
Influence of Different Arm Positions in the Localizer Radiograph(s) on Patient Dose during Exposure-Controlled CT Examinations of the Neck to Pelvis


Abstract
:1. Introduction
2. Materials and Methods
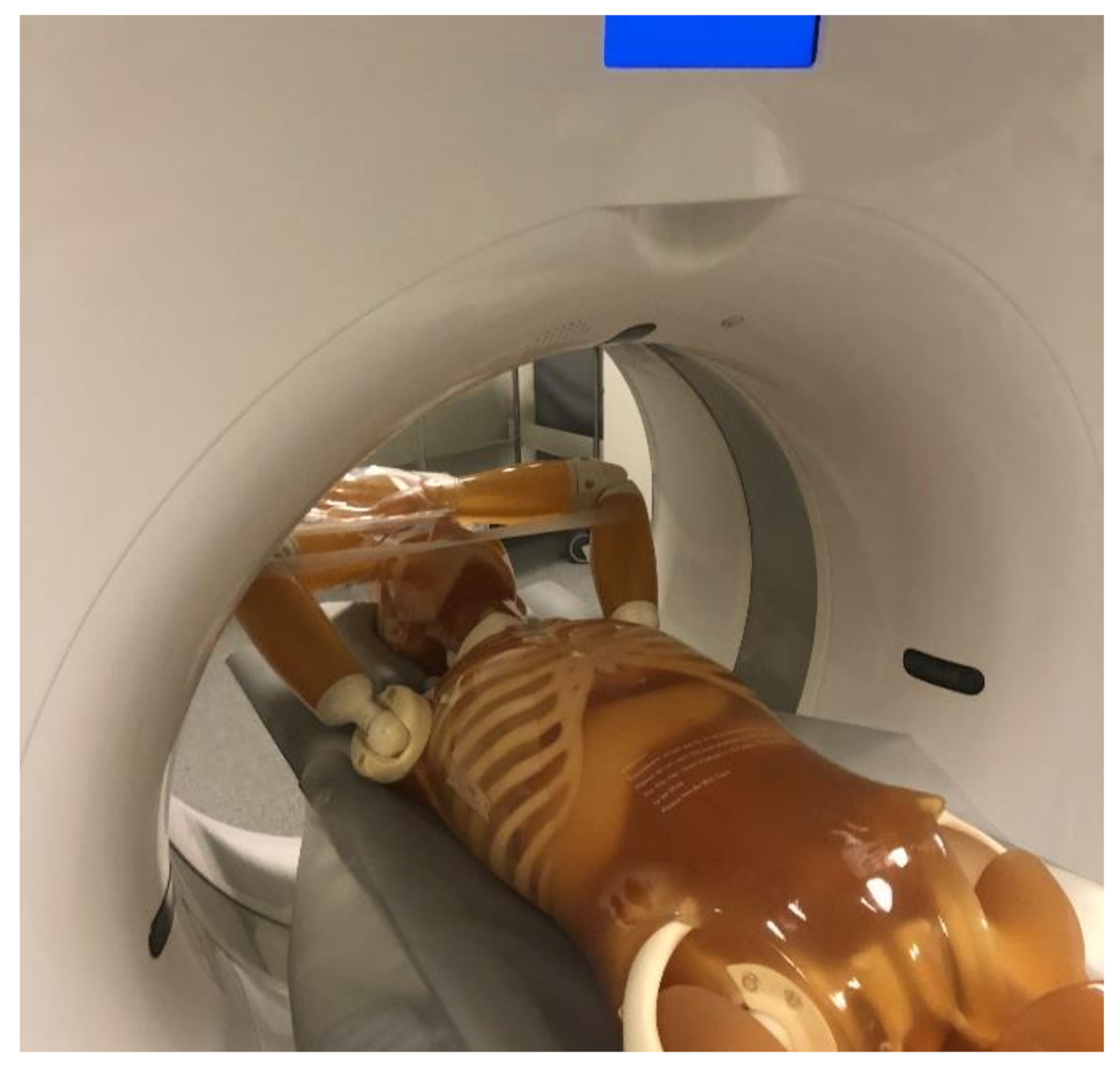
2.1. Phantom Model
2.2. CT Protocols/Image Acquisition
2.3. Tube Out-Put
2.4. Radiation Dose
2.5. Statistical Analysis
3. Results
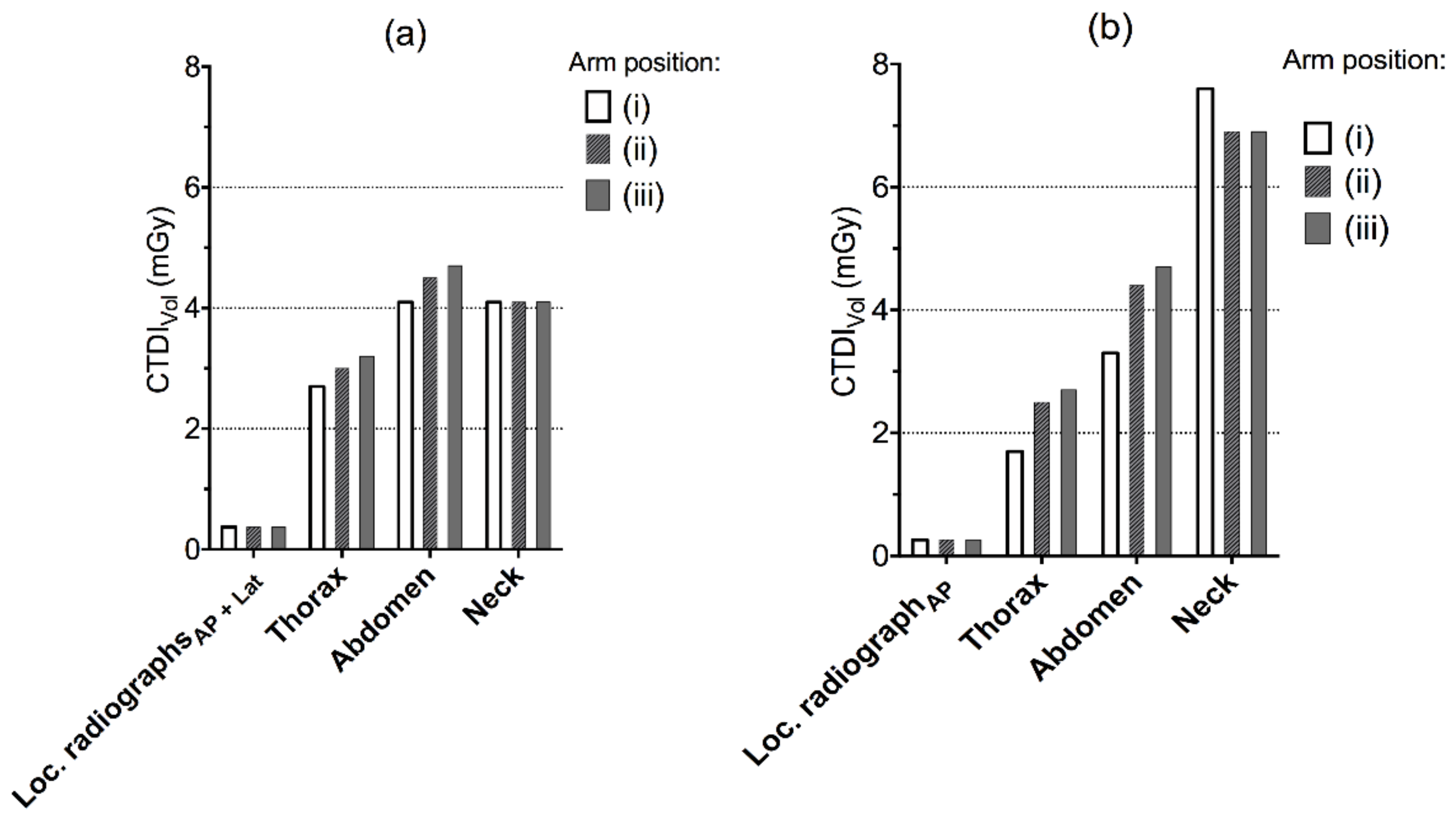
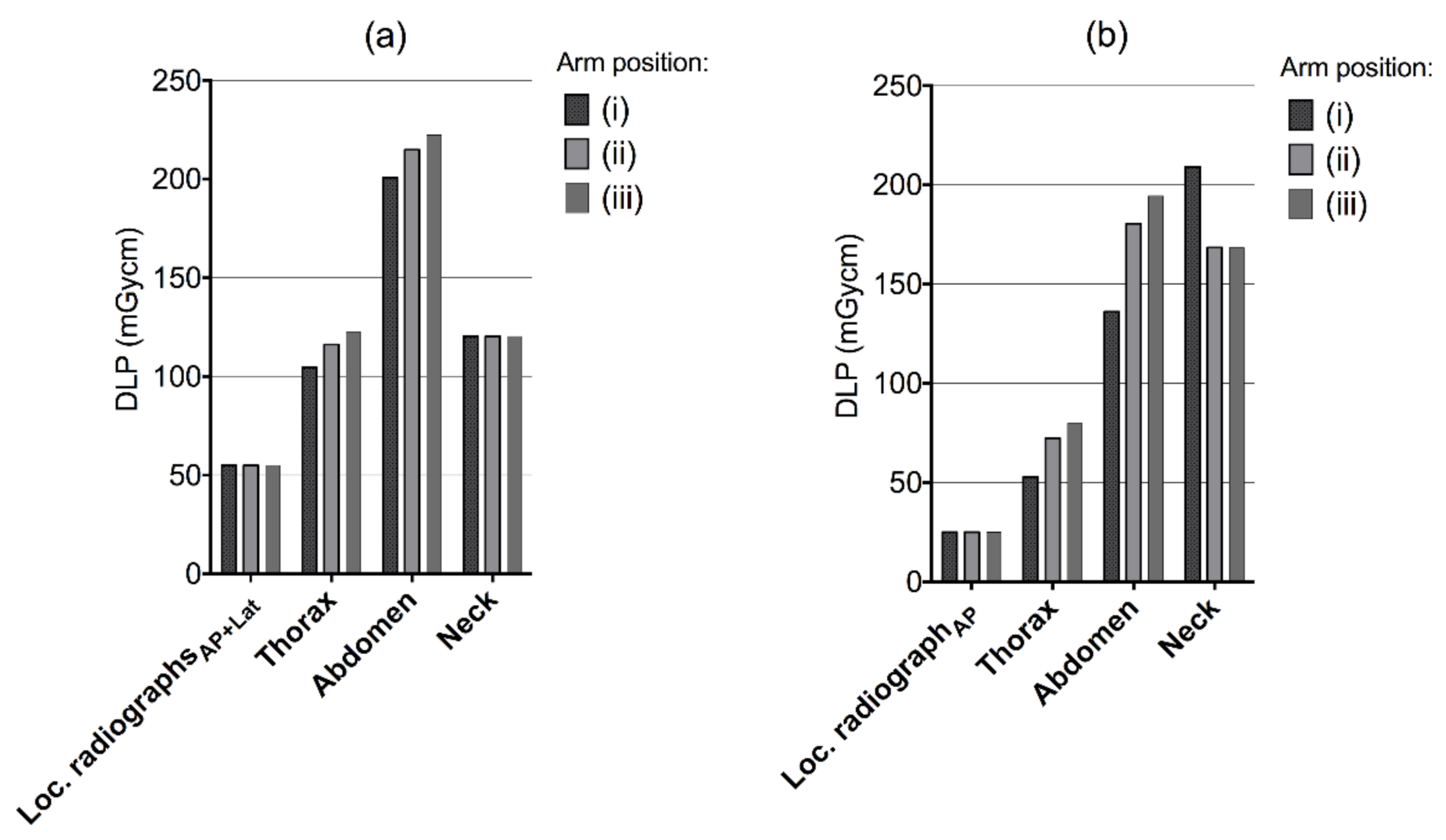
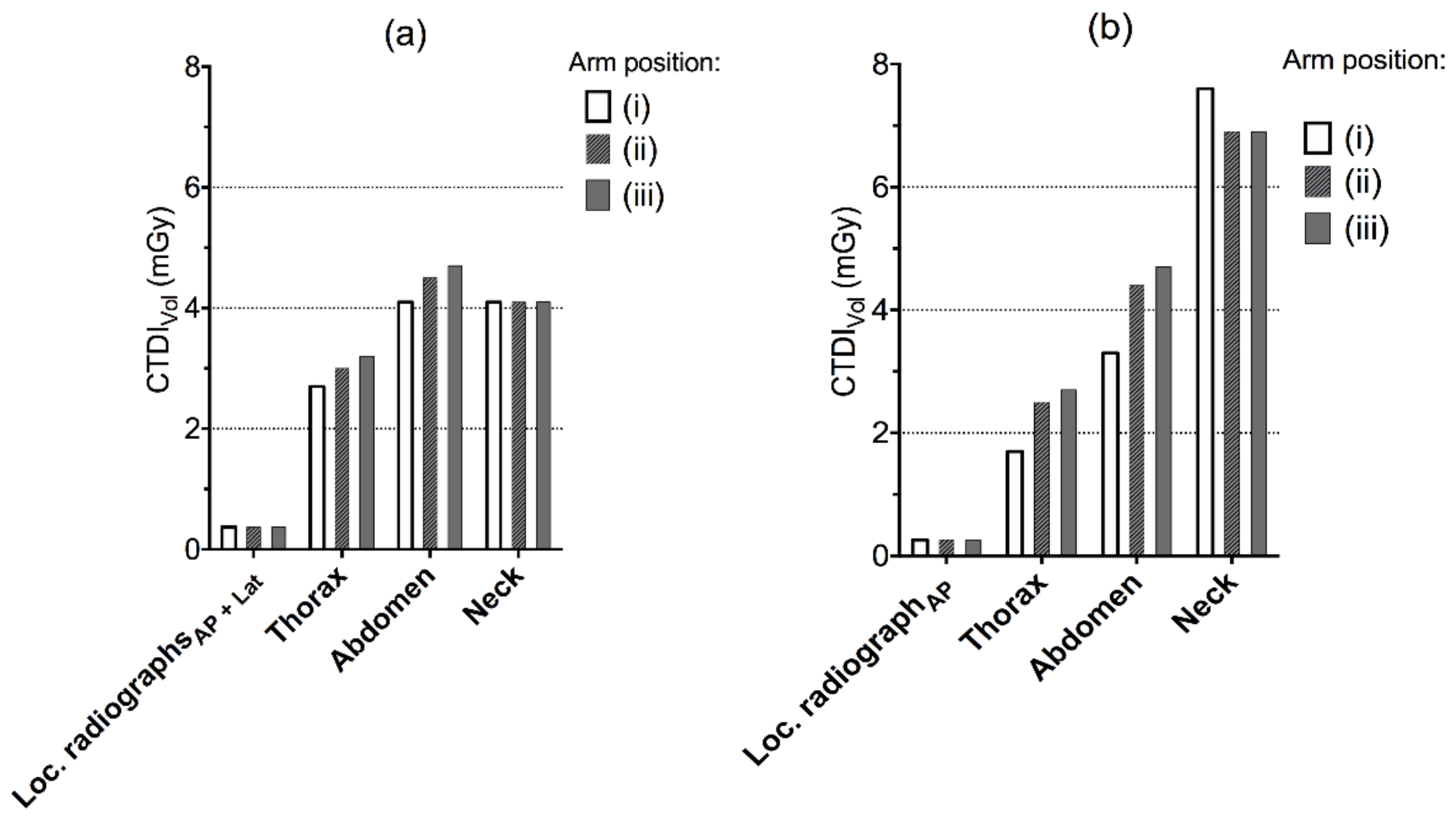
3.1. CTDIVOL and DLPs
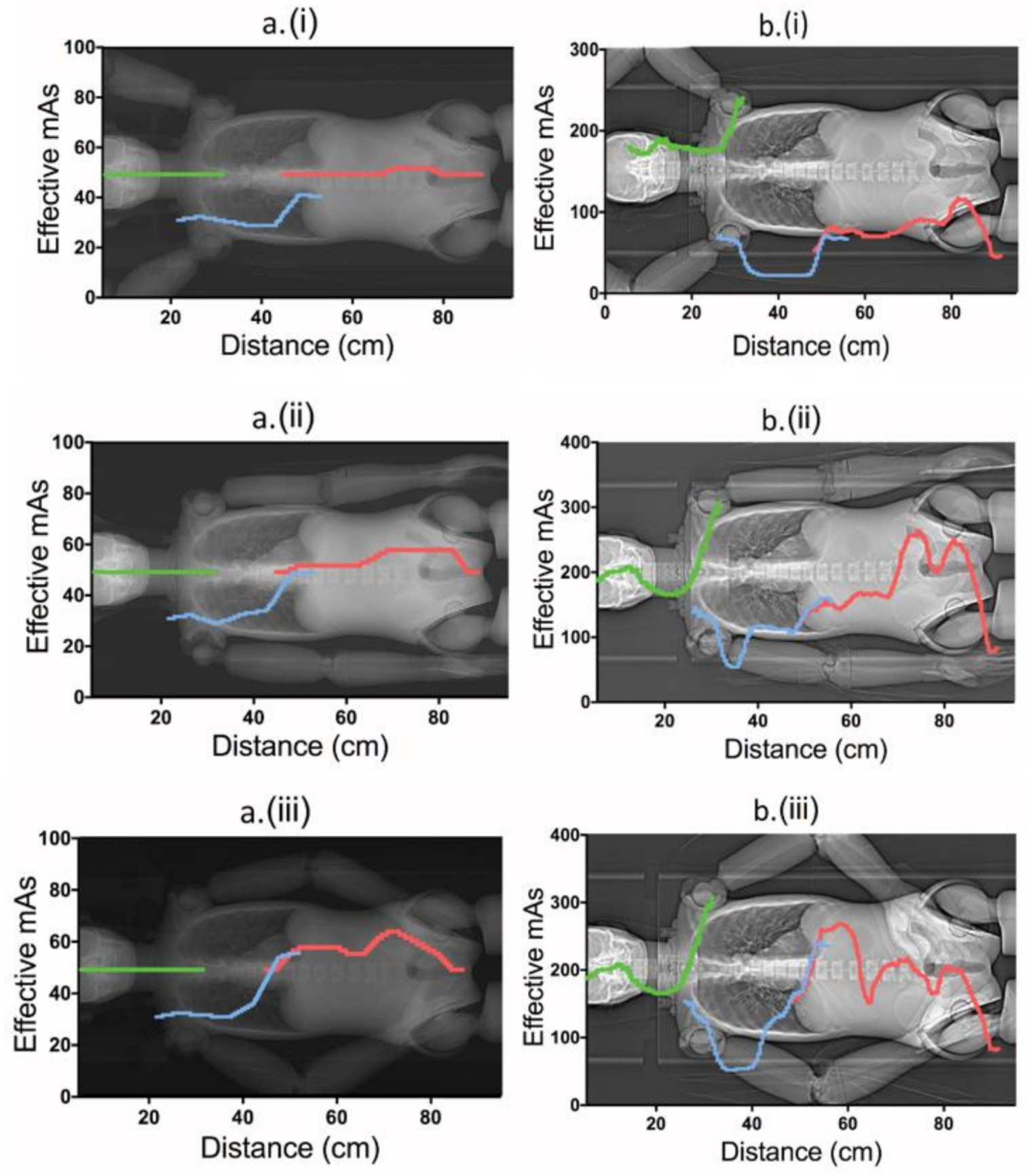
3.2. Effective mAs
3.2.1. Canon’s Protocol
3.2.2. Siemens’ Protocol
