
From Sedentary to Success: How Physical Activity Transforms Diabetes Management: A Systematic Review


 , , , , ,
, , , , , 
Abstract
1. Introduction
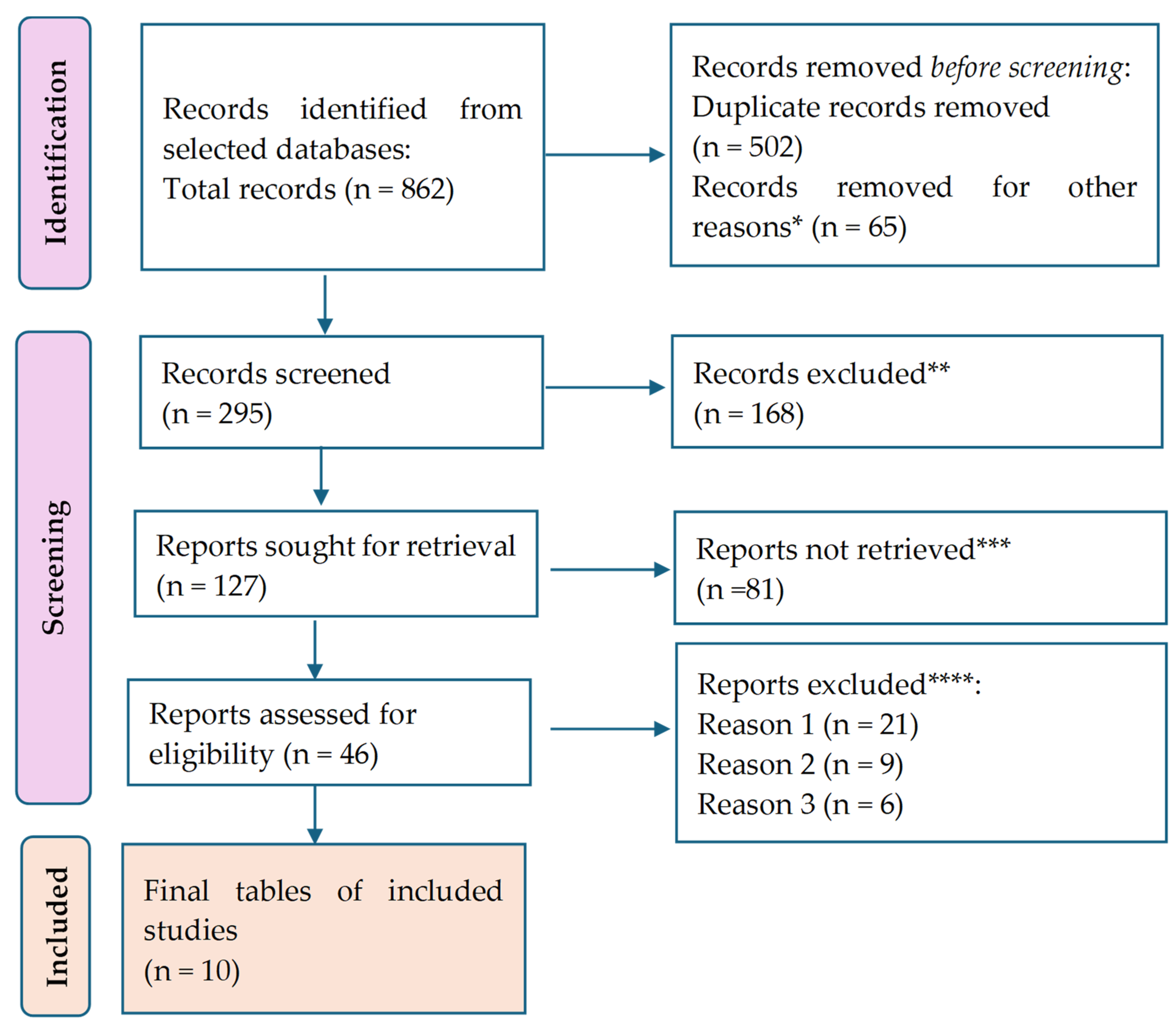
2. Materials and Methods
3. Results

| Study (Year) | Participants | Mean Age (±S.D.) | FBG */HbA1C/HOMA-IR ** Means at Baseline (±SD ***) | Intervention | FBG/HbA1C/HOMA-IR Means After Intervention (±SD) | Differences in FBG/HbA1C/HOMA-IR (±SD) | p Value | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Whitaker et al. [28] (2019) | 1922 | 45.3 years (±3.5) | FBG: 95.0 mg/dL (±12.6) | The activity recorded by the accelerometer during the 20-year examination, including sedentary behavior, light physical activity (L.P.A.), and moderate-to-vigorous physical activity (M.V.P.A.), was linked to cardiometabolic risk factors after a decade, specifically during the year 30 examination. Subsequently, we replicated this procedure by analyzing the impact of alterations in accelerometer-measured activity during the two examinations (e.g., sedentary = year 30 sedentary − year 20 sedentary) on modifications in the dependent variable, specifically the change in cardiometabolic risk factors over the same 10-year span (e.g., risk score = year 30 risk score − year 20 risk score). Sedentary time at year 20 − 490.1 ± 102.4, sedentary time at year 30 − 532.3 ± 102.7 | FBG: 94.6 mg/dL (±14.0) | FBG: −0.4 mg/dL | 0.034 | Substituting 30 min of inactive time with 30 min of low-intensity physical activity led to a decrease of 0.15 cm in waist circumference, a decrease of 0.20 μU/mL in insulin levels, an increase of 0.20 mg/dL in HDL-C levels, and a decrease of 0.01 standard deviation in the composite risk score. Substituting an equivalent amount of inactive time with moderate-to-vigorous physical activity led to a decrease of 0.73 μU/mL in insulin levels and a decrease of 4.57 mg/dL in lipid levels. Substituting L.P.A. with M.V.P.A. led to a decrease of 0.54 μU/mL in insulin levels and a decrease of 4.51 mg/dL in triglyceride levels. |
| Zheng et al. [29] (2020) | 94 | 21.7 years (±3.38) | FBG: 106 mg/dL (±5.4) | At their initial visit, participants were directed to wear the activPAL device for a continuous period of seven days while adhering to their usual daily routine. The activPAL device was removed on the morning of the seventh day. On the ninth day, participants returned to the laboratory after a 10 h period of not eating to collect blood samples and return the activPAL device. | FBG: 86.3 mg/dL (±2.1) | FBG: −9.7 mg/dL | 0.001 | Essentially, inactive behaviors such as prolonged periods of sitting, extended sedentary episodes, and sedentary bouts can significantly contribute to the development of cardiovascular and metabolic disorders in physically active young boys. |
| Debache et al. [30] (2019) | 131 | 50.55 years (±9.57) | FBG: 96.9 mg/dL (±11.4) | Participants were instructed to wear accelerometers on their trunk and right upper leg for seven consecutive days while engaging in their normal daily activities, excluding water-based activities, throughout their waking hours under unrestricted living conditions. Furthermore, they donned a compact G.P.S. gadget and meticulously recorded the locations they frequented along with the duration of device usage. | FBG: 74.84 mg/dL (±37.74) | FBG: −21.16 mg/dL | 0.001 | The glucose level was shown to be greater when both short and long sedentary sequences contributed equally to the overall inactive duration. For instance, a 0.1 increase in the Gini index corresponded to a 3.0 mg/dL fall in glucose levels. The counter-intuitive finding was validated by the inverse relationship between the ratio of sedentary time spent in bouts to total sedentary time and the glucose level. As the proportion of sedentary time spent in bouts fell, the glucose level climbed. The transition from a ratio of 0.9707 (1st quartile) to 0.9892 (3rd quartile) corresponded to a 1.3 mg/dL reduction in glucose level. |
| Honda et al. [31] (2019) | 1758 | 63.6 years (±0.8) | HOMA-IR: 1.49 (±1.35) | Participants were equipped with an accelerometer for a minimum of seven days and had a thorough health check-in in 2012. A 75 g oral glucose tolerance test confirmed the diagnosis of diabetes mellitus. Logistic and linear regression models were used to estimate the relationships among sedentary time, the occurrence of diabetes mellitus, the levels of the homeostasis model assessment of insulin resistance. | H.O.M.A.-I.R.: 1.15 (±0.97) | HOMA-IR: 0.34 | 0.102 | After accounting for demographic and lifestyle factors, such as moderate-to-vigorous physical activity, individuals who spent ten or more hours engaging in sedentary time had a significantly greater likelihood of developing diabetes than those who spent less than 6 h engaging in sedentary time. This notable correlation persisted even after accounting for general and abdominal obesity (as assessed by body mass index and waist circumference). However, it diminished after accounting for dietary energy consumption or the homeostasis model assessment of insulin resistance. There was a positive correlation between sedentary time and degrees of insulin resistance, as measured by the homeostasis model evaluation, among non-diabetic subjects. This correlation remained significant even after adjusting for factors such as obesity or calorie intake. |
