
Homocysteine and Stroke: A 30-Year Bibliometric Study Uncovering Research Trends and Future Directions


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Data Source and Search Strategy
2.3. Bibliometric Analyses
3. Results
3.1. Overview of Research Landscape
3.2. Scholarly Journal Influence and Collaboration Networks
3.3. Bibliographic Coupling
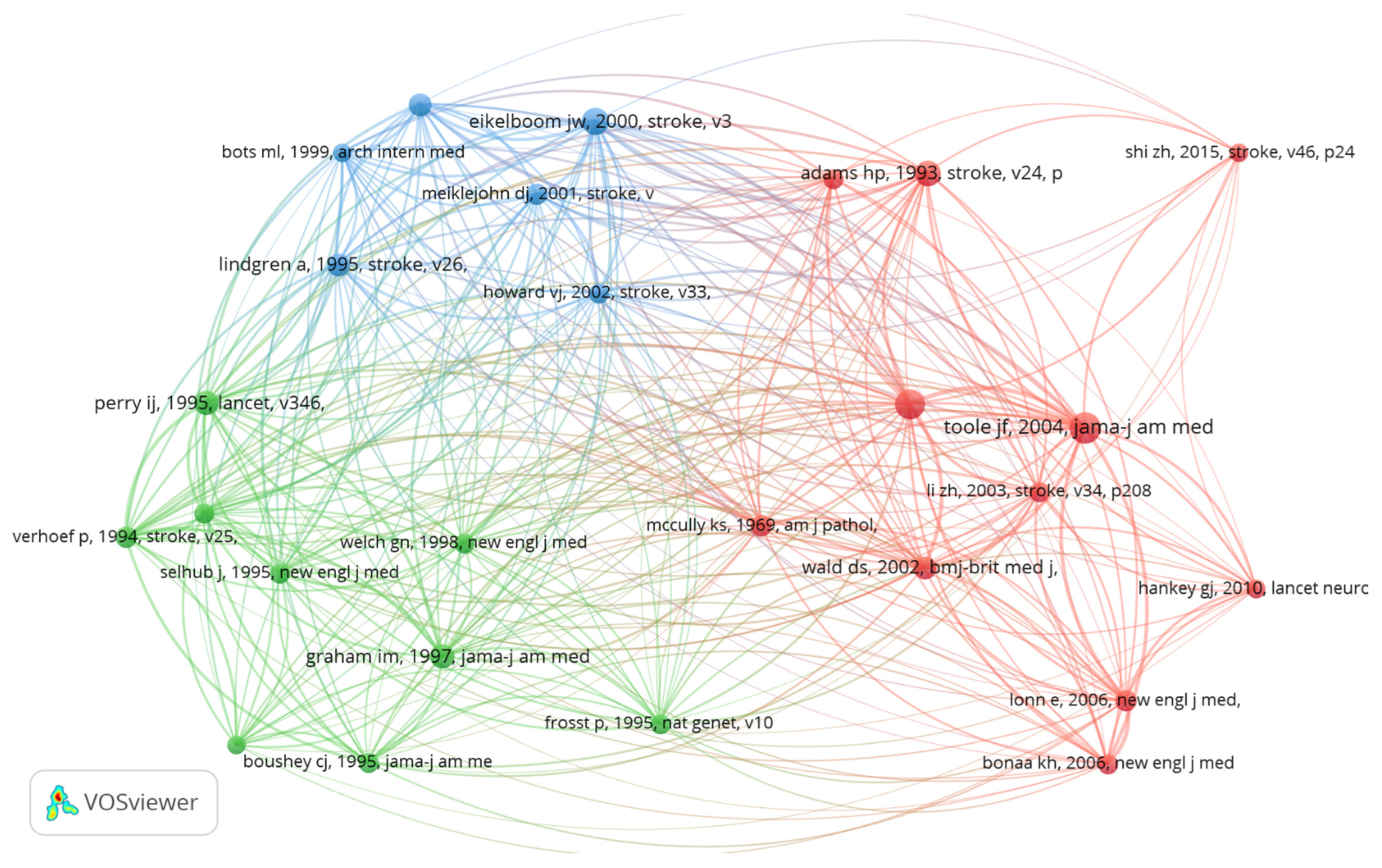
3.4. Co-Cited References
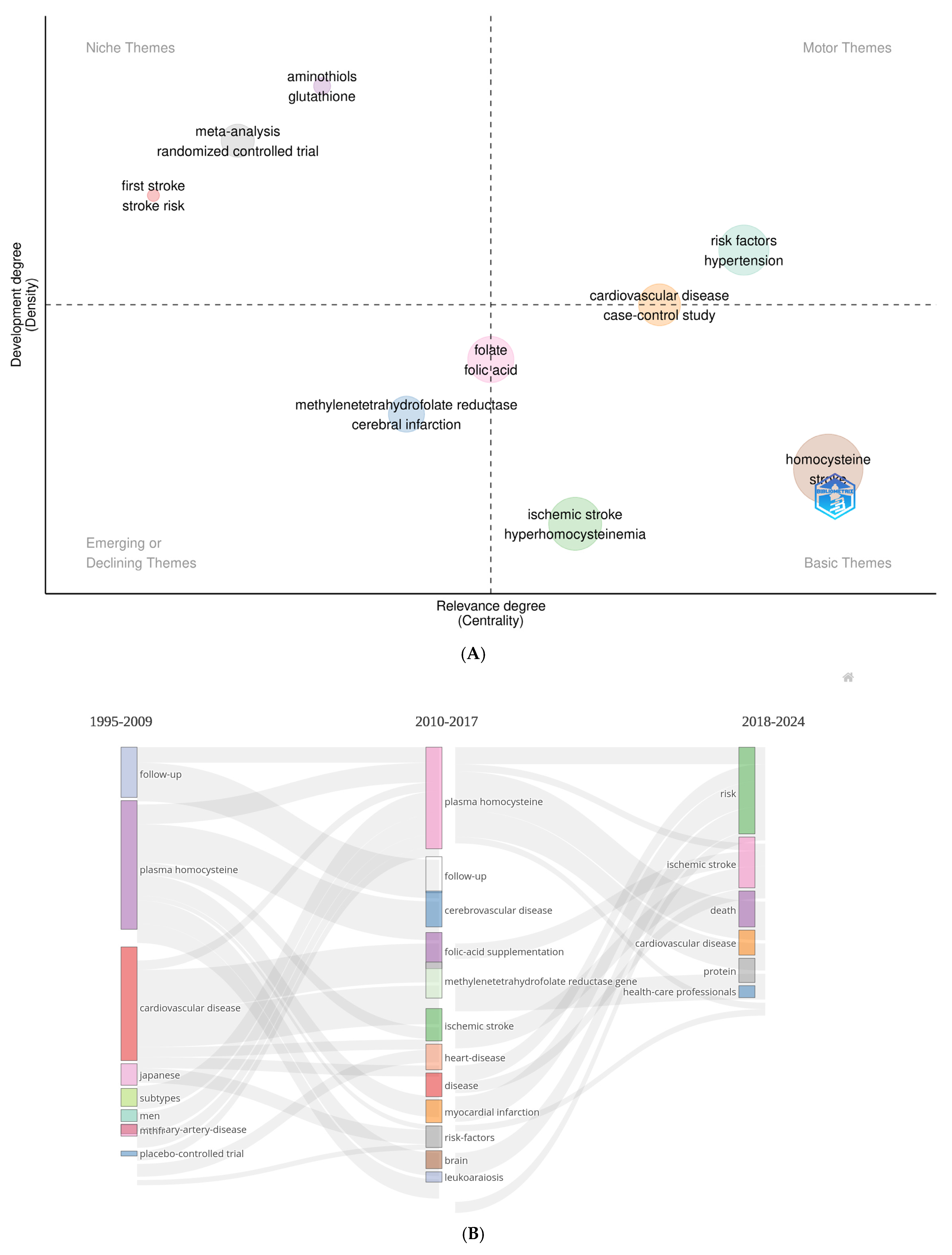
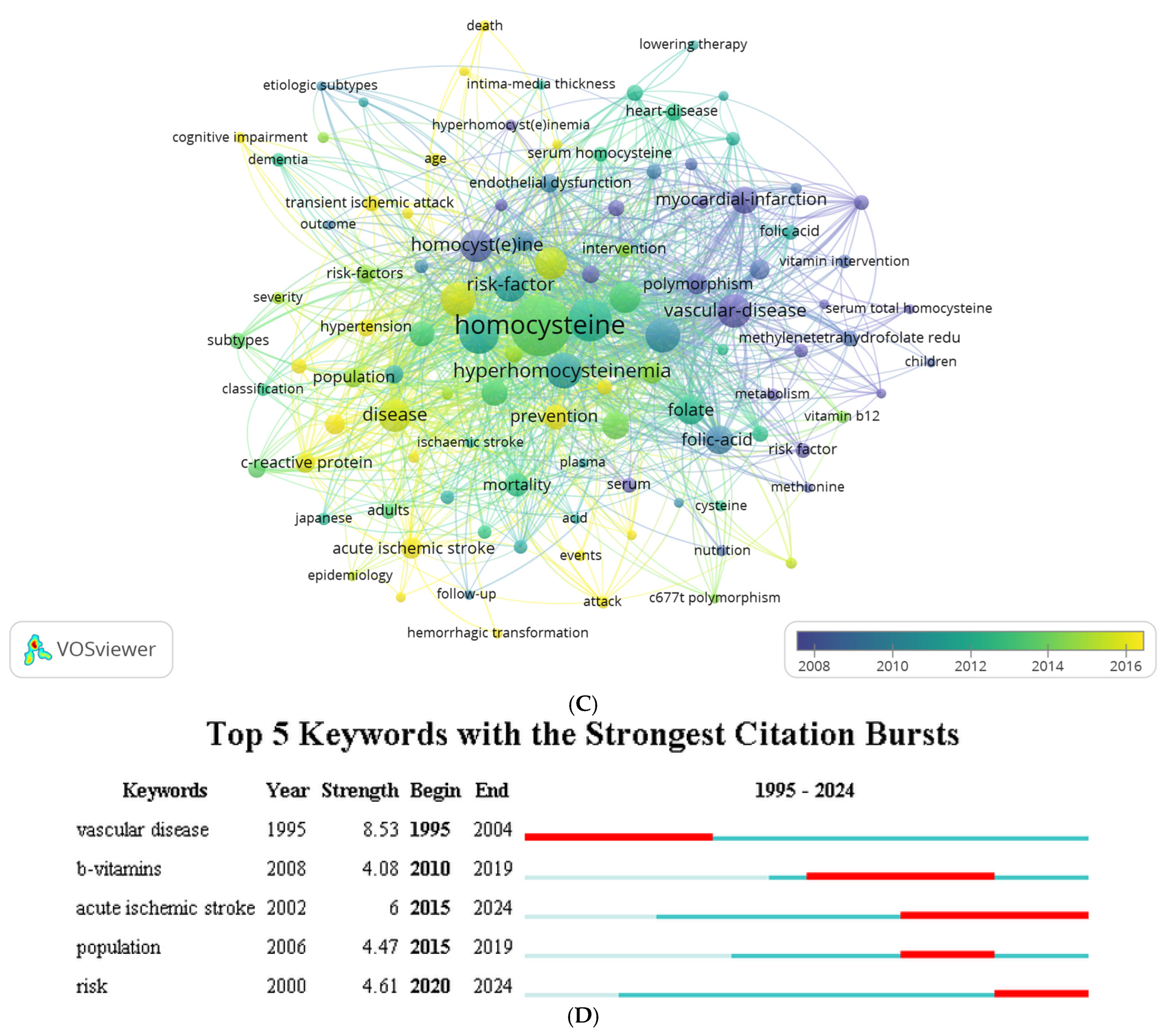
3.5. Thematic Structure, Thematic Evolution, Co-Word, and Burst Analysis
4. Discussion
4.1. Research Landscape and Evolution of Concepts
4.2. Research Trends and Key Hotspots
4.2.1. Evolution of Theories on Homocysteine and Vascular Disease
4.2.2. Emerging Focus on Ischemic Stroke and Risk Factors
4.2.3. Rethinking B-Vitamin Supplementation for Stroke Prevention
4.2.4. Homocysteine Dynamics in Acute Versus Chronic Stroke Phases
4.3. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hankey, G.J.; Eikelboom, J.W. Homocysteine and stroke. Curr. Opin. Neurol. 2001, 14, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.K.; Au, A.; Menon, S.; Gan, S.H.; Griffiths, L.R. Clinical relevance of MTHFR, eNOS, ACE, and ApoE gene polymorphisms and serum vitamin profile among Malay patients with ischemic stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 2017–2025. [Google Scholar] [CrossRef]
- Holmes, M.V.; Newcombe, P.; Hubacek, J.A.; Sofat, R.; Ricketts, S.L.; Cooper, J.; Breteler, M.M.B.; Bautista, L.E.; Sharma, P.; Whittaker, J.C.; et al. Effect modification by population dietary folate on the association between MTHFR genotype, homocysteine, and stroke risk: A meta-analysis of genetic studies and randomised trials. Lancet 2011, 378, 584–594. [Google Scholar] [CrossRef]
- Wei, L.K.; Sutherland, H.G.; Griffiths, L.R. Epigenetics and ischemic stroke: A bibliometric analysis from 2014 to 2024. Epigenet. Insights 2024, 17, e004. [Google Scholar]
