
Myocardial Contractility Pattern Characterization in Radiation-Induced Cardiotoxicity Using Magnetic Resonance Imaging: A Pilot Study with ContractiX

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Animal Model of Radiation Therapy
2.2. MRI Scans
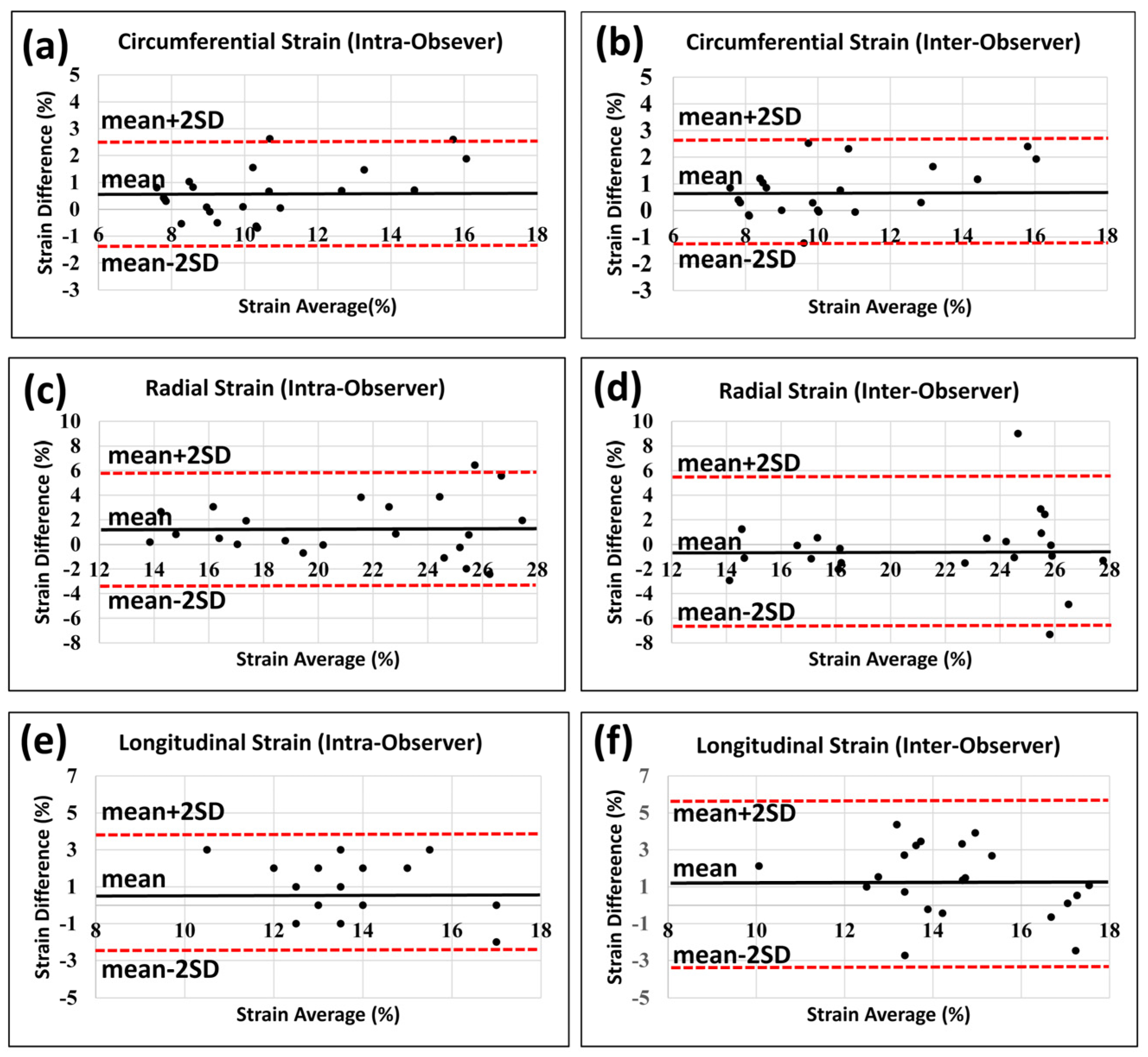
2.3. Image Analysis and Statistics
2.4. The ContractiX Parameter
2.5. Other Contractility Parameters
2.6. Statistical Analysis
3. Results
3.1. LVEF and Mass Are Increased Post-RT
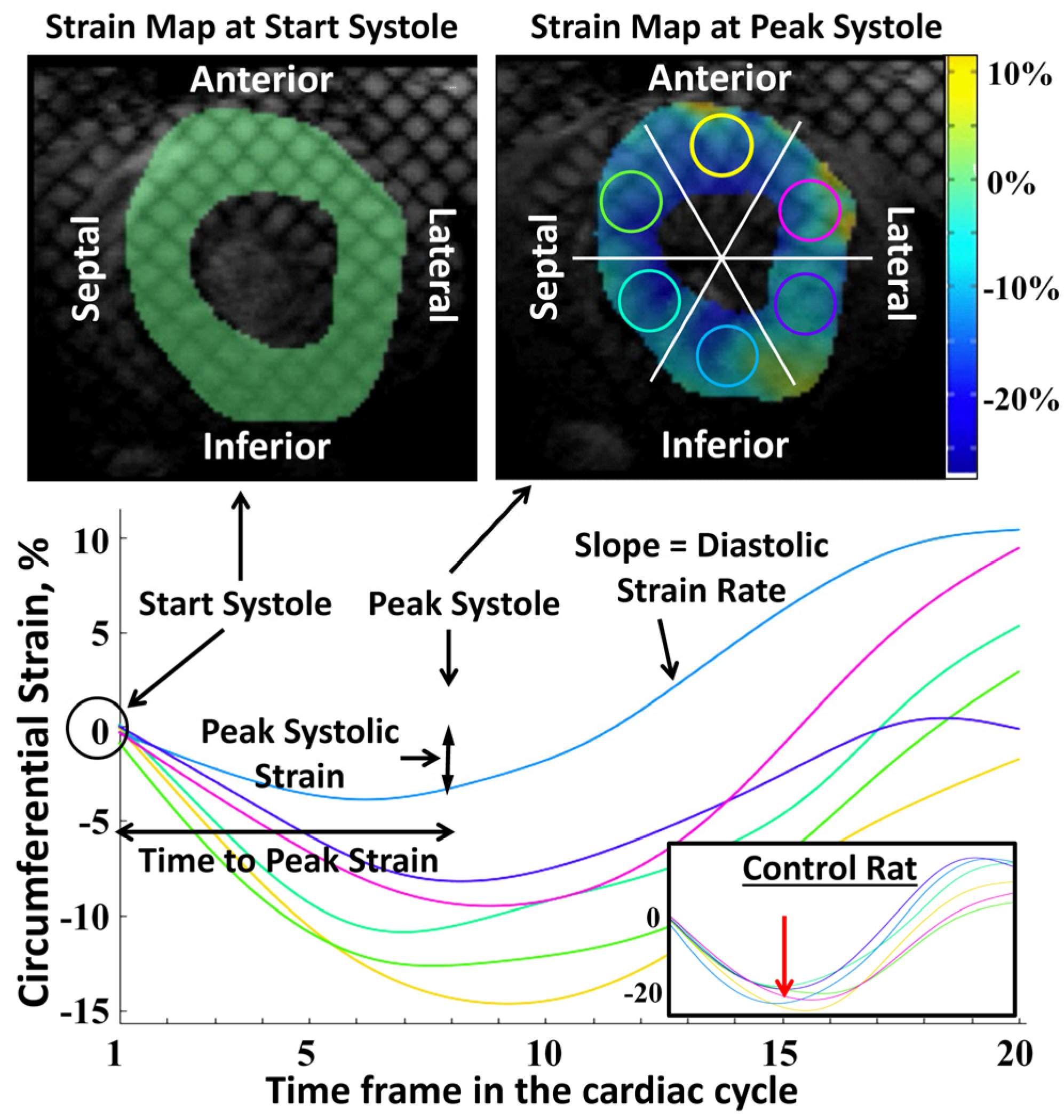
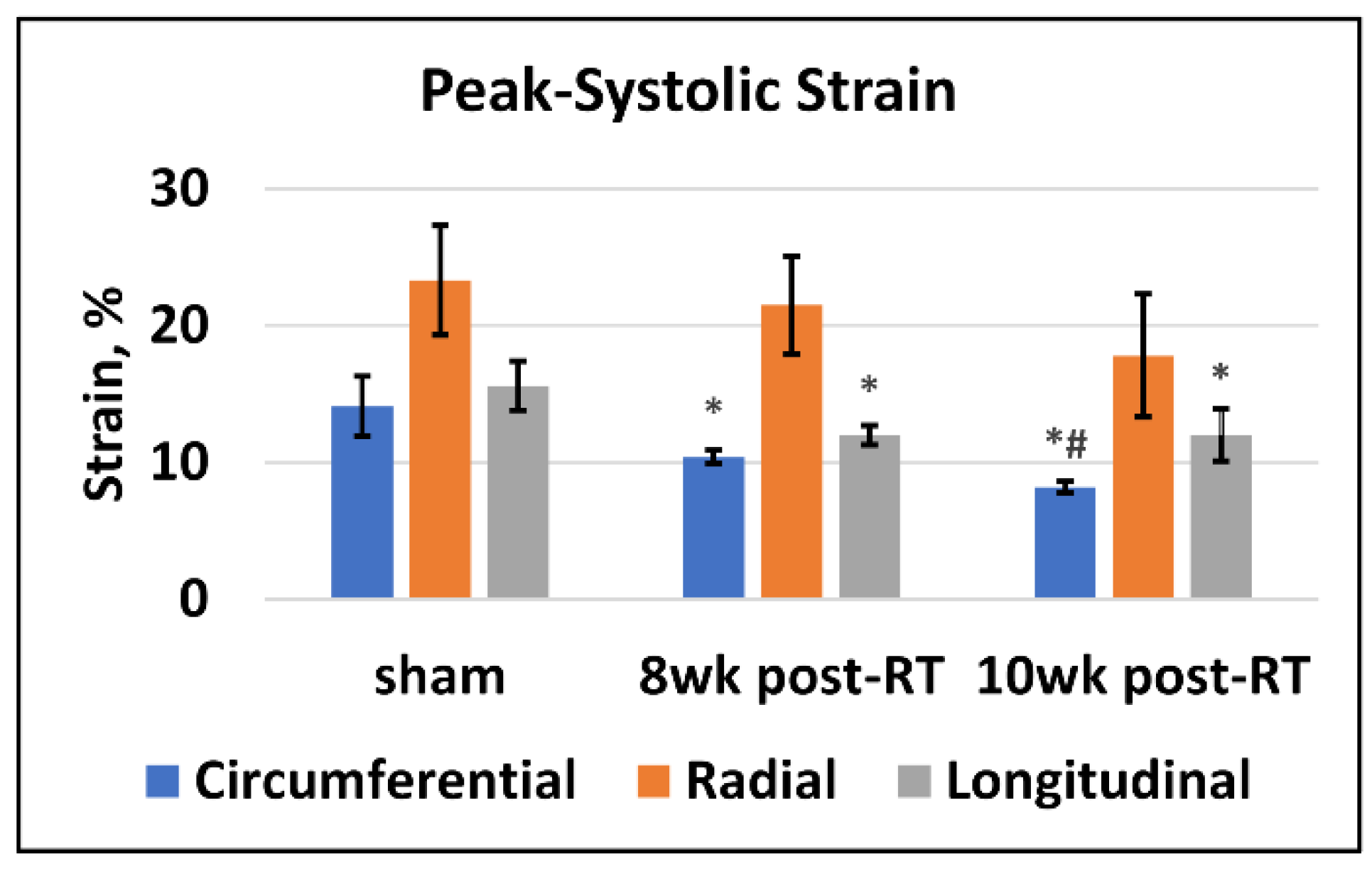
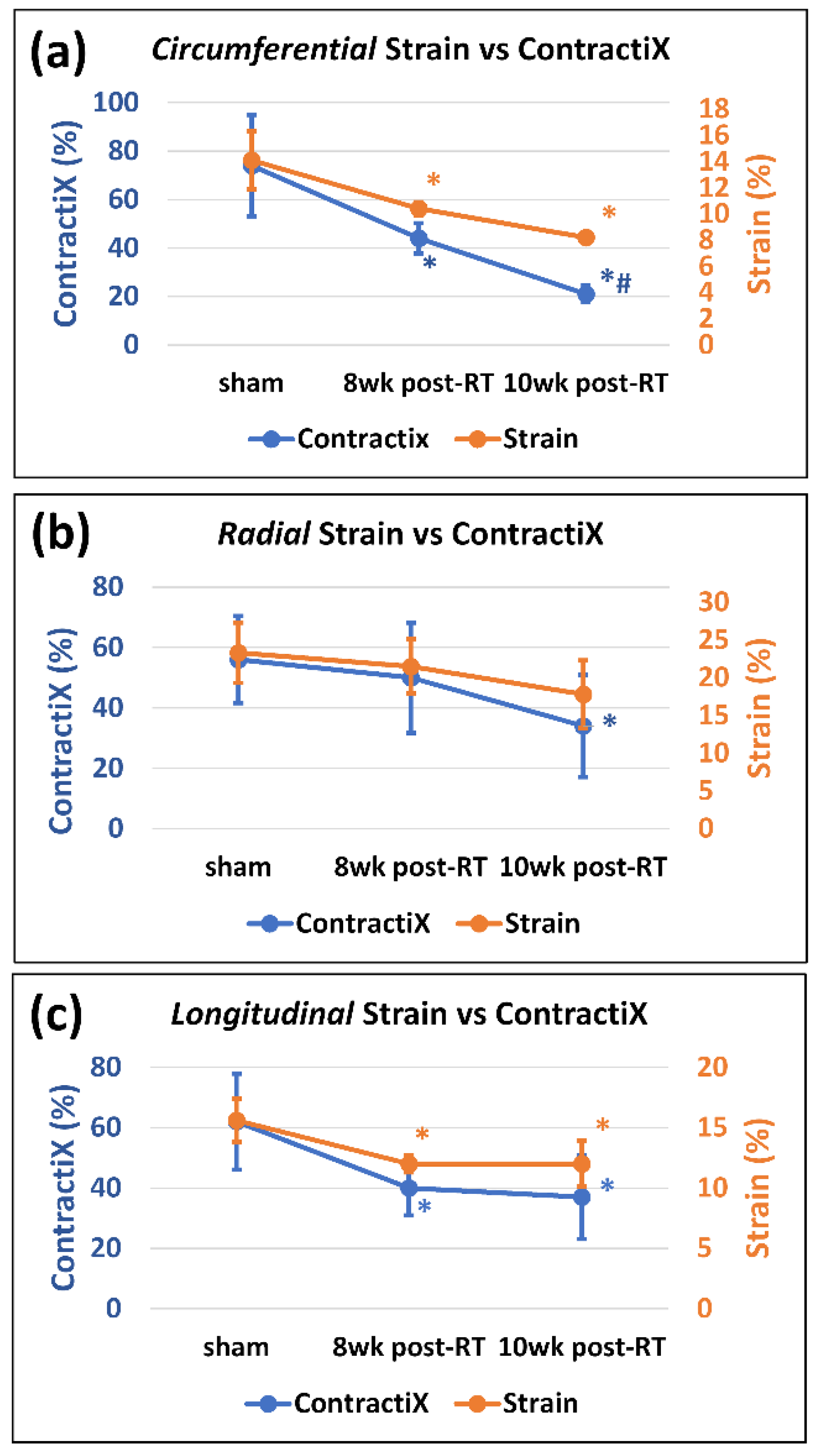
3.2. Strain Is Reduced Post-RT
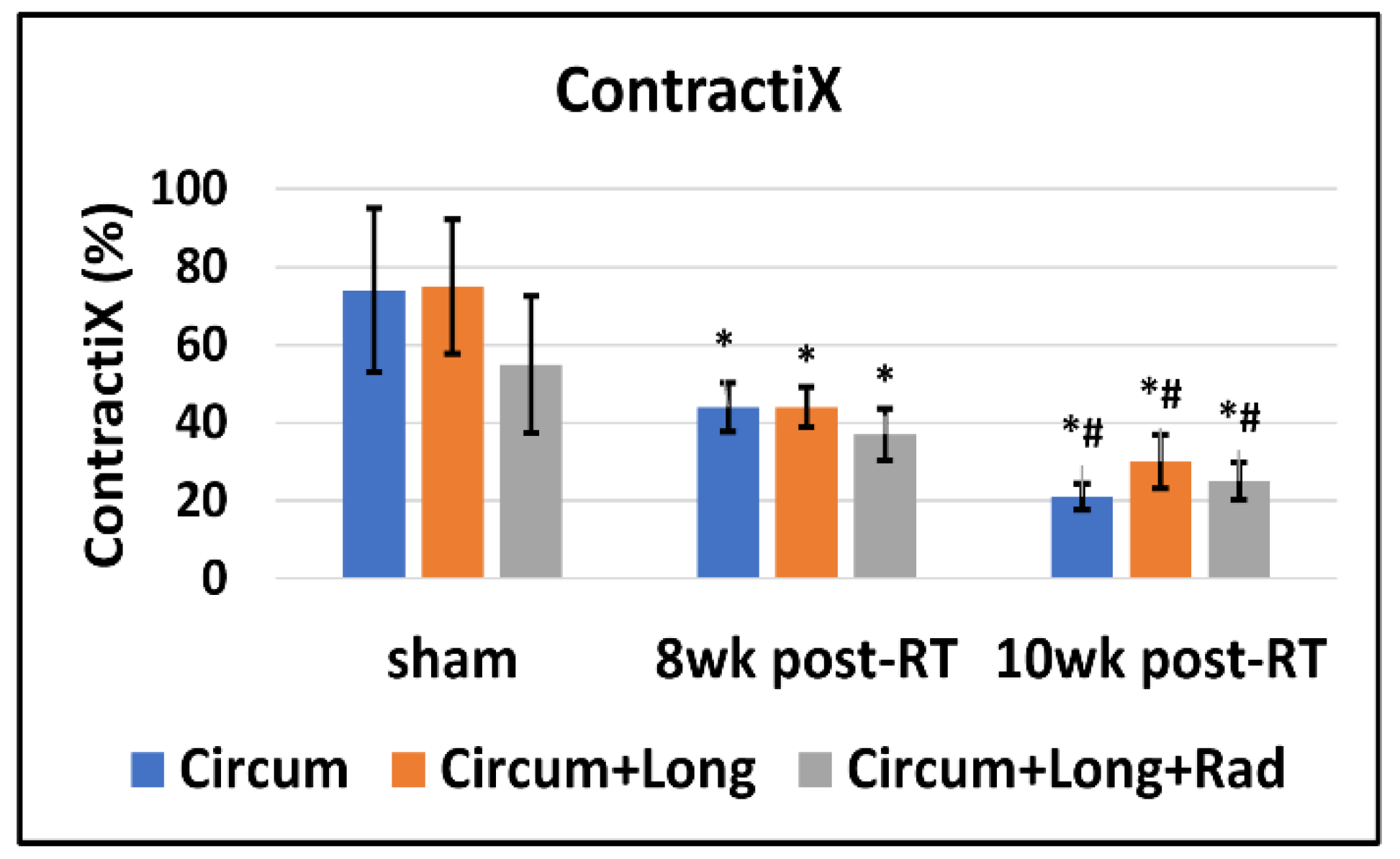
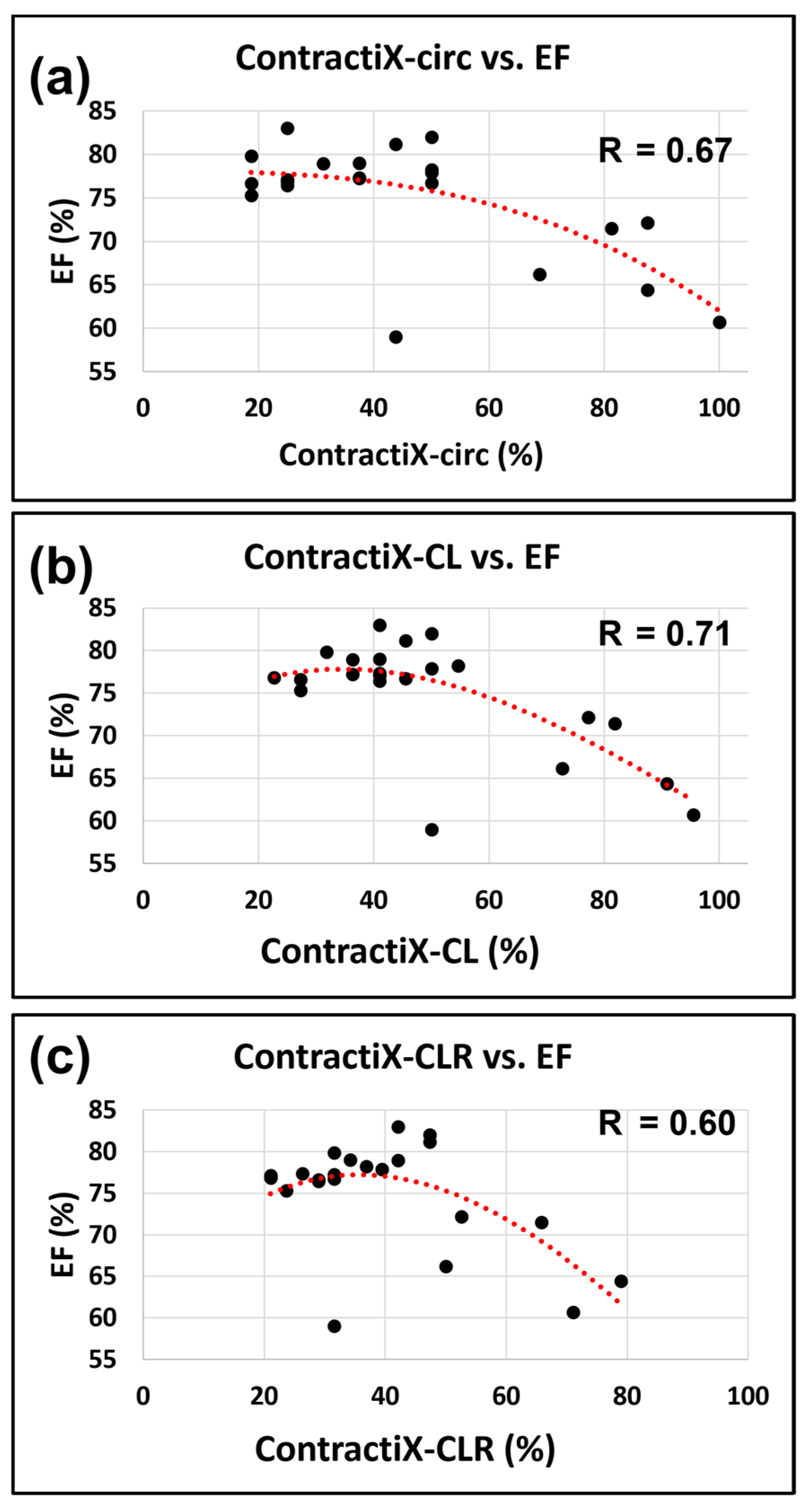
3.3. ContractiX Is a Sensitive Early Marker of Subclinical Cardiac Dysfunction Post-RT
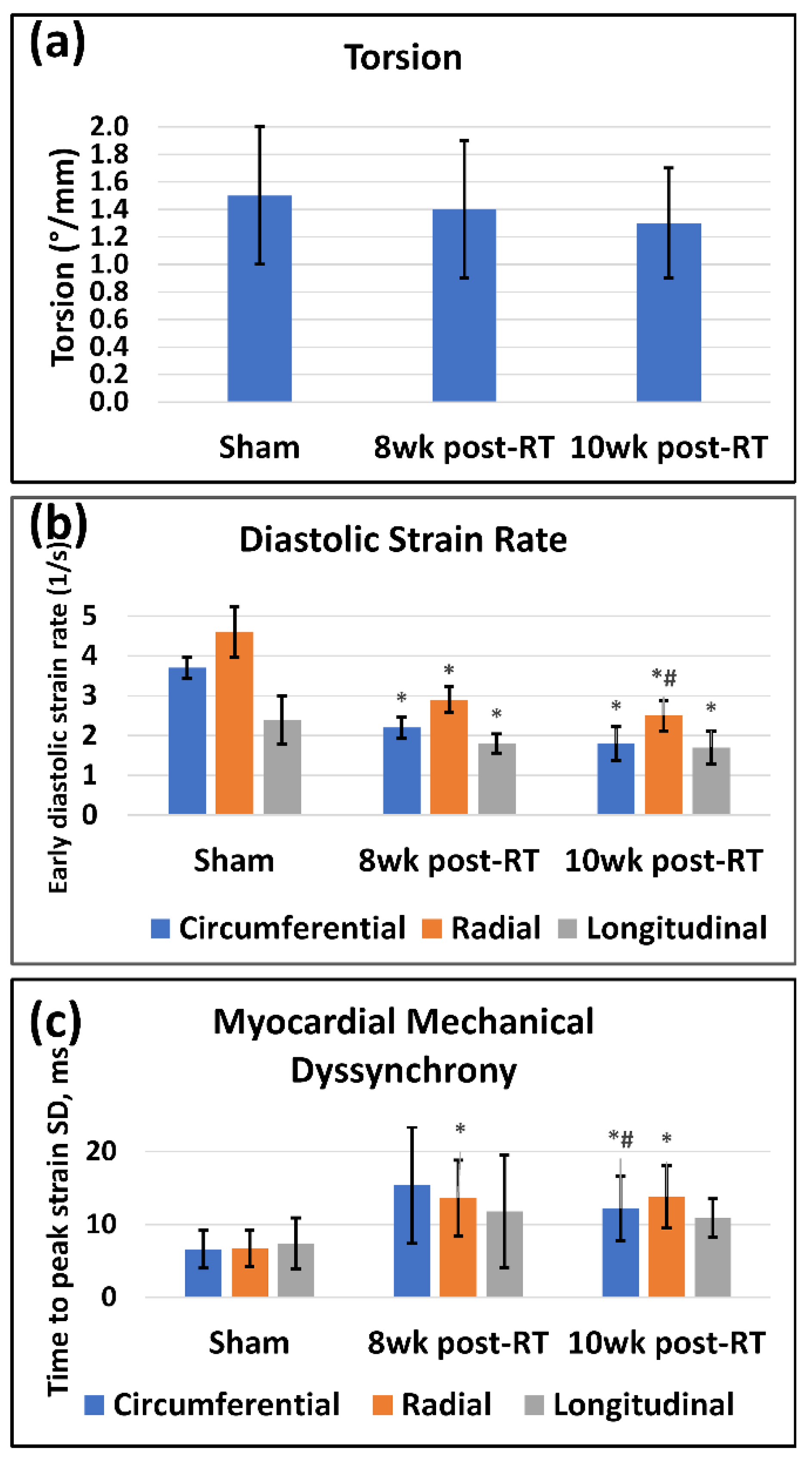
3.4. Other Heart Contractility Parameters Are Affected Post-RT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verma, V.; Fakhreddine, M.H.; Haque, W.; Butler, E.B.; Teh, B.S.; Simone, C.B. 2nd Cardiac mortality in limited-stage small cell lung cancer. Radiother. Oncol. 2018, 128, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Hardy, D.; Liu, C.C.; Cormier, J.N.; Xia, R.; Du, X.L. Cardiac toxicity in association with chemotherapy and radiation therapy in a large cohort of older patients with non-small-cell lung cancer. Ann. Oncol. 2010, 21, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Lally, B.E.; Detterbeck, F.C.; Geiger, A.M.; Thomas, C.R., Jr.; Machtay, M.; Miller, A.A.; Wilson, L.D.; Oaks, T.E.; Petty, W.J.; Robbins, M.E.; et al. The risk of death from heart disease in patients with nonsmall cell lung cancer who receive postoperative radiotherapy: Analysis of the Surveillance, Epidemiology, and End Results database. Cancer 2007, 110, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Dess, R.T.; Sun, Y.; Matuszak, M.M.; Sun, G.; Soni, P.D.; Bazzi, L.; Murthy, V.L.; Hearn, J.W.D.; Kong, F.M.; Kalemkerian, G.P.; et al. Cardiac Events After Radiation Therapy: Combined Analysis of Prospective Multicenter Trials for Locally Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2017, 35, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Pearlstein, K.A.; Patchett, N.D.; Deal, A.M.; Mavroidis, P.; Jensen, B.C.; Lipner, M.B.; Zagar, T.M.; Wang, Y.; Lee, C.B.; et al. Heart dosimetric analysis of three types of cardiac toxicity in patients treated on dose-escalation trials for Stage III non-small-cell lung cancer. Radiother. Oncol. 2017, 125, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Eblan, M.J.; Deal, A.M.; Lipner, M.; Zagar, T.M.; Wang, Y.; Mavroidis, P.; Lee, C.B.; Jensen, B.C.; Rosenman, J.G.; et al. Cardiac Toxicity After Radiotherapy for Stage III Non-Small-Cell Lung Cancer: Pooled Analysis of Dose-Escalation Trials Delivering 70 to 90 Gy. J. Clin. Oncol. 2017, 35, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Stam, B.; van der Bijl, E.; van Diessen, J.; Rossi, M.M.G.; Tijhuis, A.; Belderbos, J.S.A.; Damen, E.; Sonke, J.J. Heart dose associated with overall survival in locally advanced NSCLC patients treated with hypofractionated chemoradiotherapy. Radiother. Oncol. 2017, 125, 62–65. [Google Scholar] [CrossRef]
- Speirs, C.K.; DeWees, T.A.; Rehman, S.; Molotievschi, A.; Velez, M.A.; Mullen, D.; Fergus, S.; Trovo, M.; Bradley, J.D.; Robinson, C.G. Heart Dose Is an Independent Dosimetric Predictor of Overall Survival in Locally Advanced Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 293–301. [Google Scholar] [CrossRef]
