Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mak, C.M.; Lee, H.C.; Chan, A.Y.; Lam, C.W. Inborn errors of metabolism and expanded newborn screening: Review and update. Crit. Rev. Clin. Lab. Sci. 2013, 50, 142–162. [Google Scholar] [CrossRef]
- Gurian, E.A.; Kinnamon, D.D.; Henry, J.J.; Waisbren, S.E. Expanded newborn screening for biochemical disorders: The effect of a false-positive result. Pediatrics 2006, 117, 1915–1921. [Google Scholar] [CrossRef]
- Yamada, K.; Osawa, Y.; Kobayashi, H.; Hasegawa, Y.; Fukuda, S.; Yamaguchi, S.; Taketani, T. Serum C14:1/C12:1 ratio is a useful marker for differentiating affected patients with very long-chain acyl-CoA dehydrogenase deficiency from heterozygous carriers. Mol. Genet. Metab. Rep. 2019, 21, 100535. [Google Scholar] [CrossRef] [PubMed]
- Gavrilov, D.K.; Piazza, A.L.; Pino, G.; Turgeon, C.; Matern, D.; Oglesbee, D.; Raymond, K.; Tortorelli, S.; Rinaldo, P. The Combined Impact of CLIR Post-Analytical Tools and Second Tier Testing on the Performance of Newborn Screening for Disorders of Propionate, Methionine, and Cobalamin Metabolism. Int. J. Neonatal Screen. 2020, 6, 33. [Google Scholar] [CrossRef]
- Yeung, M.C.W.; Chan, T.C.H.; Mak, C.M. Clinical Utility of Second-tier Testing in Newborn Screening for Congenital Adrenal Hyperplasia: The Hong Kong Experience. HK J. Paediatr. New Ser. 2020, 25, 3–7. [Google Scholar]
- Chen, H.A.; Hsu, R.H.; Chang, K.L.; Huang, Y.C.; Chiang, Y.C.; Lee, N.C.; Hwu, W.L.; Chiu, P.C.; Chien, Y.H. Asymptomatic ASS1 carriers with high blood citrulline levels. Mol. Genet. Genom. Med. 2022, 10, e2007. [Google Scholar] [CrossRef]
- Siri, B.; Olivieri, G.; Angeloni, A.; Cairoli, S.; Carducci, C.; Cotugno, G.; Di Michele, S.; Giovanniello, T.; La Marca, G.; Lepri, F.R.; et al. The diagnostic challenge of mild citrulline elevation at newborn screening. Mol. Genet. Metab. 2022, 135, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Spiekerkoetter, U.; Bick, D.; Scott, R.; Hopkins, H.; Krones, T.; Gross, E.S.; Bonham, J.R. Genomic newborn screening: Are we entering a new era of screening? J. Inherit. Metab. Dis. 2023, 46, 778–795. [Google Scholar] [CrossRef]
- Ferlini, A.; Gross, E.S.; Garnier, N.; on behalf of the Screen4Care consortium. Rare diseases’ genetic newborn screening as the gateway to future genomic medicine: The Screen4Care EU-IMI project. Orphanet J. Rare Dis. 2023, 18, 310. [Google Scholar] [CrossRef]
- Holm, I.A.; Agrawal, P.B.; Ceyhan-Birsoy, O.; Christensen, K.D.; Fayer, S.; Frankel, L.A.; Genetti, C.A.; Krier, J.B.; LaMay, R.C.; Levy, H.L.; et al. The BabySeq project: Implementing genomic sequencing in newborns. BMC Pediatr. 2018, 18, 225. [Google Scholar] [CrossRef]
- Ji, C.; Farrar, M.A.; Norris, S.; Bhattacharya, K.; Bennetts, B.; Newson, A.J.; Healy, L.; Millis, N.; Kariyawasam, D.S. The Australian landscape of newborn screening in the genomics. Rare Dis. Orphan Drugs J. 2023, 2, 26. [Google Scholar] [CrossRef]
