
High-Resolution Vessel Wall MRI of Endovascularly Treated Intracranial Aneurysms


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. HR-VW MRI Protocol
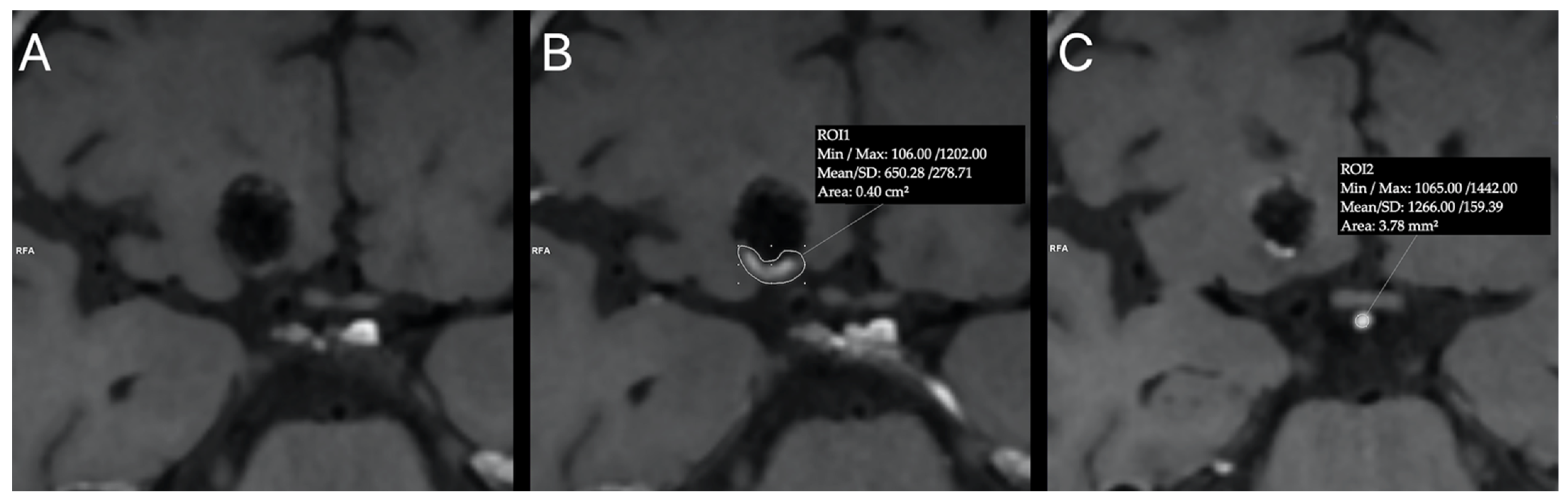
2.3. HR-VW MRI Analysis
2.4. Post-Procedural Angiographic Findings
2.5. Statistical Analysis
3. Results
3.1. Patients and Aneurysms Characteristics
3.2. Procedural Details and Immediate Angiographic Outcome
3.3. Follow-Up MR Angiography
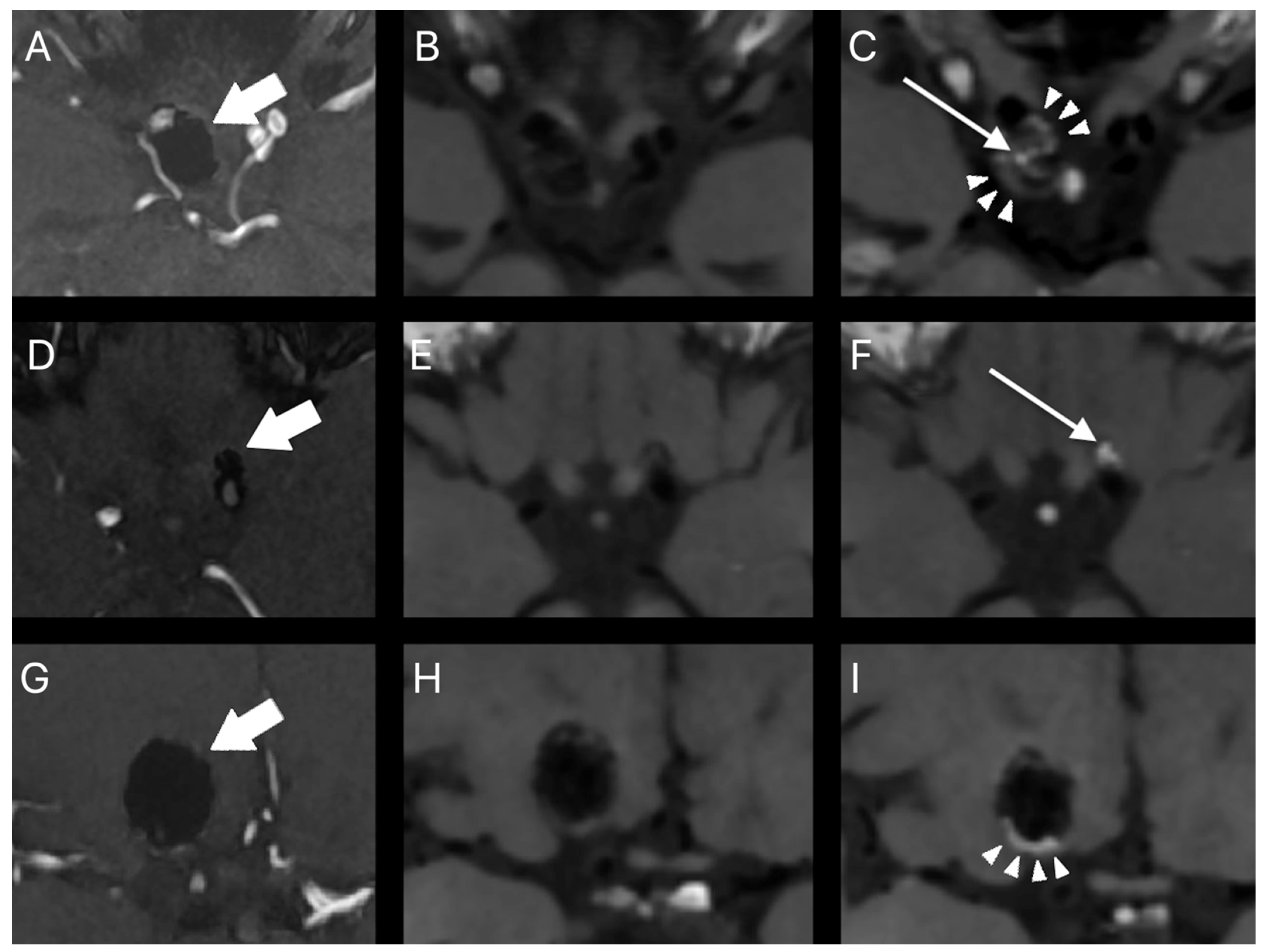
3.4. Post-Procedural Aneurysm Contrast Enhancement on HR-VW MRI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferns, S.P.; Sprengers, M.E.S.; van Rooij, W.J.; Rinkel, G.J.E.; van Rijn, J.C.; Bipat, S.; Sluzewski, M.; Majoie, C.B.L.M. Coiling of intracranial aneurysms: A systematic review on initial occlusion and reopening and retreatment rates. Stroke 2009, 40, e523–e529. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Velthuis, B.K.; Majoie, C.B.L.M.; van der Berg, R.; Brouwer, P.A.; Barkhof, F.; Eshghi, O.; de Kort, G.A.P.; Lo, R.T.H.; Witkamp, T.D.; et al. Intracranial Aneurysms Treated with Coil Placement: Test Characteristics of Follow-up MR Angiography—Multicenter Study. Radiology 2010, 256, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandell, D.; Mossa-Basha, M.; Qiao, Y.; Hess, C.P.; Hui, F.; Matouk, C.C.; Johnson, M.; Daemen, M.J.; Vossough, A.; Edjlali, M.; et al. Intracranial Vessel Wall MRI: Principles and Expert Consensus Recommendations of the American Society of Neuroradiology. Am. J. Neuroradiol. 2016, 38, 218–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matouk, C.C.; Mandell, D.M.; Günel, M.; Bulsara, K.R.; Malhotra, A.; Heber, R.; Johnson, M.H.; Mikulis, D.J.; Minja, F. Vessel wall magnetic resonance imaging identifies the site of rupture in patients with multiple intracranial aneurysms: Proof of principle. Neurosurgery 2013, 72, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Matsushige, T.; Shimonaga, K.; Mizoue, T.; Hosogai, M.; Hashimoto, Y.; Kaneko, M.; Ono, C.; Ishii, D.; Sakamoto, S.; Kurisu, K. Focal Aneurysm Wall Enhancement on Magnetic Resonance Imaging Indicates Intraluminal Thrombus and the Rupture Point. World Neurosurg. 2019, 127, e578–e584. [Google Scholar] [CrossRef]