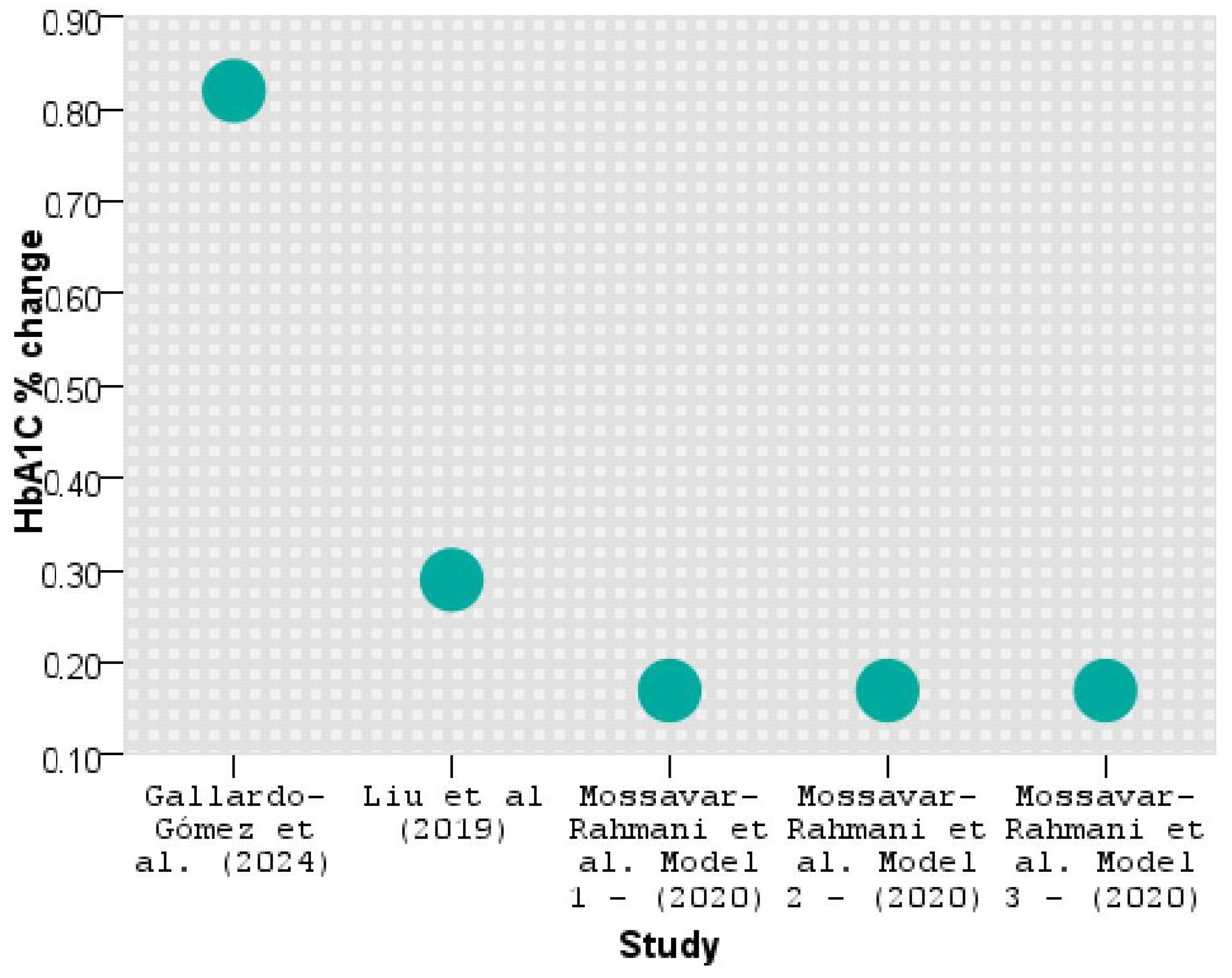
| Mossavar-Rahmani et al. [32] (2020) | Not provided | Not provided | Not provided | The measured activity was quantified as 150 min per week of moderate-intensity physical activity, 75 min per week of high-intensity activity, or an equivalent combination of both when scaled to 7 days of accelerometer wear. Model 1 was adjusted for age, sex, and use of medications; model 2 adjusted model 1 for income, education, employment status, smoking, alcohol consumption, and health insurance status; model 3 adjusted model 2 for time and covariates. We considered HbA1C from model 3 only from each quartile as it considered most variables. | HbA1C: 0.17% (±0.15–0.19) | There was a tendency for a decrease in the average increase in HbA1c when comparing the groups | 0.001 | There was a tendency for a decrease in the average increase in HbA1c when comparing the group with the least amount of sedentary behavior to the group with the highest amount. In general, independent of the glycemic level or presence of cardiometabolic disease, persons who followed the recommendations for moderate-to-vigorous physical activity during visit 1 experienced considerably smaller average increases in fasting glucose levels compared to adults who did not follow the recommendations, after accounting for all relevant factors. |
| Banitalebi et al. [33] (2019) | 14 SIT, 14 A + R | 55.36 years (±5.94) SIT; 54.14 years (±5.43) A + R | FBG: 210.07 mg/dL (±32.91) SIT; 214.64 mg/dL (±27.67) A + R | 3 days a week, 50 min, 10 weeks, S.I.T.: treadmill, cycle ergometer | FBG: 137.36 mg/dL (±32.95) SIT; 163.86 mg/dL (±71.47) A + R | FBG: −72.71 mg/dL (SIT group); −50.78 mg/dL (A + R group) | 0.001 | Both exercise groups showed significant and equivalent improvements in aerobic capacity, fasting glucose, and HbA1c compared to the control group. The insulin, weight, and body mass index levels, regardless of the group, decreased dramatically over time. There was no correlation between alterations in myokines and changes in body composition or metabolic profile. |
| A + R: bilateral leg press, lateral pull-down, bench press, bilateral biceps curl, and bilateral triceps push-down | Both S.I.T. and A + R training did not affect myokines tested 48 h after exercise in individuals with type 2 diabetes, even though they improved aerobic capacity and glucose homeostasis compared to the control group. | |||||||
| Gallardo-Gómez et al. [34] (2024) | 1446 T2DM patients from 126 studies | Not provided | HbA1C: 9% (±0.62) | To investigate the correlation between varying amounts of physical activity (both overall and specific to interventions) and glycemic control in individuals diagnosed with type 2 diabetes. | HbA1C: 8.18% (±0.16) | HbA1C: 0.82% (±0.11) | 0.001 | When individuals accumulated 1100 MET min/week (metabolic equivalent task), which is considered the ideal dose with multicomponent therapies, they experienced clinically significant reductions in HbA1c levels for severe uncontrolled diabetes (ranging from −1.06% to −0.67%) and uncontrolled diabetes (ranging from −0.65% to −0.50%). |
| Mendes et al. [35] (2019) | 15 | 60.25 years (±3.14) | FBG: 114.25 mg/dL (±24.65) control session of rest (CON); 112.67 mg/dL (±21.98) HIIT; 115.75 mg/dL (± 21.84) moderate-intensity continuous training (MICN) | While in the postprandial stage, the participants experienced three different experimental conditions in a random order. These conditions included a treadmill walking H.I.I.T. session consisting of five sets of 3 min at 70% of heart rate reserve (H.R.R.) followed by 3 min at 30% H.R.R., a treadmill walking M.I.C.T. session lasting 30 min at 50% H.R.R., and CON. FBG measurements were obtained before, throughout, and up to 50 min following the experimental circumstances. | FBG: 114.08 mg/dL (±24.27) CON; 110.50 mg/dL (±17.73) HIIT; 114.00 mg/dL (±22.31) MICN | FBG: 0.17 mg/dL CON; 2.17 mg/dL HIIT; 1.75 mg/dL MICN | 0.001 | Both high-intensity interval training and moderate-intensity continuous training treadmill walking sessions resulted in decreased blood glucose levels during exercise and a 50 min recovery period in the laboratory compared to the control group. This effect was observed due to the interaction between time and condition. The impact of H.I.I.T. was more significant than that of M.I.C.T. |
