

Comparative Efficacy of Novel Biomimetic Remineralising Technologies


Abstract
1. Introduction
2. Materials and Methods
2.1. Biomimetic Remineralisation Products
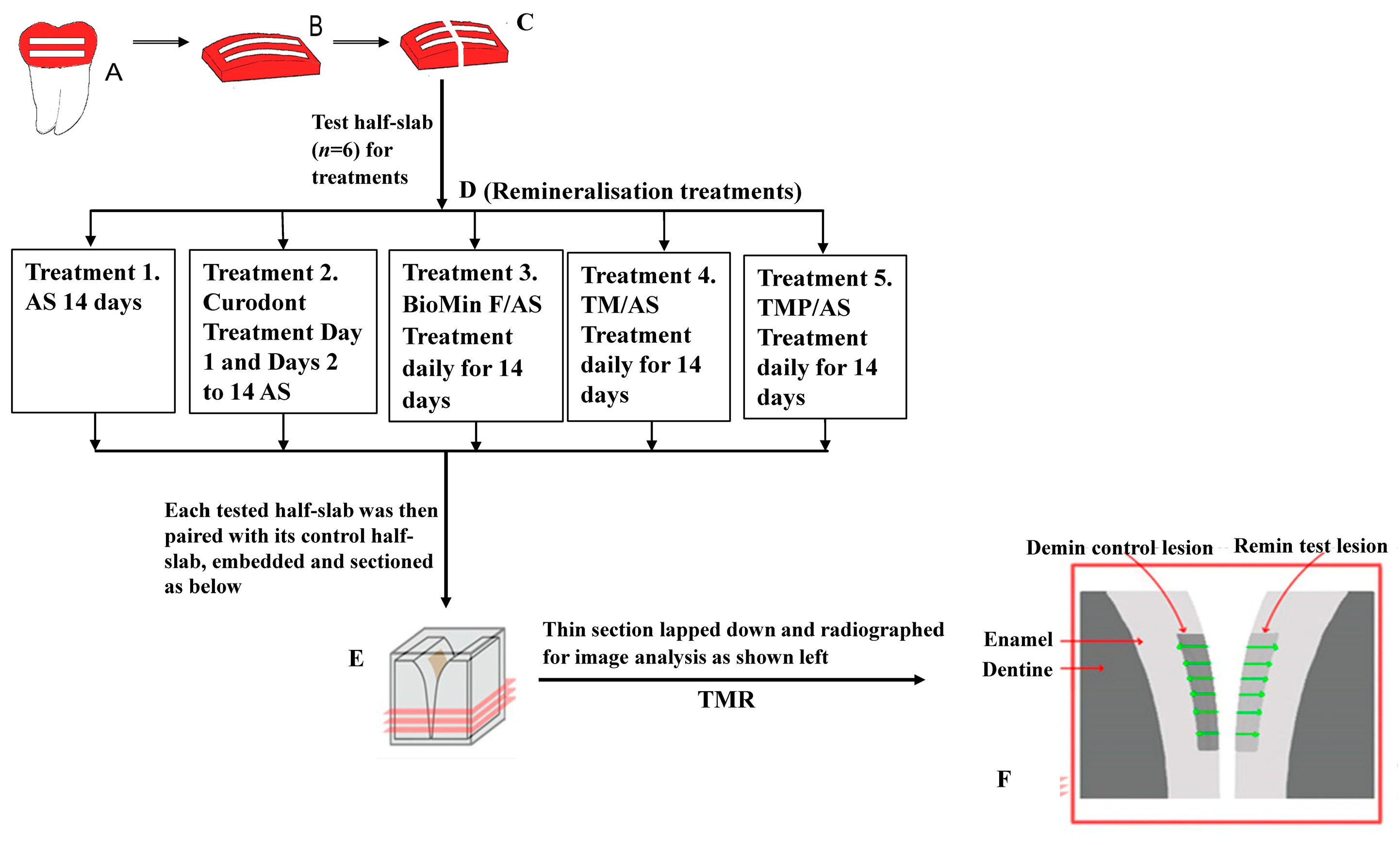
2.2. Enamel Subsurface Lesion Preparation
2.3. Remineralisation Protocol
2.4. Sectioning and Transverse Microradiography
2.5. Statistical Analysis
3. Results
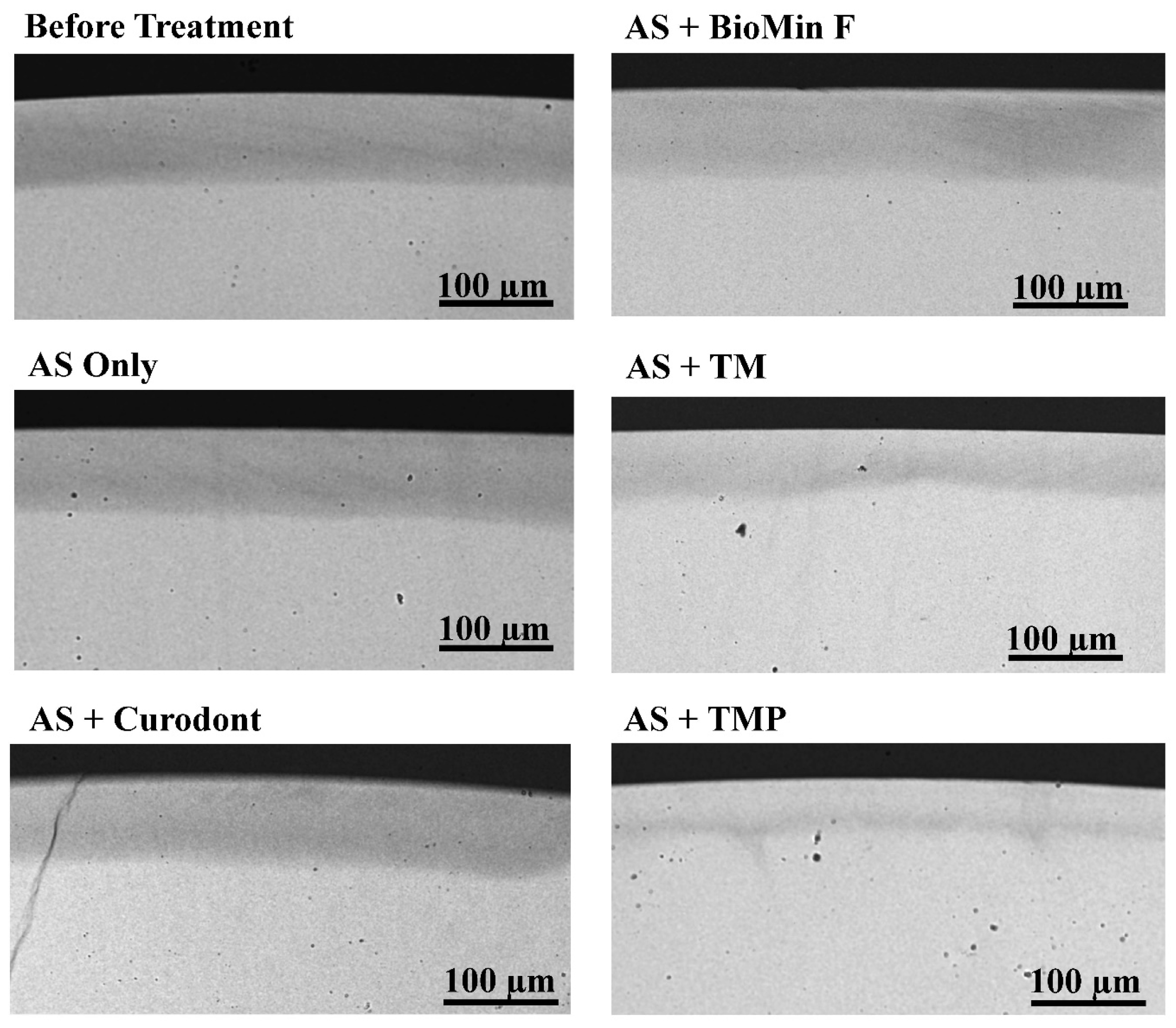
3.1. Mineral Content Change after Treatment
3.2. Enamel Subsurface Lesions Depths
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.S.; Chu, C.H.; Yu, O.Y. Oral microbiome and dental caries development. Dent. J. 2022, 10, 184. [Google Scholar] [CrossRef]
- Wong, M.C.; Clarkson, J.; Glenny, A.M.; Lo, E.C.; Marinho, V.C.; Tsang, B.W.; Walsh, T.; Worthington, H.V. Cochrane reviews on the benefits/risks of fluoride toothpastes. J. Dent. Res. 2011, 90, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.Y.; Campus, G.; Giuliana, G.; Piscopo, M.R.; Pizzo, G. Topical fluoride for preventing dental caries in children and adolescents. Curr. Pharm. Des. 2012, 18, 5532–5541. [Google Scholar] [CrossRef]
- dos Santos, A.P.; Nadanovsky, P.; de Oliveira, B.H. A systematic review and meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the primary dentition of preschool children. Community Dent. Oral Epidemiol. 2013, 41, 1–12. [Google Scholar] [CrossRef]
- He, L.; Deng, D.; Zhou, X.; Cheng, L.; ten Cate, J.M.; Li, J.; Li, X.; Crielaard, W. Novel tea polyphenol-modified calcium phosphate nanoparticle and its remineralization potential. J. Biomed. Mater. Res. B Appl. Biomater. 2015, 103, 1525–1531. [Google Scholar] [CrossRef]
- Vogel, G.L. Oral fluoride reservoirs and the prevention of dental caries. Monogr. Oral Sci. 2011, 22, 146–157. [Google Scholar] [PubMed]
- Cochrane, N.J.; Reynolds, E.C. Calcium phosphopeptides—Mechanisms of action and evidence for clinical efficacy. Adv. Dent. Res. 2012, 24, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Ogaard, B.; Rolla, G.; Arends, J. Orthodontic appliances and enamel demineralization. Part 1. Lesion development. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Sangamesh, B.; Kallury, A. Iatrogenic effects of orthodontic treatment–Review on white spot lesions. Int. J. Sci. Eng. Res. 2011, 2, 2–16. [Google Scholar]
