

Recognition of Facial Emotion Expressions in Patients with Depressive Disorders: A Functional MRI Study

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethics Approval
2.3. Data Acquisition and Analyses
2.3.1. Functional MRI Protocol
2.3.2. Emotion Recognition Task
2.3.3. fMRI Data Processing
2.4. Statistical Analysis
3. Results
3.1. Brain Activation Patterns in Depressive Patients before Treatment (Background)
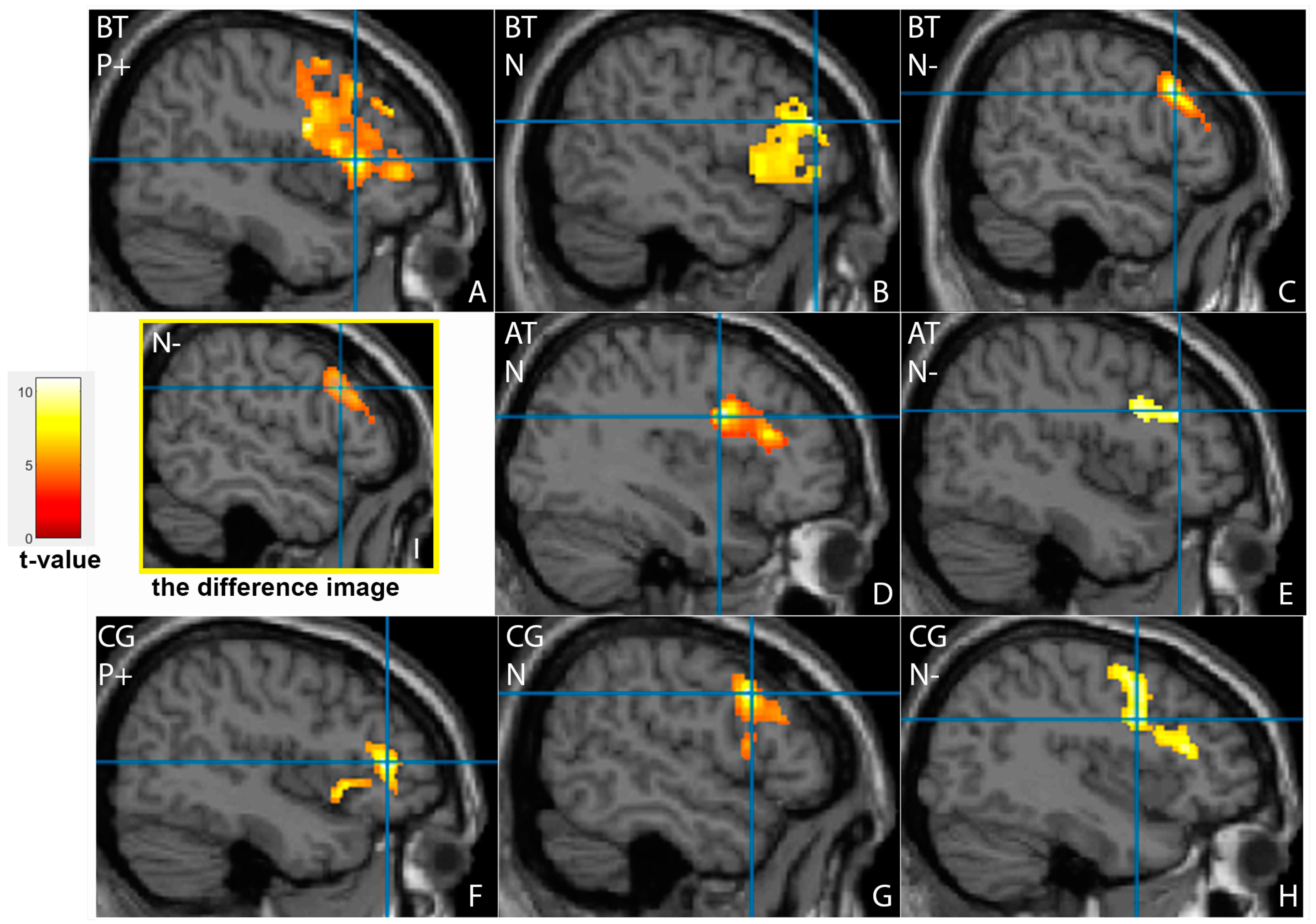
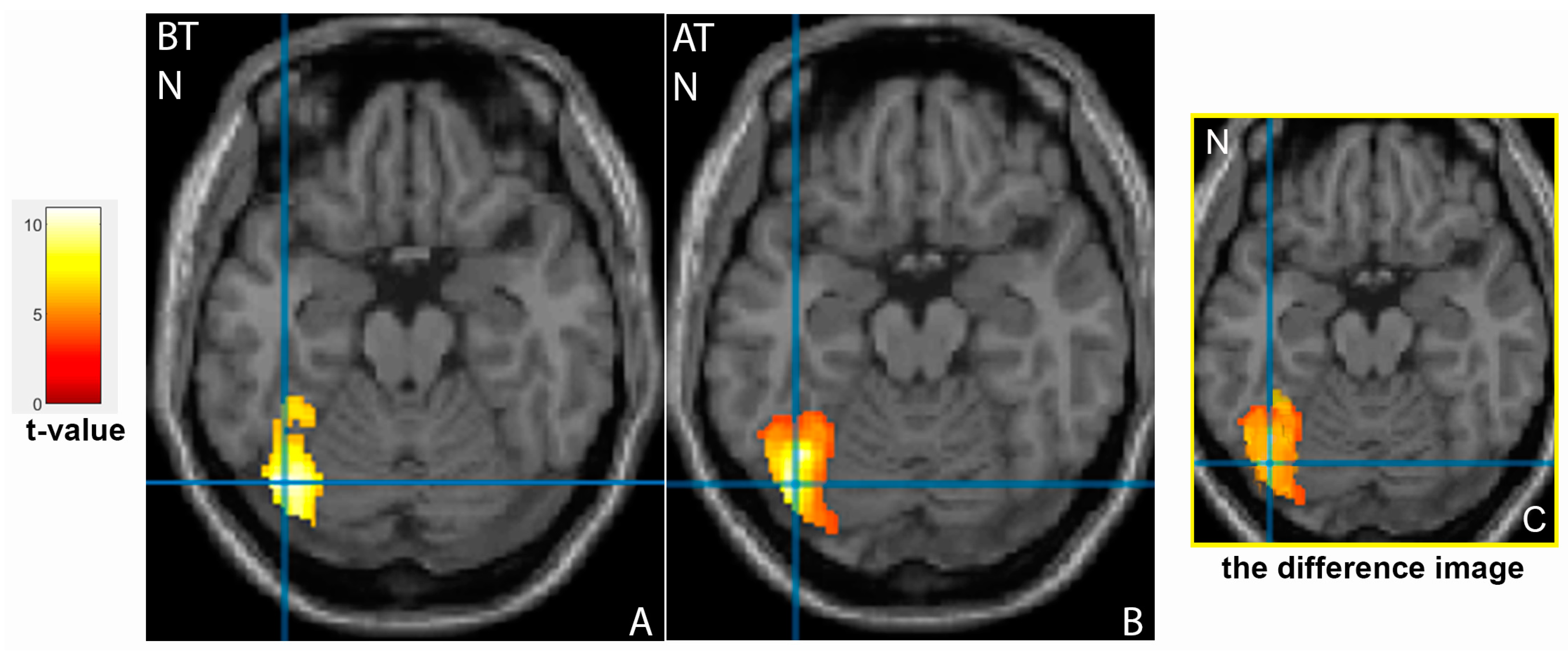
3.2. Comparison of Brain Activation Patterns in Patients before and after Treatment
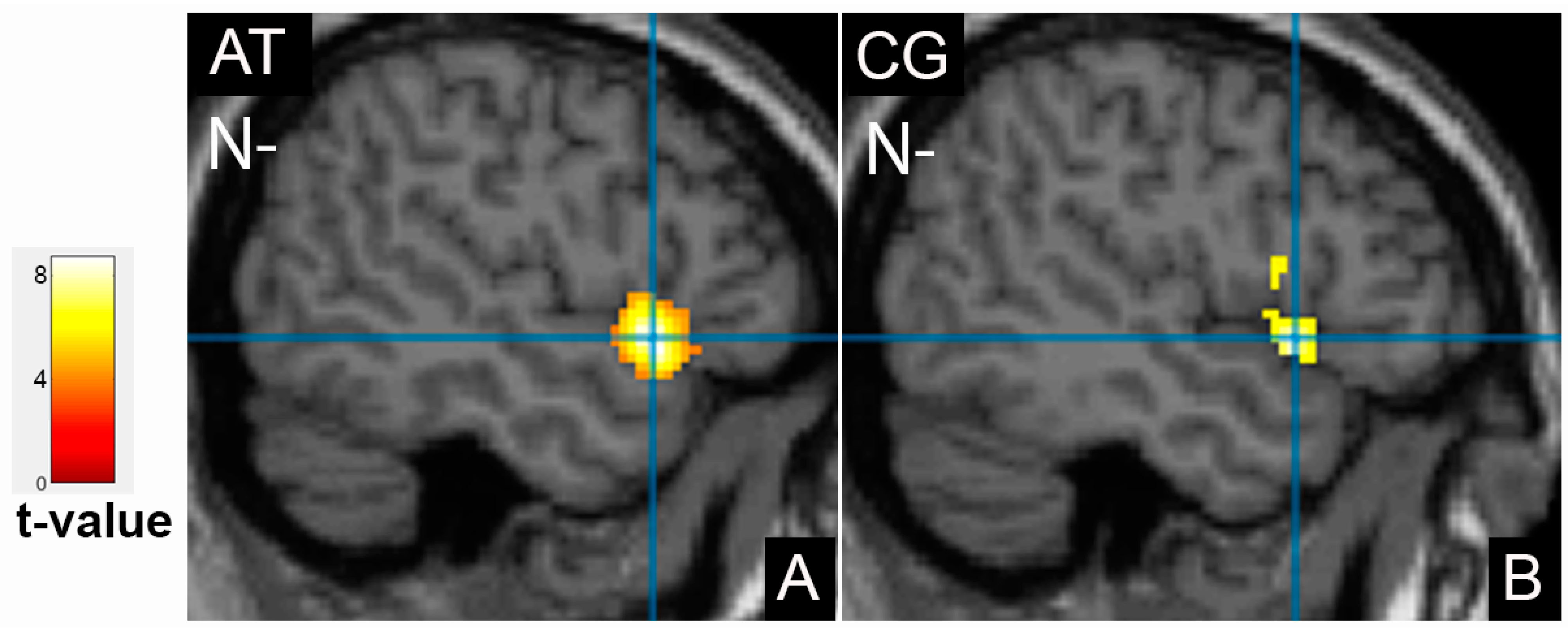
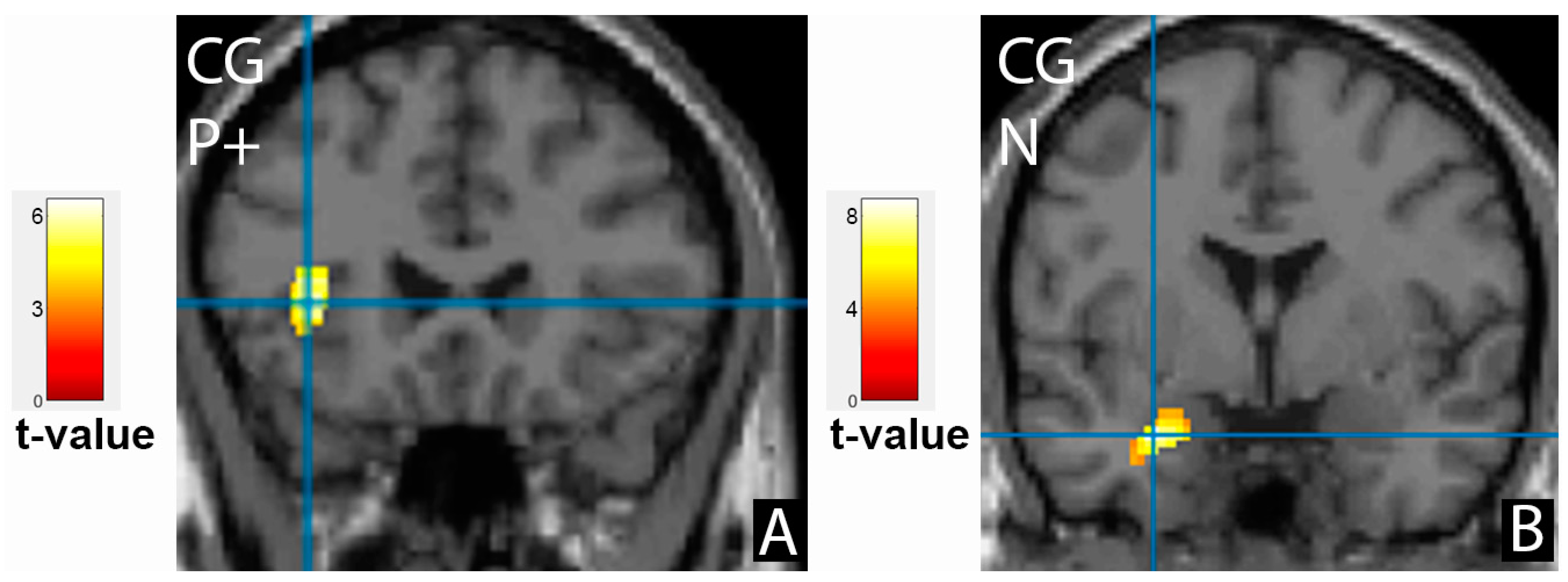
3.3. Comparison of Brain Activation Patterns in Patients before Treatment and Healthy Controls
4. Discussion
4.1. Limitations of This Study
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joormann, J.; Gotlib, I.H. Emotion Regulation in Depression: Relation to Cognitive Inhibition. Cogn. Emot. 2010, 24, 281–298. [Google Scholar] [CrossRef]
- Elliott, R.; Zahn, R.; Deakin, J.F.W.; Anderson, I.M. Affective Cognition and Its Disruption in Mood Disorders. Neuropsychopharmacology 2011, 36, 153–182. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Byrow, Y.; Fritz, K.; Das, P.; Baune, B.T.; Porter, R.J.; Outhred, T. Mood Disorders: Neurocognitive Models. Bipolar Disord. 2015, 17, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.P.; Chen, M.C.; Gotlib, I.H. Neural Systems Approaches to Understanding Major Depressive Disorder: An Intrinsic Functional Organization Perspective. Neurobiol. Dis. 2013, 52, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Mayberg, H.S. Limbic-Cortical Dysregulation: A Proposed Model of Depression. J. Neuropsychiatry Clin. Neurosci. 1997, 9, 471–481. [Google Scholar] [CrossRef]
- Groves, S.J.; Pitcher, T.L.; Melzer, T.R.; Jordan, J.; Carter, J.D.; Malhi, G.S.; Johnston, L.C.; Porter, R.J. Brain Activation during Processing of Genuine Facial Emotion in Depression: Preliminary Findings. J. Affect. Disord. 2018, 225, 91–96. [Google Scholar] [CrossRef]