- Nagahata, S.; Nagahata, M.; Obara, M.; Minagawa, N.; Sato, S.; Sato, S.; Mouri, W.; Saito, S.; Kayama, T. Wall Enhancement of theIntracranial Aneurysms Revealed by Magnetic Resonance Vessel Wall Imaging Using Three-Dimensional Turbo Spin-Echo Sequence with Motion-Sensitized Driven-Equilibrium: A Sign of Ruptured Aneurysm? Clin. Neuroradiol. 2016, 26, 277–283. [Google Scholar] [CrossRef]
- Omodaka, S.; Endo, H.; Niizuma, K.; Fujimura, M.; Endo, T.; Sato, K.; Sugiyama, S.I.; Inoue, T.; Tominaga, T. Circumferential Wall Enhancement on Magnetic Resonance Imaging is Useful to Identify Rupture Site in Patients with Multiple Cerebral Aneurysms. Neurosurgery 2018, 82, 638–644. [Google Scholar] [CrossRef]
- Wang, G.X.; Wen, L.; Lei, S.; Ran, Q.; Yin, J.B.; Gong, Z.L.; Zhang, D. Wall enhancement ratio and partial wall enhancement on MRI associated with the rupture of intracranial aneurysms. J. Neurointerv. Surg. 2018, 10, 566–570. [Google Scholar] [CrossRef]
- Edjlali, M.; Gentric, J.C.; Régent-Rodriguez, C.; Trystram, D.; Hassen, W.B.; Lion, S.; Nataf, F.; Raymond, J.; Wieben, O.; Turski, P.; et al. Does aneurysmal wall enhancement on vessel wall MRI help to distinguish stable from unstable intracranial aneurysms? Stroke 2014, 45, 3704–3706. [Google Scholar] [CrossRef] [Green Version]
- Edjlali, M.; Guédon, A.; Ben Hassen, W.; Boulouis, G.; Benzakoun, J.; Rodriguez-Régent, C.; Trystram, D.; Nataf, F.; Meder, J.-F.; Turski, P.; et al. Circumferential Thick Enhancement at Vessel Wall MRI Has High Specificity for Intracranial Aneurysm Instability. Radiology 2018, 289, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Hu, P.; Yang, Q.; Wang, D.-D.; Guan, S.-C.; Zhang, H.-Q. Wall enhancement on high-resolution magnetic resonance imaging may predict an unsteady state of an intracranial saccular aneurysm. Neuroradiology 2016, 58, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.; von der Brelie, C.; Trick, D.; Riedel, C.; Lindner, T.; Madjidyar, J.; Jansen, O.; Synowitz, M.; Flüh, C. Vessel Wall Enhancement in Unruptured Intracranial Aneurysms: An Indicator for Higher Risk of Rupture? High-Resolution MR Imaging and Correlated Histologic Findings. Am. J. Neuroradiol. 2018, 39, 1617–1621. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.S.; Zanaty, M.; Nakagawa, D.; Kung, D.K.; Jabbour, P.; Samaniego, E.A.; Hasan, D. Magnetic Resonance Vessel Wall Imaging in Human Intracranial Aneurysms. Stroke 2019, 50, e1. [Google Scholar] [CrossRef] [PubMed]