- Mizrahi, E. Enamel demineralization following orthodontic treatment. Am. J. Orthod. 1982, 82, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, L.; Geiger, A.M.; Gwinnett, A.J. Incidence of white spot formation after bonding and banding. Am. J. Orthod. 1982, 81, 93–98. [Google Scholar] [CrossRef]
- Mitchell, L. Decalcification during orthodontic treatment with fixed appliances—An overview. Br. J. Orthod. 1992, 19, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Roveri, N.; Battistella, E.; Bianchi, C.; Foltran, I.; Foresti, F.; Iafisco, M.; Lelli, M.; Naldoni, A.; Palazzo, B.; Rimondini, L. Surface enamel remineralization: Biomimetic apatite nanocrystals and fluoride ions different effects. J. Nanomater. 2009, 2009, 746383. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Trapani, B.; Gallo, S.; Radu, M.; Scribante, A. Biomimetic hydroxyapatite paste for molar-incisor hypomineralization: A randomized clinical trial. Oral Dis. 2022; Early View. [Google Scholar] [CrossRef]
- Cochrane, N.J.; Cai, F.; Huq, N.L.; Burrow, M.F.; Reynolds, E.C. New approaches to enhanced remineralization of tooth enamel. J. Dent. Res. 2010, 89, 1187–1197. [Google Scholar] [CrossRef]
- Brauer, D.S.; Karpukhina, N.; O’Donnell, M.D.; Law, R.V.; Hill, R.G. Fluoride-containing bioactive glasses: Effect of glass design and structure on degradation, pH and apatite formation in simulated body fluid. Acta Biomater. 2010, 6, 3275–3282. [Google Scholar] [CrossRef] [PubMed]
- Lynch, E.; Brauer, D.S.; Karpukhina, N.; Gillam, D.G.; Hill, R.G. Multi-component bioactive glasses of varying fluoride content for treating dentin hypersensitivity. Dent. Mater. 2012, 28, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Meyer, F.; Amaechi, B.T.; Fabritius, H.O.; Enax, J. Overview of calcium phosphates used in biomimetic oral care. Open Dent. J. 2018, 12, 406–423. [Google Scholar] [CrossRef]
- Gonzalez-Cabezas, C.; Fernandez, C.E. Recent advances in remineralization therapies for caries lesions. Adv. Dent. Res. 2018, 29, 55–59. [Google Scholar] [CrossRef]
- Naumova, E.A.; Staiger, M.; Kouji, O.; Modric, J.; Pierchalla, T.; Rybka, M.; Hill, R.G.; Arnold, W.H. Randomized investigation of the bioavailability of fluoride in saliva after administration of sodium fluoride, amine fluoride and fluoride containing bioactive glass dentifrices. BMC Oral Health 2019, 19, 119. [Google Scholar] [CrossRef] [PubMed]