- Bourke, C.; Douglas, K.; Porter, R. Processing of Facial Emotion Expression in Major Depression: A Review. Aust. N. Z. J. Psychiatry 2010, 44, 681–696. [Google Scholar] [CrossRef]
- Palmer, S.M.; Crewther, S.G.; Carey, L.M. A Meta-Analysis of Changes in Brain Activity in Clinical Depression. Front. Hum. Neurosci. 2015, 8, 1045. [Google Scholar] [CrossRef]
- Fu, C.H.Y.; Williams, S.C.R.; Cleare, A.J.; Brammer, M.J.; Walsh, N.D.; Kim, J.; Andrew, C.M.; Pich, E.M.; Williams, P.M.; Reed, L.J.; et al. Attenuation of the Neural Response to Sad Faces in Major Depression by Antidepressant Treatment: A Prospective, Event-Related Functional Magnetic Resonance Imaging Study. Arch. Gen. Psychiatry 2004, 61, 877–889. [Google Scholar] [CrossRef]
- Siegle, G.J.; Thompson, W.; Carter, C.S.; Steinhauer, S.R.; Thase, M.E. Increased Amygdala and Decreased Dorsolateral Prefrontal BOLD Responses in Unipolar Depression: Related and Independent Features. Biol. Psychiatry 2007, 61, 198–209. [Google Scholar] [CrossRef]
- Rosenblau, G.; Sterzer, P.; Stoy, M.; Park, S.; Friedel, E.; Heinz, A.; Pilhatsch, M.; Bauer, M.; Ströhle, A. Functional Neuroanatomy of Emotion Processing in Major Depressive Disorder Is Altered after Successful Antidepressant Therapy. J. Psychopharmacol. 2012, 26, 1424–1433. [Google Scholar] [CrossRef]
- Tassone, V.K.; Demchenko, I.; Salvo, J.; Mahmood, R.; Di Passa, A.-M.; Kuburi, S.; Rueda, A.; Bhat, V. Contrasting the Amygdala Activity and Functional Connectivity Profile between Antidepressant-Free Participants with Major Depressive Disorder and Healthy Controls: A Systematic Review of Comparative fMRI Studies. Psychiatry Res. Neuroimaging 2022, 325, 111517. [Google Scholar] [CrossRef]
- Scheuerecker, J.; Meisenzahl, E.M.; Koutsouleris, N.; Roesner, M.; Schöpf, V.; Linn, J.; Wiesmann, M.; Brückmann, H.; Möller, H.-J.; Frodl, T. Orbitofrontal Volume Reductions during Emotion Recognition in Patients with Major Depression. J. Psychiatry Neurosci. 2010, 35, 311–320. [Google Scholar] [CrossRef]