- Yegya-Raman, N.; Wang, K.; Kim, S.; Reyhan, M.; Deek, M.P.; Sayan, M.; Li, D.; Patel, M.; Malhotra, J.; Aisner, J.; et al. Dosimetric Predictors of Symptomatic Cardiac Events after Conventional-Dose Chemoradiation Therapy for Inoperable Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2018, 13, 1508–1518. [Google Scholar] [CrossRef]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar]
- Niska, J.R.; Thorpe, C.S.; Allen, S.M.; Daniels, T.B.; Rule, W.G.; Schild, S.E.; Vargas, C.E.; Mookadam, F. Radiation and the heart: Systematic review of dosimetry and cardiac endpoints. Expert Rev. Cardiovasc. Ther. 2018, 16, 931–950. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.F.; Ky, B. Roadmap for biomarkers of cancer therapy cardiotoxicity. Heart 2016, 102, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Nakamori, S.; Jang, J.; Tschabrunn, C.M.; Pierce, P.; Goddu, B.; Rodriguez, J.; Ngo, L.H.; Tung, N.M.; Manning, W.J.; Nezafat, R. Noncontrast CMR for Detecting Early Myocardial Tissue Injury in a Swine Model of Anthracycline-Induced Cardiotoxicity. JACC Cardiovasc. Imaging 2019, 12, 2085–2087. [Google Scholar] [CrossRef] [PubMed]
- Kongbundansuk, S.; Hundley, W.G. Noninvasive imaging of cardiovascular injury related to the treatment of cancer. JACC Cardiovasc. Imaging 2014, 7, 824–838. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.-S.; Baruah, D.; Croisille, P.; Stojanovska, J.; Rubenstein, J.; Frei, A.; Schlaak, R.; Lin, C.; Pipke, J.L.; Lemke, A.; et al. Cardiac Magnetic Resonance for Early Detection of Radiation Therapy-Induced Cardiotoxicity in a Small Animal Model. JACC Cardio-Oncol. 2021, 3, 113–130. [Google Scholar] [CrossRef] [PubMed]
- Schlaak, R.A.; Frei, A.; Schottstaedt, A.M.; Tsaih, S.W.; Fish, B.L.; Harmann, L.; Liu, Q.; Gasperetti, T.; Medhora, M.; North, P.E.; et al. Mapping genetic modifiers of radiation-induced cardiotoxicity to rat chromosome 3. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H1267–H1280. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.H.; D’Agostino, R.B., Jr.; Hamilton, C.A.; Vasu, S.; Hall, M.E.; Kitzman, D.W.; Thohan, V.; Lawrence, J.A.; Ellis, L.R.; Lash, T.L.; et al. Longitudinal assessment of concurrent changes in left ventricular ejection fraction and left ventricular myocardial tissue characteristics after administration of cardiotoxic chemotherapies using T1-weighted and T2-weighted cardiovascular magnetic resonance. Circ. Cardiovasc. Imaging 2014, 7, 872–879. [Google Scholar]
- Ibrahim, E.-S.H. Myocardial tagging by cardiovascular magnetic resonance: Evolution of techniques--pulse sequences, analysis algorithms, and applications. J. Cardiovasc. Magn. Reson. 2011, 13, 36. [Google Scholar] [CrossRef]
- Toro-Salazar, O.H.; Gillan, E.; O’Loughlin, M.T.; Burke, G.S.; Ferranti, J.; Stainsby, J.; Liang, B.; Mazur, W.; Raman, S.V.; Hor, K.N. Occult cardiotoxicity in childhood cancer survivors exposed to anthracycline therapy. Circ. Cardiovasc. Imaging 2013, 6, 873–880. [Google Scholar] [CrossRef]
- Drafts, B.C.; Twomley, K.M.; D’Agostino, R., Jr.; Lawrence, J.; Avis, N.; Ellis, L.R.; Thohan, V.; Jordan, J.; Melin, S.A.; Torti, F.M.; et al. Low to moderate dose anthracycline-based chemotherapy is associated with early noninvasive imaging evidence of subclinical cardiovascular disease. JACC Cardiovasc. Imaging 2013, 6, 877–885. [Google Scholar] [CrossRef]
- Suerken, C.K.; D’Agostino, R.B., Jr.; Jordan, J.H.; Melendez, G.C.; Vasu, S.; Lamar, Z.S.; Hundley, W.G. Simultaneous Left Ventricular Volume and Strain Changes During Chemotherapy Associate with 2-Year Postchemotherapy Measures of Left Ventricular Ejection Fraction. J. Am. Heart Assoc. 2020, 9, e015400. [Google Scholar] [CrossRef] [PubMed]
- Barac, A. Optimal Treatment of Stage B Heart Failure in Cardio-Oncology?: The Promise of Strain. JACC Cardiovasc. Imaging 2018, 11, 1106–1108. [Google Scholar] [CrossRef] [PubMed]