- Tsang, K.; Chan, T.; Yeung, M.; Wong, T.; Lau, W.; Mak, C. Validation of amplicon-based next generation sequencing panel for second-tier test in newborn screening for inborn errors of metabolism. J. Lab. Med. 2021, 45, 267–274. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Lin, Y.; Liu, Y.; Zhu, L.; Le, K.; Shen, Y.; Yang, C.; Chen, X.; Hu, H.; Ma, Q.; Shi, X.; et al. Combining newborn metabolic and genetic screening for neonatal intrahepatic cholestasis caused by citrin deficiency. J. Inherit. Metab. Dis. 2020, 43, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Turgeon, C.T.; Magera, M.J.; Cuthbert, C.D.; Loken, P.R.; Gavrilov, D.K.; Tortorelli, S.; Raymond, K.M.; Oglesbee, D.; Rinaldo, P.; Matern, D. Determination of total homocysteine, methylmalonic acid, and 2-methylcitric acid in dried blood spots by tandem mass spectrometry. Clin. Chem. 2010, 56, 1686–1695. [Google Scholar] [CrossRef] [PubMed]
- Currier, R.J.; Sciortino, S.; Liu, R.; Bishop, T.; Alikhani Koupaei, R.; Feuchtbaum, L. Genomic sequencing in cystic fibrosis newborn screening: What works best, two-tier predefined CFTR mutation panels or second-tier CFTR panel followed by third-tier sequencing? Genet. Med. 2017, 19, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.H.; Gong, J.Y.; Wang, J.S. Citrin deficiency presenting as acute liver failure in an eight-month-old infant. World J. Gastroenterol. 2015, 21, 7331–7334. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Zhu, S.; Miao, H.; Yang, J.; Shi, Y.; Yue, Y.; Zhang, Y.; Yang, R.; Wu, B.; Huang, X. Dynamic changes of metabolic characteristics in neonatal intrahepatic cholestasis caused by citrin deficiency. Front. Mol. Biosci. 2022, 9, 939837. [Google Scholar] [CrossRef] [PubMed]
- Shigetomi, H.; Tanaka, T.; Nagao, M.; Tsutsumi, H. Early Detection and Diagnosis of Neonatal Intrahepatic Cholestasis Caused by Citrin Deficiency Missed by Newborn Screening Using Tandem Mass Spectrometry. Int. J. Neonatal Screen. 2018, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Lund, A.M.; Wibrand, F.; Skogstrand, K.; Bækvad-Hansen, M.; Gregersen, N.; Andresen, B.S.; Hougaard, D.M.; Dunø, M.; Olsen, R.K.J. Use of Molecular Genetic Analyses in Danish Routine Newborn Screening. Int. J. Neonatal Screen. 2021, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.T.; Hsiao, K.J.; Chen, C.Y.; Wu, C.C.; Lin, S.J.; Chou, Y.Y.; Shiesh, S.C. High resolution melting analysis for the detection of SLC25A13 gene mutations in Taiwan. Clin. Chim. Acta 2011, 412, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.W.; Atkins, A.E.; Cordovado, S.K.; Hendrix, M.; Earley, M.C.; Farrell, P.M. Improving newborn screening for cystic fibrosis using next-generation sequencing technology: A technical feasibility study. Genet. Med. 2016, 18, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Sicko, R.J.; Stevens, C.F.; Hughes, E.E.; Leisner, M.; Ling, H.; Saavedra-Matiz, C.A.; Caggana, M.; Kay, D.M. Validation of a Custom Next-Generation Sequencing Assay for Cystic Fibrosis Newborn Screening. Int. J. Neonatal Screen. 