

The Infraoptic or Infrachiasmatic Course of the Anterior Cerebral Artery Emerging an Elongated Internal Carotid Artery


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Osborn, A.G. Diagnostic Cerebral Angiography, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1999. [Google Scholar]
- Gray, H.; Standring, S.; Anand, N.; Birch, R.; Collins, P.; Crossman, A.; Gleeson, M.; Jawaheer, G.; Smith, A.L.; Spratt, J.D.; et al. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 41 ed.; Elsevier: London, UK, 2016. [Google Scholar]
- Dumitrescu, A.M.; Costea, C.F.; Cucu, A.I.; Dumitrescu, G.F.; Turliuc, M.D.; Scripcariu, D.V.; Ciocoiu, M.; Tanase, D.M.; Turliuc, S.; Bogdanici, C.M.; et al. The discovery of the circle of Willis as a result of using the scientific method in anatomical dissection. Rom. J. Morphol. Embryol. 2020, 61, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Ahn, J.G. Infraoptic course of both anterior cerebral arteries. J. Korean Neurosurg. Soc. 2010, 47, 71–73. [Google Scholar] [CrossRef] [PubMed]
- Chua, M.H.; Thomas, A.J.; Fusco, M.R.; Ogilvy, C.S. An unruptured anterior communicating artery aneurysm with bilateral infraoptic anterior cerebral arteries. Case report and review of the literature. J. Cereb. Endovasc. Neurosurg. 2014, 16, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Given, C.A., 2nd; Morris, P.P. Recognition and importance of an infraoptic anterior cerebral artery: Case report. AJNR Am. J. Neuroradiol. 2002, 23, 452–454. [Google Scholar]
- Chakraborty, S.; Fanning, N.F.; Lee, S.K.; Terbrugge, K.G. Bilateral infraoptic origin of anterior cerebral arteries: A rare anomaly and its embryological and clinical significance. Interv. Neuroradiol. 2006, 12, 155–159. [Google Scholar] [CrossRef]
