
Predictors of Metastatic Lymph Nodes at Preoperative Staging CT in Gastric Adenocarcinoma

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
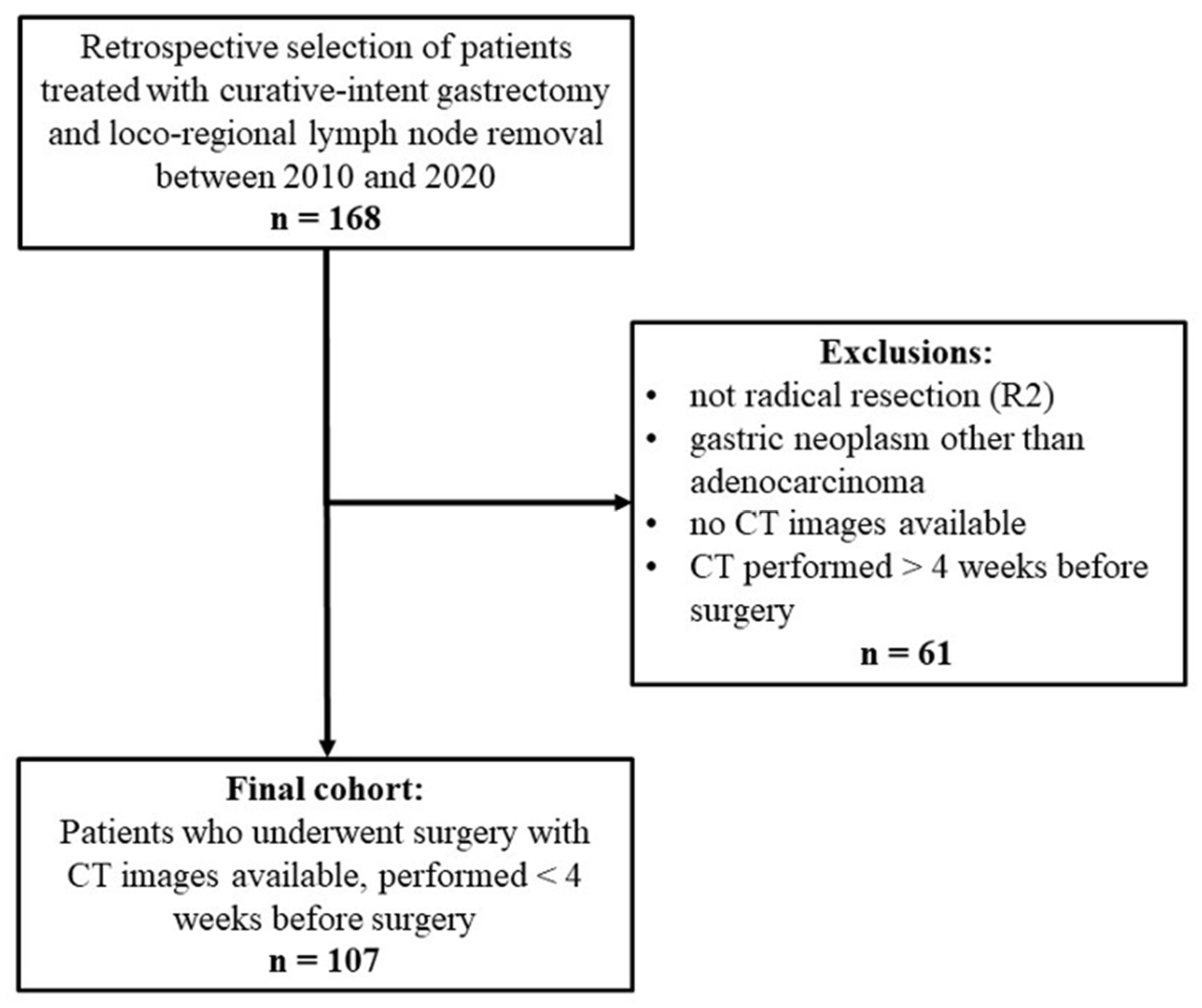
2.1. Patient Selection and Definition of Outcomes
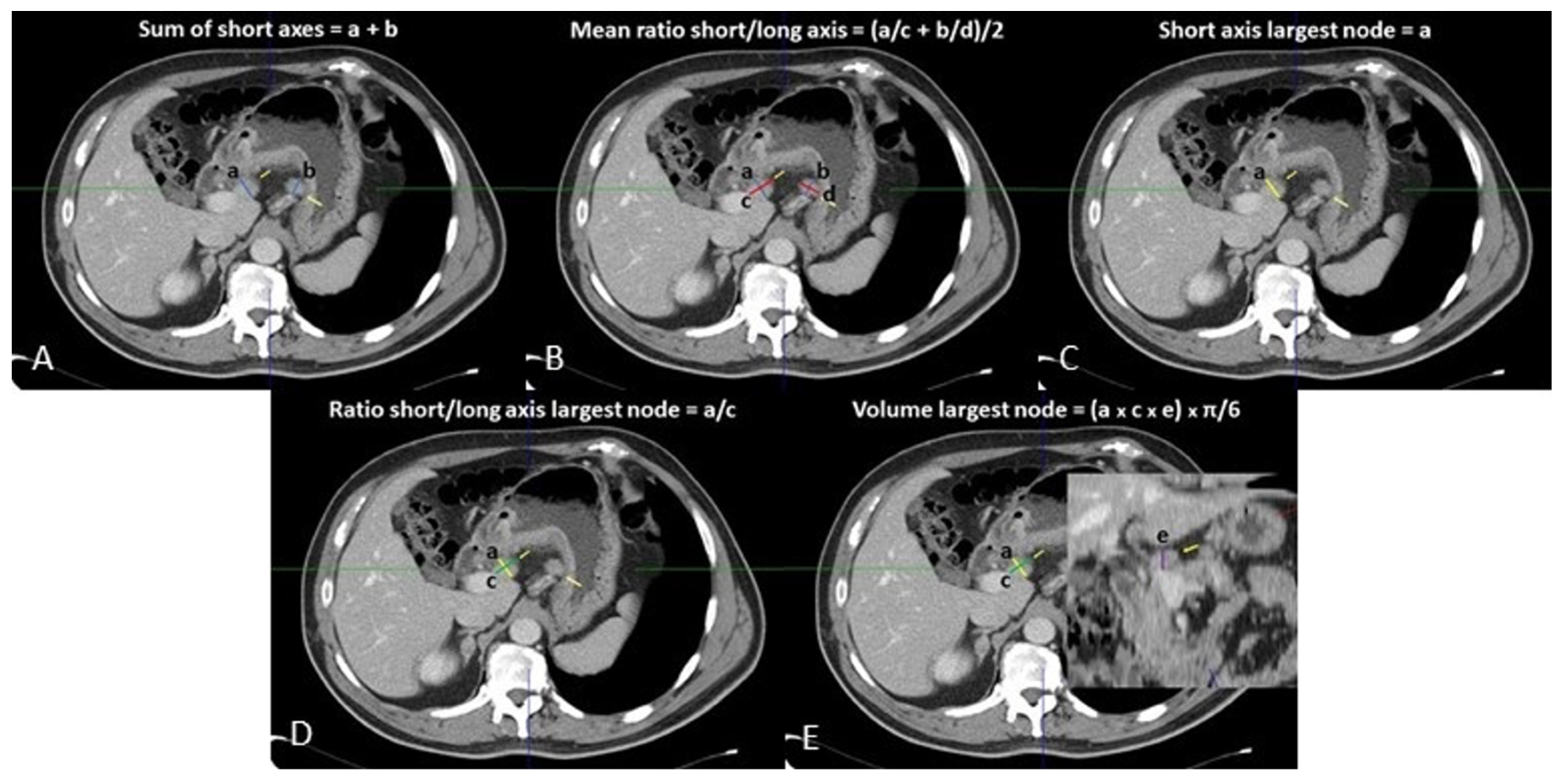
2.2. Radiological Analysis
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Radiological Results
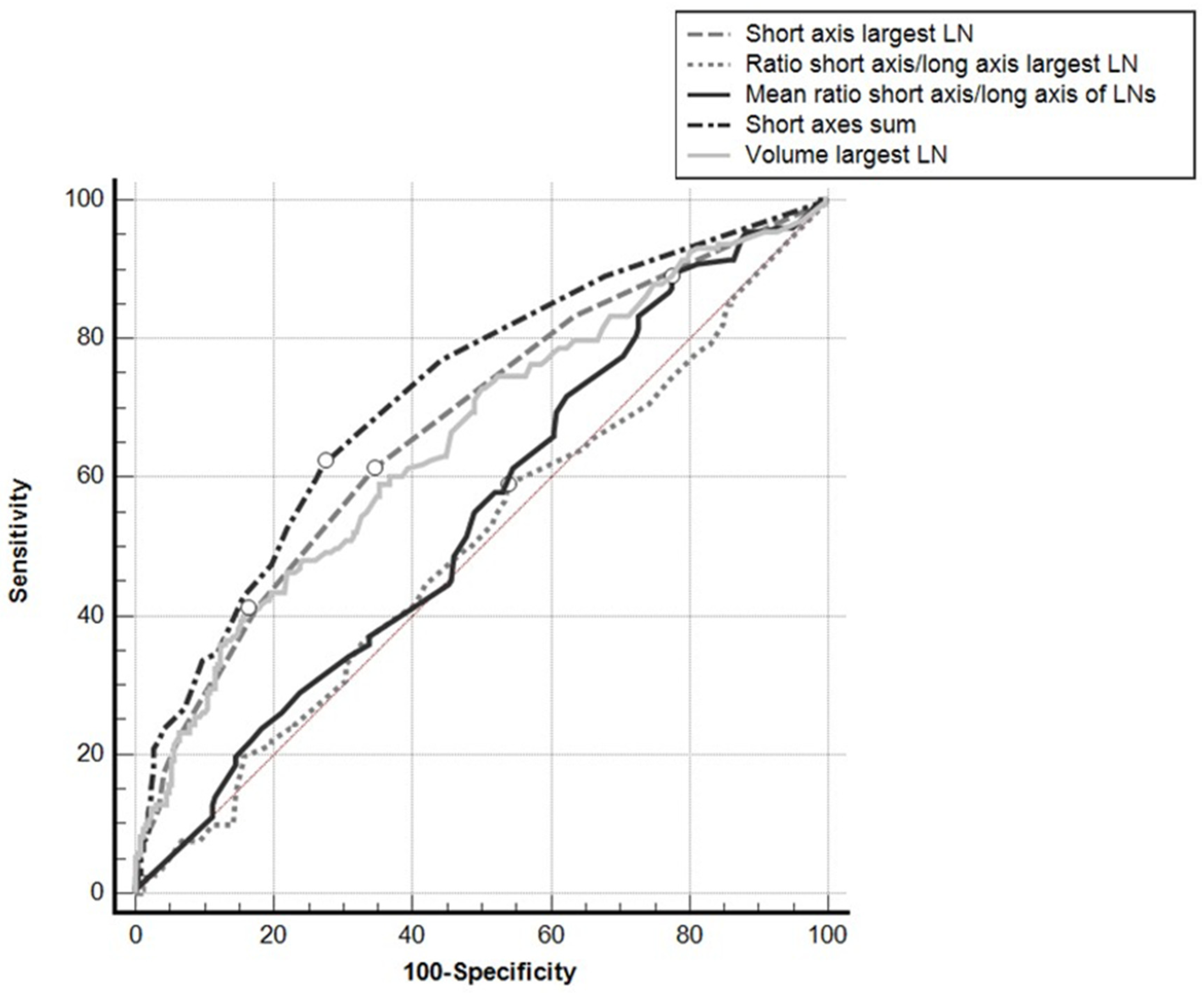
3.3. Analysis by Nodal Group
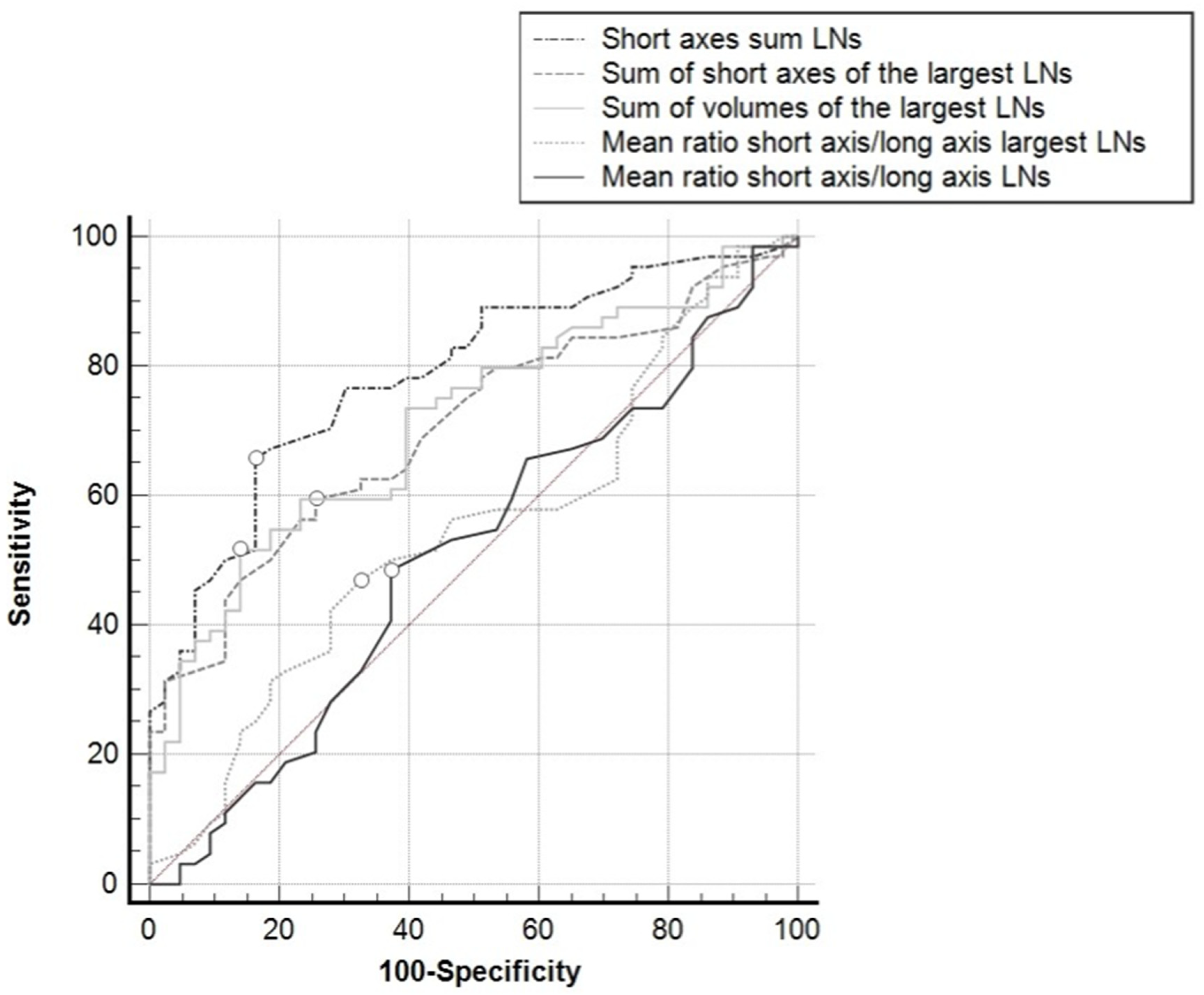
3.4. Patient-Based Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Tonello, A.S.; Capelli, G.; Bao, Q.R.; Marchet, A.; Farinati, F.; Pawlik, T.M.; Gregori, D.; Pucciarelli, S.; Spolverato, G. A nomogram to predict overall survival and disease-free survival after curative-intent gastrectomy for gastric cancer. Updates Surg. 2021, 73, 1879–1890. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Ejaz, A.; Kim, Y.; Squires, M.H.; Poultsides, G.A.; Fields, R.C.; Schmidt, C.; Weber, S.M.; Votanopoulos, K.; Maithel, S.K.; et