- Quan, K.; Song, J.; Yang, Z.; Wang, D.; An, Q.; Huang, L.; Liu, P.; Li, P.; Tian, Y.; Zhou, L.; et al. Validation of Wall Enhancement as a New Imaging Biomarker of Unruptured Cerebral Aneurysm. Stroke 2019, 50, 1570–1573. [Google Scholar] [CrossRef]
- Backes, D.; Hendrikse, J.; van der Schaaf, I.; Algra, A.; Lindgren, A.; Verweij, B.H.; Rinkel, G.J.E.; Vergouwen, M.D.I. Determinants of Gadolinium-Enhancement of the Aneurysm Wall in Unruptured Intracranial Aneurysms. Neurosurgery 2017, 83, 719–725. [Google Scholar] [CrossRef]
- Liu, P.; Qi, H.; Liu, A.; Lv, X.; Jiang, Y.; Zhao, X.; Li, R.; Lu, B.; Lv, M.; Chen, H.; et al. Relationship between aneurysm wall enhancement and conventional risk factors in patients with unruptured intracranial aneurysms: A black-blood MRI study. Interv. Neuroradiol. 2016, 22, 501–505. [Google Scholar] [CrossRef] [Green Version]
- Lv, N.; Karmonik, C.; Chen, S.; Wang, X.; Fang, Y.; Huang, Q.; Liu, J. Relationship Between Aneurysm Wall Enhancement in Vessel Wall Magnetic Resonance Imaging and Rupture Risk of Unruptured Intracranial Aneurysms. Neurosurgery 2018, 84, E385–E391. [Google Scholar] [CrossRef]
- Larsen, N.; Flüh, C.; Saalfeld, S.; Voß, S.; Hille, G.; Trick, D.; Wodarg, F.; Synowitz, M.; Jansen, O.; Berg, P. Multimodal validation of focal enhancement in intracranial aneurysms as a surrogate marker for aneurysm instability. Neuroradiology 2020, 62, 1627–1635. [Google Scholar] [CrossRef]
- Khan, M.O.; Arana, V.T.; Rubbert, C.; Cornelius, J.F.; Fischer, I.; Bostelmann, R.; Mijderwijk, H.-J.; Turowski, B.; Steiger, H.-J.; May, R.; et al. Association between aneurysm hemodynamics and wall enhancement on 3D vessel wall MRI. J. Neurosurg. 2020, 134, 565–575. [Google Scholar] [CrossRef]
- Fu, Q.; Guan, S.; Liu, C.; Wang, K.; Cheng, J. Clinical Significance of Circumferential Aneurysmal Wall Enhancement in Symptomatic Patients with Unruptured Intracranial Aneurysms: A High-resolution MRI Study. Clin. Neuroradiol. 2017, 28, 509–514. [Google Scholar] [CrossRef]
- Hartman, J.B.; Watase, H.; Sun, J.; Hippe, D.S.; Kim, L.; Levitt, M.; Sekhar, L.; Balu, N.; Hatsukami, T.; Yuan, C.; et al. Intracranial aneurysms at higher clinical risk for rupture demonstrate increased wall enhancement and thinning on multicontrast 3D vessel wall MRI. Br. J. Radiol. 2019, 92, 1096. [Google Scholar] [CrossRef] [PubMed]