- Cross, K.J.; Huq, N.L.; Stanton, D.P.; Sum, M.; Reynolds, E.C. NMR studies of a novel calcium, phosphate and fluoride delivery vehicle-alpha(S1)-casein(59-79) by stabilized amorphous calcium fluoride phosphate nanocomplexes. Biomaterials 2004, 25, 5061–5069. [Google Scholar] [CrossRef] [PubMed]
- Cross, K.J.; Huq, N.L.; Palamara, J.E.; Perich, J.W.; Reynolds, E.C. Physicochemical characterization of casein phosphopeptide-amorphous calcium phosphate nanocomplexes. J. Biol. Chem. 2005, 280, 15362–15369. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.; Turdean-Ionescu, C.; Yu, Y.; Stevensson, B.; Izquierdo-Barba, I.; Garcia, A.; Arcos, D.; Vallet-Regi, M.; Eden, M. Proton environments in biomimetic calcium phosphates formed from mesoporous bioactive CaO-SiO(2)-P(2)O(5) glasses in vitro: Insights from solid-state NMR. J. Phys. Chem. C 2017, 121, 13223–13238. [Google Scholar] [CrossRef]
- Silvertown, J.D.; Wong, B.P.Y.; Sivagurunathan, K.S.; Abrams, S.H.; Kirkham, J.; Amaechi, B.T. Remineralization of natural early caries lesions in vitro by P11 -4 monitored with photothermal radiometry and luminescence. J. Investig. Clin. Dent. 2017, 8, e12257. [Google Scholar] [CrossRef]
- Alkilzy, M.; Santamaria, R.M.; Schmoeckel, J.; Splieth, C.H. Treatment of carious lesions using self-assembling peptides. Adv. Dent. Res. 2018, 29, 42–47. [Google Scholar] [CrossRef]
- Kirkham, J.; Firth, A.; Vernals, D.; Boden, N.; Robinson, C.; Shore, R.C.; Brookes, S.J.; Aggeli, A. Self-assembling peptide scaffolds promote enamel remineralization. J. Dent. Res. 2007, 86, 426–430. [Google Scholar] [CrossRef]
- Kind, L.; Stevanovic, S.; Wuttig, S.; Wimberger, S.; Hofer, J.; Muller, B.; Pieles, U. Biomimetic remineralization of carious lesions by self-assembling peptide. J. Dent. Res. 2017, 96, 790–797. [Google Scholar] [CrossRef]
- Shen, P.; Walker, G.D.; Yuan, Y.; Reynolds, C.; Reynolds, E.C. Polyols and remineralisation of enamel subsurface lesions. J. Dent. 2017, 66, 71–75. [Google Scholar] [CrossRef]
- Cochrane, N.J.; Saranathan, S.; Cai, F.; Cross, K.J.; Reynolds, E.C. Enamel subsurface lesion remineralisation with casein phosphopeptide stabilised solutions of calcium, phosphate and fluoride. Caries Res. 2008, 42, 88–97. [Google Scholar] [CrossRef]