- Toole, J.F.; Malinow, M.R.; Chambless, L.E.; Spence, J.D.; Pettigrew, L.C.; Howard, V.J.; Howard, G. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death: The Vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial. JAMA 2004, 291, 565–575. [Google Scholar] [CrossRef]
- Perry, I.J.; Morris, R.W.; Ebrahim, S.B.; Shaper, A.G.; Refsum, H.; Ueland, P.M. Prospective study of serum total homocysteine concentration and risk of stroke in middle-aged British men. Lancet 1995, 346, 1395–1398. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, A.; Brattström, L.; Norrving, B.; Hultberg, B.; Andersson, A.; Johansson, B.B. Plasma homocysteine in the acute and convalescent phases after stroke. Stroke 1995, 26, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Bostom, A.G.; Rosenberg, I.H.; Silbershatz, H.; Jacques, P.F.; Selhub, J.; D’Agostino, R.B.; Wilson, P.W. Nonfasting plasma total homocysteine levels and stroke incidence in elderly persons: The Framingham Study. Ann. Intern. Med. 1999, 131, 352–355. [Google Scholar] [CrossRef]
- Meiklejohn, D.J.; Vickers, M.A.; Dijkhuisen, R.; Greaves, M. Plasma homocysteine concentrations in the acute and convalescent periods of atherothrombotic stroke. Stroke 2001, 32, 57–62. [Google Scholar] [CrossRef]
- Iso, H.; Moriyama, Y.; Sato, S.; Kitamura, A.; Tanigawa, T.; Yamagishi, K.; Konishi, M. Serum total homocysteine concentrations and risk of stroke and its subtypes in Japanese. Circulation 2004, 109, 2766–2772. [Google Scholar] [CrossRef]
- Li, Z.; Sun, L.; Zhang, H.; Liao, Y.; Wang, D.; Zhao, B.; Zhu, Z.; Zhao, J.; Ma, A.; Han, Y.; et al. Elevated plasma homocysteine was associated with hemorrhagic and ischemic stroke, but methylenetetrahydrofolate reductase gene C677T polymorphism was a risk factor for thrombotic stroke. Stroke 2003, 34, 2085–2090. [Google Scholar] [CrossRef] [PubMed]