2021, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.L.; Qian, G.L.; Wu, D.W.; Miao, J.K.; Yang, X.; Wu, B.Q.; Yan, Y.Q.; Li, H.B.; Mao, X.M.; He, J.; et al. A multicenter prospective study of next-generation sequencing-based newborn screening for monogenic genetic diseases in China. World J. Pediatr. 2023, 19, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Ceyhan-Birsoy, O.; Murry, J.B.; Machini, K.; Lebo, M.S.; Timothy, W.Y.; Fayer, S.; Genetti, C.A.; Schwartz, T.S.; Agrawal, P.B.; Parad, R.B.; et al. Interpretation of Genomic Sequencing Results in Healthy and Ill Newborns: Results from the BabySeq Project. Am. J. Hum. Genet. 2019, 104, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Fan, C.; Huang, Y.; Feng, J.; Zhang, Y.; Miao, J.; Wang, X.; Li, Y.; Huang, C.; Jin, W.; et al. Genomic Sequencing as a First-Tier Screening Test and Outcomes of Newborn Screening. JAMA Netw. Open 2023, 6, e2331162. [Google Scholar] [CrossRef]
- Kingsmore, S.F.; Smith, L.D.; Kunard, C.M.; Bainbridge, M.; Batalov, S.; Benson, W.; Blincow, E.; Caylor, S.; Chambers, C.; Del Angel, G.; et al. A genome sequencing system for universal newborn screening, diagnosis, and precision medicine for severe genetic diseases. Am. J. Hum. Genet. 2022, 109, 1605–1619. [Google Scholar] [CrossRef]
- Wojcik, M.H.; Zhang, T.; Ceyhan-Birsoy, O.; Genetti, C.A.; Lebo, M.S.; Yu, T.W.; Parad, R.B.; Holm, I.A.; Rehm, H.L.; Beggs, A.H.; et al. Discordant results between conventional newborn screening and genomic sequencing in the BabySeq Project. Genet. Med. 2021, 23, 1372–1375. [Google Scholar] [CrossRef]
- Kilgore, M.B.; Platis, D.; Lim, T.; Isenberg, S.; Pickens, C.A.; Cuthbert, C.; Petritis, K. Development of a Universal Second-Tier Newborn Screening LC-MS/MS Method for Amino Acids, Lysophosphatidylcholines, and Organic Acids. Anal. Chem. 2023, 95, 3187–3194. [Google Scholar] [CrossRef]
- Mak, J.; Peng, G.; Le, A.; Gandotra, N.; Enns, G.M.; Scharfe, C.; Cowan, T.M. Validation of a targeted metabolomics panel for improved second-tier newborn screening. J. Inherit. Metab. Dis. 2023, 46, 194–205. [Google Scholar] [CrossRef]
- Stenton, S.L.; Campagna, M.; Philippakis, A.; O’Donnell-Luria, A.; Gelb, M.H. First-tier next-generation sequencing for newborn screening: An important role for biochemical second-tier testing. Genet. Med. Open 2023, 1, 100821. [Google Scholar] [CrossRef]
- Peng, G.; Shen, P.; Gandotra, N.; Le, A.; Fung, E.; Jelliffe-Pawlowski, L.; Davis, R.W.; Enns, G.M.; Zhao, H.; Cowan, T.M.; et al. Combining newborn metabolic and DNA analysis for second-tier testing of methylmalonic acidemia. Genet. Med. 2019, 21, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, Y.Y.; Hong, D.Y.; Zhang, Z.L.; Li, Y.H.; Yang, P.Y.; Sun, Y.; Jiang, T.; Xu, Z.F. Combined genetic screening and traditional biochemical screening to optimize newborn screening systems. Clin. Chim. Acta 2022, 528, 44–51. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
