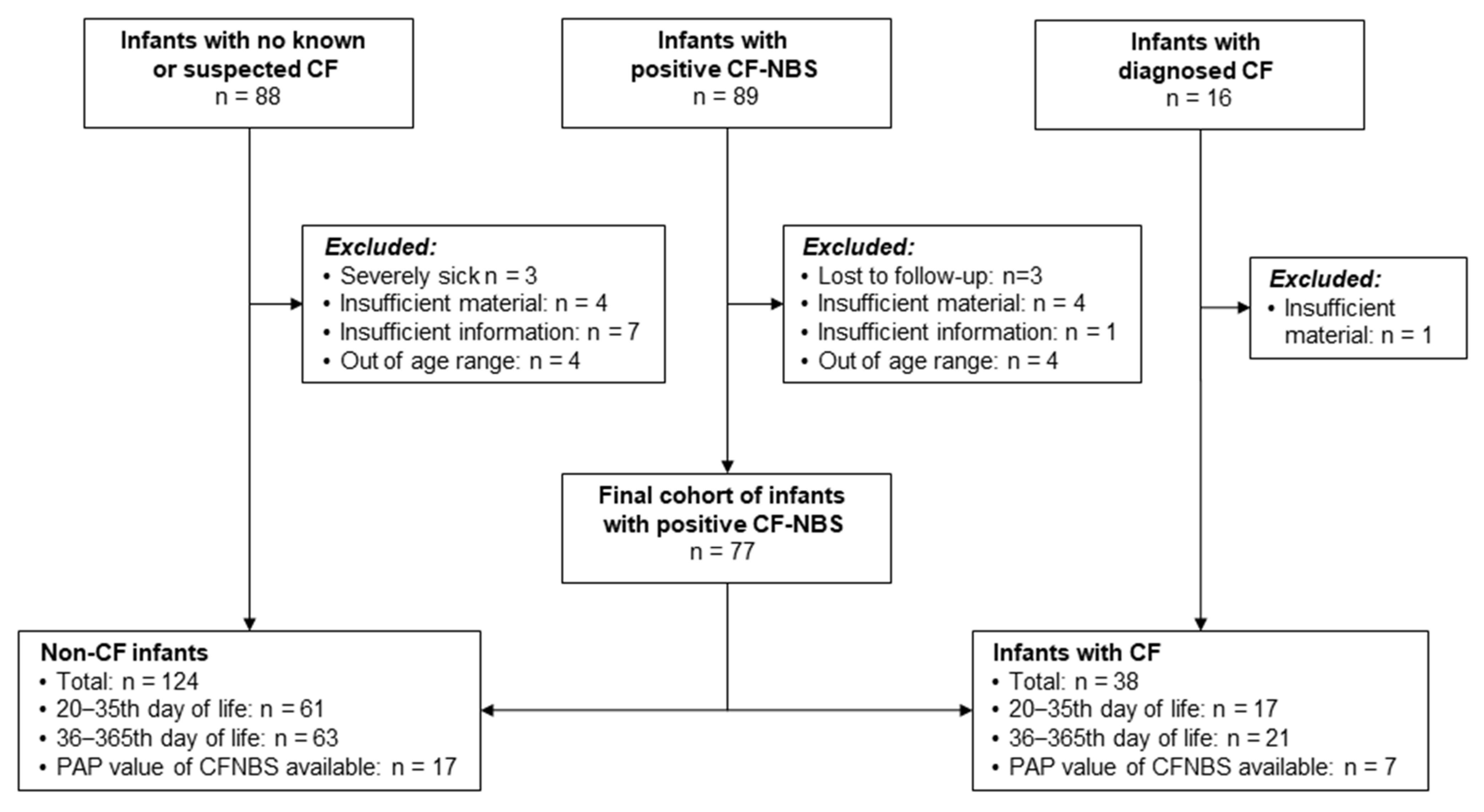
2.1. Study Population, Test Methods and CF-NBS Algorithms
2.2. Study Design
2.2.1. Evaluation of a Possible Seasonal Effect on IRT/PAP Determination
2.2.2. Storage Tests on Possible Temperature Effects on PAP Determination
2.2.3. Course of Blood PAP Concentrations in the First Days of Life
2.2.4. Course of Blood PAP Concentrations from 20th to the 365th Day of Life
3. Results
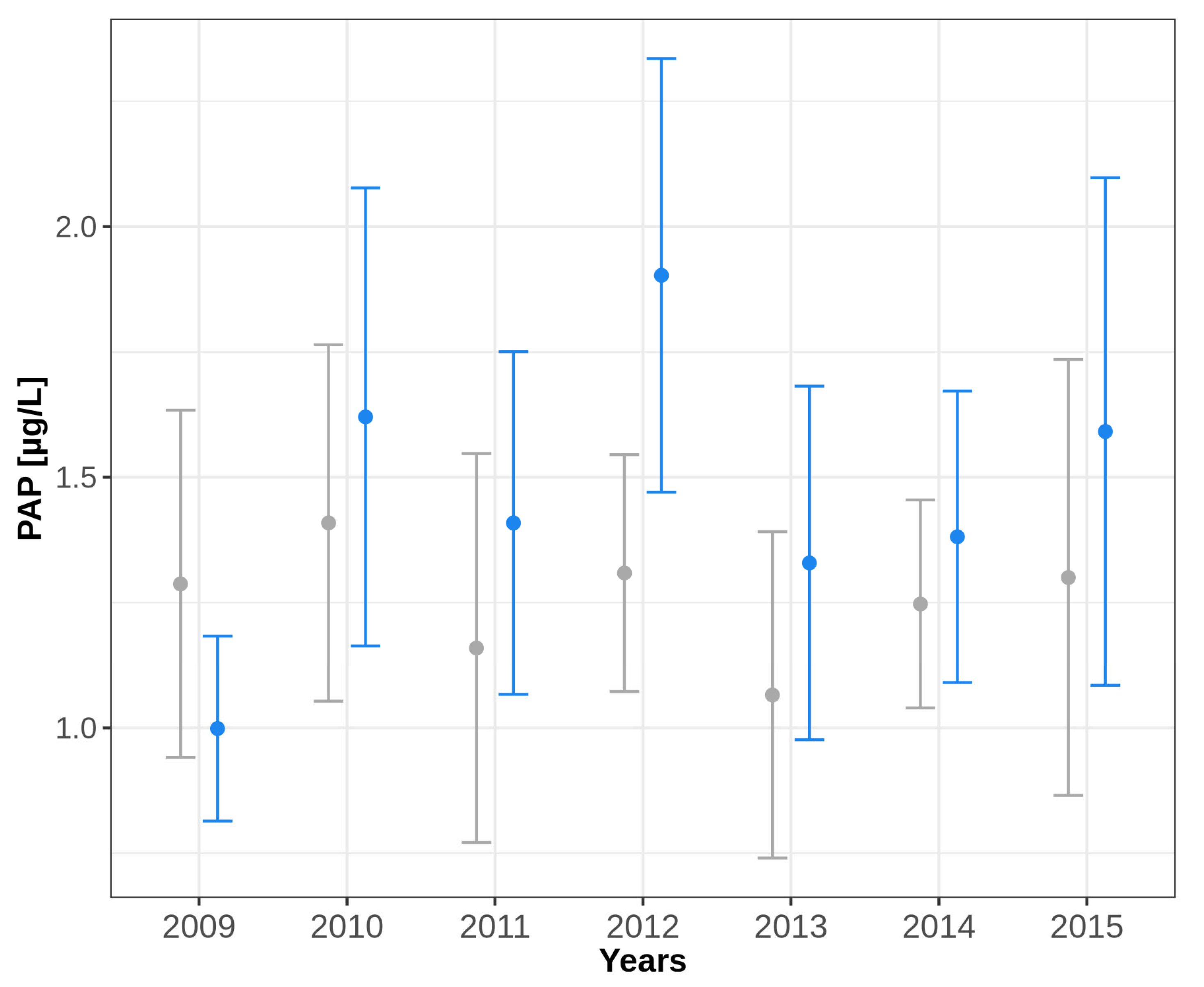
3.1. Evaluation of a Possible Seasonal Effect on IRT/PAP Determination
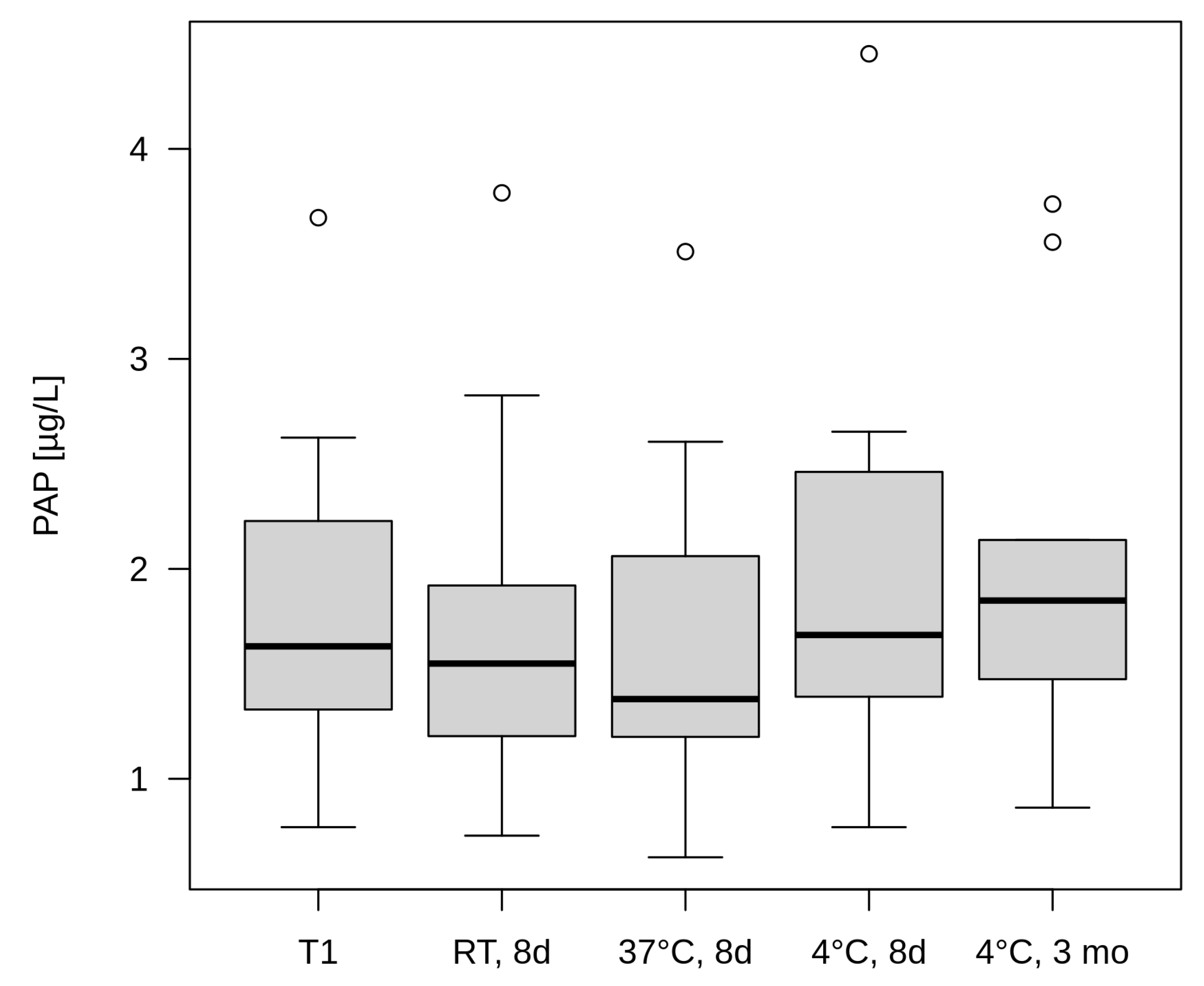
3.2. Direct Temperature Effect on PAP Determination
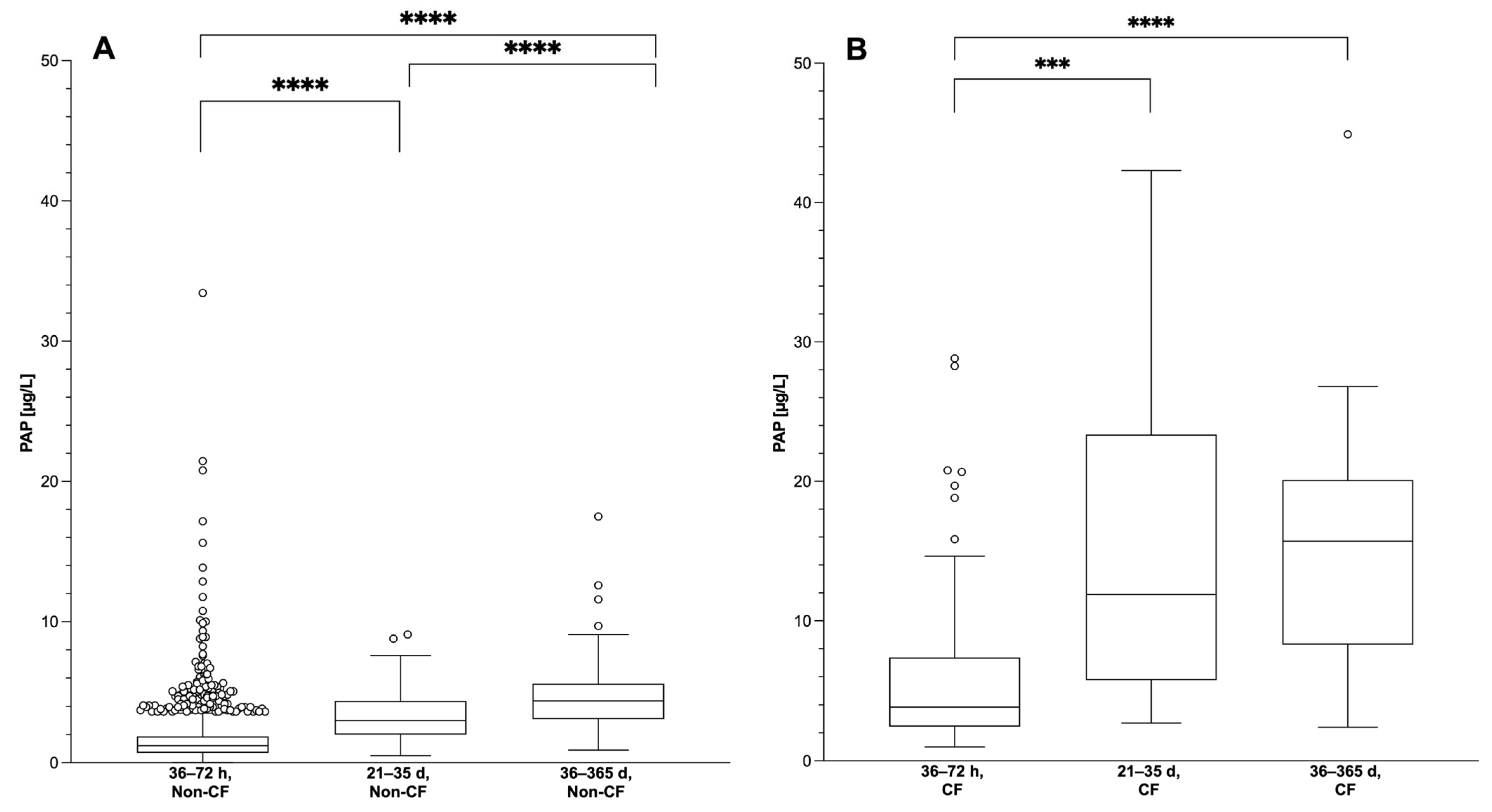
3.3. Course of Blood PAP Concentrations in the First Days of Life
3.4. Course of Blood PAP Concentrations in the First Year of Life
4. Discussion
4.1. Evaluation of Climate and Temperature Effects on the IRT/PAP Determination
4.2. Influence of Time of Sampling on PAP Value
4.3. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Mean IRT in Summer (µg/L) | Mean IRT in Winter (µg/L) | p-Value a |
|---|---|---|---|
| 2009 | 20.39 | 22.65 | <0.001 |
| 2010 | 21.61 | 22.43 | <0.001 |
| 2011 | 20.94 | 21.06 | 0.987 |
| 2012 | 21.12 | 21.97 | <0.001 |
| 2013 | 21.16 | 21.73 | <0.01 |
| Year | Summer | Winter | p-Value a | ||
|---|---|---|---|---|---|
| N | Mean PAP (µg/L) | N | Mean PAP (µg/L) | ||
| 2009 | 53 | 1.29 | 96 | 1.00 | 1.00 |
| 2010 | 70 | 1.41 | 119 | 1.62 | 1.00 |
| 2011 | 65 | 1.16 | 85 | 1.41 | 1.00 |
| 2012 | 77 | 1.31 | 79 | 1.90 | 0.31 |
| 2013 | 114 | 1.07 | 100 | 1.33 | 1.00 |
| 2014 | 110 | 1.25 | 122 | 1.38 | 1.00 |
| 2015 | 102 | 1.30 | 115 | 1.59 | 1.00 |
| Condition | N | Mean | 25th Percentile | 50th Percentile | 75th Percentile | Min | Max |