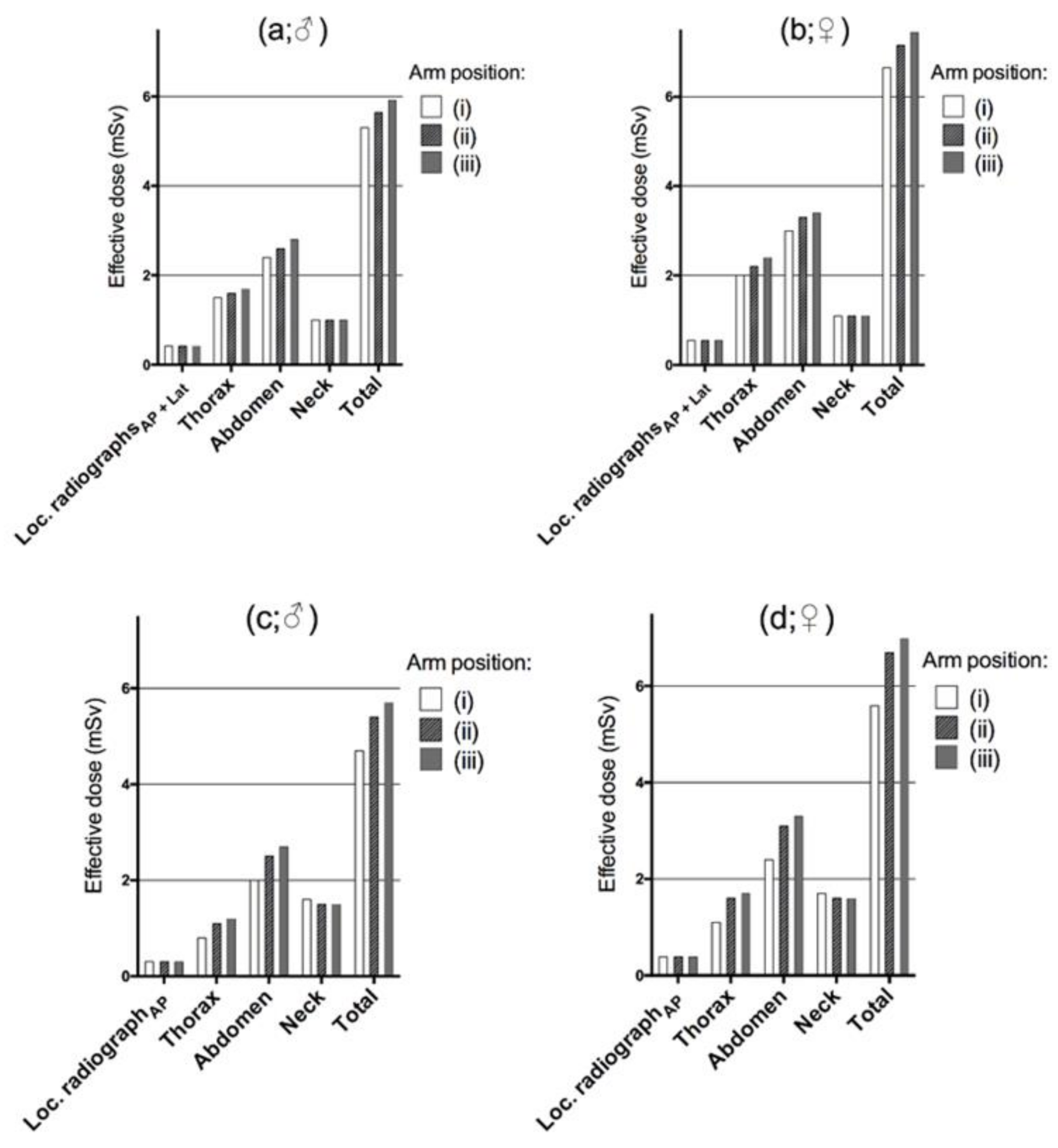
3.3. Effective Dose
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith-Bindman, R.; Lipson, J.; Marcus, R.; Kim, K.P.; Mahesh, M.; Gould, R.; Berrington de Gonzalez, A.; Miglioretti, D.L. Radiation Dose Associated with Common Computed Tomography Examinations and the Associated Lifetime Attributable Risk of Cancer. Arch. Intern. Med. 2009, 169, 2078–2086. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.; Elliston, C.; Hall, E.; Berdon, W. Estimated Risks of Radiation-induced Fatal Cancer from Pediatric CT. AJR Am. J. Roentgenol. 