2.1. Simulation Data
We retrospectively identified and retrieved studies from the local PACS system (IDS7, Sectra AB, Linköping, Sweden) at the Department of Radiology & Nuclear Medicine, Hospital of Southwest Jutland, according to the criteria below. All patient-sensitive information was removed before further processing. Images were acquired on Dual-Source cardiac CT scanners (Somatom FLASH or FORCE, Siemens Healthineers, Erlangen, Germany) between October 2009 and January 2021.
The inclusion criteria were as follows:
Helical CCTAs performed without ECG-based dose reduction, including ED and ES phases.
Maximum phase interval equal to or less than 10% of the cardiac cycle.
The exclusion criteria were as follows:
LV contrast attenuation below 250 HU, defined as minimally acceptable by SCCT guidelines [
13]. ROI measurement was performed on a single axial slice in the ED phase, midway between the mitral valve and apex.
Severe cardiac motion or respiratory artefacts with distortion of endocardial contours.
Metal implant artefacts, e.g., from pacemaker leads, metallic aortic valves, or thoracic spine implants.
Excessive noise. Studies were excluded if the PACS report noted compromised image quality related to noise. Otherwise, the study was evaluated subjectively by the first author, who has over 17 years of experience in cardiac CT.
Failure to reliably identify ED and ES phases in the time–volume curves as clearly distinguishable maximum and minimum volumes.
Slice thickness and increment were 0.6/0.4 mm, and images were reconstructed at kernel Br32 or Bv40 with an Advanced Model-Based Iterative Reconstruction (ADMIRE) level of 3 and 5, respectively.
2.2. Optimisation of Simulation Parameters
All image processing was performed in MATLAB R2021a (MathWorks Inc., Natick, MA, USA). Furthermore, the “TIGRE” plugin was installed [
14], in which a function called “addCTnoise” can insert realistic Poisson noise in the sinogram domain by controlling a “photon flux” parameter, linearly correlated with dose. Using retrospective studies, for which raw data were not available, this required transforming images to sinogram space using the Radon transform (native to MATLAB image processing toolbox). Processing was performed on a standard desktop PC with a 3.2 GHz processor, 16 GB RAM and an Nvidia Geforce 1050Ti 4 GB GPU.
We followed the approach demonstrated by Pelt and Batenburg [
15] of approximating iterative reconstructions with filtered backprojection (FBP) to keep computational load and reconstruction time within reasonable limits, as each dataset consisted of approximately 2500 to 4000 images. Instead of deriving customised filter functions, we used iterative testing of native reconstruction parameters to determine the combinations yielding the highest correspondence
We used an anatomically and radiologically accurate 3D-printed heart phantom with contrast-filled left heart chambers. The production and validation of using the phantom for automated LVEF measurements was described in a previous paper [
16]. This phantom was placed inside an anthropomorphic chest phantom (LungMan N1, Kyoto Kagaku, Kyoto, Japan), and a series of scans were performed on a Siemens Somatom FORCE CT scanner (Siemens Healthineers, Forchheim, Germany). Using a synthetic ECG at 60 BPM, Dual Source, retrospectively gated helical was performed at 13 dose levels, with scan and reconstruction parameters listed in
Table 1.
The two kernels were identical to those encountered in the clinical dataset.