|---|---|---|---|---|---|---|---|
| PAP > 2.2 µg/L | |||||||
| T1 | 5 | 2.39 | 1.74 | 2.23 | 2.63 | 1.67 | 3.67 |
| RT, 8 d | 5 | 2.33 | 1.59 | 1.92 | 2.83 | 1.54 | 3.79 |
| 37 °C, 8 d | 5 | 2.21 | 1.60 | 2.06 | 2.61 | 1.28 | 3.51 |
| 4 °C, 8 d | 5 | 2.67 | 2.11 | 2.46 | 2.65 | 1.64 | 4.45 |
| 4 °C, 3 mo | 5 | 2.63 | 2.04 | 2.14 | 3.56 | 1.67 | 3.74 |
| PAP < 2.2 µg/L | |||||||
| T1 | 5 | 1.26 | 1.04 | 1.33 | 1.57 | 0.77 | 1.59 |
| RT, 8 d | 5 | 1.15 | 0.91 | 1.20 | 1.33 | 0.73 | 1.56 |
| 37 °C, 8 d | 5 | 1.08 | 0.80 | 1.20 | 1.29 | 0.63 | 1.47 |
| 4 °C, 8 d | 5 | 1.31 | 1.18 | 1.39 | 1.46 | 0.77 | 1.73 |
| 4 °C, 3 mo | 5 | 1.43 | 1.10 | 1.47 | 1.79 | 0.86 | 1.91 |
| T1 | 36 | 0.98 | 0.48 | 0.79 | 1.29 | 0.25 | 2.76 |
| RT, 2–3 mo | 36 | 0.90 | 0.47 | 0.73 | 1.04 | 0.25 | 2.53 |
| N | Median (µg/L) | Mann–Whitney p a | ||
|---|---|---|---|---|
| Non-CF | 36–72 h | 2301 | 1.21 | <0.0001 |
| Vs. 21–35 d | 61 | 3.00 | ||
| 36–72 h | 2301 | 1.21 | <0.0001 | |
| Vs. 36–365 d | 63 | 4.40 | ||
| 21–35 d | 61 | 3.00 | 0.0006 | |
| Vs. 36–365 d | 63 | 4.40 | ||
| CF | 36–72 h | 92 | 3.85 | 0.0001 |
| Vs. 21–35 d | 17 | 11.9 | ||
| 36–72 h | 92 | 3.85 | <0.0001 | |
| Vs. 36–365 d | 21 | 15.70 | ||
| 21–35 d | 17 | 11.90 | 0.6268 | |
| Vs. 36–365 d | 21 | 15.70 |
| Month/Year | Monthly Mean of Daily Average Temperature (°C) | Monthly Mean of Daily Maximum Temperature (°C) | Monthly Mean of Daily Minimum Temperature (°C) | Total Hours of Sunshine Per Month (Hours) | Rainfall Per Month(mm) |
|---|---|---|---|---|---|
| Jun 2009 | 17.2 | 22.2 | 11.9 | 217.8 | 86.6 |
| Jul 2009 | 19.8 | 25.1 | 14.8 | 223.0 | 98.4 |
| Aug 2009 | 20.9 | 27.2 | 14.5 | 262.7 | 20.5 |
| Dec 2009 | 2.1 | 4.7 | −0.9 | 35.0 | 74.1 |
| Jan 2010 | −1.7 | 0.3 | −3.9 | 26.6 | 43.0 |