- Jolly, M.P.; Jordan, J.H.; Melendez, G.C.; McNeal, G.R.; D’Agostino, R.B., Jr.; Hundley, W.G. Automated assessments of circumferential strain from cine CMR correlate with LVEF declines in cancer patients early after receipt of cardio-toxic chemotherapy. J. Cardiovasc. Magn. Reson. 2017, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Kar, J.; Cohen, M.V.; McQuiston, S.A.; Figarola, M.S.; Malozzi, C.M. Fully automated and comprehensive MRI-based left-ventricular contractility analysis in post-chemotherapy breast cancer patients. Br. J. Radiol. 2020, 93, 20190289. [Google Scholar] [CrossRef]
- Zhang, K.W.; Finkelman, B.S.; Gulati, G.; Narayan, H.K.; Upshaw, J.; Narayan, V.; Plappert, T.; Englefield, V.; Smith, A.M.; Zhang, C.; et al. Abnormalities in 3-Dimensional Left Ventricular Mechanics With Anthracycline Chemotherapy Are Associated With Systolic and Diastolic Dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1059–1068. [Google Scholar] [CrossRef]
- Schlaak, R.A.; SenthilKumar, G.; Boerma, M.; Bergom, C. Advances in Preclinical Research Models of Radiation-Induced Cardiac Toxicity. Cancers 2020, 12, 415. [Google Scholar] [CrossRef]
- Ibrahim, E.H.; Baruah, D.; Budde, M.; Rubenstein, J.; Frei, A.; Schlaak, R.; Gore, E.; Bergom, C. Optimized cardiac functional MRI of small-animal models of cancer radiation therapy. Magn. Reson. Imaging 2020, 73, 130–137. [Google Scholar] [CrossRef]
- Arts, T.; Prinzen, F.W.; Delhaas, T.; Milles, J.R.; Rossi, A.C.; Clarysse, P. Mapping displacement and deformation of the heart with local sine-wave modeling. IEEE Trans. Med. Imaging 2010, 29, 1114–1123. [Google Scholar] [CrossRef]