All possible combinations of parameters listed in
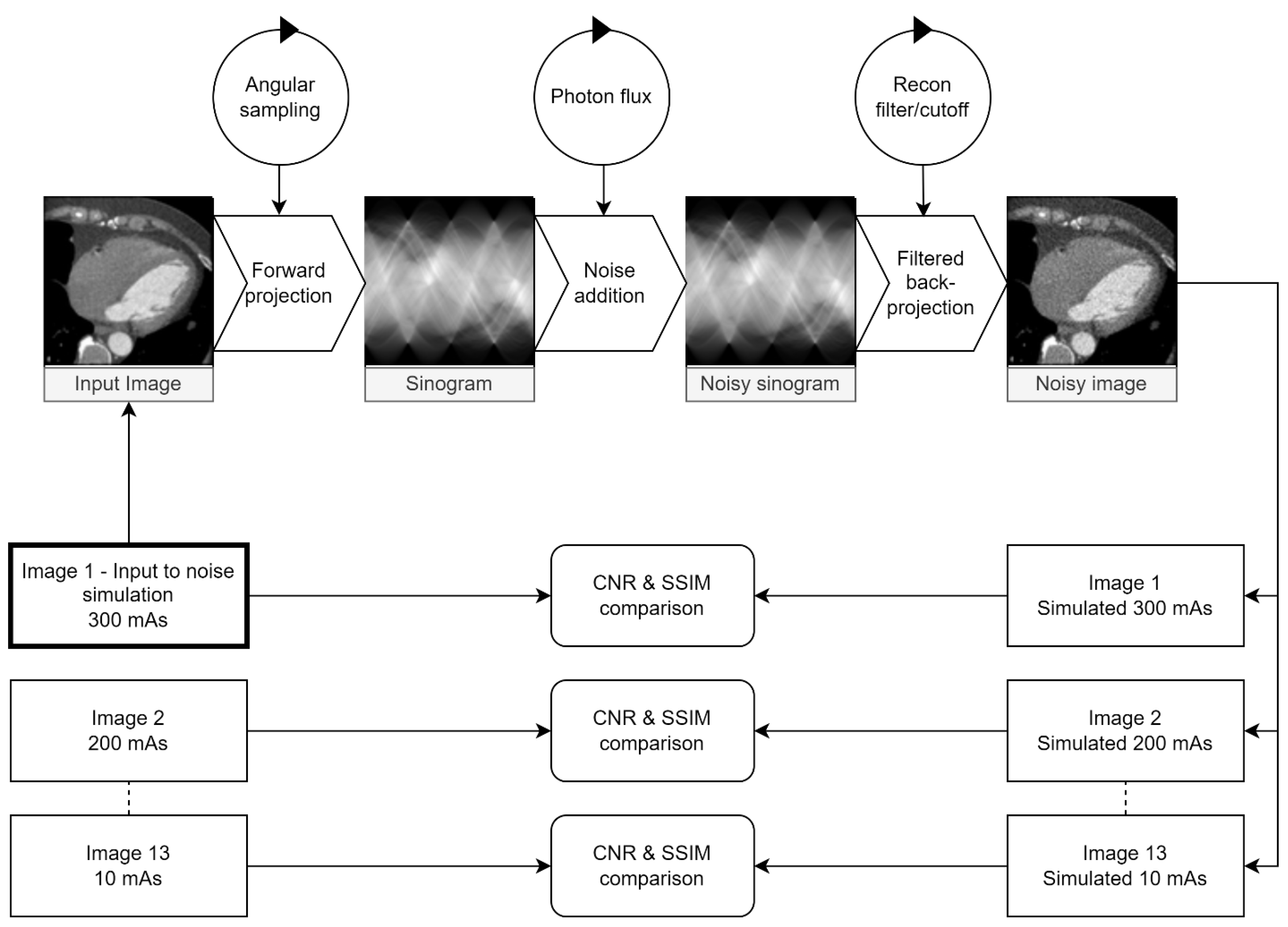
Table 2 were tested. For each parameter combination, the full-dose (300 mAs) image was used as the simulation input for 13 simulated dose-reduction images corresponding to the physically dose-reduced images. Images were transformed to sinogram space at differing angular resolutions, sampled over 180 degrees. For each simulated dose level, the maximum photon flux value was multiplied by the relative dose reduction, e.g., 20 mAs/300 mAs = 0.07 for the simulated 20 mAs images for a simulated dose reduction to 7% of the original value. After noise insertion, the images were reconstructed with FPB with a combination of reconstruction filter and associated cutoff frequency. All real/simulated image pairs were compared using the metrics described below. The entire process is visualised in
Figure 1.