| Feb 2010 | 1.7 | 4.5 | −1.0 | 33.8 | 50.0 |
| Jun 2010 | 18.8 | 24.4 | 12.5 | 299.4 | 61.4 |
| Jul 2010 | 22.2 | 28.3 | 15.8 | 293.8 | 61.4 |
| Aug 2010 | 18.3 | 23.0 | 13.7 | 160.6 | 101.3 |
| Dec 2010 | −1.6 | 0.3 | −3.9 | 22.3 | 72.5 |
| Jan 2011 | 2.6 | 5.0 | −0.4 | 42.0 | 37.2 |
| Feb 2011 | 3.0 | 6.1 | 0.0 | 69.8 | 23.1 |
| Jun 2011 | 18.5 | 23.4 | 13.8 | 189.9 | 82.8 |
| Jul 2011 | 17.8 | 22.8 | 13.1 | 166.9 | 59.9 |
| Aug 2011 | 19.5 | 25.1 | 14.3 | 208.3 | 79.7 |
| Dec 2011 | 5.1 | 7.7 | 2.2 | 28.2 | 107.4 |
| Jan 2012 | 3.7 | 6.4 | 0.8 | 63.1 | 57.8 |
| Feb 2012 | −8.1 | 3.1 | −4.8 | 124.0 | 6.8 |
| Jun 2012 | 17.3 | 22.3 | 12.6 | 174.3 | 104.0 |
| Jul 2012 | 19.4 | 24.5 | 14.3 | 212.7 | 66.0 |
| Aug 2012 | 20.8 | 26.5 | 14.9 | 247.0 | 78.5 |
| Dec 2012 | 3.8 | 6.0 | 1.3 | 26.7 | 71.0 |
| Jan 2013 | 1.8 | 3.6 | −0.5 | 19.2 | 33.1 |
| Feb 2013 | 1.1 | 3.2 | −1.1 | 27.7 | 33.5 |
| Jun 2013 | 17.8 | 22.8 | 12.4 | 220.6 | 78.2 |
| Jul 2013 | 22.3 | 27.9 | 16.3 | 301.1 | 17.8 |
| Aug 2013 | 19.9 | 26.0 | 14.1 | 221.4 | 47.9 |
| Dec 2013 | 4.6 | 7.5 | 1.4 | 59.4 | 21.9 |
| Jan 2014 | 4.7 | 7.3 | 1.8 | 54.5 | 38.8 |
| Feb 2014 | 5.7 | 9.5 | 1.8 | 59.1 | 45.6 |
| Jun 2014 | 18.6 | 24.3 | 12.4 | 253.0 | 36.5 |
| Jul 2014 | 21.2 | 26.6 | 16.1 | 242.2 | 128.7 |
| Aug 2014 | 17.5 | 22.4 | 13.0 | 175.2 | 101.6 |
| Dec 2014 | 3.9 | 6.0 | 1.2 | 18.6 | 56.2 |
| Jan 2015 | 3.1 | 5.6 | 0.2 | 29.6 | 62.8 |
| Feb 2015 | 2.2 | 5.2 | −0.8 | 69.3 | 20.9 |
| Jun 2015 | 18.1 | 23.5 | 12.4 | 214.4 | 57.5 |
| Jul 2015 | 22.3 | 28.6 | 15.9 | 263.5 | 26.1 |
| Aug 2015 | 21.8 | 28.1 | 16.0 | 234.8 | 43.3 |
| Dec 2015 | 7.2 | 10.1 | 3.5 | 53.5 | 28.1 |
| Jan 2016 | 3.3 | 6.0 | 0.4 | 42.2 | 66.8 |
| Feb 2016 | 4.5 | 7.9 | 1.7 | 46.5 | 81.9 |