- Maurer, J.; Maurer, E.; Perneczky, A. Surgically verified variations in the A1 segment of the anterior cerebral artery. Report of two cases. J. Neurosurg. 1991, 75, 950–953. [Google Scholar] [CrossRef]
- Moraru, L.; Rusu, M.C.; Popescu, S.A. True terminal pentafurcation of the external carotid artery and terminal trifurcation of the contralateral one, occipitoauricular trunk, retropharyngeal internal carotid artery. Surg. Radiol. Anat. 2021, 43, 1895–1900. [Google Scholar] [CrossRef]
- Horos Project 2018 DICOM Image Viewing and Measuring. Available online: http://horosproject.org/ (accessed on 15 August 2022).
- Nandish, H.S.; Selvapandian, S.; Ghosh, S. Surgical Significance of Infra-Optic Course of A1 Segment of Anterior Cerebral Artery: Report of Two Cases. Asian J. Neurosurg. 2019, 14, 927–929. [Google Scholar] [CrossRef]
- Robinson, L.R. An unusual human anterior cerebral artery. J. Anat. 1959, 93, 131–133. [Google Scholar]
- Spinnato, S.; Pasqualin, A.; Chioffi, F.; Da Pian, R. Infraoptic course of the anterior cerebral artery associated with an anterior communicating artery aneurysm: Anatomic case report and embryological considerations. Neurosurgery 1999, 44, 1315–1319. [Google Scholar]
- Kang, H.J.; Lee, Y.S.; Suh, S.J.; Lee, J.H.; Ryu, K.Y.; Kang, D.G. A Ruptured Aneurysm at the Infraoptic Azygous Anterior Cerebral Artery with the Contralateral Internal Carotid Artery Agenesis Treated by Y-stent Assisted Coil Embolization. J. Cereb. Endovasc. Neurosurg. 2012, 14, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Kochar, P.S.; Soin, P.; Elfatairy, K. Infraoptic anterior cerebral artery or carotid-anterior cerebral artery anastomosis: A very rare embryological variation. Case series and review of literature. Clin. Imaging 2021, 79, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Isherwood, I.; Dutton, J. Unusual anomaly of anterior cerebral artery. Acta. Radiol. Diagn. (Stockh.) 1969, 9, 345–351. [Google Scholar] [PubMed]