- Bots, M.L.; Launer, L.J.; Lindemans, J.; Hoes, A.W.; Hofman, A.; Witteman, J.C.M.; Koudstaal, P.J.; Grobbee, D.E. Homocysteine and short-term risk of myocardial infarction and stroke in the elderly. Arch. Intern. Med. 1999, 159, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Guan, Y.; Huo, Y.R.; Liu, S.; Zhang, M.; Lu, H.; Yue, W.; Wang, J.; Ji, Y. Elevated total homocysteine levels in acute ischemic stroke are associated with long-term mortality. Stroke 2015, 46, 2419–2425. [Google Scholar] [CrossRef]
- Saposnik, G.; Ray, J.G.; Sheridan, P.; McQueen, M.; Lonn, E. Homocysteine-lowering therapy and stroke risk, severity, and disability. Stroke 2009, 40, 1365–1372. [Google Scholar] [CrossRef]
- Casas, J.P.; Bautista, L.E.; Smeeth, L.; Sharma, P.; Hingorani, A.D. Homocysteine and stroke: Evidence on a causal link from mendelian randomisation. Lancet 2005, 365, 224–232. [Google Scholar] [CrossRef]
- Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke. JAMA 2002, 288, 2015–2022. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Hankey, G.J.; Anand, S.S.; Lofthouse, E.; Staples, N.; Baker, R.I. Association between high homocyst(e)ine and ischemic stroke due to large- and small-artery disease but not other etiologic subtypes of ischemic stroke. Stroke 2000, 31, 1069–1075. [Google Scholar] [CrossRef]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, G.E.E., 3rd. Classification of subtype of acute ischemic stroke: Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Graham, I.M.; Daly, L.E.; Refsum, H.M.; Robinson, K.; Brattström, L.E.; Ueland, P.M.; Palma-Reis, R.J.; Boers, G.H.; Sheahan, R.G.; O Israelsson, B.; et al. Plasma homocysteine as a risk factor for vascular disease. JAMA 1997, 277, 1775–1781. [Google Scholar] [CrossRef]
- Wald, D.S. Homocysteine and cardiovascular disease: Evidence on causality from a meta-analysis. BMJ 2002, 325, 1202–1206. [Google Scholar] [CrossRef]
- Marti-Carvajal, A.J.; Sola, I.; Lathyris, D.; Dayer, M. Homocysteine-lowering interventions for preventing cardiovascular events. Cochrane Database Syst. Rev. 2017, 8, CD006612. [Google Scholar] [PubMed]
- McCully, S.K. Homocysteine, vitamins, and vascular disease prevention. Am. J. Clin. Nutr. 2007, 86, 1563S–1568S. [Google Scholar] [CrossRef]