References
- Munck, A.; Dhondt, J.L.; Sahler, C.; Roussey, M. Implementation of the French nationwide cystic fibrosis newborn screening program. J. Pediatr. 2008, 153, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Gemeinsamer-Bundesausschuss. Kinder-Richtlinie: Änderung des Beschlusses zur Neufassung—Screening auf Mukoviszidose (Zystische Fibrose)—Tragende Gründe zum Beschluss. Available online: https://www.g-ba.de/informationen/beschluesse/2316/ (accessed on 27 October 2023).
- Sarles, J.; Berthezene, P.; Le, L.C.; Somma, C.; Perini, J.M.; Catheline, M.; Mirallie, S.; Luzet, K.; Roussey, M.; Farriaux, J.P.; et al. Combining immunoreactive trypsinogen and pancreatitis-associated protein assays, a method of newborn screening for cystic fibrosis that avoids DNA analysis. J. Pediatr. 2005, 147, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Sarles, J.; Barthellemy, S.; Ferec, C.; Iovanna, J.; Roussey, M.; Farriaux, J.P.; Toutain, A.; Berthelot, J.; Maurin, N.; Codet, J.P.; et al. Blood concentrations of pancreatitis associated protein in neonates: Relevance to neonatal screening for cystic fibrosis. Arch. Dis. Child. Fetal Neonatal Ed. 1999, 80, F118–F122. [Google Scholar] [CrossRef] [PubMed]
- Sommerburg, O.; Lindner, M.; Muckenthaler, M.; Kohlmueller, D.; Leible, S.; Feneberg, R.; Kulozik, A.E.; Mall, M.A.; Hoffmann, G.F. Initial evaluation of a biochemical cystic fibrosis newborn screening by sequential analysis of immunoreactive trypsinogen and pancreatitis-associated protein (IRT/PAP) as a strategy that does not involve DNA testing in a Northern European population. J. Inherit. Metab. Dis. 2010, 33, S263–S271. [Google Scholar] [CrossRef] [PubMed]