2001, 176, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Rehani, M.M.; Berry, M. Radiation Doses in Computed Tomography. The increasing Doses of Radiation Need to be Controlled. BMJ 2000, 320, 593–594. [Google Scholar] [CrossRef] [PubMed]
- Parker, L. Computed Tomography Scanning in Children: Radiation Risks. J. Pediatr. Hematol. Oncol. 2001, 18, 307–308. [Google Scholar] [CrossRef]
- Paterson, A.; Frush, D.P.; Donnelly, L.F. Helical CT of The Body: Are Settings Adjusted for Pediatric Patients? AJR Am. J. Roentgenol. 2001, 176, 297–301. [Google Scholar] [CrossRef]
- Brenner, D.J.; Elliston, C.D. Estimated Radiation Risks Potentially Associated with Full-body CT Screening. Radiology 2004, 232, 735–738. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.J.; Hall, E.J. Computed Tomography--An Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Pearce, M.S.; Salotti, J.A.; Little, M.P.; McHugh, K.; Lee, C.; Kim, K.P.; Howe, N.L.; Ronckers, C.M.; Rajaraman, P.; Sir Craft, A.W.; et al. Radiation Exposure from CT Scans in Childhood and Subsequent Risk of Leukaemia and Brain Tumours: A Retrospective Cohort Study. Lancet 2012, 380, 499–505. [Google Scholar] [CrossRef] [Green Version]