- Sundermann, B.; Olde lütke Beverborg, M.; Pfleiderer, B. Toward Literature-Based Feature Selection for Diagnostic Classification: A Meta-Analysis of Resting-State fMRI in Depression. Front. Hum. Neurosci. 2014, 8, 692. [Google Scholar] [CrossRef] [PubMed]
- Akhapkin, R.V.; Volel, B.A.; Shishorin, R.M.; Ustyuzhanin, D.V.; Petelin, D.S. Recognition of Facial Emotion Expressions in Patients with Depressive Disorders: A Prospective, Observational Study. Neurol. Ther. 2021, 10, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.A.; Asberg, M. A New Depression Scale Designed to Be Sensitive to Change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Ustyuzhanin, D.; Beliaevskaia, A.; Morozova, Y.; Zashezova, M.; Shariya, M.A.; Kropotov, J.; Konovalov, R.; Smulevich, A.; Smirnov, V.; Ternovoy, S. Brain Activation/deactivation Evaluation in Patients with Schizophrenia Using Functional MRI. Russ. Electron. J. Radiol. 2021, 11, 83–89. [Google Scholar] [CrossRef]
- Gur, R.C.; Sara, R.; Hagendoorn, M.; Marom, O.; Hughett, P.; Macy, L.; Turner, T.; Bajcsy, R.; Posner, A.; Gur, R.E. A Method for Obtaining 3-Dimensional Facial Expressions and Its Standardization for Use in Neurocognitive Studies. J. Neurosci. Methods 2002, 115, 137–143. [Google Scholar] [CrossRef]
- Ternovoy, S.; Ustyuzhanin, D.; Morozova, Y.; Shariya, M.; Roldan-Valadez, E.; Smirnov, V. Functional MRI Evince the Safety and Efficacy of Umbilical Cord Blood Cells Therapy in Patients with Schizophrenia. Schizophr. Res. 2020, 224, 175–177. [Google Scholar] [CrossRef]
- Nichols, T.; Hayasaka, S. Controlling the Familywise Error Rate in Functional Neuroimaging: A Comparative Review. Stat. Methods Med. Res. 2003, 12, 419–446. [Google Scholar] [CrossRef]
- Kanwisher, N.; McDermott, J.; Chun, M.M. The Fusiform Face Area: A Module in Human Extrastriate Cortex Specialized for Face Perception. J. Neurosci. 1997, 17, 4302–4311. [Google Scholar] [CrossRef] [PubMed]
- Stuhrmann, A.; Suslow, T.; Dannlowski, U. Facial Emotion Processing in Major Depression: A Systematic Review of Neuroimaging Findings. Biol. Mood Anxiety Disord. 2011, 1, 10. [Google Scholar] [CrossRef] [PubMed]