- Vernooij-van Langen, A.M.; Loeber, J.G.; Elvers, B.; Triepels, R.H.; Gille, J.J.; Van der Ploeg, C.P.; Reijntjens, S.; Dompeling, E.; Dankert-Roelse, J.E.; Group, C.S. Novel strategies in newborn screening for cystic fibrosis: A prospective controlled study. Thorax 2012, 67, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Dankert-Roelse, J.E.; Bouva, M.J.; Jakobs, B.S.; Janssens, H.M.; de Winter-de Groot, K.M.; Schonbeck, Y.; Gille, J.J.P.; Gulmans, V.A.M.; Verschoof-Puite, R.K.; Schielen, P.; et al. Newborn blood spot screening for cystic fibrosis with a four-step screening strategy in the Netherlands. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2019, 18, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Marcão, A.; Barreto, C.; Pereira, L.; Vaz, L.G.; Cavaco, J.; Casimiro, A.; Félix, M.; Silva, T.R.; Barbosa, T.; Freitas, C.; et al. Cystic Fibrosis Newborn Screening in Portugal: PAP Value in Populations with Stringent Rules for Genetic Studies. Int. J. Neon. Screen. 2018, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Zeyda, M.; Schanzer, A.; Basek, P.; Bauer, V.; Eber, E.; Ellemunter, H.; Kallinger, M.; Riedler, J.; Thir, C.; Wadlegger, F.; et al. Cystic Fibrosis Newborn Screening in Austria Using PAP and the Numeric Product of PAP and IRT Concentrations as Second-Tier Parameters. Diagnostics 2021, 11, 299. [Google Scholar] [CrossRef] [PubMed]
- Vernooij-van Langen, A.M.; Loeber, J.G.; Elvers, B.; Triepels, R.H.; Roefs, J.; Gille, J.J.; Reijntjens, S.; Dompeling, E.; Dankert-Roelse, J.E. The influence of sex, gestational age, birth weight, blood transfusion, and timing of the heel prick on the pancreatitis-associated protein concentration in newborn screening for cystic fibrosis. J. Inherit. Metab. Dis. 2013, 36, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Weidler, S.; Stopsack, K.H.; Hammermann, J.; Sommerburg, O.; Mall, M.A.; Hoffmann, G.F.; Kohlmuller, D.; Okun, J.G.; Macek, M., Jr.; Votava, F.; et al. A product of immunoreactive trypsinogen and pancreatitis-associated protein as second-tier strategy in cystic fibrosis newborn screening. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2016, 15, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Bowling, F.G.; Brown, A.R. Newborn screening for cystic fibrosis using an enzyme linked immunoabsorbent assay (ELISA) technique. Clin. Chim. Acta 1988, 171, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Sarles, J.; Giorgi, R.; Berthezene, P.; Munck, A.; Cheillan, D.; Dagorn, J.C.; Roussey, M. Neonatal screening for cystic fibrosis: Comparing the performances of IRT/DNA and IRT/PAP. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2014, 13, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Sommerburg, O.; Hammermann, J.; Lindner, M.; Stahl, M.; Muckenthaler, M.; Kohlmueller, D.; Happich, M.; Kulozik, A.E.; Stopsack, M.; Gahr, M.; et al. Five years of experience with biochemical cystic fibrosis newborn screening based on IRT/PAP in Germany. Pediatr. Pulmonol. 2015, 50, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Sommerburg, O.; Krulisova, V.; Hammermann, J.; Lindner, M.; Stahl, M.; Muckenthaler, M.; Kohlmueller, D.; Happich, M.; Kulozik, A.E.; Votava, F.; et al. Comparison of different IRT-PAP protocols to screen newborns for cystic fibrosis in three central European populations. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2014, 13, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Wobbrock, J.O.; Findlater, L.; Gergle, D.; Higgins, J.J. The Aligned Rank Transform for Nonparametric Factorial Analyses Using Only ANOVA Procedures. In CHI 2011: Proceedings of the SIGCHI Conference on Human Factors in Computing Systems; Association for Computing Machinery: New York, NY, USA, 2011; pp. 143–146. [Google Scholar] [CrossRef]