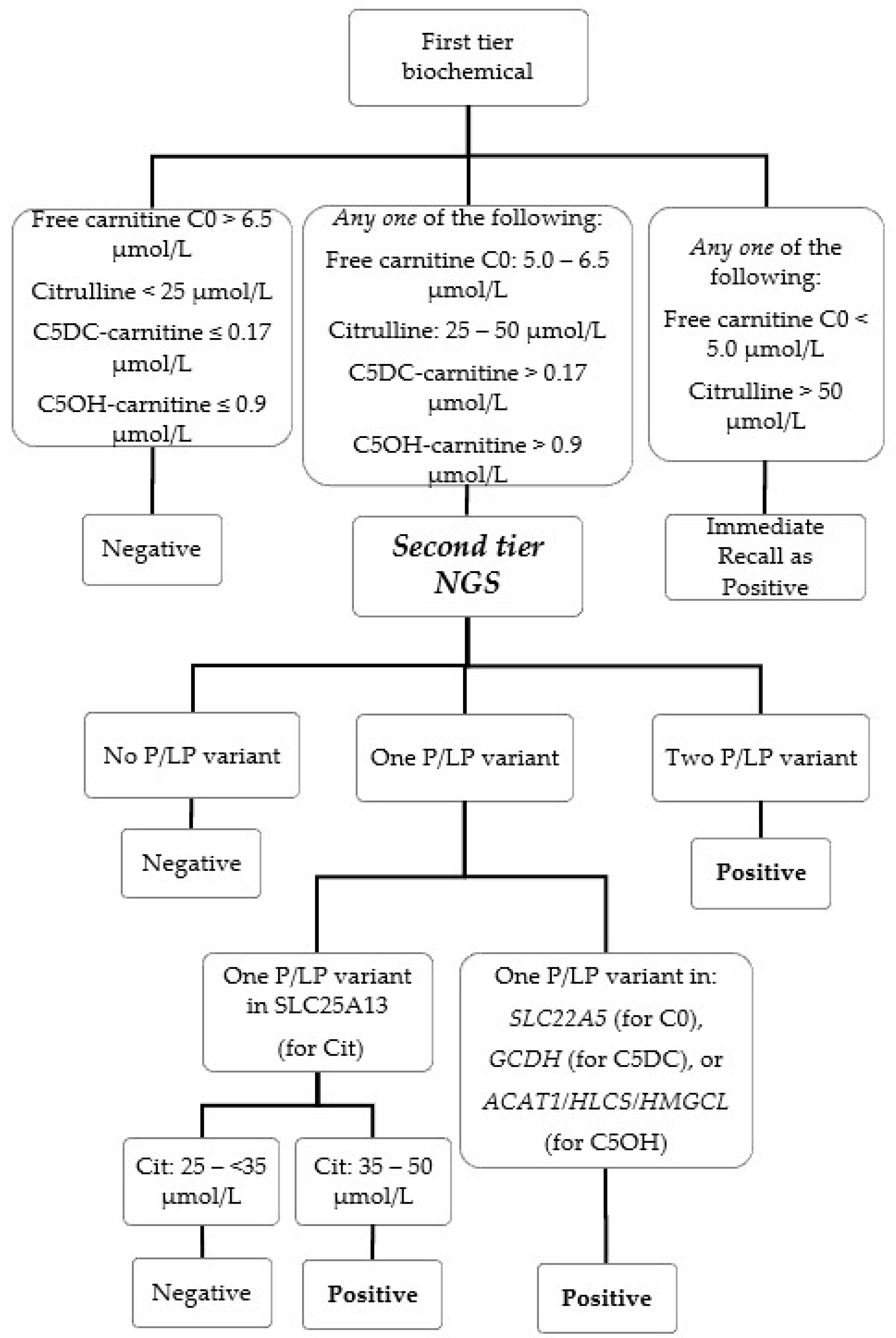
| First-Tier Biochemical | Second-Tier Genetic | Target Condition | Historical Biochemical Cutoff for Recall without 2nd Tier (μmol/L) | ||
|---|---|---|---|---|---|
| Biochemical Marker | Cutoff (μmol/L) | Genotyping Marker | Cutoff | ||
| Free carnitine-C0 | 5.0–6.5 n/c * | Sequence variant in SLC22A5 gene | ≥one P/LP variant | Carnitine uptake defect (CUD, MIM #212140, also known as systemic primary carnitine deficiency) | ≤6.2 c |
| Citrulline | 25–50 n/c ^ | Sequence variant and target screening for IVS16ins3kb in SLC25A13 gene $ | 1. ≥one P/LP variant and citrulline ≥ 35 μmol/L, or 2. ≥two P/LP variant and citrulline ≥25 and <35 μmol/L @ | Citrin deficiency (CD, MIM #605814, also known as citrullinemia type II) | ≥35 c |
| C5DC-carnitine | >0.17 n >0.35 c | Sequence variant in GCDH gene | ≥one P/LP variant | Glutaric acidemia type I (MIM #231670) | ≥0.35 c |
| C5OH-carnitine | >0.9 n >0.7 c | Sequence variant in ACAT1, HLCS and HMGCL gene | ≥one P/LP variant | Beta-ketothiolase deficiency (#203750) Holocarboxylase synthetase deficiency (MIM #253270) 3-Hydroxy-3-methylglutaryl-CoA lyase deficiency (MIM #246450). | ≥0.78 c |
| Case Number | Newborn Screening Result | Confirmatory Genetic Test Result | Clinical Summary | |
|---|---|---|---|---|
| First-Tier Biochemical | Second-Tier Genetic | |||
| Cit-1 (TP) | Citrulline: 27 μmol/L | Homozygous for the pathogenic variant: c.852_855del in SLC25A13 gene | Genetically confirmed as CD, both parents were heterozygote carrier. | 21 months old during latest clinic visit with satisfactory growth and development, on lactose-free formula, uneventful clinical course. |
| Cit-2 (TP) | Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.1311+1G>A, and Target screening positive for heterozygous IVS16ins3kb variant, in SLC25A13 gene | Genetically confirmed as CD, both parents were heterozygote carrier. | 19 months old during latest visit, now with satisfactory growth and development, on lactose-free MCT-enriched formula. Initially screened negative with sequence analysis alone. Presented with conjugated hyperbilirubinemia and failure to thrive at 2 months while on breastfeeding, with no definitive diagnosis despite extensive investigation performed including plasma amino acids and liver biopsy. Jaundice resolved spontaneously at 3 months. Recalled and eventually diagnosed as citrin deficiency at 13 months of age after implementation of target screening for IVS16ins3kb variant. Catch-up growth with appropriate dietary management. |