- Vergouwen, M.; Backes, D.; van der Schaaf, I.; Hendrikse, J.; Kleinloog, R.; Algra, A.; Rinkel, G.J. Gadolinium Enhancement of the Aneurysm Wall in Unruptured Intracranial Aneurysms Is Associated with an Increased Risk of Aneurysm Instability: A Follow-Up Study. Am. J. Neuroradiol. 2019, 40, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Tian, B.; Toossi, S.; Eisenmenger, L.; Faraji, F.; Ballweber, M.K.; Josephson, S.A.; Haraldsson, H.; Zhu, C.; Ahn, S.; Laub, G.; et al. Visualizing wall enhancement over time in unruptured intracranial aneurysms using 3D vessel wall imaging. J. Magn. Reson. Imaging 2019, 50, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Larson, A.; Lehman, V.; Lanzino, G.; Brinjikji, W. Lack of Baseline Intracranial Aneurysm Wall Enhancement Predicts Future Stability: A Systematic Review and Meta-Analysis of Longitudinal Studies. Am. J. Neuroradiol. 2020, 41, 1606–1610. [Google Scholar] [CrossRef]
- Roa, J.A.; Zanaty, M.; Osorno-Cruz, C.; Ishii, D.; Bathla, G.; Ortega-Gutierrez, S.; Hasan, D.M.; Samaniego, E.A. Objective quantification of contrast enhancement of unruptured intracranial aneurysms: A high-resolution vessel wall imaging validation study. J. Neurosurg. 2020, 134, 862–869. [Google Scholar] [CrossRef]
- Omodaka, S.; Endo, H.; Niizuma, K.; Fujimura, M.; Inoue, T.; Sato, K.; Sugiyama, S.-I.; Tominaga, T. Quantitative Assessment of Circumferential Enhancement along the Wall of Cerebral Aneurysms Using MR Imaging. Am. J. Neuroradiol. 2016, 37, 1262–1266. [Google Scholar] [CrossRef] [Green Version]
- Zwarzany, Ł.; Tyburski, E.; Poncyljusz, W. High-Resolution Vessel Wall Magnetic Resonance Imaging of Small Unruptured Intracranial Aneurysms. J. Clin. Med. 2021, 10, 225. [Google Scholar] [CrossRef]
- Larsen, N.; Flüh, C.; Madjidyar, J.; Synowitz, M.; Jansen, O.; Wodarg, F. Visualization of Aneurysm Healing: Enhancement Patterns and Reperfusion in Intracranial Aneurysms after Embolization on 3T Vessel Wall MRI. Clin. Neuroradiol. 2020, 30, 811–815. [Google Scholar] [CrossRef]
- Elsheikh, S.; Urbach, H.; Meckel, S. Contrast Enhancement of Intracranial Aneurysms on 3T 3D Black-Blood MRI and Its Relationship to Aneurysm Recurrence following Endovascular Treatment. Am. J. Neuroradiol. 2020, 41, 495–500. [Google Scholar] [CrossRef]