- Ibrahim, E.H.; Stojanovska, J.; Hassanein, A.; Duvernoy, C.; Croisille, P.; Pop-Busui, R.; Swanson, S.D. Regional cardiac function analysis from tagged MRI images. Comparison of techniques: Harmonic-Phase (HARP) versus Sinusoidal-Modeling (SinMod) analysis. Magn. Reson. Imaging 2018, 54, 271–282. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Tsai, H.R.; Gjesdal, O.; Wethal, T.; Haugaa, K.H.; Fossa, A.; Fossa, S.D.; Edvardsen, T. Left ventricular function assessed by two-dimensional speckle tracking echocardiography in long-term survivors of Hodgkin’s lymphoma treated by mediastinal radiotherapy with or without anthracycline therapy. Am. J. Cardiol. 2011, 107, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Erven, K.; Jurcut, R.; Weltens, C.; Giusca, S.; Ector, J.; Wildiers, H.; Van den Bogaert, W.; Voigt, J.U. Acute radiation effects on cardiac function detected by strain rate imaging in breast cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1444–1451. [Google Scholar] [CrossRef] [PubMed]
- Saiki, H.; Petersen, I.A.; Scott, C.G.; Bailey, K.R.; Dunlay, S.M.; Finley, R.R.; Ruddy, K.J.; Yan, E.; Redfield, M.M. Risk of Heart Failure With Preserved Ejection Fraction in Older Women After Contemporary Radiotherapy for Breast Cancer. Circulation 2017, 135, 1388–1396. [Google Scholar] [CrossRef] [PubMed]
- Walker, V.; Lairez, O.; Fondard, O.; Pathak, A.; Pinel, B.; Chevelle, C.; Franck, D.; Jimenez, G.; Camilleri, J.; Panh, L.; et al. Early detection of subclinical left ventricular dysfunction after breast cancer radiation therapy using speckle-tracking echocardiography: Association between cardiac exposure and longitudinal strain reduction (BACCARAT study). Radiat. Oncol. 2019, 14, 204. [Google Scholar] [CrossRef]
- Donnellan, E.; Phelan, D.; McCarthy, C.P.; Collier, P.; Desai, M.; Griffin, B. Radiation-induced heart disease: A practical guide to diagnosis and management. Cleve Clin. J. Med. 2016, 83, 914–922. [Google Scholar] [CrossRef]
