
Efficacy and Safety of Oral Probiotics in Children with Allergic Rhinitis: A Review

 , ,
, ,  ,
,  ,
,  and
and
Abstract
1. Introduction
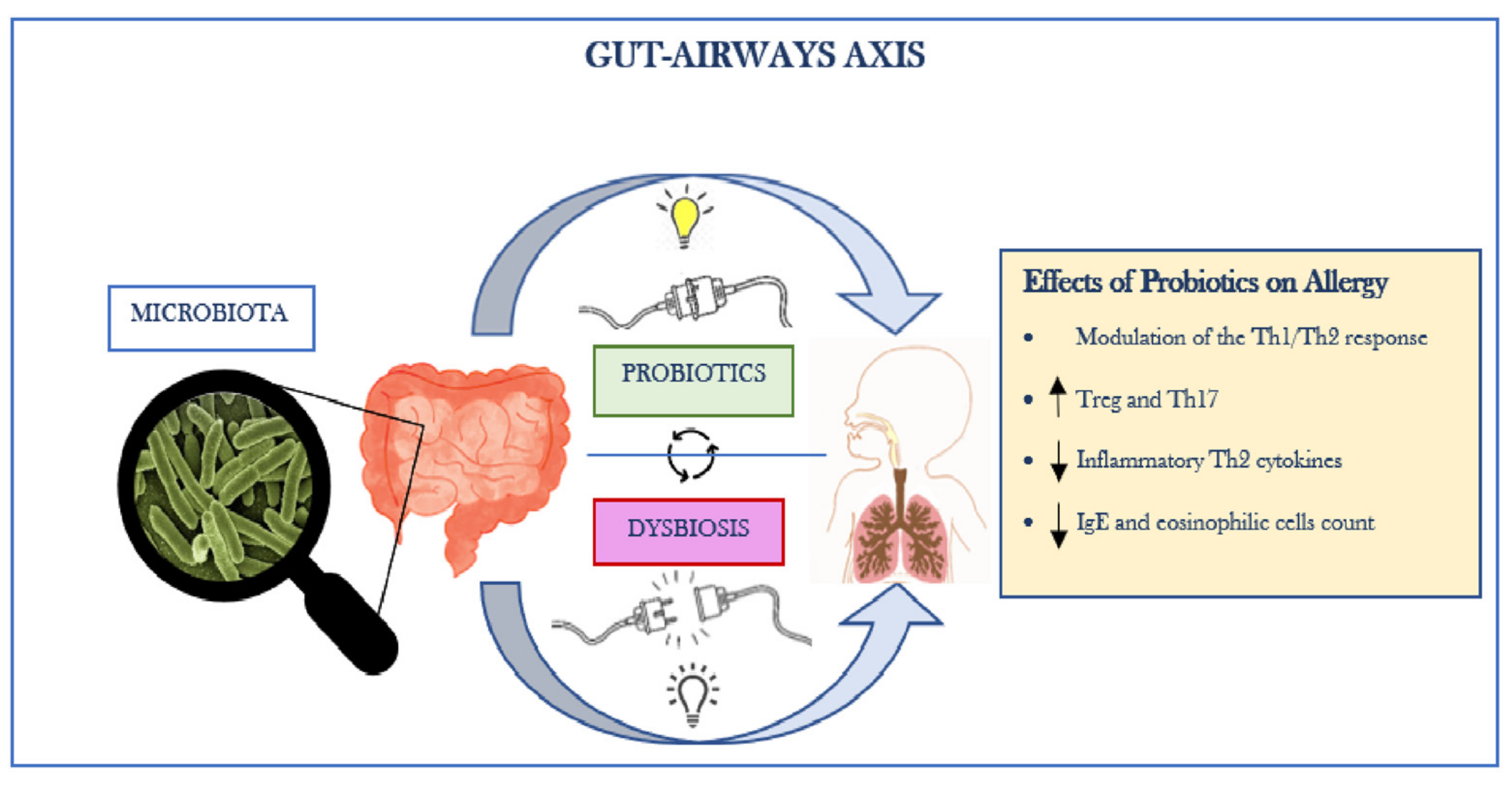
2. Gut–Lung Axis
3. Probiotic Food
4. Probiotics and Allergic Rhinitis: Evidence and Challenges
5. Lactobacilli
6. Bifidobacteria
7. Enterococci
8. Saccharomyces
9. Butyric Acid Producing Bacteria
10. The Role of Probiotics in the Prevention of Allergy during Pregnancy
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Del Giudice, M.M.; Marseglia, A.; Leonardi, S.; La Rosa, M.; Salpietro, C.; Brunese, F.; Arrigo, T.; Perrone, L. Allergic Rhinitis and Quality of Life in Children. Int. J. Immunopathol. Pharmacol. 2011, 24 (Suppl. 4), 25–28. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, M.M.; Allegorico, A.; Marseglia, G.L.; Martelli, A.; Calvani, M.; Cardinale, F.; Duse, M.; Chiappini, E.; Manti, S.; Cravidi, C.; et al. Allergic Rhinoconjunctivitis. Acta Bio Medica Atenei Parm. 2020, 91 (Suppl. 11), 1–3. [Google Scholar] [CrossRef]
- Brożek, J.L.; Bousquet, J.; Baena-Cagnani, C.E.; Bonini, S.; Canonica, G.W.; Casale, T.B.; van Wijk, R.G.; Ohta, K.; Zuberbier, T.; Schünemann, H.J. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 Revision. J. Allergy Clin. Immunol. 2010, 126, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, F.; Mastrorilli, C.; Tripodi, S.; Ricci, G.; Perna, S.; Panetta, V.; Asero, R.; Dondi, A.; Bianchi, A.; Maiello, N.; et al. Diagnostic relevance of IgE sensitization profiles to eight recombinant Phleum pratense molecules. Allergy 2017, 73, 673–682. [Google Scholar] [CrossRef]
- Kay, A. Asthma and inflammation. J. Allergy Clin. Immunol. 1991, 87, 893–910. [Google Scholar] [CrossRef]
- Lanz, M.J.; Leung, D.Y.; White, C.W. Comparison of exhaled nitric oxide to spirometry during emergency treatment of asthma exacerbations with glucocorticoids in children. Ann. Allergy Asthma Immunol. 1999, 82, 161–164. [Google Scholar] [CrossRef]
- Kharitonov, S.A.; Yates, D.H.; Barnes, P.J. Inhaled glucocorticoids decrease nitric oxide in exhaled air of asthmatic patients. Am. J. Respir. Crit. Care Med. 1996, 153, 454–457. [Google Scholar] [CrossRef]
- Cox, L. Approach to Patients with Allergic Rhinitis: Testing and Treatment. Med. Clin. N. Am. 2019, 104, 77–94. [Google Scholar] [CrossRef]
- Bousquet, J.; Schünemann, H.J.; Togias, A.; Bachert, C.; Erhola, M.; Hellings, P.W.; Klimek, L.; Pfaar, O.; Wallace, D.; Ansotegui, I.; et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J. Allergy Clin. Immunol. 2019, 145, 70–80.e3. [Google Scholar] [CrossRef]
- Bernstein, D.I.; Schwartz, G.; Bernstein, J.A. Allergic Rhinitis: Mechanisms and Treatment. Immunol. Allergy Clin. N. Am. 2016, 36, 261–278. [Google Scholar] [CrossRef]
- Bousquet, J.; Schunemann, H.J.; Fonseca, J.; Samolinski, B.; Bachert, C.; Canonica, G.W.; Casale, T.; Cruz, A.A.; Demoly, P.; Hellings, P.; et al. MACVIA-ARIA Sentinel NetworK for allergic rhinitis (MASK-rhinitis): The new generation guideline implementation. Allergy 2015, 70, 1372–1392. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Anto, J.M.; Bachert, C.; Baiardini, I.; Bosnic-Anticevich, S.; Canonica, G.W.; Melén, E.; Palomares, O.; Scadding, G.K.; Togias, A.; et al. Allergic rhinitis. Nat. Rev. Dis. Prim. 2020, 6, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Carr, W.; Bernstein, J.; Lieberman, P.; Meltzer, E.; Bachert, C.; Price, D.; Munzel, U.; Bousquet, J. A novel intranasal therapy of azelastine with fluticasone for the treatment of allergic rhinitis. J. Allergy Clin. Immunol. 2012, 129, 1282–1289.e10. [Google Scholar] [CrossRef]