- Zhou, Q.; Xu, Z.; Duan, Y.; Tang, H.; Zhang, H.; Liu, H. MTHFR C677T, hyperhomocysteinemia, and their interactions with traditional risk factors in early neurological deterioration in Chinese patients with ischemic stroke. Heliyon 2024, 10, e31003. [Google Scholar] [CrossRef]
- Yang, Z.J.; Huang, S.Y.; Zhong, K.Y.; Huang, W.G.; Huang, Z.H.; He, T.T.; Yang, M.-T.; Wusiman, M.; Zhou, D.-D.; Chen, S.; et al. Betaine alleviates cognitive impairment induced by homocysteine through attenuating NLRP3-mediated microglial pyroptosis in an m6A-YTHDF2-dependent manner. Redox Biol. 2024, 69, 103026. [Google Scholar] [CrossRef]
- Holmen, M.; Hvas, A.M.; Arendt, J.F.H. Hyperhomocysteinemia and ischemic stroke: A potential dose-response association—A systematic review and meta-analysis. TH Open 2021, 5, e420–e437. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Chen, Y.; Yang, T.; He, X.; Yang, Y.; Chen, J.; Han, L. Blood biomarkers for post-stroke cognitive impairment: A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2024, 33, 107632. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.H.; Li, J.; Li, X.L.; Ding, M.; Mao, C.J.; Zhu, X.Y.; Liu, C.-F. Hypertension with hyperhomocysteinemia increases the risk of early cognitive impairment after first-ever ischemic stroke. Eur. Neurol. 2019, 82, 75–85. [Google Scholar] [CrossRef]
- Li, H.; Shu, L.; Dai, Q.; Wu, T. Association between plasma total homocysteine (tHcy) and strokes: A meta-analysis. Pteridines 2022, 33, 58–68. [Google Scholar] [CrossRef]
- Ji, Y.; Tan, S.; Xu, Y.; Chandra, A.; Shi, C.; Song, B.; Qin, J.; Gao, Y. Vitamin B supplementation, homocysteine levels, and the risk of cerebrovascular disease. Neurology 2013, 81, 1298–1307. [Google Scholar] [CrossRef]
- Wei, L.K.; Sutherland, H.; Au, A.; Camilleri, E.; Haupt, L.M.; Gan, S.H.; Griffiths, L.R. A potential epigenetic marker mediating serum folate and vitamin B12 levels contributes to the risk of ischemic stroke. Biomed. Res. Int. 2015, 2015, 167976. [Google Scholar]