- Besson, G. Anomalie rare du polygone de Willis: Trajet sous-optique des deux artères cérébrales antérieures. Anévrysme associé de la bifurcation du tronc basilaire. Neurochirurgie 1980, 26, 71–75. [Google Scholar] [PubMed]
- Lehmann, G.; Vincentelli, F.; Ebagosti, A. Rare abnormalities of the circle of Willis: Infra-optic pathway of the anterior cerebral arteries (author’s transl). Neurochirurgie 1980, 26, 243–246. [Google Scholar]
- Wong, S.T.; Yuen, S.C.; Fok, K.F.; Yam, K.Y.; Fong, D. Infraoptic anterior cerebral artery: Review, report of two cases and an anatomical classification. Acta. Neurochir. (Wien.) 2008, 150, 1087–1096. [Google Scholar] [CrossRef]
- Rao, A.S.; Kiran, N.A.; Assis, Z.A.; Hegde, A.S. Infraoptic course of the anterior cerebral artery associated with anterior communicating artery and distal anterior cerebral artery aneurysms. Neurol India 2015, 63, 797–799. [Google Scholar]
- Kawaji, H.; Amano, S.; Hiramatsu, H.; Sakai, N.; Kamio, Y.; Namba, H. Dissecting Aneurysm at the Proximal Segment of the Anterior Cerebral Artery Associated with Infraoptic Course Anterior Cerebral Artery. NMC Case Rep. J. 2014, 1, 12–15. [Google Scholar] [CrossRef]
- Takeshita, M.; Kubo, O.; Onda, H.; Nagao, T.; Kawamata, T.; Uchinuno, H.; Nitta, M.; Yamamura, K.; Kagawa, M. A case showing the infraoptic course of the anterior cerebral artery associated with anterior cerebral artery aneurysm. No Shinkei Geka 1991, 19, 871–876. [Google Scholar]
- Kim, M.S.; Sim, S.Y. Infraoptic anterior cerebral artery: Case series report and literature review. Surg. Radiol. Anat. 2016, 38, 887–891. [Google Scholar] [CrossRef]