- Indolfi, C.; Dinardo, G.; Umano, G.R.; Klain, A.; Contieri, M.; Decimo, A.; Decimo, F.; Ciprandi, G.; Del Giudice, M.M. Mometasone furoate nasal spray in Italian children with seasonal allergic rhinitis: A comprehensive assessment. Allergol. Immunopathol. 2022, 50, 61–67. [Google Scholar] [CrossRef]
- Grainger, J.; Drake-Lee, A. Montelukast in allergic rhinitis: A systematic review and meta-analysis. Clin. Otolaryngol. 2006, 31, 360–367. [Google Scholar] [CrossRef]
- Tenero, L.; Vaia, R.; Ferrante, G.; Maule, M.; Venditto, L.; Piacentini, G.; Senna, G.; Caminati, M. Diagnosis and Management of Allergic Rhinitis in Asthmatic Children. J. Asthma Allergy 2023, 16, 45–57. [Google Scholar] [CrossRef]
- Lin, C.-F.; Lin, Y.-T.; Liao, C.-K.; Yeh, T.-H. Recent Updates of Immunotherapy for Allergic Rhinitis in Children. Curr. Otorhinolaryngol. Rep. 2023, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tosca, M.A.; Licari, A.; Olcese, R.; Castagnoli, R.; Marseglia, A.; Marseglia, G.L.; del Giudice, M.M.; Martelli, A.; Calvani, M.; Caffarelli, C.; et al. Allergen immunotherapy in children and adolescents with respiratory diseases. Acta Bio Medica Atenei Parm. 2020, 91 (Suppl. 11), 1–4. [Google Scholar] [CrossRef]
- Ponda, P.; Carr, T.; Rank, M.A.; Bousquet, J. Nonallergic Rhinitis, Allergic Rhinitis, and Immunotherapy: Advances in the Last Decade. J. Allergy Clin. Immunol. Pract. 2022, 11, 35–42. [Google Scholar] [CrossRef]
- Liu, W.; Zeng, Q.; He, C.; Chen, R.; Tang, Y.; Yan, S.; Luo, X.; Luo, R. Compliance, efficacy, and safety of subcutaneous and sublingual immunotherapy in children with allergic rhinitis. Pediatr. Allergy Immunol. 2020, 32, 86–91. [Google Scholar] [CrossRef]
- Del Giudice, M.M.; Licari, A.; Brambilla, I.; Tosca, M.; Ciprandi, G. Allergen Immunotherapy in Pediatric Asthma: A Pragmatic Point of View. Children 2020, 7, 58. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Hu, T.; Kang, C.; Liu, J.; Zhang, J.; Ran, H.; Zeng, X.; Qiu, S. Research Advances in the Treatment of Allergic Rhinitis by Probiotics. J. Asthma Allergy 2022, 15, 1413–1428. [Google Scholar] [CrossRef]
- Capponi, M.; Gori, A.; De Castro, G.; Ciprandi, G.; Anania, C.; Brindisi, G.; Tosca, M.; Cinicola, B.L.; Salvatori, A.; Loffredo, L.; et al. (R)Evolution in Allergic Rhinitis Add-On Therapy: From Probiotics to Postbiotics and Parabiotics. J. Clin. Med. 2022, 11, 5154. [Google Scholar] [CrossRef]
- Klain, A.; Dinardo, G.; Salvatori, A.; Indolfi, C.; Contieri, M.; Brindisi, G.; Decimo, F.; Zicari, A.M.; del Giudice, M.M. An Overview on the Primary Factors That Contribute to Non-Allergic Asthma in Children. J. Clin. Med. 2022, 11, 6567. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, G.P.; Lee, S.M.; Mazmanian, S.K. Gut biogeography of the bacterial microbiota. Nat. Rev. Microbiol. 2016, 14, 20–32. [Google Scholar] [CrossRef]
- De Benedictis, F.; del Giudice, M.; Severini, S.; Bonifazi, F. Rhinitis, sinusitis and asthma: One linked airway disease. Paediatr. Respir. Rev. 2001, 2, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Klain, A.; Indolfi, C.; Dinardo, G.; Licari, A.; Cardinale, F.; Caffarelli, C.; Manti, S.; Ricci, G.; Pingitore, G.; Tosca, M.; et al. United Airway Disease. Acta Bio Medica Atenei Parm. 2021, 92 (Suppl 7), 2021526. [Google Scholar] [CrossRef]
- Probiotics in Food Health and Nutritional Properties and Guidelines for Evaluation FAO Food and Nutrition Paper. Available online: https://books.google.rs/books/about/Probiotics_in_Food.html?id=kNxxQgAACAAJ&redir_esc=y (accessed on 13 December 2022).