- Frodl, T.; Scheuerecker, J.; Albrecht, J.; Kleemann, A.M.; Müller-Schunk, S.; Koutsouleris, N.; Möller, H.-J.; Brückmann, H.; Wiesmann, M.; Meisenzahl, E. Neuronal Correlates of Emotional Processing in Patients with Major Depression. World J. Biol. Psychiatry 2009, 10, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Gotlib, I.H.; Sivers, H.; Gabrieli, J.D.E.; Whitfield-Gabrieli, S.; Goldin, P.; Minor, K.L.; Canli, T. Subgenual Anterior Cingulate Activation to Valenced Emotional Stimuli in Major Depression. Neuroreport 2005, 16, 1731–1734. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.H.Y.; Williams, S.C.R.; Cleare, A.J.; Scott, J.; Mitterschiffthaler, M.T.; Walsh, N.D.; Donaldson, C.; Suckling, J.; Andrew, C.; Steiner, H.; et al. Neural Responses to Sad Facial Expressions in Major Depression Following Cognitive Behavioral Therapy. Biol. Psychiatry 2008, 64, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Zhong, M.; Wang, X.; Xiao, J.; Yi, J.; Zhu, X.; Liao, J.; Wang, W.; Yao, S. Amygdala Hyperactivation and Prefrontal Hypoactivation in Subjects with Cognitive Vulnerability to Depression. Biol. Psychol. 2011, 88, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Suslow, T.; Konrad, C.; Kugel, H.; Rumstadt, D.; Zwitserlood, P.; Schöning, S.; Ohrmann, P.; Bauer, J.; Pyka, M.; Kersting, A.; et al. Automatic Mood-Congruent Amygdala Responses to Masked Facial Expressions in Major Depression. Biol. Psychiatry 2010, 67, 155–160. [Google Scholar] [CrossRef]
- Koenigs, M.; Grafman, J. The Functional Neuroanatomy of Depression: Distinct Roles for Ventromedial and Dorsolateral Prefrontal Cortex. Behav. Brain Res. 2009, 201, 239–243. [Google Scholar] [CrossRef]
- Li, G.; Ma, X.; Bian, H.; Sun, X.; Zhai, N.; Yao, M.; Qu, H.; Ji, S.; Tian, H.; Zhuo, C. A Pilot fMRI Study of the Effect of Stressful Factors on the Onset of Depression in Female Patients. Brain Imaging Behav. 2016, 10, 195–202. [Google Scholar] [CrossRef]