- Smith-Bindman, R.; Wang, Y.; Chu, P.; Chung, R.; Einstein, A.J.; Balcombe, J.; Cocker, M.; Das, M.; Delman, B.N.; Flynn, M.; et al. International Variation in Radiation Dose for Computed Tomography Examinations: Prospective Cohort Study. BMJ 2019, 364, k4931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terra-Filho, M.; Bagatin, E.; Nery, L.E.; Napolis, L.M.; Neder, J.A.; Meirelles, G.S.; Silva, C.I.; Muller, N.L. Screening of Miners and Millers at Decreasing Levels of Asbestos Exposure: Comparison of Chest Radiography and Thin-section Computed Tomography. PLoS ONE 2015, 10, e0118585. [Google Scholar] [CrossRef] [Green Version]
- Deak, P.D.; Smal, Y.; Kalender, W.A. Multisection CT Protocols: Sex- And Age-specific Conversion Factors Used to Determine Effective Dose from Dose-length Product. Radiology 2010, 257, 158–166. [Google Scholar] [CrossRef] [Green Version]
- McKenney, S.E.; Seibert, J.A.; Lamba, R.; Boone, J.M. Methods for CT Automatic Exposure Control Protocol Translation between Scanner Platforms. J. Am. Coll. Radiol. 2014, 11, 285–291. [Google Scholar] [CrossRef] [Green Version]
- McCollough, C.H.; Bruesewitz, M.R.; Kofler, J.M. CT Dose Reduction and Dose Management Tools: Overview of Available Options. Radiographics 2006, 26, 503–512. [Google Scholar] [CrossRef] [Green Version]
- Soderberg, M. Overview, Practical Tips and Potential Pitfalls of Using Automatic Exposure Control in Ct: Siemens Care Dose 4d. Radiat. Prot. Dosim. 2016, 169, 84–91. [Google Scholar] [CrossRef]
- Hansen, S.L.; Bebbington, N.A. Estimation of CARE Dose 4D Quality Reference mAs Conversion Factors for Child to Adult Reference Patient in Child Protocols on Siemens Symbia SPECT-CT Systems. Nucl. Med. Commun. 2021, 42, 107–112. [Google Scholar] [CrossRef]
- Murata, K. Multipurpose Chest Phantom N1. Available online: https://www.kyotokagaku.com/en/products_introduction/ph-2b/ (accessed on 28 July 2021).