- Mahajan, A.; Banga, V.; Chatterjee, A.; Goel, G. Infraoptic Course of Anterior Cerebral Artery Coexistence with Double Fenestration of Proximal A2 Segment of Anterior Cerebral Artery with Associated Dysplastic Anterior Communicating Artery Aneurysm Treated with Stent-Assisted Coiling. Asian J. Neurosurg. 2020, 15, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Turkoglu, E.; Arat, A.; Patel, N.; Kertmen, H.; Baskaya, M.K. Anterior communicating artery aneurysm associated with an infraoptic course of anterior cerebral artery and rare variant of the persistent trigeminal artery: A case report and literature review. Clin. Neurol. Neurosurg. 2011, 113, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Ogura, K.; Hasegawa, K.; Kobayashi, T.; Kohno, M.; Hondo, H. A case of bilateral infraoptic course of ACA associated with multiple cerebral artery aneurysms. No Shinkei Geka 1998, 26, 525–530. [Google Scholar] [PubMed]
- Matsuura, K.; Uchino, A.; Saito, N.; Ishida, J.; Suzuki, T. Carotid-anterior cerebral artery (ACA) anastomosis associated with azygos ACA and ophthalmic artery arising from the middle meningeal artery: A case report. Surg. Radiol. Anat. 2020, 42, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Nutik, S.; Dilenge, D. Carotid-anterior cerebral artery anastomosis. Case report. J. Neurosurg. 1976, 44, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Odake, G. Carotid-anterior cerebral artery anastomosis with aneurysm: Case report and review of the literature. Neurosurgery 1988, 23, 654–658. [Google Scholar] [CrossRef]
- Uchino, A.; Saito, N.; Okada, Y.; Inoue, K. Carotid-anterior cerebral artery anastomosis on MR angiography: A university hospital-based study. Neuroradiology 2012, 54, 13–18. [Google Scholar] [CrossRef]