- Shallice, T.; Cipolotti, L. The Prefrontal Cortex and Neurological Impairments of Active Thought. Annu. Rev. Psychol. 2018, 69, 157–180. [Google Scholar] [CrossRef]
- Andrews, S.C.; Hoy, K.E.; Enticott, P.G.; Daskalakis, Z.J.; Fitzgerald, P.B. Improving Working Memory: The Effect of Combining Cognitive Activity and Anodal Transcranial Direct Current Stimulation to the Left Dorsolateral Prefrontal Cortex. Brain Stimul. 2011, 4, 84–89. [Google Scholar] [CrossRef]
- Pizzagalli, D.A.; Roberts, A.C. Prefrontal Cortex and Depression. Neuropsychopharmacology 2022, 47, 225–246. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Zhang, X.; Zhou, X.; Song, X.; Zhang, Z.; Xu, L.; Zhou, F.; Kendrick, K.M. Depression Mediates the Association between Insula-frontal Functional Connectivity and Social Interaction Anxiety. Hum. Brain Mapp. 2022, 43, 4266–4273. [Google Scholar] [CrossRef] [PubMed]
- Majrashi, N.A.; Alyami, A.S.; Shubayr, N.A.; Alenezi, M.M.; Waiter, G.D. Amygdala and Subregion Volumes Are Associated with Photoperiod and Seasonal Depressive Symptoms: A Cross-sectional Study in the UK Biobank Cohort. Eur. J. Neurosci. 2022, 55, 1388–1404. [Google Scholar] [CrossRef]
- Spies, M.; Kraus, C.; Geissberger, N.; Auer, B.; Klöbl, M.; Tik, M.; Stürkat, I.-L.; Hahn, A.; Woletz, M.; Pfabigan, D.M.; et al. Default Mode Network Deactivation during Emotion Processing Predicts Early Antidepressant Response. Transl. Psychiatry 2017, 7, 1008. [Google Scholar] [CrossRef]
- Liu, X.; Hou, Z.; Yin, Y.; Xie, C.; Zhang, H.; Zhang, H.; Zhang, Z.; Yuan, Y. Dopamine Multilocus Genetic Profile, Spontaneous Activity of Left Superior Temporal Gyrus, and Early Therapeutic Effect in Major Depressive Disorder. Front. Psychiatry 2020, 11, 591407. [Google Scholar] [CrossRef]
- Bae, S.; Kang, K.D.; Kim, S.W.; Shin, Y.J.; Nam, J.J.; Han, D.H. Investigation of an Emotion Perception Test Using Functional Magnetic Resonance Imaging. Comput. Methods Programs Biomed. 2019, 179, 104994. [Google Scholar] [CrossRef]