al. Rates and patterns of recurrence after curative intent resection for gastric cancer: A United States multi-institutional analysis. J. Am. Coll. Surg. 2014, 219, 664–675. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Ejaz, A.; Spolverato, G.; Squires, M.H.; Poultsides, G.; Fields, R.C.; Bloomston, M.; Weber, S.M.; Votanopoulos, K.; Acher, A.W.; et al. Conditional survival after surgical resection of gastric cancer: A multi-institutional analysis of the us gastric cancer collaborative. Ann. Surg. Oncol. 2015, 22, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Randle, R.W.; Swords, D.S.; Levine, E.A.; Fino, N.F.; Squires, M.H.; Poultsides, G.; Fields, R.C.; Bloomston, M.; Weber, S.M.; Pawlik, T.M.; et al. Optimal extent of lymphadenectomy for gastric adenocarcinoma: A 7-institution study of the U.S. gastric cancer collaborative. J. Surg. Oncol. 2016, 113, 750–755. [Google Scholar] [CrossRef] [Green Version]
- Songun, I.; Putter, H.; Kranenbarg, E.M.-K.; Sasako, M.; van de Velde, C.J.H. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010, 11, 439–449. [Google Scholar] [CrossRef]
- Degiuli, M.; Sasako, M.; Ponti, A.; Vendrame, A.; Tomatis, M.; Mazza, C.; Borasi, A.; Capussotti, L.; Fronda, G.; Morino, M. Randomized clinical trial comparing survival after D1 or D2 gastrectomy for gastric cancer. Br. J. Surg. 2014, 101, 23–31. [Google Scholar] [CrossRef]
- Sasako, M.; Sano, T.; Yamamoto, S.; Kurokawa, Y.; Nashimoto, A.; Kurita, A.; Hiratsuka, M.; Tsujinaka, T.; Kinoshita, T.; Arai, K.; et al. D2 lymphadenectomy alone or with para-aortic nodal dissection for gastric cancer. N. Engl. J. Med. 2008, 359, 453–462. [Google Scholar] [CrossRef]
- Macdonald, J.S.; Smalley, S.R.; Benedetti, J.; Hundahl, S.A.; Estes, N.C.; Stemmermann, G.N.; Haller, D.G.; Ajani, J.A.; Gunderson, L.L.; Jessup, J.M.; et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N. Engl. J. Med. 2001, 345, 725–730. [Google Scholar] [CrossRef]