- Sikora, M.; Bretes, E.; Perła-Kaján, J.; Utyro, O.; Borowczyk, K.; Piechocka, J.; Głowacki, R.; Wojtasz, I.; Kaźmierski, R.; Jakubowski, H. Homocysteine thiolactone and other sulfur-containing amino acid metabolites are associated with fibrin clot properties and the risk of ischemic stroke. Sci. Rep. 2024, 14, 11222. [Google Scholar] [CrossRef]
- Mathew, A.R.; Di Matteo, G.; La Rosa, P.; Barbati, S.A.; Mannina, L.; Moreno, S.; Tata, A.M.; Cavallucci, V.; Fidaleo, M. Vitamin B12 deficiency and the nervous system: Beyond metabolic decompensation—Comparing biological models and gaining new insights into molecular and cellular mechanisms. Int. J. Mol. Sci. 2024, 25, 590. [Google Scholar] [CrossRef]
- Zhang, N.; Zhou, Z.; Chi, X.; Fan, F.; Li, S.; Song, Y.; Zhang, Y.; Qin, X.; Sun, N.; Wang, X.; et al. Folic acid supplementation for stroke prevention: A systematic review and meta-analysis of 21 randomized clinical trials worldwide. Clin. Nutr. 2024, 43, 1706–1716. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Cai, J.; Tian, Y. The prognostic value of homocysteine in acute ischemic stroke patients: A systematic review and meta-analysis. Front. Syst. Neurosci. 2021, 14, 600582. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Jiang, Y.; Zhang, S.; Tie, T.; Cheng, Y.; Su, X.; Man, Z.; Hou, J.; Sun, L.; Tian, M.; et al. The association between homocysteine and ischemic stroke subtypes in Chinese. Medicine 2020, 99, e19467. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, S.; Nath, M.; Misra, S.; Kumar, P. From A to E: Uniting vitamins against stroke risk—A systematic review and network meta-analysis. Eur. J. Clin. Investig. 2024, 54, e14165. [Google Scholar] [CrossRef]
- Kataria, N.; Yadav, P.; Kumar, R.; Kumar, N.; Singh, M.; Kant, R.; Kalyani, V. Effect of vitamin B6, B9, and B12 supplementation on homocysteine level and cardiovascular outcomes in stroke patients: A meta-analysis of randomized controlled trials. Cureus 2021, 13, e14958. [Google Scholar] [CrossRef]