- Lee, C.H.; Goo, J.M.; Ye, H.J.; Ye, S.J.; Park, C.M.; Chun, E.J.; Im, J.G. Radiation Dose Modulation Techniques in the Multidetector CT era: From Basics to Practice. Radiographics 2008, 28, 1451–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzo, S.; Kalra, M.; Schmidt, B.; Dalal, T.; Suess, C.; Flohr, T.; Blake, M.; Saini, S. Comparison of Angular and Combined Automatic Tube Current Modulation Techniques with Constant Tube Current CT of the Abdomen and Pelvis. AJR Am. J. Roentgenol. 2006, 186, 673–679. [Google Scholar] [CrossRef]
- Stamm, G.; Nagel, H.D. CT-expo--A novel Program for Dose Evaluation in CT. RöFo 2002, 174, 1570–1576. [Google Scholar] [PubMed]
- Rueden, C.T.; Schindelin, J.; Hiner, M.C.; DeZonia, B.E.; Walter, A.E.; Arena, E.T.; Eliceiri, K.W. ImageJ2: ImageJ for the Next Generation of Scientific Image Data. BMC Bioinform. 2017, 18, 529. [Google Scholar] [CrossRef] [PubMed]
- The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann. ICRP 2007, 37, 1–332.
- Svahn, T.M.; Sjoberg, T.; Ast, J.C. Dose Estimation of Ultra-low-dose Chest CT to Different Sized Adult Patients. Eur. Radiol. 2019, 29, 4315–4323. [Google Scholar] [CrossRef]
- Schegerer, A.A.; Nagel, H.D.; Stamm, G.; Adam, G.; Brix, G. Current CT Practice in Germany: Results and Implications of a Nationwide Survey. Eur. J. Radiol. 2017, 90, 114–128. [Google Scholar] [CrossRef] [PubMed]
- Lungren, M.P.; Yoshizumi, T.T.; Brady, S.M.; Toncheva, G.; Anderson-Evans, C.; Lowry, C.; Zhou, X.R.; Frush, D.; Hurwitz, L.M. Radiation Dose Estimations to the Thorax using Organ-based Dose Modulation. AJR Am. J. Roentgenol. 2012, 199, W65–W73. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Sung, Y.M.; Choi, J.H.; Kim, E.Y.; Kim, H.S. Reduced Radiation Exposure of the Female Breast During Low-dose Chest CT Using Organ-based Tube Current modulation and a Bismuth Shield: Comparison of Image Quality and Radiation Dose. AJR Am. J. Roentgenol. 2013, 200, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Svahn, T.M.; Ast, J.C. Effective Dose and Effect of Dose Modulation for Localizer Radiographs Using Applied and Alternative Settings on Toshiba/Canon CT Systems. Radiat. Prot. Dosim. 2021. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Canon Aquilion One *, § | Siemens Definition AS £, § |
|---|---|---|
| Beam collimation (mm) | 80 × 0.5 | 64 × 0.6 |
| Scanning mode | Helical | Helical |
| Pitch [neck] | 0.813 | 0.8 |
| Pitch [thorax] | 1.388 | 0.5 |
| Pitch [abdomen] | 0.813 | 0.6 |
| Rotation time | 0.5 | 0.35 |
| Tube voltage (kVp) | 120 | 100 |
| AEC | SureExposure 3D | Care Dose 4D |
| Scanning direction | Head first | Head first |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Svahn, T.M.; Peric, L.; Ast, J.C. Influence of Different Arm Positions in the Localizer Radiograph(s) on Patient Dose during Exposure-Controlled CT Examinations of the Neck to Pelvis. Tomography 2021, 7, 313-322. https://doi.org/10.3390/tomography7030028
Svahn TM, Peric L, Ast JC. Influence of Different Arm Positions in the Localizer Radiograph(s) on Patient Dose during Exposure-Controlled CT Examinations of the Neck to Pelvis. Tomography. 2021; 7(3):313-322. https://doi.org/10.3390/tomography7030028
Chicago/Turabian StyleSvahn, Tony M., Lovre Peric, and Jennifer C. Ast. 2021. "Influence of Different Arm Positions in the Localizer Radiograph(s) on Patient Dose during Exposure-Controlled CT Examinations of the Neck to Pelvis" Tomography 7, no. 3: 313-322. https://doi.org/10.3390/tomography7030028
APA StyleSvahn, T. M., Peric, L., & Ast, J. C. (2021). Influence of Different Arm Positions in the Localizer Radiograph(s) on Patient Dose during Exposure-Controlled CT Examinations of the Neck to Pelvis. Tomography, 7(3), 313-322. https://doi.org/10.3390/tomography7030028