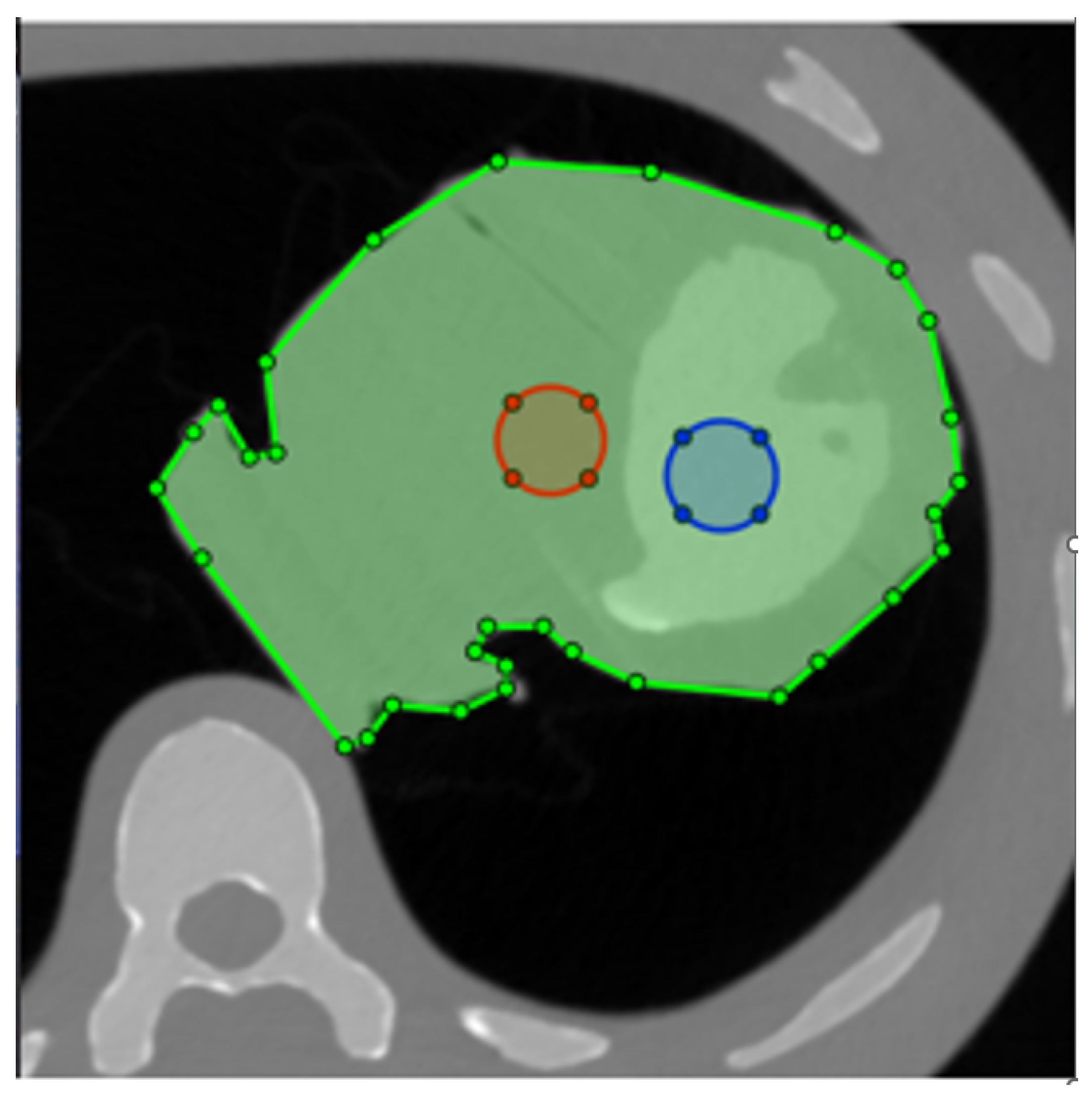
As LV-to-myocardium differentiation relies on differences in Hounsfield Units (HU) between myocardium and contrast, we calculated the CNR between the phantom LV cavity and the myocardium, whereby two circular ROIs with a diameter of 2 cm were drawn in the phantom LV cavity and “myocardium” as shown in
Figure 2. Myocardium-to-LV CNR was calculated as shown in Equation (
1) [
17]. For the non-simulated images, these values were, of course, constant within the same dose level. The ROIs were automatically propagated to all tested images, eliminating placement variability.
Figure 1.