- Songsaeng, D.; Sakarunchai, I.; Harmontree, S.; Mongkolnaowarat, S.; Charnchaowanish, P.; Zhang, S.; Krings, T. Black-blood vessel wall magnetic resonance imaging—A new imaging biomarker for regrowth of coiled saccular aneurysms? Interdiscip. Neurosurg. Adv. Tech. Case Manag. 2021, 23, 100920. [Google Scholar] [CrossRef]
- Roy, D.; Milot, G.; Raymond, J. Endovascular treatment of unruptured aneurysms. Stroke 2001, 32, 1998–2004. [Google Scholar] [CrossRef] [PubMed]
- Long, J.S. Regression Models for Categorical and Limited Dependent Variables; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 1996. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Ishihara, S.; Mawad, M.E.; Ogata, K.; Suzuki, C.; Tsuzuki, N.; Katoh, H.; Ohnuki, A.; Miyazawa, T.; Nawashiro, H.; Kaji, T.; et al. Histopathologic findings in human cerebral aneurysms embolized with platinum coils: Report of two cases and review of the literaturę. Am. J. Neuroradiol. 2002, 23, 970–974. [Google Scholar]
- Bavinzski, G.; Talazoglu, V.; Killer, M.; Richling, B.; Gruber, A.; Gross, C.E.; Plenk, H., Jr. Gross and microscopic histopathological findings in aneurysms of the human brain treated with Guglielmi detachable coils. J. Neurosurg. 1999, 91, 284–293. [Google Scholar] [CrossRef]
- Groden, C.; Hagel, C.; Delling, G.; Zeumer, H. Histological findings in ruptured aneurysms treated with GDcs: Six examples at varying times after treatment. Am. J. Neuroradiol. 2003, 24, 579–584. [Google Scholar]
- Stiver, S.I.; Porter, P.J.; Willinsky, R.A.; Wallace, M.C. Acute human histopathology of an intracranial aneurysm treated using Guglielmi detachable coils: Case report and review of the literature. Neurosurgery 1998, 43, 1203–1207. [Google Scholar] [CrossRef]
- Horowitz, M.B.; Purdy, P.D.; Burns, D.; Bellotto, D. Scanning electron microscopic findings in a basilar tip aneurysm embolized with Guglielmi detachable coils. Am. J. Neuroradiol. 1997, 18, 688–690. [Google Scholar]
- Shimizu, S.; Kurata, A.; Takano, M.; Takagi, H.; Yamazaki, H.; Miyasaka, Y.; Fujii, K. Tissue response of a small saccular aneurysm after incomplete occlusion with a Guglielmi detachable coil. Am. J. Neuroradiol. 1999, 20, 546–548. [Google Scholar]