- Hajavi, J.; Esmaeili, S.; Varasteh, A.; Vazini, H.; Atabati, H.; Mardani, F.; Momtazi-Borojeni, A.A.; Hashemi, M.; Sankian, M.; Sahebkar, A. The immunomodulatory role of probiotics in allergy therapy. J. Cell. Physiol. 2018, 234, 2386–2398. [Google Scholar] [CrossRef]
- Farahmandi, K.; Mohr, A.E.; McFarland, L.V. Effects of Probiotics on Allergic Rhinitis: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Am. J. Rhinol. Allergy 2022, 36, 440–450. [Google Scholar] [CrossRef]
- Luo, C.; Peng, S.; Li, M.; Ao, X.; Liu, Z. The Efficacy and Safety of Probiotics for Allergic Rhinitis: A Systematic Review and Meta-Analysis. Front. Immunol. 2022, 13, 848279. [Google Scholar] [CrossRef]
- Luoto, R.; Ruuskanen, O.; Waris, M.; Kalliomäki, M.; Salminen, S.; Isolauri, E. Prebiotic and probiotic supplementation prevents rhinovirus infections in preterm infants: A randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2014, 133, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Waki, N.; Matsumoto, M.; Fukui, Y.; Suganuma, H. Effects of probiotic Lactobacillus brevis KB290 on incidence of influenza infection among schoolchildren: An open-label pilot study. Lett. Appl. Microbiol. 2014, 59, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Namba, K.; Hatano, M.; Yaeshima, T.; Takase, M.; Suzuki, K. Effects of Bifidobacterium longum BB536 Administration on Influenza Infection, Influenza Vaccine Antibody Titer, and Cell-Mediated Immunity in the Elderly. Biosci. Biotechnol. Biochem. 2010, 74, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.S.; Hung, I.F.N.; Chan, P.P.Y.; Lung, K.C.; Tso, E.; Liu, R.; Ng, Y.Y.; Chu, M.Y.; Chung, T.W.H.; Tam, A.R.; et al. Gastrointestinal Manifestations of SARS-CoV-2 Infection and Virus Load in Fecal Samples from a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L.; et al. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef]
- Liu, Y.; Kuang, D.; Li, D.; Yang, J.; Yan, J.; Xia, Y.; Zhang, F.; Cao, H. Roles of the gut microbiota in severe SARS-CoV-2 infection. Cytokine Growth Factor Rev. 2022, 63, 98–107. [Google Scholar] [CrossRef]
- De Oliveira, G.L.V.; Oliveira, C.N.S.; Pinzan, C.F.; de Salis, L.V.V.; Cardoso, C.R.D.B. Microbiota Modulation of the Gut-Lung Axis in COVID-19. Front. Immunol. 2021, 12, 635471. [Google Scholar] [CrossRef]
- Terpou, A.; Papadaki, A.; Lappa, I.; Kachrimanidou, V.; Bosnea, L.; Kopsahelis, N. Probiotics in Food Systems: Significance and Emerging Strategies Towards Improved Viability and Delivery of Enhanced Beneficial Value. Nutrients 2019, 11, 1591. [Google Scholar] [CrossRef]
- Hadjimbei, E.; Botsaris, G.; Chrysostomou, S. Beneficial Effects of Yoghurts and Probiotic Fermented Milks and Their Functional Food Potential. Foods 2022, 11, 2691. [Google Scholar] [CrossRef]
- Marco, M.L.; Heeney, D.; Binda, S.; Cifelli, C.J.; Cotter, P.D.; Foligné, B.; Gänzle, M.; Kort, R.; Pasin, G.; Pihlanto, A.; et al. Health benefits of fermented foods: Microbiota and beyond. Curr. Opin. Biotechnol. 2017, 44, 94–102. [Google Scholar] [CrossRef]
- Sağiroğlu, A.; Özdemir, N.; Çon, A.H. Multifunctional Potentials of Lactic Acid Bacterial Isolates from Turkish Traditional Fermented Foods. Lett. Appl. Microbiol. 2023, 76, 1–14. [Google Scholar] [CrossRef]
- Butler, M.I.; Bastiaanssen, T.F.S.; Long-Smith, C.; Berding, K.; Morkl, S.; Cusack, A.-M.; Strain, C.; Busca, K.; Porteous-Allen, P.; Claesson, M.J.; et al. Recipe for a Healthy Gut: Intake of Unpasteurised Milk Is Associated with Increased Lactobacillus Abundance in the Human Gut Microbiome. Nutrients 2020, 12, 1468. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.-Y.; Kim, K.-S.; Kim, S. Effects of yogurt containing probiotics on respiratory virus infections: Influenza H1N1 and SARS-CoV-2. J. Dairy Sci. 2023, 106, 1549–1561. [Google Scholar] [CrossRef] [PubMed]
- Steiner, N.C.; Lorentz, A. Probiotic Potential of Lactobacillus Species in Allergic Rhinitis. Int. Arch. Allergy Immunol. 2021, 182, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Matsumoto, K.; Matsumoto, N.; Kobatake, E.; Kabuki, T. Anti-allergic effect of Lactobacillus helveticus SBT2171 on murine model of pollen allergy. Funct. Foods Health Dis. 2019, 9, 166. [Google Scholar] [CrossRef]
- Peng, G.-C.; Hsu, C.-H. The efficacy and safety of heat-killed Lactobacillus paracasei for treatment of perennial allergic rhinitis induced by house-dust mite. Pediatr. Allergy Immunol. 2005, 16, 433–438. [Google Scholar] [CrossRef]
- Haghighat, L.; Crum-Cianflone, N.F. The potential risks of probiotics among HIV-infected persons: Bacteraemia due to Lactobacillus acidophilus and review of the literature. Int. J. STD AIDS 2016, 27, 1223–1230. [Google Scholar] [CrossRef]
- Joshi, S.; Udani, S.; Sen, S.; Kirolikar, S.; Shetty, A. Bacillus Clausii Septicemia in a Pediatric Patient After Treatment with Probiotics. Pediatr. Infect. Dis. J. 2019, 38, e228–e230. [Google Scholar] [CrossRef]
- Vahabnezhad, E.; Mochon, A.B.; Wozniak, L.; Ziring, D.A. Lactobacillus Bacteremia Associated with Probiotic Use in a Pediatric Patient With Ulcerative Colitis. J. Clin. Gastroenterol. 2013, 47, 437–439. [Google Scholar] [CrossRef]