- Stahl, M.; Walz, M.K.; Stuschke, M.; Lehmann, N.; Meyer, H.J.; Riera-Knorrenschild, J.; Langer, P.; Engenhart-Cabillic, R.; Bitzer, M.; Königsrainer, A.; et al. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J. Clin. Oncol. 2009, 27, 851–856. [Google Scholar] [CrossRef] [Green Version]
- Ajani, J.A.; Mansfield, P.F.; Janjan, N.; Morris, J.; Pisters, P.W.; Lynch, P.M.; Feig, B.; Myerson, R.; Nivers, R.; Cohen, D.S.; et al. Multi-institutional trial of preoperative chemoradiotherapy in patients with potentially resectable gastric carcinoma. J. Clin. Oncol. 2004, 22, 2774–2780. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.D.; Schwarz, R.R.; Schwarz, R.E. Impact of total lymph node count on staging and survival after gastrectomy for gastric cancer: Data from a large US-population database. J. Clin. Oncol. 2005, 23, 7114–7124. [Google Scholar] [CrossRef] [PubMed]
- Yokota, T.; Ishiyama, S.; Saito, T.; Teshima, S.; Narushima, Y.; Murata, K.; Iwamoto, K.; Yashima, R.; Yamauchi, H.; Kikuchi, S. Lymph node metastasis as a significant prognostic factor in gastric cancer: A multiple logistic regression analysis. Scand. J. Gastroenterol. 2004, 39, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Ejaz, A.; Kim, Y.; Squires, M.H.; Poultsides, G.; Fields, R.C.; Bloomston, M.; Weber, S.M.; Votanopoulos, K.; Acher, A.W.; et al. Prognostic Performance of Different Lymph Node Staging Systems after Curative Intent Resection for Gastric Adenocarcinoma. Ann. Surg. 2015, 262, 991–998. [Google Scholar] [CrossRef]
- Gholami, S.; Janson, L.; Worhunsky, D.J.; Tran, T.B.; Squires, M.H., 3rd; Jin, L.X.; Spolverato, G.; Votanopoulos, K.I.; Schmidt, C.; Weber, S.M.; et al. Number of Lymph Nodes Removed and Survival after Gastric Cancer Resection: An Analysis from the US Gastric Cancer Collaborative. J. Am. Coll. Surg. 2015, 221, 291–299. [Google Scholar] [CrossRef] [Green Version]
- National Comprehensive Cancer Network. Gastric Cancer Version 3. 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf (accessed on 15 October 2021).