- Szikora, I.; Seifert, P.; Hanzely, Z.; Kulcsar, Z.; Berentei, Z.; Marosfoi, M.; Czirjak, S.; Vajda, J.; Nyary, I. Histopathologic evaluation of aneurysms treated with Guglielmi detachable coils or matrix detachable microcoils. Am. J. Neuroradiol. 2006, 27, 283–288. [Google Scholar]
- Su, I.C.; Willinsky, R.A.; Fanning, N.F.; Agid, R. Aneurysmal wall enhancement and perianeurysmal edema after endovascular treatment of unruptured cerebral aneurysms. Neuroradiology 2014, 56, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Fanning, N.F.; Willinsky, R.A.; ter Brugge, K.G. Wall enhancement, edema, and hydrocephalus after endovascular coil occlusion of intradural cerebral aneurysms. J. Neurosurg. 2008, 108, 1074–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehman, V.T.; Brinjikji, W.; Mossa-Basha, M.M.; Lanzino, G.; Rabinstein, A.A.; Kallmes, D.F.; Huston, J. Conventional and high-resolution vessel wall MRI of intracranial aneurysms: Current concepts and new horizons. J. Neurosurg. 2018, 128, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, D.G.; Cadete, R.A.; Hygino da Cruz, L.C. Vessel Wall Enhancement in Treated Unruptured Aneurysms. Am. J. Neuroradiol. 2018, 39, E129–E130. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Ahmed, S.U.; Mocco, J.; Zhang, X.; Kelly, M.; Doshi, A.; Nael, K.; De Leacy, R. MRA versus DSA for the follow-up imaging of intracranial aneurysms treated using endovascular techniques: A meta-analysis. J. Neurointerv. Surg. 2019, 11, 1009–1014. [Google Scholar] [CrossRef]
- L’Allinec, V.; Chatel, S.; Karakachoff, M.; Bourcereau, E.; Lamoureux, Z.; Gaignard, A.; Autrusseau, F.; Jouan, S.; Vion, A.C.; Loir and, G.; et al. Prediction of Unruptured Intracranial Aneurysm Evolution: The UCAN Project. Neurosurgery 2020, 87, 150–156. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Age (years) | 52.87 (30–72) |
| Female (No.) (%) | 32 (82.1%) |
| Ruptured aneurysm (No.) (%) | 11 (27.5%) |
| Aneurysm size (mm) | 6.84 (3–24) |
| Aneurysm location (No.) (%) | |
| Internal carotid artery | 16 (40.0%) |
| Middle cerebral artery | 9 (22.5%) |
| Anterior cerebral arteries | 8 (20.0%) |
| Posterior communicating artery | 5 (12.5%) |
| Posterior circulation | 2 (5.0%) |
| The data of continuous variables are present as the mean (range). | |