| Liu et al. [36] (2019) | 163 participants with H.I.I.T. out of 345 from 13 studies | 15.3 years (±2.2) and 70.1 years (±2.4) (across the 13 studies) | Not provided | The clinical parameters and social cognitive factors of the intervention and control groups were compared after 16 weeks of physical activity (P.A.) intervention among patients with prediabetes. Participants in the intervention group were instructed to do at least 150 min of moderate-intensity P.A. per week in the morning (6:00 a.m. to 11:59 a.m.) or afternoon (12:00 p.m. to 5:59 p.m.). | Not provided | HbA1C: −0.29% (±0.55) FBG: −0.41 mg/dL (±0.91) | 0.001 | HIIT resulted in a noteworthy decrease in body mass index, body fat percentage, HbA1c levels, fasting insulin levels, and VO2peak (maximum oxygen consumption) in individuals diagnosed with T2M. Concerning alterations in the body composition of patients, H.I.I.T. demonstrated a significant improvement in body weight (mean difference: −1.22 kg) and body mass index (mean difference: −0.40 kg/m2) compared to M.I.C.T. |
| Shamizadeh et al. [37] (2020) | 136 prediabetes participants in the intervention group | 51.3 years (±11.2) | FBG: 108.4 mg/dL (±6.1) | Over 16 weeks, the participants were educated about the risk of diabetes and motivated to engage in physical activity as a straightforward method to lower their chances of developing diabetes. Each participant was instructed to abstain from eating for a period of 10–12 h before the blood tests were taken at baseline and after 16 weeks. | FBG: 99.4 mg/dL (±8.1) | FBG: 9 mg/dL | 0.002 | The general linear mixed model analysis revealed substantial decreases in FBG, body mass index (B.M.I.), weight, and diastolic blood pressure (B.P.) in the intervention group compared to the control group. The primary physical activity intervention resulted in a medium-sized drop in FBG levels compared to the control group after 16 weeks. Thus, physical activity intervention positively decreases the likelihood of prediabetes progressing to diabetes in rural patients. |
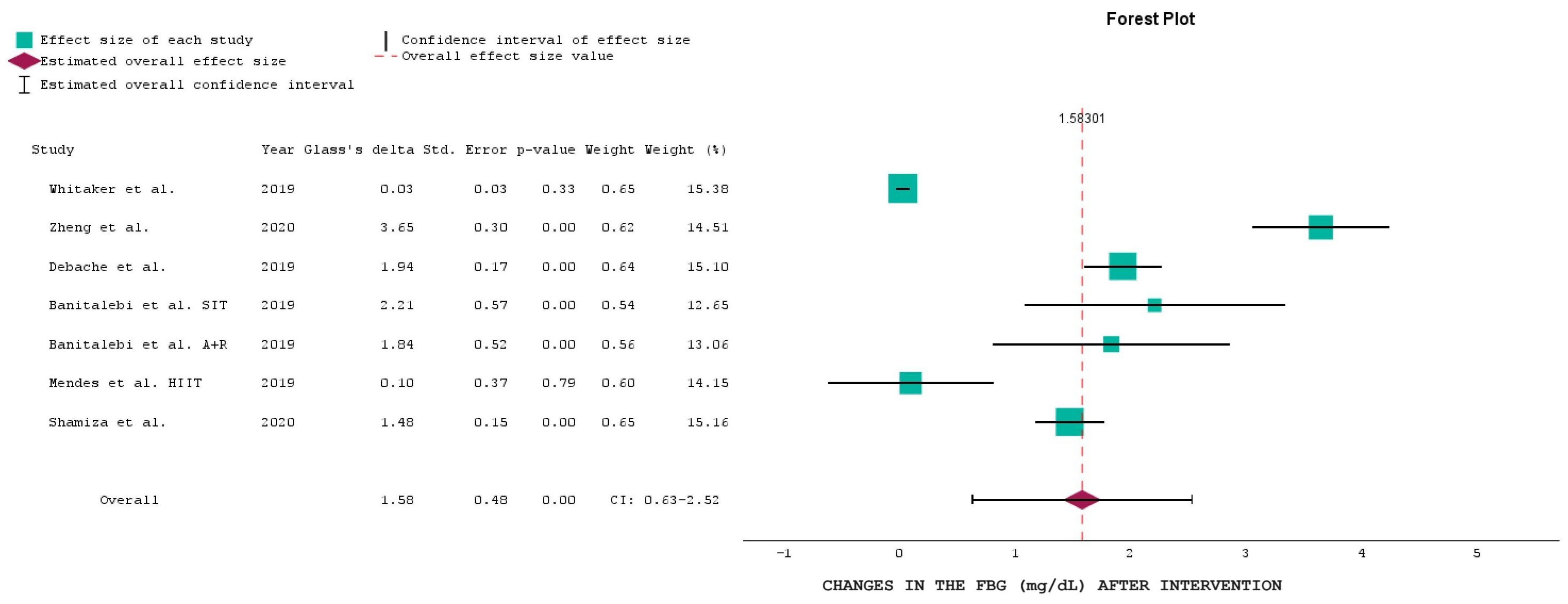
Statistical Analysis of the Results
- Diversity of study populations: some studies included participants with prediabetes or impaired glucose tolerance, rather than exclusively focusing on individuals diagnosed with T2DM. These participants may have had baseline FBG levels below the diabetic threshold but were still at risk of developing T2DM. Some studies also included mixed cohorts, where participants with both prediabetes and T2DM were analyzed together, resulting in an overall lower baseline FBG mean.
- Variability in inclusion criteria: the inclusion criteria for studies varied, with some trials assessing the impact of physical activity on glucose metabolism in individuals at different stages of metabolic dysregulation (e.g., those with insulin resistance or early-stage T2DM). Some studies focused on lifestyle interventions in high-risk populations rather than focusing exclusively on patients with established T2DM, a fact which may explain why their baseline FBG values were lower than expected for a diabetic cohort.
- Impact of medication use: although pharmacological treatment details were not available for all studies, it is possible that participants in certain trials were already receiving a glucose-lowering therapy at baseline, a fact which could have resulted in lower FBG values before the intervention.
- Variations in measurement techniques and study design: differences in laboratory standards, sample timing, and glucose measurement protocols among studies could have influenced baseline FBG values. Some studies reported mean FBG levels, which may not fully capture individual variations or the presence of outliers.
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Casari, S.; Di Paola, M.; Banci, E.; Diallo, S.; Scarallo, L.; Renzo, S.; Gori, A.; Renzi, S.; Paci, M.; de Mast, Q.; et al. Changing Dietary Habits: The Impact of Urbanization and Rising Socio-Economic Status in Families from Burkina Faso in Sub-Saharan Africa. Nutrients 2022, 14, 1782. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- American Diabetes Association Professional Practice Committee. Introduction and Methodology: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47 (Suppl. S1), S1–S4. [CrossRef]
- Nicoara, A.D.; Alexandrescu, L.; Tofolean, D.E.; Iliescu, M.G.; Condur, L.M.; Tofolean, I.T. The Impact of Cardiac Rehabilitation On Quality Of Life In Elderly Heart Failure Patients-Literature Review. Balneo PRM Res. J. 2024, 15, 723. [Google Scholar] [CrossRef]
- Hu, F.B. Globalization of diabetes: The role of diet, lifestyle, and genes. Diabetes Care. 2011, 34, 1249–1257. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sami, W.; Ansari, T.; Butt, N.S.; Hamid, M.R.A. Effect of diet on type 2 diabetes mellitus: A review. Int. J. Health Sci. 2017, 11, 65–71. [Google Scholar] [PubMed] [PubMed Central]