- Ishida, Y.; Nakamura, F.; Kanzato, H.; Sawada, D.; Hirata, H.; Nishimura, A.; Kajimoto, O.; Fujiwara, S. Clinical Effects of Lactobacillus acidophilus Strain L-92 on Perennial Allergic Rhinitis: A Double-Blind, Placebo-Controlled Study. J. Dairy Sci. 2005, 88, 527–533. [Google Scholar] [CrossRef]
- Kalliomäki, M.; Salminen, S.; Arvilommi, H.; Kero, P.; Koskinen, P.; Isolauri, E. Probiotics in primary prevention of atopic disease: A randomised placebo-controlled trial. Lancet 2001, 357, 1076–1079. [Google Scholar] [CrossRef] [PubMed]
- Kawase, M.; He, F.; Kubota, A.; Hata, J.-Y.; Kobayakawa, S.-I.; Hiramatsu, M. Inhibitory Effect of Lactobacillus gasseri TMC0356 and Lactobacillus GG on Enhanced Vascular Permeability of Nasal Mucosa in Experimental Allergic Rhinitis of Rats. Biosci. Biotechnol. Biochem. 2006, 70, 3025–3030. [Google Scholar] [CrossRef]
- Kawase, M.; He, F.; Kubota, A.; Harata, G.; Hiramatsu, M. Orally Administrated Lactobacillus gasseri TMC0356 and Lactobacillus GG Alleviated Nasal Blockage of Guinea Pig with Allergic Rhinitis. Microbiol. Immunol. 2007, 51, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Majamaa, H.; Isolauri, E. Probiotics: A novel approach in the management of food allergy. J. Allergy Clin. Immunol. 1997, 99, 179–185. [Google Scholar] [CrossRef]
- Morita, H.; He, F.; Kawase, M.; Kubota, A.; Hiramatsu, M.; Kurisaki, J.-I.; Salminen, S. Preliminary Human Study for Possible Alteration of Serum Immunoglobulin E Production in Perennial Allergic Rhinitis with Fermented Milk Prepared with Lactobacillus gasseri TMC0356. Microbiol. Immunol. 2006, 50, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Nabe, T.; Mizutani, N.; Osaki, S.; Sugahara, S.; Takenaka, H.; Kohno, S. Comparison of Cedar Pollen-Induced Allergic Rhinitis in Passively and Actively Sensitized Guinea Pigs. Jpn. J. Pharmacol. 2001, 85, 409–415. [Google Scholar] [CrossRef]
- Martínez-Cañavate, A.; Sierra, S.; Lara-Villoslada, F.; Romero, J.; Maldonado, J.; Boza, J.; Xaus, J.; Olivares, M. A probiotic dairy product containing L. gasseri CECT5714 and L. coryniformis CECT5711 induces immunological changes in children suffering from allergy. Pediatr. Allergy Immunol. 2009, 20, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Agostoni, C.; Riva, E.; Salvini, F.; Ruscitto, A.; Zuccotti, G.V.; Radaelli, G. A Randomized Prospective Double Blind Controlled Trial on Effects of Long-Term Consumption of Fermented Milk Containing Lactobacillus casei in Pre-School Children with Allergic Asthma and/or Rhinitis. Pediatr. Res. 2007, 62, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.F.; Lin, H.C.; Wang, Y.Y.; Hsu, C.H. Treatment of perennial allergic rhinitis with lactic acid bacteria. Pediatr. Allergy Immunol. 2004, 15, 152–158. [Google Scholar] [CrossRef]
- Lin, W.-Y.; Fu, L.-S.; Lin, H.-K.; Shen, C.-Y.; Chen, Y.-J. Evaluation of the Effect of Lactobacillus paracasei (HF.A00232) in Children (6–13 years old) with Perennial Allergic Rhinitis: A 12-week, Double-blind, Randomized, Placebo-controlled Study. Pediatr. Neonatol. 2014, 55, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Vliagoftis, H.; Kouranos, V.; Betsi, G.I.; Falagas, M.E. Probiotics for the treatment of allergic rhinitis and asthma: Systematic review of randomized controlled trials. Ann. Allergy Asthma Immunol. 2008, 101, 570–579. [Google Scholar] [CrossRef]
- Costa, D.J.; Marteau, P.; Amouyal, M.; Poulsen, L.K.; Hamelmann, E.; Cazaubiel, M.; Housez, B.; Leuillet, S.; Stavnsbjerg, M.; Molimard, P.; et al. Efficacy and safety of the probiotic Lactobacillus paracasei LP-33 in allergic rhinitis: A double-blind, randomized, placebo-controlled trial (GA2LEN Study). Eur. J. Clin. Nutr. 2014, 68, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Zuccotti, G.V.; Meneghin, F.; Aceti, A.; Barone, G.; Callegari, M.L.; Di Mauro, A.; Fantini, M.P.; Gori, D.; Indrio, F.; Maggio, L.; et al. Probiotics for prevention of atopic diseases in infants: Systematic review and meta-analysis. Allergy 2015, 70, 1356–1371. [Google Scholar] [CrossRef] [PubMed]
- Vilà-Nadal, G.; Phillips-Anglés, E.; Domínguez-Ortega, J. The Use of Probiotics in Respiratory Allergy. J. Pharm. Nutr. Sci. 2016, 6, 89–94. [Google Scholar] [CrossRef]
- Ahmed, M.; Billoo, A.G.; Iqbal, K. Efficacy of probiotic in perennial allergic rhinitis under five year children: A randomized controlled trial. Pak. J. Med. Sci. 2019, 35, 1538–1543. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Aste-Amezaga, M.; Valiante, N.M.; Ma, X.; Kubin, M.; Trinchieri, G. Interleukin 10 (IL-10) inhibits human lymphocyte interferon gamma-production by suppressing natural killer cell stimulatory factor/IL-12 synthesis in accessory cells. J. Exp. Med. 1993, 178, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Groux, H.; Bigler, M.; EDe Vries, J.E.; Roncarolo, M.G. Interleukin-10 induces a long-term antigen-specific anergic state in human CD4+ T cells. J. Exp. Med. 1996, 184, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Ishida, Y.; Nakamura, F.; Kanzato, H.; Sawada, D.; Yamamoto, N.; Kagata, H.; Oh-Ida, M.; Takeuchi, H.; Fujiwara, S. Effect of Milk Fermented with Lactobacillus acidophilus Strain L-92 on Symptoms of Japanese Cedar Pollen Allergy: A Randomized Placebo-Controlled Trial. Biosci. Biotechnol. Biochem. 2005, 69, 1652–1660. [Google Scholar] [CrossRef]