- Kwee, R.M.; Kwee, T.C. Imaging in local staging of gastric cancer: A systematic review. J. Clin. Oncol. 2007, 25, 2107–2116. [Google Scholar] [CrossRef]
- Spolverato, G.; Ejaz, A.; Kim, Y.; Squires, M.H.; Poultsides, G.A.; Fields, R.C.; Schmidt, C.; Weber, S.M.; Votanopoulos, K.; Maithel, S.K.; et al. Use of endoscopic ultrasound in the preoperative staging of gastric cancer: A multi-institutional study of the US gastric cancer collaborative. J. Am. Coll. Surg. 2015, 220, 48–56. [Google Scholar] [CrossRef]
- Cardoso, R.; Coburn, N.; Seevaratnam, R.; Sutradhar, R.; Lourenco, L.G.; Mahar, A.; Law, C.; Yong, E.; Tinmouth, J. A systematic review and meta-analysis of the utility of EUS for preoperative staging for gastric cancer. Gastric Cancer 2012, 15 (Suppl. 1), S19–S26. [Google Scholar] [CrossRef] [Green Version]
- Dai, C.L.; Yang, Z.G.; Xue, L.P.; Li, Y.M. Application value of multi-slice spiral computed tomography for imaging determination of metastatic lymph nodes of gastric cancer. World J. Gastroenterol. 2013, 19, 5732–5737. [Google Scholar] [CrossRef]
- You, J.M.; Kim, T.U.; Kim, S.; Lee, N.K.; Lee, J.W.; Ryu, H.; Kim, J.H.; Hong, S.B.; Jeon, T.Y.; Park, D.Y. Preoperative N stage evaluation in advanced gastric cancer patients using multidetector CT: Can the sum of the diameters of metastatic LNs be used for N stage evaluation? Clin. Radiol. 2019, 74, 782–789. [Google Scholar] [CrossRef]
- Saito, T.; Kurokawa, Y.; Takiguchi, S.; Miyazaki, Y.; Takahashi, T.; Yamasaki, M.; Miyata, H.; Nakajima, K.; Mori, M.; Doki, Y. Accuracy of multidetector-row CT in diagnosing lymph node metastasis in patients with gastric cancer. Eur. Radiol. 2015, 25, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Komatsu, S.; Ichikawa, D.; Kosuga, T.; Kubota, T.; Okamoto, K.; Konishi, H.; Shiozaki, A.; Fujiwara, H.; Otsuji, E. Clinical significance and prognostic impact of the total diameter of enlarged lymph nodes on preoperative multidetector computed tomography in patients with gastric cancer. J. Gastroenterol. Hepatol. 2015, 30, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Itabashi, M.; Shimada, Y.; Tanaka, S.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hyodo, I.; Igarashi, M.; Ishida, H.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2014 for treatment of colorectal cancer. Int. J. Clin. Oncol. 2015, 20, 207–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C. AJCC Cancer Staging Manual; Springer: New York, NY, USA, 2017. [Google Scholar]
- AIOM. Linee Guida Neoplasie Dello Stomaco e Della Giunzione Gastro-Esofagea. 2019. Available online: https://www.aiom.it/wp-content/uploads/2019/10/2019_LG_AIOM_Stomaco_giun-gastr-esof.pdf (accessed on 15 October 2021).
- Coccolini, F.; Nardi, M.; Montori, G.; Ceresoli, M.; Celotti, A.; Cascinu, S.; Fugazzola, P.; Tomasoni, M.; Glehen, O.; Catena, F.; et al. Neoadjuvant chemotherapy in advanced gastric and esophago-gastric cancer. Meta-analysis of randomized trials. Int. J. Surg. 2018, 51, 120–127. [Google Scholar] [CrossRef]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Bhandari, S.; Shim, C.S.; Kim, J.H.; Jung, I.S.; Cho, J.Y.; Lee, J.S.; Lee, M.S.; Kim, B.S. Usefulness of three-dimensional, multidetector row CT (virtual gastroscopy and multiplanar reconstruction) in the evaluation of gastric cancer: A comparison with conventional endoscopy, EUS, and histopathology. Gastrointest. Endosc. 2004, 59, 619–626. [Google Scholar] [CrossRef]
- Chen, C.Y.; Hsu, J.S.; Wu, D.C.; Kang, W.Y.; Hsieh, J.S.; Jaw, T.S.; Wu, M.T.; Liu, G.C. Gastric cancer: Preoperative local staging with 3D multi-detector row CT—Correlation with surgical and histopathologic results. Radiology 2007, 242, 472–482. [Google Scholar] [CrossRef]