- 2aviz, K.I.; Narayan, K.M.V.; Lobelo, F.; Weber, M.B. Lifestyle and the Prevention of Type 2 Diabetes: A Status Report. Am. J. Lifestyle Med. 2015, 12, 4–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- The Diabetes and Nutrition Study Group (D.N.S.G.) of the European Association for the Study of Diabetes (E.A.S.D.). Evidence-based European recommendations for the dietary management of diabetes. Diabetologia 2023, 66, 965–985. [Google Scholar] [CrossRef]
- Manoogian, E.N.C.; Zadourian, A.; Lo, H.C.; Gutierrez, N.R.; Shoghi, A.; Rosander, A.; Pazargadi, A.; Ormiston, C.K.; Wang, X.; Sui, J.; et al. Feasibility of time-restricted eating and impacts on cardiometabolic health in 24-h shift workers: The Healthy Heroes randomized control trial. Cell Metab. 2022, 34, 1442–1456.e7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Efrem, I.C.; Moța, M.; Vladu, I.M.; Mitrea, A.; Clenciu, D.; Timofticiuc, D.C.P.; Diaconu, I.D.; Turcu, A.; Crișan, A.E.; Geormăneanu, C.; et al. A Study of Biomarkers Associated with Metabolic Dysfunction-Associated Fatty Liver Disease in Patients with Type 2 Diabetes. Diagnostics 2022, 12, 2426. [Google Scholar] [CrossRef] [PubMed]
- Alexescu, T.G.; Bordea, I.R.; Cozma, A.; Rajnoveanu, R.; Buzioanu, A.D.; Nemes, R.M.; Tudorache, S.I.; Boca, B.M.; Todea, D.A. Metabolic Profile and risk of early Atherosclerosis in Patients with Obesity and Overweight. Rev. Chim. 2019, 70, 3627–3633. [Google Scholar]
- Shechter, A.; Foster, G.D.; Lang, W.; Reboussin, D.M.; St-Onge, M.P.; Zammit, G.; Newman, A.B.; Millman, R.P.; Wadden, T.A.; Jakicic, J.M.; et al. Effects of a lifestyle intervention on R.E.M. sleep-related O.S.A. severity in obese individuals with type 2 diabetes. J. Sleep Res. 2017, 26, 747–755. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hawkins, M.; Marcus, B.; Pekow, P.; Rosal, M.C.; Tucker, K.L.; Spencer, R.M.C.; Chasan-Taber, L. The Impact of a Randomized Controlled Trial of a Lifestyle Intervention on Sleep Among Latina Postpartum Women. Ann. Behav. Med. 2021, 55, 892–903. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nicolae, M.; Mihai, C.M.; Chisnoiu, T.; Balasa, A.L.; Frecus, C.E.; Mihai, L.; Lupu, V.V.; Ion, I.; Pantazi, A.C.; Nelson Twakor, A.; et al. Immunomodulatory Effects of Vitamin D in Respiratory Tract Infections and COVID-19 in Children. Nutrients 2023, 15, 3430. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Diabetes Prevention Program Research Group. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: The Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015, 3, 866–875. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, L.; Zhang, Y.; Shen, S.; Wang, X.; Dong, L.; Li, Q.; Ren, W.; Li, Y.; Bai, J.; Gong, Q.; et al. Safety and effectiveness of metformin plus lifestyle intervention compared with lifestyle intervention alone in preventing progression to diabetes in a Chinese population with impaired glucose regulation: A multicentre, open-label, randomized controlled trial. Lancet Diabetes Endocrinol. 2023, 11, 567–577, Erratum in: Lancet Diabetes Endocrinol. 2023, 11, e13. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Celli, A.; Barnouin, Y.; Jiang, B.; Blevins, D.; Colleluori, G.; Mediwala, S.; Armamento-Villareal, R.; Qualls, C.; Villareal, D.T. Lifestyle Intervention Strategy to Treat Diabetes in Older Adults: A Randomized Controlled Trial. Diabetes Care. 2022, 45, 1943–1952. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Courcoulas, A.P.; Gallagher, J.W.; Neiberg, R.H.; Eagleton, E.B.; DeLany, J.P.; Lang, W.; Punchai, S.; Gourash, W.; Jakicic, J.M. Bariatric Surgery vs Lifestyle Intervention for Diabetes Treatment: 5-Year Outcomes From a Randomized Trial. J. Clin. Endocrinol. Metab. 2020, 105, 866–876. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Johansen, M.Y.; MacDonald, C.S.; Hansen, K.B.; Karstoft, K.; Christensen, R.; Pedersen, M.; Hansen, L.S.; Zacho, M.; Wedell-Neergaard, A.S.; Nielsen, S.T.; et al. Effect of an Intensive Lifestyle Intervention on Glycemic Control in Patients With Type 2 Diabetes: A Randomized Clinical Trial. JAMA 2017, 318, 637–646. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ghavami, H.; Radfar, M.; Soheily, S.; Shamsi, S.A.; Khalkhali, H.R. Effect of lifestyle interventions on diabetic peripheral neuropathy in patients with type 2 diabetes, the result of a randomized clinical trial. Agri 2018, 30, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Snehalatha, C.; Mary, S.; Mukesh, B.; Bhaskar, A.D.; Vijay, V.; Indian Diabetes Prevention Programme (I.D.P.P.). The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 2006, 49, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.; Khoo, J.; Gani, L.U.; Malakar, R.D.; Tay, T.L.; Tirukonda, P.S.; Kam, J.W.; Tin, A.S.; Tang, T.Y. Effect of multidisciplinary intensive targeted care in improving diabetes mellitus outcomes: A randomized controlled pilot study—The Integrated Diabetes Education, Awareness and Lifestyle modification in Singapore (IDEALS) Program. Trials 2019, 20, 549. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dambha-Miller, H.; Day, A.J.; Strelitz, J.; Irving, G.; Griffin, S.J. Behaviour change, weight loss and remission of Type 2 diabetes: A community-based prospective cohort study. Diabet. Med. 2020, 37, 681–688. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kanaley, J.A.; Colberg, S.R.; Corcoran, M.H.; Malin, S.K.; Rodriguez, N.R.; Crespo, C.J.; Kirwan, J.P.; Zierath, J.R. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine. Med. Sci. Sports Exerc. 2022, 54, 353–368. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Syrjälä, M.B.; Bennet, L.; Dempsey, P.C.; Fharm, E.; Hellgren, M.; Jansson, S.; Nilsson, S.; Nordendahl, M.; Rolandsson, O.; Rådholm, K.; et al. Health effects of reduced occupational sedentary behaviour in type 2 diabetes using a mobile health intervention: A study protocol for a 12-month randomized controlled trial-the ROSEBUD study. Trials 2022, 23, 607. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Whitaker, K.M.; Pettee Gabriel, K.; Buman, M.P.; Pereira, M.A.; Jacobs DRJr Reis, J.P.; Gibbs, B.B.; Carnethon, M.R.; Staudenmayer, J.; Sidney, S.; Sternfeld, B. Associations of Accelerometer-Measured Sedentary Time and Physical Activity With Prospectively Assessed Cardiometabolic Risk Factors: The CARDIA Study. J. Am. Heart Assoc. 2019, 8, e010212. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zheng, C.; Tian, X.Y.; Sun, F.H.; Huang, W.Y.; Sheridan, S.; Wu, Y.; Wong, S.H. Associations of Sedentary Patterns with Cardiometabolic Biomarkers in Physically Active Young Males. Med. Sci. Sports Exerc. 2021, 53, 838–844. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Debache, I.; Bergouignan, A.; Chaix, B.; Sneekes, E.M.; Thomas, F.; Sueur, C. Associations of Sensor-Derived Physical Behavior with Metabolic Health: A Compositional Analysis in the Record Multisensor Study. Int. J. Environ. Res. Public Health 2019, 16, 741. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Honda, T.; Kishimoto, H.; Mukai, N.; Hata, J.; Yoshida, D.; Hirakawa, Y.; Shibata, M.; Ohara, T.; Kumagai, S.; Ninomiya, T. Objectively measured sedentary time and diabetes mellitus in a general Japanese population: The Hisayama Study. J. Diabetes Investig. 2019, 10, 809–816. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mossavar-Rahmani, Y.; Hua, S.; Qi, Q.; Strizich, G.; Sotres-Alvarez, D.; Talavera, G.A.; Evenson, K.R.; Gellman, M.D.; Stoutenberg, M.; Castañeda, S.F.; et al. Are sedentary behavior and physical activity independently associated with cardiometabolic benefits? The Hispanic Community Health Study/Study of Latinos. B.M.C. Public Health 2020, 20, 1400. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Banitalebi, E.; Kazemi, A.; Faramarzi, M.; Nasiri, S.; Haghighi, M.M. Effects of sprint interval or combined aerobic and resistance training on myokines in overweight women with type 2 diabetes: A randomized controlled trial. Life Sci. 2019, 217, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Gallardo-Gómez, D.; Salazar-Martínez, E.; Alfonso-Rosa, R.M.; Ramos-Munell, J.; Del Pozo-Cruz, J.; Del Pozo Cruz, B.; Álvarez-Barbosa, F. Optimal Dose and Type of Physical Activity to Improve Glycemic Control in People Diagnosed With Type 2 Diabetes: A Systematic Review and Meta-analysis. Diabetes Care. 2024, 47, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.; Sousa, N.; Themudo-Barata, J.L.; Reis, V.M. High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Middle-Aged and Older Patients with Type 2 Diabetes: A Randomized Controlled Crossover Trial of the Acute Effects of Treadmill Walking on Glycemic Control. Int. J. Environ. Res. Public Health 2019, 16, 4163. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, J.X.; Zhu, L.; Li, P.J.; Li, N.; Xu, Y.B. Effectiveness of high-intensity interval training on glycemic control and cardiorespiratory fitness in patients with type 2 diabetes: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2019, 31, 575–593. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shamizadeh, T.; Jahangiry, L.; Sarbakhsh, P.; Ponnet, K. Social cognitive theory-based intervention to promote physical activity among prediabetic rural people: A cluster randomized controlled trial. Trials 2019, 20, 98. [Google Scholar] [CrossRef]
- Afonso, J.; Ramirez-Campillo, R.; Clemente, F.M.; Büttner, F.C.; Andrade, R. The Perils of Misinterpreting and Misusing “Publication Bias” in Meta-analyses: An Education Review on Funnel Plot-Based Methods. Sports Med. 2024, 54, 257–269. [Google Scholar] [CrossRef]