- Cross, K.J.; Huq, N.L.; Reynolds, E.C. Casein phosphopeptides in oral health--chemistry and clinical applications. Curr. Pharm. Des. 2007, 13, 793–800. [Google Scholar] [CrossRef]
- Bailey, D.L.; Adams, G.G.; Tsao, C.E.; Hyslop, A.; Escobar, K.; Manton, D.J.; Reynolds, E.C.; Morgan, M.V. Regression of post-orthodontic lesions by a remineralizing cream. J. Dent. Res. 2009, 88, 1148–1153. [Google Scholar] [CrossRef]
- Morgan, M.V.; Adams, G.G.; Bailey, D.L.; Tsao, C.E.; Fischman, S.L.; Reynolds, E.C. The anticariogenic effect of sugar-free gum containing CPP-ACP nanocomplexes on approximal caries determined using digital bitewing radiography. Caries Res. 2008, 42, 171–184. [Google Scholar] [CrossRef]
- Reynolds, E.C.; Cai, F.; Cochrane, N.J.; Shen, P.; Walker, G.D.; Morgan, M.V.; Reynolds, C. Fluoride and casein phosphopeptide-amorphous calcium phosphate. J. Dent. Res. 2008, 87, 344–348. [Google Scholar] [CrossRef]
- Shen, P.; Manton, D.J.; Cochrane, N.J.; Walker, G.D.; Yuan, Y.; Reynolds, C.; Reynolds, E.C. Effect of added calcium phosphate on enamel remineralization by fluoride in a randomized controlled in situ trial. J. Dent. 2011, 39, 518–525. [Google Scholar] [CrossRef]
- Srinivasan, N.; Kavitha, M.; Loganathan, S.C. Comparison of the remineralization potential of CPP-ACP and CPP-ACP with 900 ppm fluoride on eroded human enamel: An in situ study. Arch. Oral Biol. 2010, 55, 541–544. [Google Scholar] [CrossRef]
- Mayne, R.J.; Cochrane, N.J.; Cai, F.; Woods, M.G.; Reynolds, E.C. In-vitro study of the effect of casein phosphopeptide amorphous calcium fluoride phosphate on iatrogenic damage to enamel during orthodontic adhesive removal. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e543–e551. [Google Scholar] [CrossRef]
- Guclu, Z.A.; Alacam, A.; Coleman, N.J. A 12-week assessment of the treatment of white spot lesions with CPP-ACP paste and/or fluoride varnish. Biomed. Res. Int. 2016, 2016, 8357621. [Google Scholar] [CrossRef]
- Heravi, F.; Ahrari, F.; Tanbakuchi, B. Effectiveness of MI Paste Plus and Remin Pro on remineralization and color improvement of postorthodontic white spot lesions. Dent. Res. J. 2018, 15, 95–103. [Google Scholar]