- Tamura, M.; Shikina, T.; Morihana, T.; Hayama, M.; Kajimoto, O.; Sakamoto, A.; Kajimoto, Y.; Watanabe, O.; Nonaka, C.; Shida, K.; et al. Effects of Probiotics on Allergic Rhinitis Induced by Japanese Cedar Pollen: Randomized Double-Blind, Placebo-Controlled Clinical Trial. Int. Arch. Allergy Immunol. 2006, 143, 75–82. [Google Scholar] [CrossRef]
- Xiao, J.-Z.; Kondo, S.; Yanagisawa, N.; Takahashi, N.; Odamaki, T.; Iwabuchi, N.; Miyaji, K.; Iwatsuki, K.; Togashi, H.; Enomoto, K. Probiotics in the treatment of Japanese cedar pollinosis: A double-blind placebo-controlled trial. Clin. Exp. Allergy 2006, 36, 1425–1435. [Google Scholar] [CrossRef]
- Lin, T.-Y.; Chen, C.-J.; Chen, L.-K.; Wen, S.-H.; Jan, R.-H. Effect of probiotics on allergic rhinitis in Df, Dp or dust-sensitive children: A randomized double blind controlled trial. Indian Pediatr. 2013, 50, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Miyoshi, M.; Iwai, M.; Takeda, R.; Ono, T.; Kabuki, T. Lactobacillus helveticus SBT2171 Alleviates Perennial Allergic Rhinitis in Japanese Adults by Suppressing Eosinophils: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2020, 12, 3620. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Fang, Z.; Liu, X.; Hu, W.; Lu, W.; Lee, Y.-K.; Zhao, J.; Zhang, H.; Chen, W. Lactobacillus reuteri attenuated allergic inflammation induced by HDM in the mouse and modulated gut microbes. PLoS ONE 2020, 15, e0231865. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Fang, Z.; Liu, Z.; Zhao, J.; Zhang, H.; Wang, S.; He, J.; Lu, W.; Chen, W. Lactobacillus reuteri CCFM1072 and CCFM1040 with the role of Treg cells regulation alleviate airway inflammation through modulating gut microbiota in allergic asthma mice. J. Funct. Foods 2020, 76, 104286. [Google Scholar] [CrossRef]
- Cervantes-Barragan, L.; Chai, J.N.; Tianero, M.D.; Di Luccia, B.; Ahern, P.P.; Merriman, J.; Cortez, V.S.; Caparon, M.G.; Donia, M.S.; Gilfillan, S.; et al. Lactobacillus reuteri induces gut intraepithelial CD4+CD8αα+T cells. Science 2017, 357, 806–810. [Google Scholar] [CrossRef] [PubMed]
- Zelante, T.; Iannitti, R.G.; Cunha, C.; De Luca, A.; Giovannini, G.; Pieraccini, G.; Zecchi, R.; D’Angelo, C.; Massi-Benedetti, C.; Fallarino, F.; et al. Tryptophan catabolites from microbiota engage aryl hydrocarbon receptor and balance mucosal reactivity via interleukin-22. Immunity 2013, 39, 372–385. [Google Scholar] [CrossRef]
- Kepert, I.; Fonseca, J.; Müller, C.; Milger, K.; Hochwind, K.; Kostric, M.; Fedoseeva, M.; Ohnmacht, C.; Dehmel, S.; Nathan, P.; et al. D-tryptophan from probiotic bacteria influences the gut microbiome and allergic airway disease. J. Allergy Clin. Immunol. 2017, 139, 1525–1535. [Google Scholar] [CrossRef]
- Li, L.; Fang, Z.; Lee, Y.-K.; Zhao, J.; Zhang, H.; Peng, H.; Zhang, Y.; Lu, W.; Chen, W. Efficacy and Safety of Lactobacillus reuteri CCFM1040 in Allergic Rhinitis and Asthma: A Randomized, Placebo-Controlled Trial. Front. Nutr. 2022, 9, 862934. [Google Scholar] [CrossRef]
- Choi, S.-P.; Oh, H.-N.; Choi, C.-Y.; Ahn, H.; Yun, H.; Chung, Y.; Kim, B.; Lee, S.; Chun, T. Oral administration of Lactobacillus plantarum CJLP133 and CJLP243 alleviates birch pollen-induced allergic rhinitis in mice. J. Appl. Microbiol. 2017, 124, 821–828. [Google Scholar] [CrossRef]
- Pennock, B.E.; Cox, C.P.; Rogers, R.M.; Cain, W.A.; Wells, J.H. A noninvasive technique for measurement of changes in specific airway resistance. J. Appl. Physiol. 1979, 46, 399–406. [Google Scholar] [CrossRef]
- Chen, Y.-S.; Lin, Y.-L.; Jan, R.-L.; Chen, H.-H.; Wang, J.-Y. Randomized placebo-controlled trial of lactobacillus on asthmatic children with allergic rhinitis. Pediatr. Pulmonol. 2010, 45, 1111–1120. [Google Scholar] [CrossRef]
- Olivares, M.; Díaz-Ropero, M.P.; Gómez, N.; Lara-Villoslada, F.; Sierra, S.; Maldonado, J.A.; Martín, R.; Lopez-Huertas, E.; Rodríguez, J.; Xaus, J. Oral administration of two probiotic strains, Lactobacillus gasseri CECT5714 and Lactobacillus coryniformis CECT5711, enhances the intestinal function of healthy adults. Int. J. Food Microbiol. 2006, 107, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Olivares, M.; Díaz-Ropero, M.P.; Gómez, N.; Lara-Villoslada, F.; Sierra, S.; Maldonado, A.J.; Martín, R.; Rodríguez, J.M.; Xaus, J. The consumption of two new probiotic strains, Lactobacillus gasseri CECT 5714 and Lactobacillus coryniformis CECT 5711, boosts the immune system of healthy humans. Int. Microbiol. 2006, 9, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Olivares, M.; Díaz-Ropero, M.P.; Gómez, N.; Sierra, S.; Lara-Villoslada, F.; Martín, R.; Rodríguez, J.M.; Xaus, J. Dietary deprivation of fermented foods causes a fall in innate immune response. Lactic acid bacteria can counteract the immunological effect of this deprivation. J. Dairy Res. 2006, 73, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Lara-Villoslada, F.S.S. [Beneficial Effects of Consumption of a Dairy Product Containing Two Probiotic Strains, Lactobacillus coryniformis CECT5711 and Lactobacillus gasseri CECT5714 in Healthy Children]-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/17650892/ (accessed on 24 November 2022).