| Cit-3 (FP) | Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.615+5G>A | Genetically confirmed as CD carrier. | Case closed at 7 months old during latest clinic visit after extensive biochemical and genetic investigations, normal growth and development. |
| Cit-4 (FP) | Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.615 + 5G>A | Genetically confirmed as CD carrier. | Case closed at 7 months old during latest clinic visit after extensive biochemical and genetic investigations, normal growth and development. |
| C0-1 (TP) | Free carnitine C0: 6.9 μmol/L Citrulline: 26 μmol/L | Heterozygous for the pathogenic variant, c.51C>G, and Heterozygous for the pathogenic variant, c.1400C>G in the SLC22A5 gene No P/LP variants in the SLC25A13 gene | Genetically confirmed as CUD, both parents were heterozygote carrier. | 12 months old during latest clinic visit with satisfactory growth and development, on levocarnitine, uneventful clinical course |
| C0-2 (FP) | Free carnitine C0: 6.3 μmol/L | Heterozygous for the pathogenic variant, c.1400C>G in the SLC22A5 gene | Genetically confirmed as CUD carrier | Case closed at 3 months old during latest clinic visit after full biochemical and genetic investigations, normal growth and development. |
| C5DC-1 (FP) | C5DC-carnitine: 0.18 μmol/L | Heterozygous for the pathogenic variant, c.1156C>T in the GCDH gene | Genetically confirmed as GA1 carrier | Case closed at 7 months old during latest clinic visit after full biochemical and genetic investigations, normal growth and development. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, T.C.H.; Mak, C.M.; Yeung, M.C.W.; Law, E.C.-Y.; Cheung, J.; Wong, T.K.; Cheng, V.W.-S.; Lee, J.K.H.; Wong, J.C.L.; Fung, C.W.; et al. Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism. Int. J. Neonatal Screen. 2024, 10, 19. https://doi.org/10.3390/ijns10010019
Chan TCH, Mak CM, Yeung MCW, Law EC-Y, Cheung J, Wong TK, Cheng VW-S, Lee JKH, Wong JCL, Fung CW, et al. Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism. International Journal of Neonatal Screening. 2024; 10(1):19. https://doi.org/10.3390/ijns10010019
Chicago/Turabian StyleChan, Toby Chun Hei, Chloe Miu Mak, Matthew Chun Wing Yeung, Eric Chun-Yiu Law, Jana Cheung, Tsz Ki Wong, Vincent Wing-Sang Cheng, Jacky Kwan Ho Lee, Jimmy Chi Lap Wong, Cheuk Wing Fung, and et al. 2024. "Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism" International Journal of Neonatal Screening 10, no. 1: 19. https://doi.org/10.3390/ijns10010019
APA StyleChan, T. C. H., Mak, C. M., Yeung, M. C. W., Law, E. C.-Y., Cheung, J., Wong, T. K., Cheng, V. W.-S., Lee, J. K. H., Wong, J. C. L., Fung, C. W., Belaramani, K. M., Kwok, A. M. K., & Tsang, K. Y. (2024). Harnessing Next-Generation Sequencing as a Timely and Accurate Second-Tier Screening Test for Newborn Screening of Inborn Errors of Metabolism. International Journal of Neonatal Screening, 10(1), 19. https://doi.org/10.3390/ijns10010019