- Yan, R.; Geng, J.T.; Huang, Y.H.; Zou, H.W.; Wang, X.M.; Xia, Y.; Zhao, S.; Chen, Z.L.; Zhou, H.; Chen, Y.; et al. Aberrant Functional Connectivity in Insular Subregions in Somatic Depression: A Resting-State fMRI Study. BMC Psychiatry 2022, 22, 146. [Google Scholar] [CrossRef]
- Roldan-Valadez, E.; Rios, C.; Suarez-May, M.A.; Favila, R.; Aguilar-Castañeda, E. Main Effect and Interactions of Brain Regions and Gender in the Calculation of Volumetric Asymmetry Indices in Healthy Human Brains: Ancova Analyses of In Vivo 3T MRI Data. Anat. Rec. 2013, 296, 1913–1922. [Google Scholar] [CrossRef] [PubMed]
- Roldan-Valadez, E.; Suarez-May, M.A.; Favila, R.; Aguilar-Castañeda, E.; Rios, C. Selected Gray Matter Volumes and Gender but Not Basal Ganglia nor Cerebellum Gyri Discriminate Left Versus Right Cerebral Hemispheres: Multivariate Analyses in Human Brains at 3T. Anat. Rec. 2015, 298, 1336–1346. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Carmona, R. Main Effects and Interactions of Cerebral Hemispheres, Gender, and Age in the Calculation of Volumes and Asymmetries of Selected Structures of Episodic Memory. Funct. Neurol. 2016, 31, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, C.; Vöckel, J.; MacMaster, F.P.; Farzan, F.; Croarkin, P.E.; Galletly, C.; Kaess, M.; Bender, S.; Koenig, J. Transcranial Magnetic Stimulation in the Treatment of Adolescent Depression: A Systematic Review and Meta-Analysis of Aggregated and Individual-Patient Data from Uncontrolled Studies. Eur. Child. Adolesc. Psychiatry 2022, 31, 1501–1525. [Google Scholar] [CrossRef] [PubMed]
- Loh, A.; Gwun, D.; Chow, C.T.; Boutet, A.; Tasserie, J.; Germann, J.; Santyr, B.; Elias, G.; Yamamoto, K.; Sarica, C.; et al. Probing Responses to Deep Brain Stimulation with Functional Magnetic Resonance Imaging. Brain Stimul. 2022, 15, 683–694. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Patients (n = 16) | Controls (n = 16) | p Value |
|---|---|---|---|
| Gender, n (%) | |||
| Male | 2 (12.5) | 3 (18.8) | 0.87 |
| Female | 14 (87.5) | 13 (81.3) | |
| Age, years | 37.9 ± 12.5 | 37.3 ± 11.7 | 0.64 |
| Education, years | 16.3 ± 1.7 | 16.4 ± 2.7 | 0.73 |
| Marital status, n (%) | |||