- Wassenberg, J.; Nutten, S.; Audran, R.; Barbier, N.; Aubert, V.; Moulin, J.; Mercenier, A.; Spertini, F. Effect of Lactobacillus paracasei ST11 on a nasal provocation test with grass pollen in allergic rhinitis. Clin. Exp. Allergy 2011, 41, 565–573. [Google Scholar] [CrossRef]
- Perrin, Y.; Nutten, S.; Audran, R.; Berger, B.; Bibiloni, R.; Wassenberg, J.; Barbier, N.; Aubert, V.; Moulin, J.; Singh, A.; et al. Comparison of two oral probiotic preparations in a randomized crossover trial highlights a potentially beneficial effect of Lactobacillus paracasei NCC2461 in patients with allergic rhinitis. Clin. Transl. Allergy 2014, 4, 1. [Google Scholar] [CrossRef]
- Ouwehand, A.C.; Nermes, M.; Collado, M.C.; Rautonen, N.; Salminen, S.; Isolauri, E. Specific probiotics alleviate allergic rhinitis during the birch pollen season. World J. Gastroenterol. 2009, 15, 3261–3268. [Google Scholar] [CrossRef]
- Nembrini, C.; Singh, A.; De Castro, C.A.; Mercenier, A.; Nutten, S. Oral administration of Lactobacillus paracasei NCC 2461 for the modulation of grass pollen allergic rhinitis: A randomized, placebo-controlled study during the pollen season. Clin. Transl. Allergy 2015, 5, 41. [Google Scholar] [CrossRef]
- Helin, T.; Haahtela, S. No effect of oral treatment with an intestinal bacterial strain, Lactobacillus rhamnosus (ATCC 53103), on birch-pollen allergy: A placebo-controlled double-blind study. Allergy 2002, 57, 243–246. [Google Scholar] [CrossRef]
- Hidalgo-Cantabrana, C.; Delgado, S.; Ruiz, L.; Ruas-Madiedo, P.; Sánchez, B.; Margolles, A. Bifidobacteria and Their Health-Promoting Effects. Microbiol. Spectr. 2017, 5. [Google Scholar] [CrossRef]
- Ficara, M.; Pietrella, E.; Spada, C.; Muttini, E.D.C.; Lucaccioni, L.; Iughetti, L.; Berardi, A. Changes of intestinal microbiota in early life. J. Matern. Neonatal Med. 2018, 33, 1036–1043. [Google Scholar] [CrossRef]
- Kim, W.-G.; Kang, G.-D.; Kim, H.; Han, M.; Kim, D.-H. Bifidobacterium longum IM55 and Lactobacillus plantarum IM76 alleviate allergic rhinitis in mice by restoring Th2/Treg imbalance and gut microbiota disturbance. Benef. Microbes 2019, 10, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Zhao, Y.; Huang, S.; Lv, D.; Yang, F.; Lou, L.; Zheng, Y.; Zhang, J.; Liu, S.; Zhang, N.; et al. Immunomodulatory effect of Bifidobacterium breve on experimental allergic rhinitis in BALB/c mice. Exp. Ther. Med. 2018, 16, 3996–4004. [Google Scholar] [CrossRef]
- Tsunemine, S.; Isa, Y.; Shimakawa, M.; Ohno, H.; Yamamura, H. Effects of Bifidobacterium bifidum G9-1 on Nasal Symptoms in a Guinea Pig Model of Experimental Allergic Rhinitis. Biosci. Microflora 2011, 30, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Di Pierro, F.; Basile, I.; Danza, M.L.; Venturelli, L.; Contini, R.; Risso, P.; Colombo, M. Use of a probiotic mixture containing Bifidobacterium animalis subsp. lactis BB12 and Enterococcus faecium L3 in atopic children. Minerva Pediatr. 2018, 70, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, M.M.; Indolfi, C.; Capasso, M.; Maiello, N.; Decimo, F.; Ciprandi, G. Bifidobacterium mixture (B longum BB536, B infantis M-63, B breve M-16V) treatment in children with seasonal allergic rhinitis and intermittent asthma. Ital. J. Pediatr. 2017, 43, 25. [Google Scholar] [CrossRef]
- Rho, M.-K.; Kim, Y.-E.; Rho, H.-I.; Kim, T.-R.; Kim, Y.-B.; Sung, W.-K.; Kim, T.-W.; Kim, D.-O.; Kang, H. Enterococcus faecium FC-K Derived from Kimchi Is a Probiotic Strain That Shows Anti-Allergic Activity. J. Microbiol. Biotechnol. 2017, 27, 1071–1077. [Google Scholar] [CrossRef]
- Luping, Z.; Takashi, S.; Ruoxi, C.; Meiping, L.; Qingzhao, Z.; Wenmin, L.; Min, Y.; Tadao, E.; Lei, C. Effects of lysed Enterococcus faecalis FK-23 on experimental allergic rhinitis in a murine model. J. Biomed. Res. 2012, 26, 226–234. [Google Scholar] [CrossRef]
- Lo Skiavo LA, G.N. [Dynamics of Contamination and Persistence of Clostridium difficile in Intestinal Microbiota in Newborn Infants during Antibiotic Therapy and Use of Probiotic Strain Enterococcus Faecium L3]-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/24734423/ (accessed on 24 November 2022).