- Klotz, S.; Hay, I.; Zhang, G.; Maurer, M.; Wang, J.; Burkhoff, D. Development of heart failure in chronic hypertensive Dahl rats: Focus on heart failure with preserved ejection fraction. Hypertension 2006, 47, 901–911. [Google Scholar] [CrossRef]
- Reshko, L.B.; Kalman, N.S.; Hugo, G.D.; Weiss, E. Cardiac radiation dose distribution, cardiac events and mortality in early-stage lung cancer treated with stereotactic body radiation therapy (SBRT). J. Thorac. Dis. 2018, 10, 2346–2356. [Google Scholar] [CrossRef]
- Mallio, C.A.; Quattrocchi, C.C.; Rovira, A.; Parizel, P.M. Gadolinium Deposition Safety: Seeking the Patient’s Perspective. AJNR Am. J. Neuroradiol. 2020, 41, 944–946. [Google Scholar] [CrossRef]
- Ibrahim, E.H.; Dennison, J.; Frank, L.; Stojanovska, J. Diastolic Cardiac Function by MRI-Imaging Capabilities and Clinical Applications. Tomography 2021, 7, 893–914. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sham | 8-Weeks Post-RT | p (8 Weeks vs. Sham) | 10-Weeks Post-RT | p (10 Weeks vs. Sham) | p (8 Weeks vs. 10 Weeks) | |
|---|---|---|---|---|---|---|
| EF (%) | 67 ± 6.9 | 78 ± 1.8 | <0.01 | 77 ± 1.7 | <0.01 | 0.37 |
| EDV (mL) | 0.29 ± 0.02 | 0.26 ± 0.03 | 0.05 | 0.27 ± 0.02 | 0.06 | 0.38 |
| ESV (mL) | 0.1 ± 0.02 | 0.06 ± 0.01 | <0.01 | 0.06 ± 0.01 | <0.01 | 0.30 |
| SV (mL) | 0.2 ± 0.02 | 0.2 ± 0.02 | 0.71 | 0.2 ± 0.01 | 0.42 | 0.52 |
| Mass (g) | 0.38 ± 0.04 | 0.49 ± 0.05 | <0.01 | 0.56 ± 0.04 | <0.01 | 0.04 |
| Ecc (%) | 14.1 ± 2.2 | 10.4 ± 0.5 | <0.01 | 8.2 ± 0.4 | <0.01 | <0.01 |
| Err (%) | 23.3 ± 4.0 | 22.5 ± 3.6 | 0.71 | 17.8 ± 4.5 | 0.06 | 0.11 |
| Ell (%) | 15.6 ± 1.8 | 12.0 ± 0.7 | <0.01 | 12.0 ± 1.9 | <0.01 | 0.99 |
| ContractiX-circ (%) | 74 ± 20.9 | 44 ± 6.3 | <0.01 | 21 ± 3.4 | <0.01 | <0.01 |
| ContractiX-rad (%) | 56 ± 14.4 | 50 ± 18.2 | 0.54 | 34 ± 16.9 | 0.04 | 0.09 |
| ContractiX-long (%) | 62 ± 15.9 | 40 ± 9.1 | 0.01 | 37 ± 13.9 | 0.02 | 0.62 |