- Dettori, J.R.; Norvell, D.C.; Chapman, J.R. Seeing the Forest by Looking at the Trees: How to Interpret a Meta-Analysis Forest Plot. Glob. Spine J. 2021, 11, 614–616. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marfo, P.; Okyere, G.A. The accuracy of effect-size estimates under normals and contaminated normals in meta-analysis. Heliyon 2019, 5, e01838. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Panjeh, S.; Nordahl-Hansen, A.; Cogo-Moreira, H. Establishing new cutoffs for Cohen’s d: An application using known effect sizes from trials for improving sleep quality on composite mental health. Int. J. Methods Psychiatr. Res. 2023, 32, e1969. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Taylor, J.M.; Alanazi, S. Cohen’s and Hedges’ g. J. Nurs. Educ. 2023, 62, 316–317. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Aloe, A.M. Evaluation of various estimators for standardized mean difference in meta-analysis. Stat. Med. 2021, 40, 403–426. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.P.L.; Edwards, H.; Do, T.N.D.; Finlayson, K. Effectiveness of a theory-based foot care education program (3STEPFUN) in improving foot self-care behaviours and foot risk factors for ulceration in people with type 2 diabetes. Diabetes Res. Clin. Pract. 2019, 152, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Patti, A.M.; Rizvi, A.A.; Giglio, R.V.; Stoian, A.P.; Ligi, D.; Mannello, F. Impact of Glucose-Lowering Medications on Cardiovascular and Metabolic Risk in Type 2 Diabetes. J. Clin. Med. 2020, 9, 912. [Google Scholar] [CrossRef]
- Barnard, N.D.; Cohen, J.; Jenkins, D.J.; Turner-McGrievy, G.; Gloede, L.; Jaster, B.; Seidl, K.; Green, A.A.; Talpers, S. A low-fat vegan diet improves glycemic control and cardiovascular risk factors in a randomized clinical trial in individuals with type 2 diabetes. Diabetes Care. 2006, 29, 1777–1783. [Google Scholar] [CrossRef] [PubMed]
- Borba, A.K.O.T.; Arruda, I.K.G.; Marques, A.P.O.; Leal, M.C.C.; Diniz, A.D.S. Knowledge and attitude about diabetes self-care of older adults in primary health care. Cien Saude Colet. 2019, 24, 125–136, (In Portuguese; In English). [Google Scholar] [CrossRef] [PubMed]
- Mesarwi, O.; Polak, J.; Jun, J.; Polotsky, V.Y. Sleep disorders and the development of insulin resistance and obesity. Endocrinol. Metab. Clin. N. Am. 2013, 42, 617–634. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Munteanu, I.; Marc, M.; Gheorghevici, C.; Diaconu, G.A.; Feraru, N.; Sion, D.; Nemes, R.M.; Mahler, B. Sleep Quality Aspects in Post-COVID-19 Patients. J. Pers. Med. 2023, 13, 1125. [Google Scholar] [CrossRef] [PubMed]
- Anca, P.S.; Toth, P.P.; Kempler, P.; Rizzo, M. Gender differences in the battle against COVID-19: Impact of genetics, comorbidities, inflammation and lifestyle on differences in outcomes. Int. J. Clin. Pract. 2021, 75, e13666. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, D.; Jenkins, A.J.; Greenlaw, N.; Dudman, K.; Fernandes, T.; Carty, D.M.; Hughes, A.D.; Januszewski, A.S.; Stehouwer, C.D.; Petrie, J.R. Cardiometabolic risk factors, peripheral arterial tonometry and metformin in adults with type 1 diabetes participating in the REducing with MetfOrmin Vascular Adverse Lesions trial. Diab. Vasc. Dis. Res. 2023, 20, 14791641231183634. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Crofford, O.B. Diabetes control and complications. Annu. Rev. Med. 1995, 46, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Pippi, R.; Mascherini, G.; Izzicupo, P.; Bini, V.; Fanelli, C.G. Effects of a Mixed Exercise Program on Overweight and Obese Children and Adolescents: A Pilot, Uncontrolled Study. Int. J. Environ. Res. Public Health 2022, 19, 9258. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maranna, H.; Lal, P.; Mishra, A.; Bains, L.; Sawant, G.; Bhatia, R.; Kumar, P.; Beg, M.Y. Negative pressure wound therapy in grade 1 and 2 diabetic foot ulcers: A randomized controlled study. Diabetes Metab. Syndr. 2021, 15, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Atila, C.; Holze, F.; Murugesu, R.; Rommers, N.; Hutter, N.; Varghese, N.; Sailer, C.O.; Eckert, A.; Heinrichs, M.; Liechti, M.E.; et al. Oxytocin in response to MDMA provocation test in patients with arginine vasopressin deficiency (central diabetes insipidus): A single-centre, case-control study with nested, randomized, double-blind, placebo-controlled crossover trial. Lancet Diabetes Endocrinol. 2023, 11, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, G.; Cucinotta, D. The late complications of diabetes mellitus. Ann. Ital. Med. Int. 1991, 6 Pt 2, 126–136. [Google Scholar] [PubMed]