- Anania, C.; Di Marino, V.; Olivero, F.; De Canditiis, D.; Brindisi, G.; Iannilli, F.; De Castro, G.; Zicari, A.; Duse, M. Treatment with a Probiotic Mixture Containing Bifidobacterium animalis Subsp. Lactis BB12 and Enterococcus faecium L3 for the Prevention of Allergic Rhinitis Symptoms in Children: A Randomized Controlled Trial. Nutrients 2021, 13, 1315. [Google Scholar] [CrossRef]
- Fang, G.X.; Li, Z.; Su, C.; Hu, G.H. Clinical observation of saccharomyces boulardii combined with cetirizine hydrochloride in children allergic rhinitis. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2017, 31, 1649–1652. [Google Scholar] [CrossRef]
- Louis, P.; Flint, H.J. Diversity, metabolism and microbial ecology of butyrate-producing bacteria from the human large intestine. FEMS Microbiol. Lett. 2009, 294, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Van Immerseel, F.; Ducatelle, R.; De Vos, M.; Boon, N.; Van De Wiele, T.; Verbeke, K.; Rutgeerts, P.; Sas, B.; Louis, P.; Flint, H.J. Butyric acid-producing anaerobic bacteria as a novel probiotic treatment approach for inflammatory bowel disease. J. Med. Microbiol. 2010, 59, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Sokol, H.; Pigneur, B.; Watterlot, L.; Lakhdari, O.; Bermúdez-Humaran, L.G.; Gratadoux, J.-J.; Blugeon, S.; Bridonneau, C.; Furet, J.-P.; Corthier, G.; et al. Faecalibacterium prausnitzii is an anti-inflammatory commensal bacterium identified by gut microbiota analysis of Crohn disease patients. Proc. Natl. Acad. Sci. USA 2008, 105, 16731–16736. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, M.; Akagawa, S.; Akagawa, Y.; Nakai, Y.; Yamanouchi, S.; Kimata, T.; Hashiyada, M.; Akane, A.; Tsuji, S.; Kaneko, K. Decreased butyric acid-producing bacteria in gut microbiota of children with egg allergy. Allergy 2021, 76, 2279–2282. [Google Scholar] [CrossRef] [PubMed]
- Roduit, C.; Frei, R.; Ferstl, R.; Loeliger, S.; Westermann, P.; Rhyner, C.; Schiavi, E.; Barcik, W.; Rodriguez-Perez, N.; Wawrzyniak, M.; et al. High levels of butyrate and propionate in early life are associated with protection against atopy. Allergy 2018, 74, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Akagawa, S.; Kaneko, K. Gut microbiota and allergic diseases in children. Allergol. Int. 2022, 71, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Berni Canani, R.; Sangwan, N.; Stefka, A.; Nocerino, R.; Paparo, L.; Aitoro, R.; Calignano, A.; Khan, A.A.; Gilbert, J.; Nagler, C.R. Lactobacillus rhamnosus GG-supplemented formula expands butyrate-producing bacterial strains in food allergic infants. ISME J. 2016, 10, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, A.; Pawankar, R.; Cuello-Garcia, C.; Ahn, K.; Al-Hammadi, S.; Agarwal, A.; Beyer, K.; Burks, W.; Canonica, G.W.; Ebisawa, M.; et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics. World Allergy Organ. J. 2015, 8, 1–4. [Google Scholar] [CrossRef]
- Koren, O.; Goodrich, J.K.; Cullender, T.C.; Spor, A.; Laitinen, K.; Bäckhed, H.K.; Gonzalez, A.; Werner, J.J.; Angenent, L.T.; Knight, R.; et al. Host Remodeling of the Gut Microbiome and Metabolic Changes during Pregnancy. Cell 2012, 150, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Obuchowska, A.; Gorczyca, K.; Standyło, A.; Obuchowska, K.; Kimber-Trojnar, Ż.; Wierzchowska-Opoka, M.; Leszczyńska-Gorzelak, B. Effects of Probiotic Supplementation during Pregnancy on the Future Maternal Risk of Metabolic Syndrome. Int. J. Mol. Sci. 2022, 23, 8253. [Google Scholar] [CrossRef]
- Kuperman, A.A.; Koren, O. Antibiotic use during pregnancy: How bad is it? BMC Med. 2016, 14, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gomez de Agüero, M.; Ganal-Vonarburg, S.C.; Fuhrer, T.; Rupp, S.; Uchimura, Y.; Li, H.; Steinert, A.; Heikenwalder, M.; Hapfelmeier, S.; Sauer, U.; et al. The maternal microbiota drives early postnatal innate immune development. Science 2016, 351, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Neuman, H.; Koren, O. The Pregnancy Microbiome. Nestle Nutr. Inst. Workshop Ser. 2017, 88, 1–9. [Google Scholar] [CrossRef]
- Aagaard, K.; Riehle, K.; Ma, J.; Segata, N.; Mistretta, T.-A.; Coarfa, C.; Raza, S.; Rosenbaum, S.; Veyver, I.V.D.; Milosavljevic, A.; et al. A Metagenomic Approach to Characterization of the Vaginal Microbiome Signature in Pregnancy. PLoS ONE 2012, 7, e36466. [Google Scholar] [CrossRef] [PubMed]
- Lundelin, K.; Poussa, T.; Salminen, S.; Isolauri, E. Long-term safety and efficacy of perinatal probiotic intervention: Evidence from a follow-up study of four randomized, double-blind, placebo-controlled trials. Pediatr. Allergy Immunol. 2016, 28, 170–175. [Google Scholar] [CrossRef]
- Bertelsen, R.J.; Brantsæter, A.L.; Magnus, M.C.; Haugen, M.; Myhre, R.; Jacobsson, B.; Longnecker, M.P.; Meltzer, H.M.; London, S.J. Probiotic milk consumption in pregnancy and infancy and subsequent childhood allergic diseases. J. Allergy Clin. Immunol. 2013, 133, 165–171.e8. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Wang, L.; Wu, S.; Yuan, L.; Tang, S.; Xiang, Y.; Qu, X.; Liu, H.; Qin, X.; Liu, C. Efficacy of probiotic supplementary therapy for asthma, allergic rhinitis, and wheeze: A meta-analysis of randomized controlled trials. Allergy Asthma Proc. 2019, 40, 250–260. [Google Scholar] [CrossRef]
- Arango, L.F.G.; Barrett, H.L.; Callaway, L.K.; Nitert, M.D. Probiotics and Pregnancy. Curr. Diabetes Rep. 2014, 15, 1–9. [Google Scholar] [CrossRef]
- Sohn, K.; Underwood, M.A. Prenatal and postnatal administration of prebiotics and probiotics. Semin. Fetal Neonatal Med. 2017, 22, 284–289. [Google Scholar] [CrossRef]
- Boyle, R.J.; Ismail, I.H.; Kivivuori, S.; Licciardi, P.V.; Robins-Browne, R.M.; Mah, L.-J.; Axelrad, C.; Moore, S.; Donath, S.; Carlin, J.B.; et al. Lactobacillus GG treatment during pregnancy for the prevention of eczema: A randomized controlled trial. Allergy 2010, 66, 509–516. [Google Scholar] [CrossRef]
- Simpson, M.R.; Dotterud, C.K.; Storrø, O.; Johnsen, R.; Øien, T. Perinatal probiotic supplementation in the prevention of allergy related disease: 6 year follow up of a randomised controlled trial. BMC Dermatol. 2015, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.L.; Dunstan, J.A.; Prescott, S.L. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: A randomized controlled trial. J. Allergy Clin. Immunol. 2007, 119, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Wise, S.K.; Lin, S.Y.; Toskala, E.; Orlandi, R.R.; Akdis, C.A.; Alt, J.A.; Azar, A.; Baroody, F.M.; Bachert, C.; Canonica, G.W.; et al. International Consensus Statement on Allergy and Rhinology: Allergic Rhinitis. Int. Forum Allergy Rhinol. 2018, 8, 108–352. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Objective | Population | Methods | Results |
|---|---|---|---|---|