- Juarez-Lopez, M.L.; Hernandez-Palacios, R.D.; Hernandez-Guerrero, J.C.; Jimenez-Farfan, D.; Molina-Frechero, N. Preventive and remineralization effect over incipient lesions of caries decay by phosphopeptide-amorphous calcium phosphate. Rev. Investig. Clin. 2014, 66, 144–151. [Google Scholar]
- Krithikadatta, J.; Fredrick, C.; Abarajithan, M.; Kandaswamy, D. Remineralisation of occlusal white spot lesion with a combination of 10% CPP-ACP and 0.2% sodium fluoride evaluated using Diagnodent: A pilot study. Oral Health Prev. Dent. 2013, 11, 191–196. [Google Scholar] [PubMed]
- Rao, S.K.; Bhat, G.S.; Aradhya, S.; Devi, A.; Bhat, M. Study of the efficacy of toothpaste containing casein phosphopeptide in the prevention of dental caries: A randomized controlled trial in 12- to 15-year-old high caries risk children in Bangalore, India. Caries Res. 2009, 43, 430–435. [Google Scholar] [CrossRef]
- Robertson, M.A.; Kau, C.H.; English, J.D.; Lee, R.P.; Powers, J.; Nguyen, J.T. MI Paste Plus to prevent demineralization in orthodontic patients: A prospective randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 660–668. [Google Scholar] [CrossRef] [PubMed]
- de Alencar, C.R.; Magalhaes, A.C.; de Andrade Moreira Machado, M.A.; de Oliveira, T.M.; Honorio, H.M.; Rios, D. In situ effect of a commercial CPP-ACP chewing gum on the human enamel initial erosion. J. Dent. 2014, 42, 1502–1507. [Google Scholar] [CrossRef] [PubMed]
- Wierichs, R.J.; Kogel, J.; Lausch, J.; Esteves-Oliveira, M.; Meyer-Lueckel, H. Effects of self-assembling peptide P11-4, fluorides, and caries infiltration on artificial enamel caries lesions in vitro. Caries Res. 2017, 51, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Fernando, J.R.; Shen, P.; Walker, G.D.; Yuan, Y.; Stanton, D.P.; Reynolds, C.; Reynolds, E.C. Acceleration of enamel subsurface lesion remineralisation by intralesion pH modulation. Caries Res. 2021, 55, 130–136. [Google Scholar] [CrossRef]
- Singal, K.; Sharda, S.; Gupta, A.; Malik, V.S.; Singh, M.; Chauhan, A.; Agarwal, A.; Pradhan, P.; Singh, M. Effectiveness-of Calcium Phosphate derivative agents on the prevention and remineralization of caries among children- A systematic review & meta-analysis of randomized controlled trials. J. Evid. Based Dent. Pract. 2022, 22, 101746. [Google Scholar] [PubMed]