| Married | 6 (37.5) | 13 (81.25) | 0.046 |
| Single | 9 (56.25) | 3 (18.75) | |
| Divorced | 1 (6.25) | 0 | |
| Diagnosis of the primary disease, n (%) | |||
| Single depressive episode | 10 (62.5) | – | N/A |
| Recurrent depressive episode | 6 (37.5) | – | N/A |
| MADRS mean score at baseline | 26.3 ± 4.4 | – | N/A |
| Cluster Location | Emotion | Extent | t-Value | p (FWE Corrected) | MNI Coordinates |
|---|---|---|---|---|---|
| Patients group before therapy | |||||
| Frontal cortex | |||||
| Left middle frontal gyrus, BA46 | N | 1457 | 6.24 | <0.001 | −48;38;20 |
| Right inferior frontal gyrus, BA46 | N | 632 | 8.83 | 0.001 | 50;40;4 |
| Right middle frontal gyrus | N- | 2064 | 10.89 | <0.001 | 54;20;30 |
| Right inferior frontal gyrus | P+ | 2368 | 8.91 | <0.001 | 46;22;8 |
| Occipital cortex | |||||
| Left fusiform gyrus, BA37 | N | 2001 | 10.59 | <0.001 | −40;−70;−18 |
| Right inferior occipital gyrus | N- | 3095 | 16.45 | <0.001 | 40;−70;−16 |
| Right occipital cortex, BA17 | P+ | 4282 | 13.27 | <0.001 | 18;−96;−4 |
| Left middle occipital gyrus, Cuneus | P+ | 2017 | 10.8 | <0.001 | −24;−92;6 |
| Cluster Location | Emotion | Extent | t-Value | p (FWE Corrected) | MNI Coordinates |
|---|---|---|---|---|---|
| Patients group after therapy | |||||
| Frontal cortex | |||||
| Right inferior frontal gyrus | N | 1390 | 10.97 | <0.001 | 38;4;28 |
| Right middle frontal gyrus | N- | 386 | 5.51 | 0.008 | 46;30;26 |
| Occipital cortex | |||||
| Left fusiform gyrus, BA37 | N | 1532 | 6.48 | <0.001 | −40;−68;−20 |
| Right fusiform gyrus, BA37 | N | 1861 | 7.44 | <0.001 | 44;−58;−24 |
| Temporal cortex | |||||
| Left superior temporal gyrus, BA22 | N- | 420 | 5.94 | 0.005 | −48;12;−4 |
| Cluster Location | Emotion | Extent | t-Value | p (FWE Corrected) | MNI Coordinates |
|---|---|---|---|---|---|
| Control group, cortical activation | |||||
| Frontal cortex | |||||
| Right middle frontal gyrus | N | 2228 | 8.91 | <0.001 | 54;14;34 |
| Right inferior frontal gyrus, precentral gyrus | N- | 946 | 6.05 | <0.001 | 42;6;30 |
| Right inferior frontal gyrus | P+ | 280 | 7.29 | 0.041 | 46;36;8 |