- Zhang, N.; Wu, Z.; Bai, X.; Song, Y.; Li, P.; Lu, X.; Huo, Y.; Zhou, Z. Dosage exploration of combined B-vitamin supplementation in stroke prevention: A meta-analysis and systematic review. Am. J. Clin. Nutr. 2024, 119, 821–828. [Google Scholar] [CrossRef]
- Spence, J.D.; Hankey, G.J. Problem in the recent American Heart Association guideline on secondary stroke prevention: B vitamins to lower homocysteine do prevent stroke. Stroke 2022, 53, 2702–2708. [Google Scholar] [CrossRef]
- Dong, W.C.; Guo, J.L.; Xu, L.; Jiang, X.H.; Chang, C.H.; Jiang, Y.; Zhang, Y.-Z. Impact of homocysteine on acute ischemic stroke severity: Possible role of aminothiols redox status. BMC Neurol. 2024, 24, 175. [Google Scholar] [CrossRef]
- Wang, Y.; Hou, R.; Liu, Y. Plasma homocysteine (Hcy) concentration functions as a predictive biomarker of SPECT-evaluated post-ischemic hyperperfusion in acute ischemic stroke. Pharmacogenom. Pers. Med. 2023, 16, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Žitňanová, I.; Šiarnik, P.; Kollár, B.; Chomová, M.; Pazderová, P.; Andrezálová, L.; Ježovičová, M.; Koňariková, K.; Laubertová, L.; Krivošíková, Z.; et al. Oxidative stress markers and their dynamic changes in patients after acute ischemic stroke. Oxidative Med. Cell. Longev. 2016, 2016, 9761697. [Google Scholar] [CrossRef] [PubMed]
- Maksimova, M.Y.; Ivanov, A.V.; Virus, E.D.; Nikiforova, K.A.; Ochtova, F.R.; Suanova, E.T.; Kruglova, M.P.; Piradov, M.A.; Kubatiev, A.A. Impact of glutathione on acute ischemic stroke severity and outcome: Possible role of aminothiols redox status. Redox Rep. 2021, 26, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Kamal, F.Z.; Lefter, R.; Jaber, H.; Balmus, I.M.; Ciobica, A.; Iordache, A.C. The role of potential oxidative biomarkers in the prognosis of acute ischemic stroke and the exploration of antioxidants as possible preventive and treatment options. Int. J. Mol. Sci. 2023, 24, 6389. [Google Scholar] [CrossRef]
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: Strengths and weaknesses. FASEB J. 2008, 22, 338–342. [Google Scholar] [CrossRef]