- Uchino, A.; Sawada, A.; Takase, Y.; Imaizumi, T.; Egashira, R.; Matsuo, M.; Kudo, S. Carotid-anterior cerebral artery anastomosis: MR angiographic features and literature review. Clin. Imaging 2004, 28, 377–380. [Google Scholar] [CrossRef]
- Ban, S.; Nakatsu, S.; Matsumoto, S.; Sato, S.; Motozaki, T.; Yamamoto, T. Three cases of carotid anterior cerebral anastomosis. No Shinkei Geka 1990, 18, 1071–1077. [Google Scholar]
- Yi, Z.; Sasaki, T.; Satoh, D.; Muruta, T.; Kitazawa, K.; Kobayashi, S. Carotid-Anterior Cerebral Artery Anastomosis Associated with Paraclinoid Aneurysm and Ophthalmic Artery Originating From Middle Meningeal Artery: Case Report and Consideration of Terminology. World Neurosurg. 2016, 88, 689.e1–689.e4. [Google Scholar] [CrossRef]
- Uchino, A. Infraoptic anterior cerebral artery (ACA) versus carotid-ACA anastomosis. Surg. Radiol. Anat. 2017, 39, 937. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, I. Agenesis of the internal carotid artery. Neurology 1962, 12, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Bosma, N.J. Infra-optic course of anterior cerebral artery and low bifurcation of the internal carotid artery. Acta. Neurochir. (Wien.) 1977, 38, 305–312. [Google Scholar] [CrossRef]
- Laws, E.R., Jr.; Trautmann, J.C.; Hollenhorst, R.W., Jr. Transsphenoidal decompression of the optic nerve and chiasm. Visual results in 62 patients. J. Neurosurg. 1977, 46, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.F.; Scott, M.; Erwin, G. Carotid artery ectasia coexistent with primary open angle glaucoma. Clin. Exp. Ophthalmol. 2001, 29, 44–46. [Google Scholar] [CrossRef]