| Left inferior frontal gyrus, insula | P+ | 358 | 5.93 | 0.014 | −36;24;4 |
| Limbic lobe | |||||
| Left amygdala | N | 298 | 8.29 | 0.009 | −28;0;−24 |
| Occipital cortex | |||||
| Left middle occipital gyrus | N | 2977 | 9.13 | <0.001 | −40;−78;0 |
| Right fusiform gyrus, BA37 | P+ | 3809 | 12.41 | <0.001 | 36;−72;−20 |
| Temporal cortex | |||||
| Left superior temporal gyrus, BA22 | N- | 1689 | 8.4 | <0.001 | −50;14;−6 |
| Control group, cortical deactivation | |||||
| Right limbic lobe, cingulate gyrus, precuneus | N | 2851 | 9.49 | <0.001 | 6;−56;28 |
| Left limbic lobe, cingulate gyrus, BA31, precuneus | N- | 159 | 4.93 | 0.043 | −10;−58;24 |
| Left limbic lobe, cingulate gyrus, BA23 | P+ | 143 | 4.61 | 0.072 | −2;−36;30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ternovoy, S.; Ustyuzhanin, D.; Shariya, M.; Beliaevskaia, A.; Roldan-Valadez, E.; Shishorin, R.; Akhapkin, R.; Volel, B. Recognition of Facial Emotion Expressions in Patients with Depressive Disorders: A Functional MRI Study. Tomography 2023, 9, 529-540. https://doi.org/10.3390/tomography9020043
Ternovoy S, Ustyuzhanin D, Shariya M, Beliaevskaia A, Roldan-Valadez E, Shishorin R, Akhapkin R, Volel B. Recognition of Facial Emotion Expressions in Patients with Depressive Disorders: A Functional MRI Study. Tomography. 2023; 9(2):529-540. https://doi.org/10.3390/tomography9020043
Chicago/Turabian StyleTernovoy, Sergey, Dmitry Ustyuzhanin, Merab Shariya, Alena Beliaevskaia, Ernesto Roldan-Valadez, Rodion Shishorin, Roman Akhapkin, and Beatrice Volel. 2023. "Recognition of Facial Emotion Expressions in Patients with Depressive Disorders: A Functional MRI Study" Tomography 9, no. 2: 529-540. https://doi.org/10.3390/tomography9020043
APA StyleTernovoy, S., Ustyuzhanin, D., Shariya, M., Beliaevskaia, A., Roldan-Valadez, E., Shishorin, R., Akhapkin, R., & Volel, B. (2023). Recognition of Facial Emotion Expressions in Patients with Depressive Disorders: A Functional MRI Study. Tomography, 9(2), 529-540. https://doi.org/10.3390/tomography9020043