- Kloosterboer, M.; Hoffman, G.; Rock, M.; Gershan, W.; Laxova, A.; Li, Z.; Farrell, P.M. Clarification of laboratory and clinical variables that influence cystic fibrosis newborn screening with initial analysis of immunoreactive trypsinogen. Pediatrics 2009, 123, e338–e346. [Google Scholar] [CrossRef] [PubMed]
- Krulisova, V.; Balascakova, M.; Skalicka, V.; Piskackova, T.; Holubova, A.; Paderova, J.; Krenkova, P.; Dvorakova, L.; Zemkova, D.; Kracmar, P.; et al. Prospective and parallel assessments of cystic fibrosis newborn screening protocols in the Czech Republic: IRT/DNA/IRT versus IRT/PAP and IRT/PAP/DNA. Eur. J. Pediatr. 2012, 171, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Sommerburg, O.; Stahl, M.; Hammerling, S.; Gramer, G.; Muckenthaler, M.U.; Okun, J.; Kohlmuller, D.; Happich, M.; Kulozik, A.E.; Mall, M.A.; et al. Final results of the southwest German pilot study on cystic fibrosis newborn screening—Evaluation of an IRT/PAP protocol with IRT-dependent safety net. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2022, 21, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Sontag, M.K.; Lee, R.; Wright, D.; Freedenberg, D.; Sagel, S.D. Improving the Sensitivity and Positive Predictive Value in a Cystic Fibrosis Newborn Screening Program Using a Repeat Immunoreactive Trypsinogen and Genetic Analysis. J. Pediatr. 2016, 175, 150–158.e1. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://opendata.dwd.de/climate_environment/CDC/observations_germany/climate/daily/kl/historical/ (accessed on 14 December 2023).