| Torsion (°/mm) | 1.5 ± 0.5 | 1.4 ± 0.5 | 0.67 | 1.3 ± 0.4 | 0.43 | 0.86 |
| SR-cc (1/s) | 3.7 ± 0.26 | 2.2 ± 0.27 | <0.01 | 1.8 ± 0.43 | <0.01 | 0.17 |
| SR-rr (1/s) | 4.6 ± 0.63 | 2.9 ± 0.32 | <0.01 | 2.5 ± 0.38 | <0.01 | 0.04 |
| SR-ll (1/s) | 2.4 ± 0.61 | 1.8 ± 0.24 | 0.03 | 1.7 ± 0.41 | 0.03 | 0.73 |
| TTP-cc (ms) | 6.6 ± 2.6 | 15.4 ± 8.0 | 0.19 | 12.2 ± 4.4 | 0.04 | 0.40 |
| TTP-rr (ms) | 6.7 ± 2.5 | 13.6 ± 5.2 | 0.04 | 13.8 ± 4.3 | 0.02 | 0.96 |
| TTP-ll (ms) | 7.4 ± 3.5 | 11.8 ± 7.7 | 0.28 | 10.9 ± 2.6 | 0.08 | 0.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, E.-S.H.; Sosa, A.; Brown, S.-A.; An, D.; Klawikowski, S.; Baker, J.; Bergom, C. Myocardial Contractility Pattern Characterization in Radiation-Induced Cardiotoxicity Using Magnetic Resonance Imaging: A Pilot Study with ContractiX. Tomography 2023, 9, 36-49. https://doi.org/10.3390/tomography9010004
Ibrahim E-SH, Sosa A, Brown S-A, An D, Klawikowski S, Baker J, Bergom C. Myocardial Contractility Pattern Characterization in Radiation-Induced Cardiotoxicity Using Magnetic Resonance Imaging: A Pilot Study with ContractiX. Tomography. 2023; 9(1):36-49. https://doi.org/10.3390/tomography9010004
Chicago/Turabian StyleIbrahim, El-Sayed H., Antonio Sosa, Sherry-Ann Brown, Dayeong An, Slade Klawikowski, John Baker, and Carmen Bergom. 2023. "Myocardial Contractility Pattern Characterization in Radiation-Induced Cardiotoxicity Using Magnetic Resonance Imaging: A Pilot Study with ContractiX" Tomography 9, no. 1: 36-49. https://doi.org/10.3390/tomography9010004
APA StyleIbrahim, E.-S. H., Sosa, A., Brown, S.-A., An, D., Klawikowski, S., Baker, J., & Bergom, C. (2023). Myocardial Contractility Pattern Characterization in Radiation-Induced Cardiotoxicity Using Magnetic Resonance Imaging: A Pilot Study with ContractiX. Tomography, 9(1), 36-49. https://doi.org/10.3390/tomography9010004