- Wang, Z.L.; Zhang, X.P.; Tang, L.; Li, X.T.; Wu, Y.; Sun, Y.S. Lymph nodes metastasis of gastric cancer: Measurement with multidetector CT oblique multiplanar reformation-correlation with histopathologic results. Medicine 2016, 95, e5042. [Google Scholar] [CrossRef]
- Hasegawa, S.; Yoshikawa, T.; Shirai, J.; Fujikawa, H.; Cho, H.; Doiuchi, T.; Yoshida, T.; Sato, T.; Oshima, T.; Yukawa, N.; et al. A prospective validation study to diagnose serosal invasion and nodal metastases of gastric cancer by multidetector-row CT. Ann. Surg. Oncol. 2013, 20, 2016–2022. [Google Scholar] [CrossRef]
- Li, J.; Fang, M.; Wang, R.; Dong, D.; Tian, J.; Liang, P.; Liu, J.; Gao, J. Diagnostic accuracy of dual-energy CT-based nomograms to predict lymph node metastasis in gastric cancer. Eur. Radiol. 2018, 28, 5241–5249. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Suzuki, A.; Shiozaki, H.; Wada, T.; Kyosaka, T.; Kishida, A. Accuracy of Multidetector-Row Computed Tomography in the Preoperative Diagnosis of Lymph Node Metastasis in Patients with Gastric Cancer. Gastrointest. Tumors 2017, 3, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Polkowski, M.; Palucki, J.; Wronska, E.; Szawlowski, A.; Nasierowska-Guttmejer, A.; Butruk, E. Endosonography versus helical computed tomography for locoregional staging of gastric cancer. Endoscopy 2004, 36, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Gundogan, C.; Komek, H.; Can, C.; Yildirim, O.A.; Kaplan, I.; Erdur, E.; Poyraz, K.; Guzel, Y.; Oruc, Z.; Cakabay, B. Comparison of 18F-FDG PET/CT and 68Ga-FAPI-04 PET/CT in the staging and restaging of gastric adenocarcinoma. Nucl. Med. Commun. 2021, 43, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Li, J.; Xin, B.; Sun, Y.; Feng, D.; Fulham, M.J.; Wang, X.; Song, S. 18 F-FDG PET/CT Radiomics for Preoperative Prediction of Lymph Node Metastases and Nodal Staging in Gastric Cancer. Front. Oncol. 2021, 13, 723345. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhong, L.; Zhou, X.; Chen, D.; Li, R. Value of multiphase contrast-enhanced CT with three-dimensional reconstruction in detecting depth of infiltration, lymph node metastasis, and extramural vascular invasion of gastric cancer. J. Gastrointest. Oncol. 2021, 12, 1351–1362. [Google Scholar] [CrossRef]
- Yang, J.; Wu, Q.; Xu, L.; Wang, Z.; Su, K.; Liu, R.; Yen, E.A.; Liu, S.; Qin, J.; Rong, Y.; et al. Integrating tumor and nodal radiomics to predict lymph node metastasis in gastric cancer. Radiother. Oncol. 2020, 150, 89–96. [Google Scholar] [CrossRef]
- Gao, X.; Ma, T.; Cui, J.; Zhang, Y.; Wang, L.; Li, H.; Ye, Z. A radiomics-based model for prediction of lymph node metastasis in gastric cancer. Eur. J. Radiol. 2020, 129, 109069. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N (% or IQR) | |
|---|---|---|
| Age | Years, Median (IQR) | 72 (62–78) |
| Gender | Female | 40 (37.4) |
| Male | 67 (62.6) | |
| Preoperative CEA level | (>4 ug/L) | 9 (8.4) |
| BMI | kg/m2, Median (IQR) | 24.0 (22.4–27.2) |
| Tumor size | mm, Median (IQR) | 40 (25–60) |
| Tumor site | Cardia (Siewert III type) | 8 (7.4) |
| Fundus | 11 (10.3) | |
| Body | 34 (31.8) | |
| Antrum | 48 (44.9) | |
| Pylorus | 1 (0.9) | |
| Multicentric disease | 2 (1.9) | |
| Gastric remnant | 3 (2.8) | |
| Type of surgical resection | Subtotal gastrectomy | 44 (41.1) |
| Total gastrectomy | 44 (41.1) | |
| Extended total gastrectomy | 11 (10.3) | |
| Remnant gastrectomy | 3 (2.8) | |
| Proximal gastrectomy | 0 (0) | |