Visualisation of the testing loop used to identify parameters for the maximum similarity between the real and simulated images. Circles represent parameters adjusted at each step. The maximum dose (300 mAs) image was used as input for 13 simulated dose levels for each parameter combination. The contrast-to-noise ratio (CNR) between the myocardium and LV cavity and the SSIM between real and simulated images were calculated and compared for each dose level.
Figure 1.
Visualisation of the testing loop used to identify parameters for the maximum similarity between the real and simulated images. Circles represent parameters adjusted at each step. The maximum dose (300 mAs) image was used as input for 13 simulated dose levels for each parameter combination. The contrast-to-noise ratio (CNR) between the myocardium and LV cavity and the SSIM between real and simulated images were calculated and compared for each dose level.
Figure 2.
Placement of the two ROIs for contrast-to-noise ratio (CNR) calculation. The phantom is masked with the green ROI, ensuring that the structural similarity index (SSIM) is only calculated for the heart. Blue and red circles are the ROIs used to measure attenuation and noise in the LV and myocardium, respectively.
Figure 2.
Placement of the two ROIs for contrast-to-noise ratio (CNR) calculation. The phantom is masked with the green ROI, ensuring that the structural similarity index (SSIM) is only calculated for the heart. Blue and red circles are the ROIs used to measure attenuation and noise in the LV and myocardium, respectively.
For each tested parameter combination, linear regression was performed for all 13 dose levels between CNR in the real and simulated images. The slope and R2 value were calculated in each case. A slope of one is not necessarily predictive of CNR similarity if individual measurements are scattered about the prediction line, resulting in low R2. Likewise, a perfect R2 of one but a slope significantly different from one would mean systematic over- or underestimation of simulated CNR.
To optimise noise structure similarity, we calculated the structural similarity index (SSIM) [
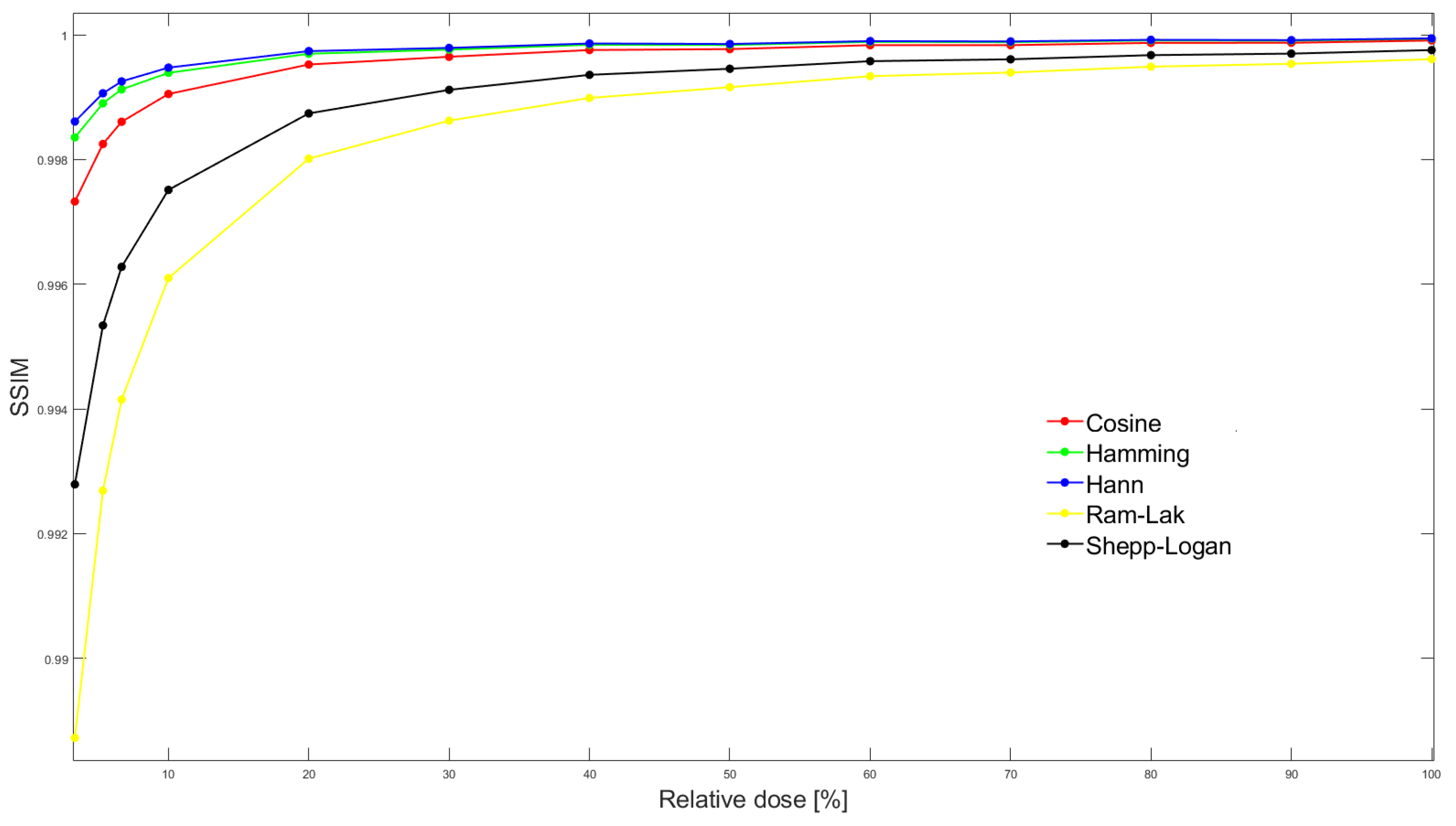
18] between all pairs of real/simulated images. Using trapezoidal integration, the area under the SSIM vs. relative dose curve (AUC
SSIM) was calculated for each parameter combination (
Figure 3). We masked the phantom contours with a polygonal ROI and thereby excluded other phantom tissue from SSIM calculation (
Figure 2).
Due to the high (16-bit) dynamic range inherent in CT images, the SSIM differences are minimal but nevertheless significant. To bring all values to the same scale, slope and coefficient of determination (R