- Liu, W. Caveats for the use of Web of Science Core Collection in old literature retrieval and historical bibliometric analysis. Technol. Forecast. Soc. Change 2021, 172, 121023. [Google Scholar] [CrossRef]
- Heart Outcomes Prevention Evaluation (HOPE) 2 Investigators. Homocysteine lowering with folic acid and B vitamins in vascular disease. N. Engl. J. Med. 2006, 354, 1567–1577. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NGC/NLC Ratio | Normalized Local Citations (NLCs) | Normalized Global Citations (NGCs) | Document Title [Reference] | Rank | |
|---|---|---|---|---|---|
| 1.28 | 3.91 | 5.00 | Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial Infarction, and death The Vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial [5] | 1 | |
| 1.54 | 1.03 | 1.59 | Prospective study of serum total homocysteine concentration and risk of stroke in middle-aged british men [6] | 2 | |
| 0.42 | 0.97 | 0.41 | Plasma homocysteine in the acute and convalescent phases after stroke [7] | 3 | |
| 1.02 | 2.18 | 2.22 | Nonfasting plasma total homocysteine levels and stroke incidence in elderly persons: The Framingham study [8] | 4 | |
| 0.36 | 3.48 | 1.26 | Plasma homocysteine concentrations in the acute and convalescent periods of atherothrombotic stroke [9] | 5 | |
| 0.33 | 1.70 | 0.56 | Serum total homocysteine concentrations and risk of stroke and its subtypes in japanese [10] | 6 | |
| 0.85 | 2.45 | 2.09 | Elevated plasma homocysteine was associated with hemorrhagic and ischemic stroke, but methylenetetrahydrofolate reductase gene C677T polymorphism was a risk factor for thrombotic stroke: A multicenter case-control study in China [11] | 7 | |
| 0.91 | 1.54 | 1.40 | Homocysteine and short-term risk of myocardial infarction and stroke in the elderly: The Rotterdam study [12] | 8 | |
| 0.91 | 3.48 | 3.18 | Elevated total homocysteine levels in acute ischemic stroke are associated with long-term mortality [13] | 9 | |