- Diepersloot, R.J.; Bouter, K.P.; Hoekstra, J.B. Influenza infection and diabetes mellitus. Case for annual vaccination. Diabetes Care 1990, 13, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Boulton, A.J. D.C.C.T.: Implications for diabetes care in the UK. Diabet. Med. 1993, 10, 687. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, J. Diabetes: The science and the art. Hyperglycemia v Complications. Arch. Intern. Med. 1983, 143, 1118–1119. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, E.; Beheshtirouy, S.; Aghamohammadzadeh, N.; Ghaffary, S.; Sarbakhsh, P.; Shaseb, E. Management of diabetic neuropathy with memantine: A randomized clinical trial. Diab Vasc. Dis. Res. 2023, 20, 14791641231191093. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mindrescu, N.M.; Guja, C.; Jinga, V.; Ispas, S.; Curici, A.; Nelson Twakor, A.; Pantea Stoian, A.M. Interactions between Gut Microbiota and Oral Antihyperglycemic Drugs: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 3540. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ispas, S.; Tuta, L.A.; Botnarciuc, M.; Ispas, V.; Staicovici, S.; Ali, S.; Nelson-Twakor, A.; Cojocaru, C.; Herlo, A.; Petcu, A. Metabolic Disorders, the Microbiome as an Endocrine Organ, and Their Relations with Obesity: A Literature Review. J. Pers. Med. 2023, 13, 1602. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Keen, H. The Diabetes Control and Complications Trial (D.C.C.T.). Health Trends. 1994, 26, 41–43. [Google Scholar] [PubMed]
- Fernando, D.J. Knowledge about diabetes and metabolic control in diabetic patients. Ceylon Med. J. 1993, 38, 18–21. [Google Scholar] [PubMed]
- Furrer, R.; Hawley, J.A.; Handschin, C. The molecular athlete: Exercise physiology from mechanisms to medals. Physiol. Rev. 2023, 103, 1693–1787. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Leibold, N. The Effect of a School Nurse Led Education Intervention on Blood Pressure and Physical Activity Levels in Adolescents. Ph.D. Thesis, College of Saint Mary, Moraga, CA, USA, March 2009. [Google Scholar]
- Motoc, N.Ș.; Man, M.A.; Tudorache, S.I.; Rusu, E.; Brailescu, C.M.; Mahler-Boca, B.; Campean, A.U.; Pop, C.M. The Importance of Mask Type and Mask Materials in Sleep Apnea Patients. Rev Chim. 2019, 70, 3273–3276. [Google Scholar] [CrossRef]
- Rizvi, A.A.; Stoian, A.P.; Rizzo, M. Metabolic Syndrome: From Molecular Mechanisms to Novel Therapies. Int. J. Mol. Sci. 2021, 22, 10038. [Google Scholar] [CrossRef]
- Sathish, T.; MacMillan, F. Prevention of Type 2 Diabetes with Lifestyle Interventions: Evidence vs. Reality. Diabetology 2023, 4, 427–429. [Google Scholar] [CrossRef]
- Bassin, S.R.; Srinath, R. The Impact of Physical Activity in Patients With Type 2 Diabetes. Am. J. Lifestyle Med. 2023, 19, 147–161. [Google Scholar] [CrossRef] [PubMed]
- Amanat, S.; Ghahri, S.; Dianatinasab, A.; Fararouei, M.; Dianatinasab, M. Exercise and Type 2 Diabetes. Adv. Exp. Med. Biol. 2020, 1228, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Cannata, F.; Vadalà, G.; Russo, F.; Papalia, R.; Napoli, N.; Pozzilli, P. Beneficial Effects of Physical Activity in Diabetic Patients. J. Funct. Morphol. Kinesiol. 2020, 5, 70. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Keadle, S.K.; Conroy, D.E.; Buman, M.P.; Dunstan, D.W.; Matthews, C.E. Targeting Reductions in Sitting Time to Increase Physical Activity and Improve Health. Med. Sci. Sports Exerc. 2017, 49, 1572–1582. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Sedentary behavior as a mediator of type 2 diabetes. Med. Sport. Sci. 2014, 60, 11–26. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lorenzo, C.; Hartnett, S.; Hanley, A.J.; Rewers, M.J.; Wagenknecht, L.E.; Karter, A.J.; Haffner, S.M. Impaired fasting glucose and impaired glucose tolerance have distinct lipoprotein and apolipoprotein changes: The insulin resistance atherosclerosis study. J. Clin. Endocrinol. Metab. 2013, 98, 1622–1630. [Google Scholar] [CrossRef]
- Suceveanu, A.I.; Mazilu, L.; Katsiki, N.; Parepa, I.; Voinea, F.; Pantea-Stoian, A.; Rizzo, M.; Botea, F.; Herlea, V.; Serban, D.; et al. NLRP3 Inflammasome Biomarker—Could Be the New Tool for Improved Cardiometabolic Syndrome Outcome. Metabolites 2020, 10, 448. [Google Scholar] [CrossRef]
- Kirwan, J.P.; Sacks, J.; Nieuwoudt, S. The essential role of exercise in the management of type 2 diabetes. Cleve Clin. J. Med. 2017, 84 (Suppl. S1), S15–S21. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Delevatti, R.S.; Kanitz, A.C.; Alberton, C.L.; Marson, E.C.; Lisboa, S.C.; Pinho, C.D.; Lovatel, G.A.; Korb, A.; Bertoldi, K.; Macedo, R.C.; et al. Glucose control can be similarly improved after aquatic or dry-land aerobic training in patients with type 2 diabetes: A randomized clinical trial. J. Sci. Med. Sport 2016, 19, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Summaries for patients. Effects of aerobic training, resistance training, or both on control of blood sugar in type 2 diabetes. Ann. Intern. Med. 2007, 147, I16. [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes—2021. Diabetes Care 2021, 44 (Suppl. S1), S151–S167. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.; Braun, B. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Owen, N. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Kirk, A.; Barnett, J.; Mutrie, N. Physical activity consultation for people with Type 2 diabetes: Evidence and guidelines. Diabet. Med. 2007, 24, 857–864. [Google Scholar] [CrossRef]