| Esophageal resection | 3 (2.8) | |
| Multivisceral resections | 1 (0.9) | |
| Extent of lymphadenectomy | D1 | 31 (29.2) |
| D2 | 76 (71.7) | |
| Preoperative treatment | Chemotherapy | 15 (14.0) |
| Radiotherapy | 3 (2.8) | |
| Adjuvant treatment | Chemotherapy | 67 (62.6) |
| Radiotherapy | 8 (7.5) | |
| Length of hospital stay in days, median (IQR) | 11 (10–13) | |
| Postoperative complications | 48 (44.9) | |
| Clavien–Dindo classification | grade 0–2 | 94 (87.9) |
| grade 3–5 | 13 (12.1) | |
| Deep abdominal collections | 18 (16.8) | |
| Bleeding requiring transfusions | 15 (14.0) | |
| Anastomotic leakage | 5 (4.7) |
| Variables | N (% or IQR) | |
|---|---|---|
| Histotype | Tubular | 42 (39.3) |
| Poorly cohesive (NOS or SRC) | 39 (36.4) | |
| Other types | 26 (24.3) | |
| Lauren’s classification | Mixed | 2 (1.9) |
| Intestinal | 43 (40.2) | |
| Diffuse | 48 (44.9) | |
| NA | 12 (11.2) | |
| Histological grade (n = 144) | G1–G2 | 33 (30.8) |
| G3 | 53 (49.5) | |
| NA | 21 (19.6) | |
| T stage | T1 | 18 (16.8) |
| T2 | 12 (11.2) | |
| T3 | 32 (29.9) | |
| T4 | 45 (42.1) | |
| N stage | N0 | 38 (35.5) |
| N1 | 14 (13.1) | |
| N2 | 14 (13.1) | |
| N3a | 21 (19.6) | |
| N3b | 20 (18.7) | |
| M stage | M1 | 15 (14.0) |
| TNM stage | Stage I | 24 (22.4) |
| Stage II | 25 (23.4) | |
| Stage III | 43 (40.2) | |
| Stage IV | 15 (14.0) | |
| Total number of nodes examined | median (IQR) | 30 (22.5–44) |
| Lymph node ratio | median (IQR) | 0.12 (0–0.47) |
| Lymphatic invasion | 75 (70.1) | |
| NA | 6 (5.6) | |
| Vascular invasion | 47 (43.9) | |
| NA | 6 (5.6) | |
| Radicality | R0 | 88 (82.2) |
| R1 | 19 (17.8) |
| Parameters | Metastatic Nodal Groups | Nonmetastatic Nodal Groups | p Value * |
|---|---|---|---|
| Short axis of the largest lymph node in the nodal group | 7 mm (IQR: 6–9 mm) | 6 mm (IQR: 5–7 mm) | <0.0001 |
| Ratio of the short axis to the long axis of the largest lymph node in the nodal group | 0.78 (IQR: 0.67–0.88) | 0.78 (IQR: 0.67–0.87) | 0.8926 |
| Mean of the ratios of the short axis to the long axis of all lymph nodes in the nodal group | 0.80 (IQR: 0.71–0.88) | 0.78 (IQR: 0.67–0.86) | 0.0969 |
| Sum of the short axes of all the lymph nodes in the nodal group | 11 mm (IQR: 7–17 mm) | 6 mm (IQR: 5–10 mm) | <0.0001 |
| Volume of the largest lymph node in the nodal group | 280.8 mm3 (IQR: 174.7–624.0 mm3) | 195.8 mm3 (IQR: 130.0–305.7 mm3) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crimì, F.; Bao, Q.R.; Mari, V.; Zanon, C.; Cabrelle, G.; Spolverato, G.; Pucciarelli, S.; Quaia, E. Predictors of Metastatic Lymph Nodes at Preoperative Staging CT in Gastric Adenocarcinoma. Tomography 2022, 8, 1196-1207. https://doi.org/10.3390/tomography8030098
Crimì F, Bao QR, Mari V, Zanon C, Cabrelle G, Spolverato G, Pucciarelli S, Quaia E. Predictors of Metastatic Lymph Nodes at Preoperative Staging CT in Gastric Adenocarcinoma. Tomography. 2022; 8(3):1196-1207. https://doi.org/10.3390/tomography8030098
Chicago/Turabian StyleCrimì, Filippo, Quoc Riccardo Bao, Valentina Mari, Chiara Zanon, Giulio Cabrelle, Gaya Spolverato, Salvatore Pucciarelli, and Emilio Quaia. 2022. "Predictors of Metastatic Lymph Nodes at Preoperative Staging CT in Gastric Adenocarcinoma" Tomography 8, no. 3: 1196-1207. https://doi.org/10.3390/tomography8030098
APA StyleCrimì, F., Bao, Q. R., Mari, V., Zanon, C., Cabrelle, G., Spolverato, G., Pucciarelli, S., & Quaia, E. (2022). Predictors of Metastatic Lymph Nodes at Preoperative Staging CT in Gastric Adenocarcinoma. Tomography, 8(3), 1196-1207. https://doi.org/10.3390/tomography8030098