- Simon, L.S.; Dash, J.K.; U, D.; Philip, S.; Sarangi, S. Management of Post Orthodontic White Spot Lesions Using Resin Infiltration and CPP-ACP Materials- A Clinical Study. J. Clin. Pediatr. Dent. 2022, 46, 70–74. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Product Name | Biomimetic Technology |
|---|---|
| Tooth Mousse® (GC, Tokyo, Japan) | 10% (w/w CPP–ACP |
| Tooth Mousse Plus® (GC, Tokyo, Japan) | 10% (w/w) CPP–ACFP with 900 ppm F |
| BioMinTM F (BioMin Technologies Ltd., London, UK) | Fluoro Calcium Phosphosilicate with 590 ppm F |
| CurodontTM Repair (Credentis, Windisch, Switzerland) | Self-assembling P11-4 peptides |
| Treatment | LDd (µm) | LDd−LDr (µm) | ∆Zd (vol%min.µm) | ∆Zd − ∆Zr (vol%min.µm) | %R |
|---|---|---|---|---|---|
| AS only | 94.33 ± 5.66 * | −3.01 ± 5.44 ab | 2059.11 ± 92.06 | 44.61 ± 12.20 abcd | 2.11 ± 0.47 abcd |
| AS + Curodont | 84.54 ± 6.63 | −0.45 ± 7.73 cd | 2171.12 ± 301.86 | 126.20 ± 46.14 aefg | 5.75 ± 1.63 aefg |
| AS + BioMin F | 87.26 ± 7.49 | 4.30 ± 5.29 ef | 2149.35 ± 262.14 | 286.53 ± 78.08 behi | 13.23 ± 2.45 behi |
| AS + TM | 92.97 ± 5.65 | 22.09 ± 6.46 ace | 2577.04 ± 246.75 | 1113.83 ± 215.53 cfh | 43.00 ± 4.94 cfhj |
| AS + TMP | 93.62 ± 7.30 | 33.23 ± 10.73 bdf | 2228.64 ± 267.49 | 1168.58 ± 112.70 dgi | 52.64 ± 2.56 dgij |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, P.; Fernando, J.R.; Yuan, Y.; Reynolds, C.; Reynolds, E.C. Comparative Efficacy of Novel Biomimetic Remineralising Technologies. Biomimetics 2023, 8, 17. https://doi.org/10.3390/biomimetics8010017
Shen P, Fernando JR, Yuan Y, Reynolds C, Reynolds EC. Comparative Efficacy of Novel Biomimetic Remineralising Technologies. Biomimetics. 2023; 8(1):17. https://doi.org/10.3390/biomimetics8010017
Chicago/Turabian StyleShen, Peiyan, James R. Fernando, Yi Yuan, Coralie Reynolds, and Eric C. Reynolds. 2023. "Comparative Efficacy of Novel Biomimetic Remineralising Technologies" Biomimetics 8, no. 1: 17. https://doi.org/10.3390/biomimetics8010017
APA StyleShen, P., Fernando, J. R., Yuan, Y., Reynolds, C., & Reynolds, E. C. (2023). Comparative Efficacy of Novel Biomimetic Remineralising Technologies. Biomimetics, 8(1), 17. https://doi.org/10.3390/biomimetics8010017