- Sigal, R.J.; Armstrong, M.J.; Colby, P.; Kenny, G.P.; Plotnikoff, R.C.; Reichert, S.M.; Riddell, M.C. Physical activity and diabetes. Can. J. Diabet. 2018, 42, S54–S63. [Google Scholar] [CrossRef]
- Umpierre, D.; Ribeiro, P.A.B.; Kramer, C.K.; Leitão, C.B.; Zucatti, A.T.N.; Azevedo, M.J.; Gross, J.L.; Ribeiro, J.P.; Schaan, B.D. Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: A systematic review and meta-analysis. JAMA 2011, 305, 1790–1799. [Google Scholar] [CrossRef]
- Rizvi, A.A.; Kathuria, A.; Al Mahmeed, W.; Al-Rasadi, K.; Al-Alawi, K.; Banach, M.; Banerjee, Y.; Ceriello, A.; Cesur, M.; Cosentino, F.; et al. Post-COVID syndrome, inflammation, and diabetes. J. Diabetes Complicat. 2022, 36, 108336. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Corina, A.; Abrudan, M.B.; Nikolic, D.; Cătoi, A.F.; Chianetta, R.; Castellino, G.; Citarrella, R.; Stoian, A.P.; Pérez-Martínez, P.; Rizzo, M. Effects of Aging and Diet on Cardioprotection and Cardiometabolic Risk Markers. Curr. Pharm. Des. 2019, 25, 3704–3714. [Google Scholar] [CrossRef] [PubMed]
- Pantea, S.A.; Andronache, L.; Hainarosie, R.; Păduraru, D.; Badiu, C.; Arsene, A.; Mehedintu, C.; Ditu, G.; Pițuru, S.M.; Orlov, C.; et al. Dietary habits and lifestyle in school-aged children from Bucharest, Romania. J. Mind Med. Sciences. 2018, 5, 85–92. [Google Scholar]
- Reurean-Pintilei, D.; Potcovaru, C.-G.; Salmen, T.; Mititelu-Tartau, L.; Cinteză, D.; Lazăr, S.; Pantea Stoian, A.; Timar, R.; Timar, B. Assessment of Cardiovascular Risk Categories and Achievement of Therapeutic Targets in European Patients with Type 2 Diabetes. J. Clin. Med. 2024, 13, 2196. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | FBG * Means at Baseline | SD ** at Baseline | Participants at Baseline | FBG After Intervention | SD After Intervention | Participants After Intervention |
|---|---|---|---|---|---|---|---|
| Whitaker et al. [28] | 2019 | 95 | 12.6 | 1922 | 94.6 | 14 | 1922 |
| Zheng et al. [29] | 2020 | 106 | 5.4 | 94 | 86.3 | 2.1 | 94 |
| Debache et al. [30] | 2019 | 96. 9 | 11.4 | 131 | 74.84 | 37.74 | 131 |
| Banitalebi et al. (SIT ***) [33] | 2019 | 210.07 | 32.91 | 14 | 137.36 | 32.95 | 14 |
| Banitalebi et al. (A + R ****) [33] | 2019 | 214.64 | 27.67 | 14 | 163.86 | 71.47 | 14 |
| Mendes et al. H.I.I.T. ***** [35] | 2019 | 112.67 | 21.98 | 15 | 110.5 | 17.73 | 15 |
| Shamizadeh et al. [37] | 2020 | 108.4 | 6.1 | 136 | 99.4 | 8.1 | 136 |
| Quartile | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Quartile 1 | 0.13 (0.11, 0.15) | 0.13 (0.10, 0.15) | 0.13 (0.11, 0.16) |
| Quartile 2 | 0.14 (0.12, 0.16) | 0.14 (0.12, 0.16) | 0.14 (0.12, 0.16) |
| Quartile 3 | 0.16 (0.13, 0.18) | 0.16 (0.14, 0.19) | 0.16 (0.14, 0.19) |
| Quartile 4 | 0.17 (0.14, 0.19) | 0.16 (0.14, 0.19) | 0.16 (0.14, 0.19) |
| p-value | 0.02 | 0.02 | 0.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ispas, S.; Nelson Twakor, A.; Mindrescu, N.M.; Ispas, V.; Tofolean, D.E.; Mercore Hutanu, E.; Petcu, A.; Deacu, S.; Iordache, I.E.; Bica, C.I.; et al. From Sedentary to Success: How Physical Activity Transforms Diabetes Management: A Systematic Review. J. Mind Med. Sci. 2025, 12, 10. https://doi.org/10.3390/jmms12010010
Ispas S, Nelson Twakor A, Mindrescu NM, Ispas V, Tofolean DE, Mercore Hutanu E, Petcu A, Deacu S, Iordache IE, Bica CI, et al. From Sedentary to Success: How Physical Activity Transforms Diabetes Management: A Systematic Review. Journal of Mind and Medical Sciences. 2025; 12(1):10. https://doi.org/10.3390/jmms12010010
Chicago/Turabian StyleIspas, Sorina, Andreea Nelson Twakor, Nicoleta Mihaela Mindrescu, Viorel Ispas, Doina Ecaterina Tofolean, Emanuela Mercore Hutanu, Adina Petcu, Sorin Deacu, Ionut Eduard Iordache, Cristina Ioana Bica, and et al. 2025. "From Sedentary to Success: How Physical Activity Transforms Diabetes Management: A Systematic Review" Journal of Mind and Medical Sciences 12, no. 1: 10. https://doi.org/10.3390/jmms12010010
APA StyleIspas, S., Nelson Twakor, A., Mindrescu, N. M., Ispas, V., Tofolean, D. E., Mercore Hutanu, E., Petcu, A., Deacu, S., Iordache, I. E., Bica, C. I., Petcu, L. C., Gherghiceanu, F., Popoviciu, M. S., & Pantea Stoian, A. (2025). From Sedentary to Success: How Physical Activity Transforms Diabetes Management: A Systematic Review. Journal of Mind and Medical Sciences, 12(1), 10. https://doi.org/10.3390/jmms12010010