- Hendricks, B.K.; Benet, A.; Lawrence, P.M.; Benner, D.; Preul, M.C.; Lawton, M.T. Anatomical Triangles for Use in Skull Base Surgery: A Comprehensive Review. World Neurosurg. 2022, 164, 79–92. [Google Scholar] [CrossRef]
- Briggs, R.G.; Conner, A.K.; Chakraborty, A.R.; Allan, P.G.; Young, I.M.; Teo, C.; Sughrue, M.E. An Eyebrow, Supracarotid Triangle Approach for Lesions at the Ventral Thalamopeduncular Junction: A Technical Report. World Neurosurg. 2020, 140, e41–e45. [Google Scholar] [CrossRef]
- Waldron, J.S.; Lawton, M.T. The supracarotid-infrafrontal approach: Surgical technique and clinical application to cavernous malformations in the anteroinferior Basal Ganglia. Neurosurgery 2009, 64, ons86–ons95, discussion ons95. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Right Side | Left Side | Other Variations | Figure |
|---|---|---|---|---|
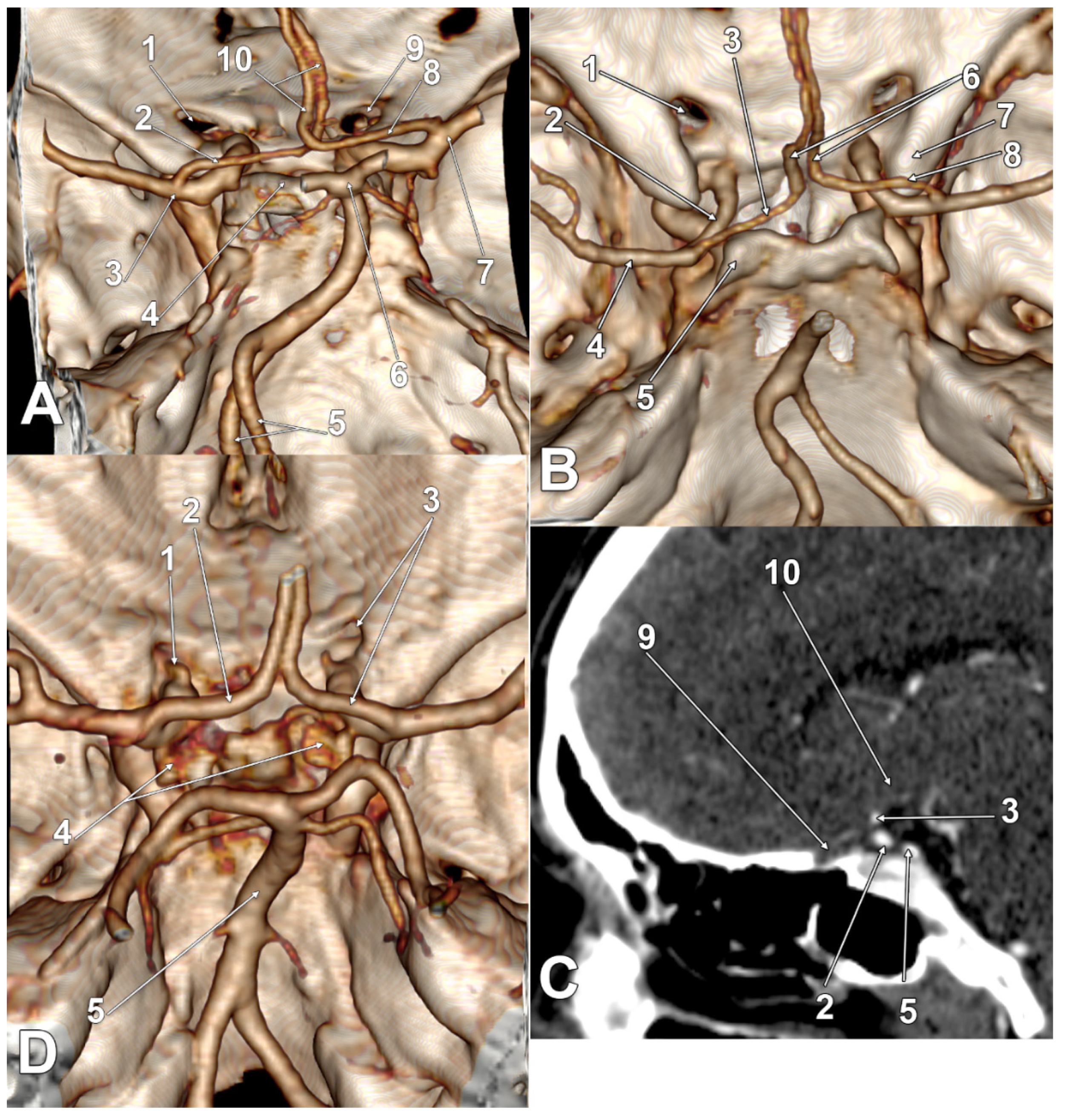
| M | type 3 IO A1 SCar | type 3 IO A1 SCar | high BA bifurcation | Figure 3A |
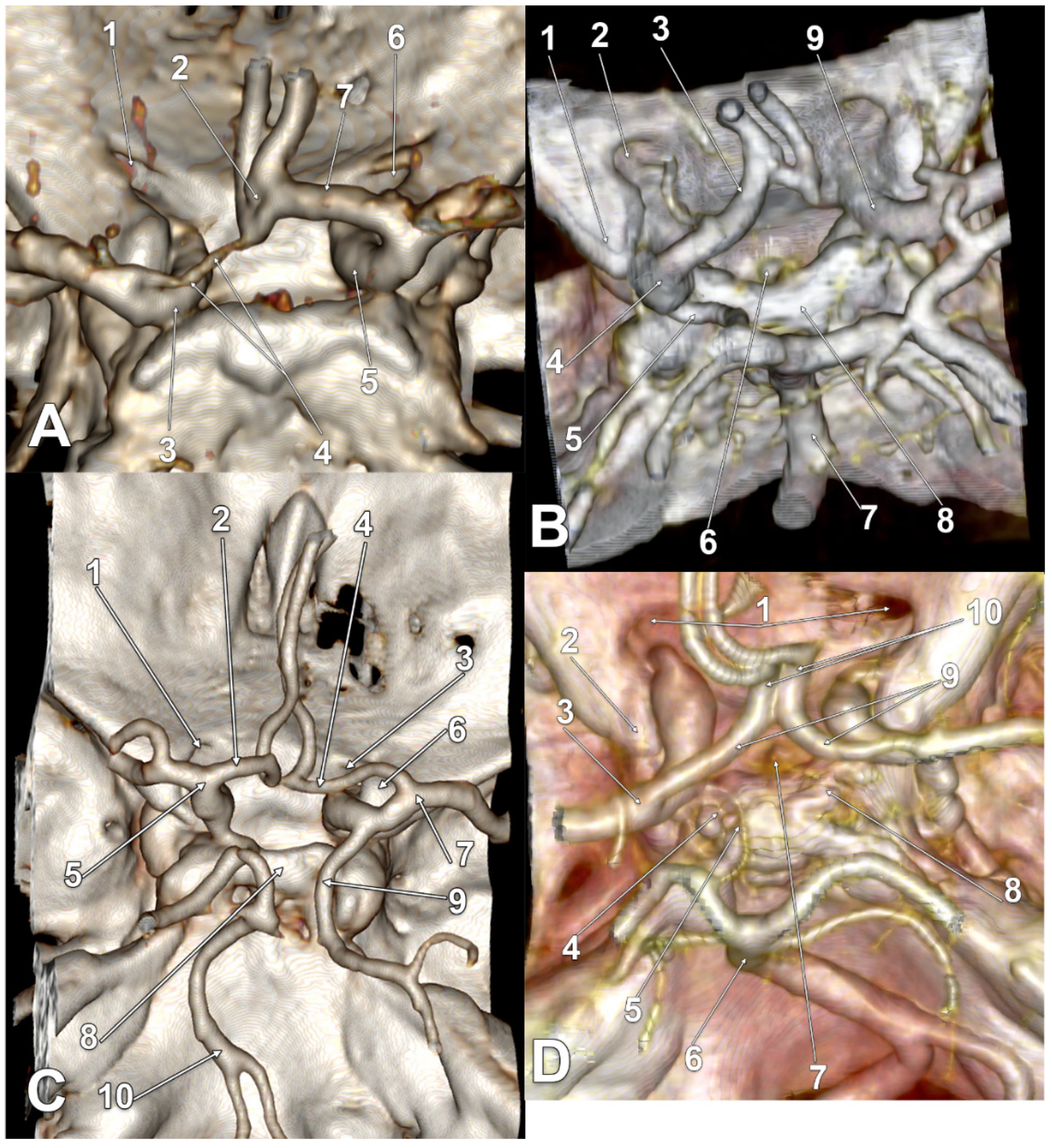
| M | type 3 IO A1 | type 3 IO A1 | Figure 2D | |
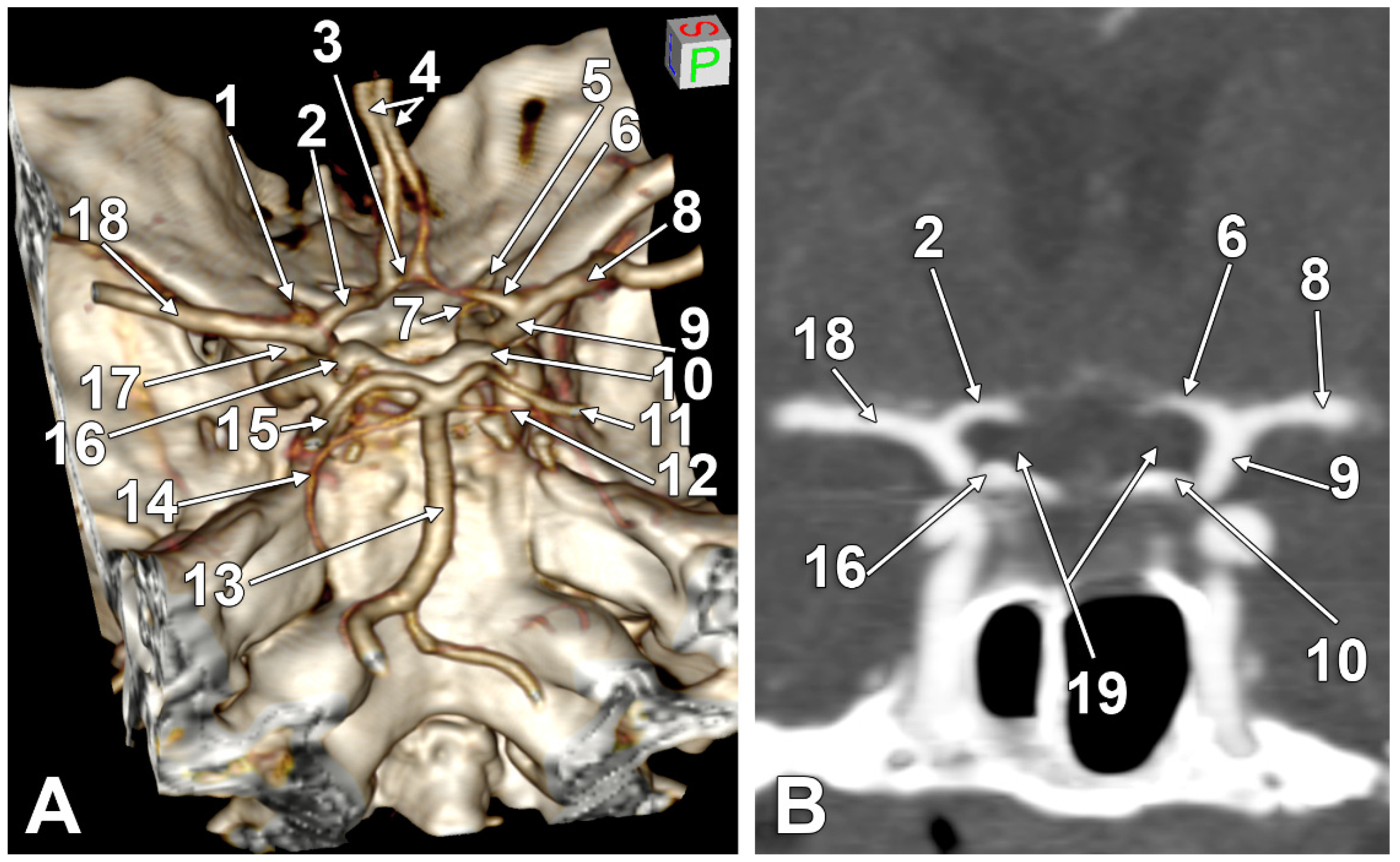
| M | type 2 IO A1 | type 1 IO A1 SCar | fenestrated AComA, hypoplastic left A1 | Figure 2A |
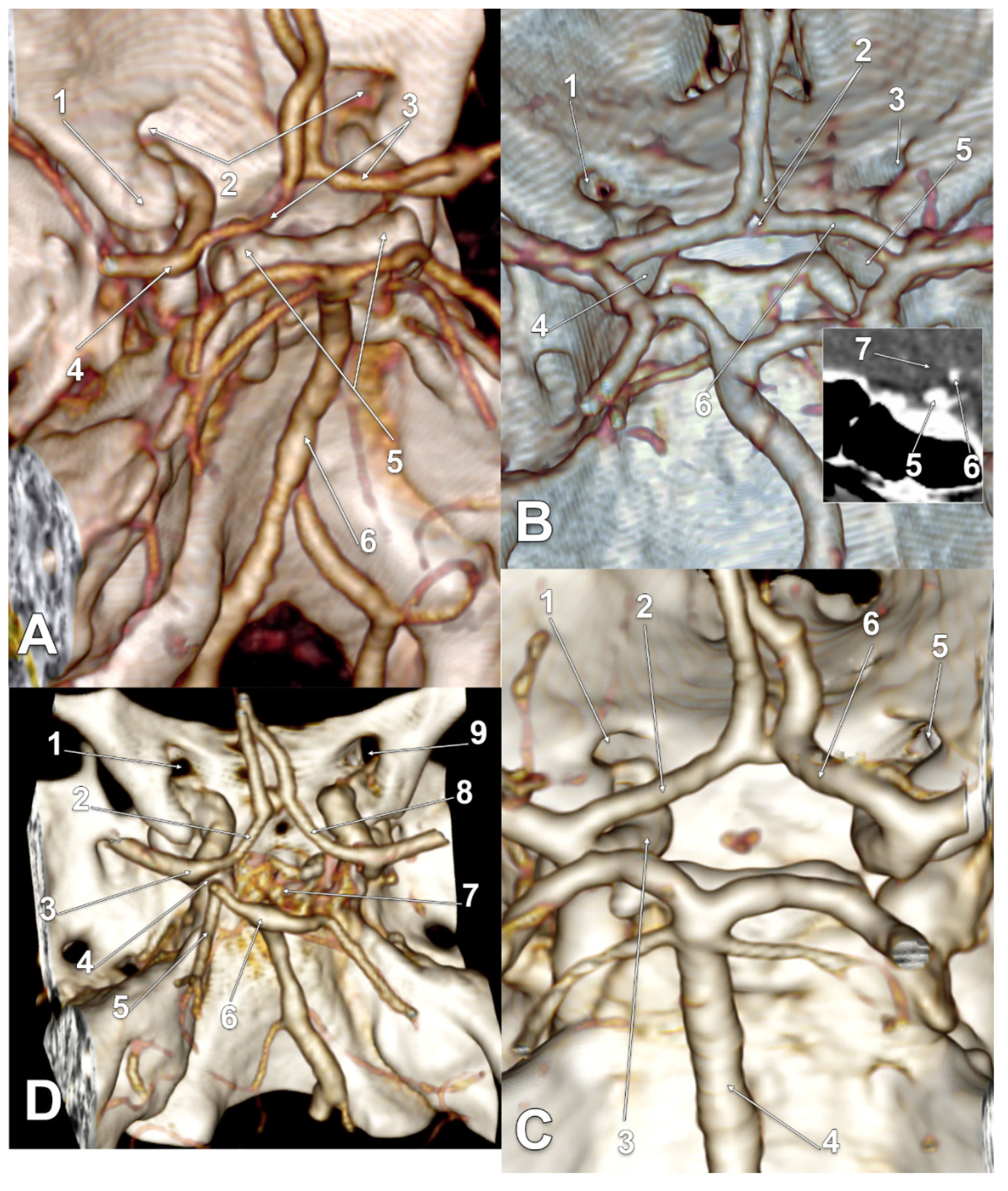
| M | type 2 IO A1 | type 2 IO A1 SCar | Figure 4C | |
| M | type 2 IO A1 | type 2 IO A1 | Figure 4A | |
| M | type 2 IO A1 | type 2 IO A1 | – | |
| M | type 2 IO A1 | type 2 IO A1 | – | |
| M | type 2 IO A1 | type 2 IO A1 | – | |
| M | type 2 IO A1 | type 2 IO A1 | Figure 5B | |
| M | type 2 IO A1 | type 2 IO A1 | – | |
| M | type 2 IO A1 | type 2 IO A1 | – | |
| M | type 2 IO A1 | type 2 IO A1 | – | |
| F | type 2 IO A1 | type 2 IO A1 | rotated BA, left PCA displaced towards the ipsilateral A1 ACA | Figure 4D |
| F | type 2 IO A1 | type 2 IO A1 | duplicated AComA | Figure 4B |