| Year | Percentile | IRT in Summer (µg/L) | IRT in Winter (µg/L) | p-Value |
|---|---|---|---|---|
| 2009 | 95.0 | 42 | 46 | <0.001 |
| 99.0 | 63 | 70 | <0.001 | |
| 99.9 | 131 | 146 | 0.584 | |
| 2010 | 95.0 | 44 | 46 | <0.001 |
| 99.0 | 63 | 75 | <0.001 | |
| 99.9 | 136 | 186 | 0.124 | |
| 2011 | 95.0 | 43 | 44 | <0.05 |
| 99.0 | 61 | 67 | <0.05 | |
| 99.9 | 131 | 124 | 0.752 | |
| 2012 | 95.0 | 44 | 45 | 0.272 |
| 99.0 | 67 | 67 | 0.840 | |
| 99.9 | 173 | 142 | 0.164 | |
| 2013 | 95.0 | 44 | 44 | 0.924 |
| 99.0 | 64 | 65 | 0.588 | |
| 99.9 | 141 | 149 | 0.560 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maier, P.; Jeyaweerasinkam, S.; Eberhard, J.; Soueidan, L.; Hämmerling, S.; Kohlmüller, D.; Feyh, P.; Gramer, G.; Garbade, S.F.; Hoffmann, G.F.; et al. Influence of Season, Storage Temperature and Time of Sample Collection in Pancreatitis-Associated Protein-Based Algorithms for Newborn Screening for Cystic Fibrosis. Int. J. Neonatal Screen. 2024, 10, 5. https://doi.org/10.3390/ijns10010005
Maier P, Jeyaweerasinkam S, Eberhard J, Soueidan L, Hämmerling S, Kohlmüller D, Feyh P, Gramer G, Garbade SF, Hoffmann GF, et al. Influence of Season, Storage Temperature and Time of Sample Collection in Pancreatitis-Associated Protein-Based Algorithms for Newborn Screening for Cystic Fibrosis. International Journal of Neonatal Screening. 2024; 10(1):5. https://doi.org/10.3390/ijns10010005
Chicago/Turabian StyleMaier, Pia, Sumathy Jeyaweerasinkam, Janina Eberhard, Lina Soueidan, Susanne Hämmerling, Dirk Kohlmüller, Patrik Feyh, Gwendolyn Gramer, Sven F. Garbade, Georg F. Hoffmann, and et al. 2024. "Influence of Season, Storage Temperature and Time of Sample Collection in Pancreatitis-Associated Protein-Based Algorithms for Newborn Screening for Cystic Fibrosis" International Journal of Neonatal Screening 10, no. 1: 5. https://doi.org/10.3390/ijns10010005
APA StyleMaier, P., Jeyaweerasinkam, S., Eberhard, J., Soueidan, L., Hämmerling, S., Kohlmüller, D., Feyh, P., Gramer, G., Garbade, S. F., Hoffmann, G. F., Okun, J. G., & Sommerburg, O. (2024). Influence of Season, Storage Temperature and Time of Sample Collection in Pancreatitis-Associated Protein-Based Algorithms for Newborn Screening for Cystic Fibrosis. International Journal of Neonatal Screening, 10(1), 5. https://doi.org/10.3390/ijns10010005