2) from CNR linear regression of simulated vs. real dose-reduced images and AUC
SSIM were normalised to a scale from zero to one. A measure of deviation between real and simulated images was defined from these three metrics. This was defined as the vector length (norm) of the three components. It is shown in Equation (
2), where the subscript “norm” indicates normalised values.
By finding the minimum of this vector for all parameter combinations tested, the combination of parameters giving the smallest deviation across all three metrics could be located.
Figure 3.
SSIM between simulated and real exposure images at all 13 dose levels. In this particular case, stratified by reconstruction filter, but for fixed values of sampling interval (0.6 degrees), default photon flux (105) and filter frequency cutoff (80%).The area under the SSIM vs dose curve (AUCSSIM) is then calculated by integrating SSIM over the entire dose range for each parameter combination.
Figure 3.
SSIM between simulated and real exposure images at all 13 dose levels. In this particular case, stratified by reconstruction filter, but for fixed values of sampling interval (0.6 degrees), default photon flux (105) and filter frequency cutoff (80%).The area under the SSIM vs dose curve (AUCSSIM) is then calculated by integrating SSIM over the entire dose range for each parameter combination.
2.3. Image Processing
A MATLAB R2021a script was used to batch-process all images by slice position and cardiac phase.
The baseline noise level varied from study to study. Therefore, the 100% photon flux level was identified individually by testing 200 initial values between 103 and 107. A circular ROI was drawn in the LV cavity, avoiding PM, while a polygonal ROI was drawn on the lateral myocardium, avoiding visible coronaries. The image was then processed at all 200 initial flux values. ROI SD was measured automatically at all levels, and noise from the corresponding image without noise insertion was subtracted. The data were smoothed using a Gaussian kernel and the minimal difference for each ROI was automatically identified. The mean of the corresponding flux values was then passed to the noise insertion algorithm, and the study reconstructed at five dose levels: 100, 25, 10, 5 and 2% relative dose.
Using a sliding average, output images were reconstructed at 1.0/0.8 mm images and a matrix size of 256 × 256 pixels. This combination has been demonstrated as a good compromise between data volume and volume measurement accuracy [
5].









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}