| Coiling (n = 15) | Stent-Assisted Coiling (n = 25) | |
|---|---|---|
| Immediate Angiographic Outcome | ||
| Complete occlusion | 12 (80.0%) | 20 (80.0%) |
| Neck remnant | 3 (20.0%) | 5 (20.0%) |
| Aneurysm remnant | 0 (0.0%) | 0 (0.0%) |
| Follow-up MR angiography | ||
| Complete occlusion | 8 (53.3%) | 17 (68.0%) |
| Neck remnant | 2 (13.3%) | 8 (32.0%) |
| Aneurysm remnant | 5 (33.3%) | 0 (0.0%) |
| Interval change in aneurysm occlusion grade | ||
| Aneurysm recurrence | 7 (46.7%) | 4 (16.0%) |
| Stable aneurysm occlusion | 7 (46.7%) | 20 (80.0%) |
| Improved aneurysm occlusion | 1 (6.7%) | 1 (4.0%) |
| Post-procedural aneurysm contrast enhancement | ||
| Yes | 12 (80%) | 18 (72%) |
| No | 3 (20%) | 7 (28%) |
| Remnant Flow on Follow-Up MRA | Post-Procedural Aneurysm Contrast Enhancement | |
| Yes | No | |
| No | 18 (45.0%) | 7 (17.5%) |
| Yes | 12 (30.0%) | 3 (12.5%) |
| Interval Change in Aneurysm Occlusion Grade | Post-Procedural Aneurysm Contrast Enhancement | |
| Yes | No | |
| Aneurysm recurrence | 9 (22.5%) | 2 (5.0%) |
| Stable aneurysm occlusion | 19 (47.5%) | 8 (20.0%) |
| Improved aneurysm occlusion | 2 (5.0%) | 0 (0.0%) |
| Variable | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Aneurysm Size | 0.67 | 0.42–1.06 | 0.089 |
| Ruptured aneurysm | 0.46 | 0.07–2.88 | 0.407 |
| Initial complete occlusion | 0.36 | 0.03–3.82 | 0.395 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwarzany, Ł.; Owsiak, M.; Tyburski, E.; Poncyljusz, W. High-Resolution Vessel Wall MRI of Endovascularly Treated Intracranial Aneurysms. Tomography 2022, 8, 303-315. https://doi.org/10.3390/tomography8010025
Zwarzany Ł, Owsiak M, Tyburski E, Poncyljusz W. High-Resolution Vessel Wall MRI of Endovascularly Treated Intracranial Aneurysms. Tomography. 2022; 8(1):303-315. https://doi.org/10.3390/tomography8010025
Chicago/Turabian StyleZwarzany, Łukasz, Mateusz Owsiak, Ernest Tyburski, and Wojciech Poncyljusz. 2022. "High-Resolution Vessel Wall MRI of Endovascularly Treated Intracranial Aneurysms" Tomography 8, no. 1: 303-315. https://doi.org/10.3390/tomography8010025
APA StyleZwarzany, Ł., Owsiak, M., Tyburski, E., & Poncyljusz, W. (2022). High-Resolution Vessel Wall MRI of Endovascularly Treated Intracranial Aneurysms. Tomography, 8(1), 303-315. https://doi.org/10.3390/tomography8010025