| F | type 2 IO A1 SCar SClin | type 1 IO A1 | supraclinoid right A1 | Figure 2C |
| F | type 2 IO A1 | type 2 IO A1 | Figure 3D | |
| F | type 2 IO A1 | type 2 IO A1 | Figure 3B,C | |
| F | type 2 IO A1 | type 2 IO A1 | hypoplastic right A1 | |
| F | type 2 IO A1 SCar | type 2 IO A1 SCar | rotated AComA, hypoplastic right A1 | Figure 5A |
| F | type 2 IO A1 | type 2 IO A1 | rotated BA, left PCA displaced towards the ipsilateral A1 ACA | Figure 5C |
| F | type 1 IO A1 | type 2 IO A1 | left bihemispheric ACA | Figure 2B |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mincă, D.I.; Rusu, M.C.; Rădoi, P.M.; Vrapciu, A.D.; Hostiuc, S.; Toader, C. The Infraoptic or Infrachiasmatic Course of the Anterior Cerebral Artery Emerging an Elongated Internal Carotid Artery. Tomography 2022, 8, 2243-2255. https://doi.org/10.3390/tomography8050188
Mincă DI, Rusu MC, Rădoi PM, Vrapciu AD, Hostiuc S, Toader C. The Infraoptic or Infrachiasmatic Course of the Anterior Cerebral Artery Emerging an Elongated Internal Carotid Artery. Tomography. 2022; 8(5):2243-2255. https://doi.org/10.3390/tomography8050188
Chicago/Turabian StyleMincă, Dragoş Ionuţ, Mugurel Constantin Rusu, Petrinel Mugurel Rădoi, Alexandra Diana Vrapciu, Sorin Hostiuc, and Corneliu Toader. 2022. "The Infraoptic or Infrachiasmatic Course of the Anterior Cerebral Artery Emerging an Elongated Internal Carotid Artery" Tomography 8, no. 5: 2243-2255. https://doi.org/10.3390/tomography8050188
APA StyleMincă, D. I., Rusu, M. C., Rădoi, P. M., Vrapciu, A. D., Hostiuc, S., & Toader, C. (2022). The Infraoptic or Infrachiasmatic Course of the Anterior Cerebral Artery Emerging an Elongated Internal Carotid Artery. Tomography, 8(5), 2243-2255. https://doi.org/10.3390/tomography8050188