| Giovannini et al., Pediatr Res. 2007 [59] | To investigate whether long-term consumption of fermented milk containing Lactobacillus casei (LC) may improve the health status of preschool children suffering from allergic asthma and/or rhinitis. | 187 children 2–5 years of age with diagnosis of allergic asthma and/or AR proved by prick test. | Patients received 12 months of either fermented milk with LC (92 patients) or a placebo (95 patients). The number of fever or diarrhea episodes and the recurrence of asthma and rhinitis symptoms were recorded. The change in serum immunoglobulin (IgA, IgE, IgG, and IgM) were measured. | As compared to the control group, in the LC group:
|
| Lin et al., Indian Pediatr. 2013 [72] | To examine the effect of Lactobacillus salivarius (LS) on the symptoms and medication use among children AR. | 199 children aged 6 to 12 years with a history of perennial allergic symptoms for at least three years with a positive skin prick test for Dermatophagoides farinae (DF) or Dermatophagoides pteronyssinus (DP). | All enrolled patients were randomly assigned either to the L. salivarius group or the placebo group (120 patients each). The 12-week course of treatment was followed by a 7-month surveillance period. At each visit, the severity of the child’s AR was assessed using the specific symptoms scores (SSS) and symptom medication scores (SMS). In addition, parents were required to keep a weekly journal of their child’s AR status. Blood samples were also collected. | In comparison to the untreated group (UT):
|
| Lin et al., Pediatr Neonatol. 2014 [61] | To evaluate the effects of Lactobacillus paracasei (LP), strain HF.A00232, as a supplementary agent to levocetirizine in treating children with perennial AR. | 60 patients aged 6–13 years with perennial AR longer than one year, with house dust mites allergy. | All patients were randomized into two groups: 28 were treated with levocetirizine plus placebo for 12 weeks and 32 with levocetirizine plus LP for the first 8 weeks, with a shift to usage of levocetirizine as rescue treatment during the last 4 weeks. At the initial screening visit, blood samples (to test for mite-specific IgE) and medical and allergy history were collected. Additionally, daily symptom diaries were given. At each visit, the Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ), Total symptom score (TSS), and nasal total symptom score (NTSS) were administered. Blood samples were taken to evaluate inflammatory cytokines at baseline and at week 8 and 12. | In comparison to the placebo group:
|
| Ouwehand et al., World J Gastroenterol 2009 [89] | To investigate whether birch pollen allergy symptoms are linked with gut microbiota changes and whether probiotics (Lactobacillus acidophilus (LA) and Bifidobacterium lactis (BL)) affect these. | 41 children (4–12 years old) with confirmed birch pollen-AR. | Children were randomly distributed in two groups to receive either a combination of LA NCFMTM and BL Bl-04 (20 patients) or a placebo (21 patients) for 4 months, starting before the birch pollen season. Symptoms were noted in a diary. Blood and fecal samples were collected. | In comparison to the UT group:
|
| Ahmed et al., Pak J Med Sci. 2019 [66] | To evaluate the efficacy of Lactobacillus paracasei (LP-33), and compare it with cetirizine for the treatment of perennial AR in children. | 212 children aged 6 to 60 months affected by AR. | Children were randomized into intervention group A (106 patients), which received probiotic LP-33, and control group B (106 patients), which received cetirizine for 6 weeks. Baseline AR symptoms were assessed after a two- and six-week follow-up. | At first and second follow-up visits, both groups A and group B majority participants showed at first a partial, then a complete, significant improvement in their baseline AR symptoms. Except for the symptoms of cough and feeding difficulties, which at the first visit appeared to be better treated by cetirizine (p < 0.05), there was no statistically significant difference between the two groups. Treatments with probiotics and cetirizine for persistent AR in children under the age of five were equally beneficial. (p > 0.05). |
| Chen et al., Pediatr Pulmonol. 2010 [82] | To determine whether daily supplementation with Lactobacillus gasseri (LG) A5 for eight weeks may improve the symptoms and immunoregulatory changes in school children with asthma and AR. | 105 asthmatic children (6–12 years old) with persistent AR. | Children were randomized into the probiotic-treated group (1 capsule of LG twice a day) or the control group (milk powder). The participants underwent clinical examinations every 2 weeks. A final evaluation was performed at week 10. Additionally, data regarding the need for drugs (such as beta2 agonists and oral prednisone), and blood samples were collected. | A significant decrease in clinical symptom scores for asthma and AR was shown in the LG-treated group compared to the placebo-treated one. The asthmatic symptoms and objective airway function measurements improved significantly in allergic asthmatic children who received probiotic supplementation. In addition, the cytokine IL-10 decreased in the probiotic group. There was no significant difference in the serum total IgE level, the degree of allergen sensitization, and no significant elevation in the Th1 cytokines before and after probiotic treatment.The medication scores decreased significantly in the probiotic-treated and control groups, with no significant difference. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klain, A.; Dinardo, G.; Indolfi, C.; Contieri, M.; Salvatori, A.; Vitale, S.; Decimo, F.; Ciprandi, G.; Miraglia del Giudice, M. Efficacy and Safety of Oral Probiotics in Children with Allergic Rhinitis: A Review. Allergies 2023, 3, 72-89. https://doi.org/10.3390/allergies3010006
Klain A, Dinardo G, Indolfi C, Contieri M, Salvatori A, Vitale S, Decimo F, Ciprandi G, Miraglia del Giudice M. Efficacy and Safety of Oral Probiotics in Children with Allergic Rhinitis: A Review. Allergies. 2023; 3(1):72-89. https://doi.org/10.3390/allergies3010006
Chicago/Turabian StyleKlain, Angela, Giulio Dinardo, Cristiana Indolfi, Marcella Contieri, Alessandra Salvatori, Sossio Vitale, Fabio Decimo, Giorgio Ciprandi, and Michele Miraglia del Giudice. 2023. "Efficacy and Safety of Oral Probiotics in Children with Allergic Rhinitis: A Review" Allergies 3, no. 1: 72-89. https://doi.org/10.3390/allergies3010006
APA StyleKlain, A., Dinardo, G., Indolfi, C., Contieri, M., Salvatori, A., Vitale, S., Decimo, F., Ciprandi, G., & Miraglia del Giudice, M. (2023). Efficacy and Safety of Oral Probiotics in Children with Allergic Rhinitis: A Review. Allergies, 3(1), 72-89. https://doi.org/10.3390/allergies3010006