| 0.96 | 5.02 | 4.81 | Homocysteine-lowering therapy and stroke risk, severity, and disability: Additional findings from the Hope 2 trial [14] | 10 | |
| TLS | Year | Co-Cited (n) | First Author [Country] | DOI [Reference] | Rank |
|---|---|---|---|---|---|
| 239 | 2004 | 59 | Toole JF [USA] | * [10.1001/jama.291.5.565] [5] | 1 |
| 246 | 2002 | 55 | Clarke R [USA] | [10.1001/jama.288.16.2015] [16] | 2 |
| 193 | 2000 | 43 | Eikelboom JW [Canada] | [10.1161/01.str.31.5.1069] [17] | 3 |
| 159 | 1993 | 42 | Adams HP [USA] | [10.1161/01.str.24.1.35] [18] | 4 |
| 162 | 1997 | 34 | Graham IM [UK] | [10.1001/jama.277.22.1775] [19] | 5 |
| 202 | 1995 | 34 | Perry IJ [UK] | * [10.1016/S0140-6736(95)92407-8] [6] | 6 |
| 161 | 1995 | 33 | Wald DS [UK] | [10.1136/bmj.325.7374.1202] [20] | 7 |
| 168 | 2002 | 32 | Lindgren A [Sweden] | * [10.1161/01.STR.26.5.795] [7] | 8 |
| 174 | 1995 | 31 | Bostom AG [USA] | * [10.7326/0003-4819-131-5-199909070-00006] [8] | 9 |
| 165 | 1999 | 29 | Meiklejohn DJ [UK] | * [10.1161/01.str.32.1.57] [9] | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, L.K.; Menon, S.; Griffiths, L.R. Homocysteine and Stroke: A 30-Year Bibliometric Study Uncovering Research Trends and Future Directions. J. Mind Med. Sci. 2025, 12, 8. https://doi.org/10.3390/jmms12010008
Wei LK, Menon S, Griffiths LR. Homocysteine and Stroke: A 30-Year Bibliometric Study Uncovering Research Trends and Future Directions. Journal of Mind and Medical Sciences. 2025; 12(1):8. https://doi.org/10.3390/jmms12010008
Chicago/Turabian StyleWei, Loo Keat, Saras Menon, and Lyn R. Griffiths. 2025. "Homocysteine and Stroke: A 30-Year Bibliometric Study Uncovering Research Trends and Future Directions" Journal of Mind and Medical Sciences 12, no. 1: 8. https://doi.org/10.3390/jmms12010008
APA StyleWei, L. K., Menon, S., & Griffiths, L. R. (2025). Homocysteine and Stroke: A 30-Year Bibliometric Study Uncovering Research Trends and Future Directions. Journal of Mind and Medical Sciences, 12(1), 8. https://doi.org/10.3390/jmms12010008