
Digitalization of Musculoskeletal Risk Assessment in a Robotic-Assisted Assembly Workstation

 ,
, 
 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
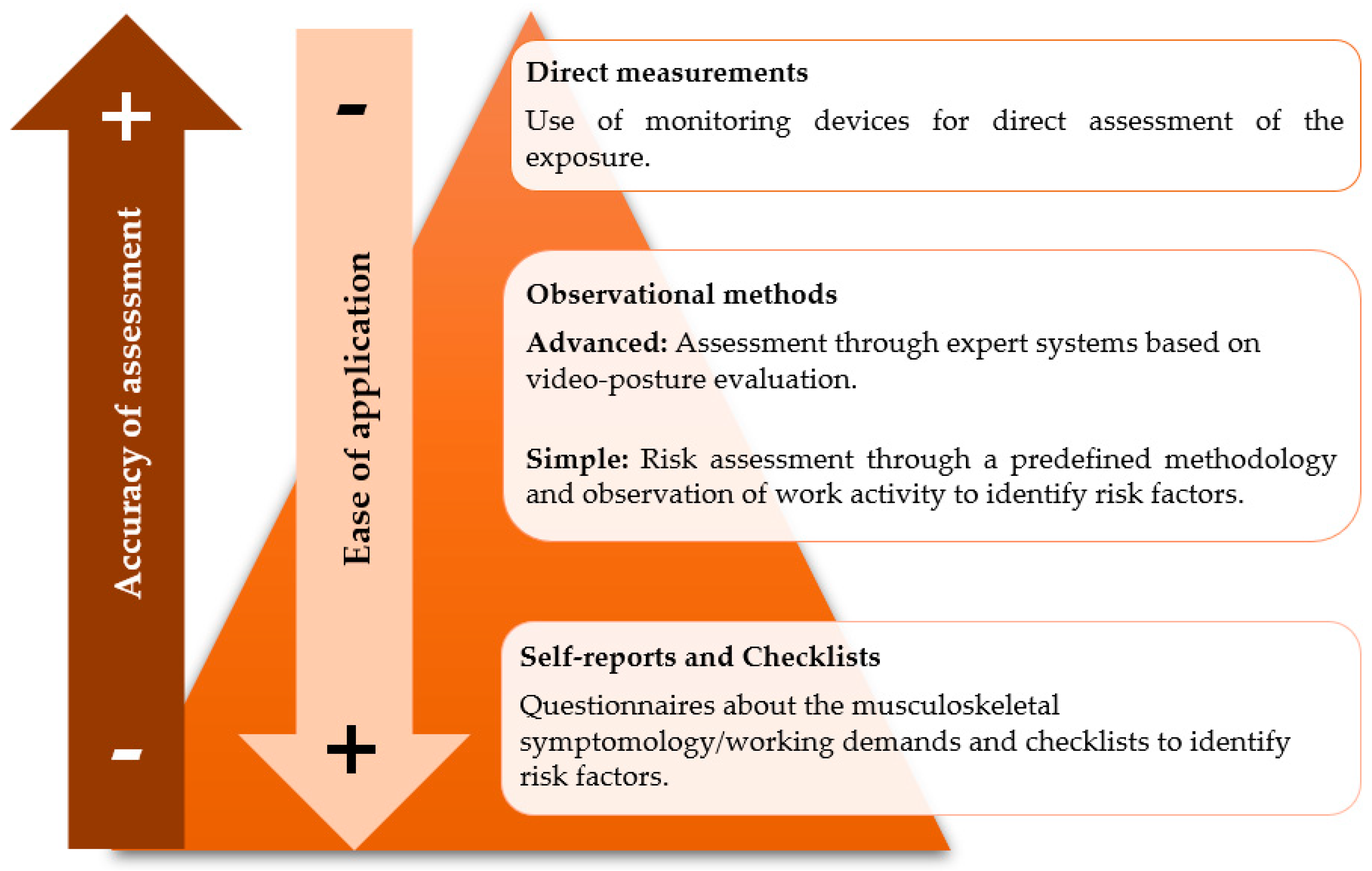
- (i)
- Self-reports and checklists collect more generic workers’ perceptions and/or identify risk factors;
- (ii)
- Observational methods may be subdivided into simple and advanced techniques/methods;
- (iii)
- (i)
- To compare the musculoskeletal risk before and after the robotic implementation of an assembly workstation using IMU-based technology;
- (ii)
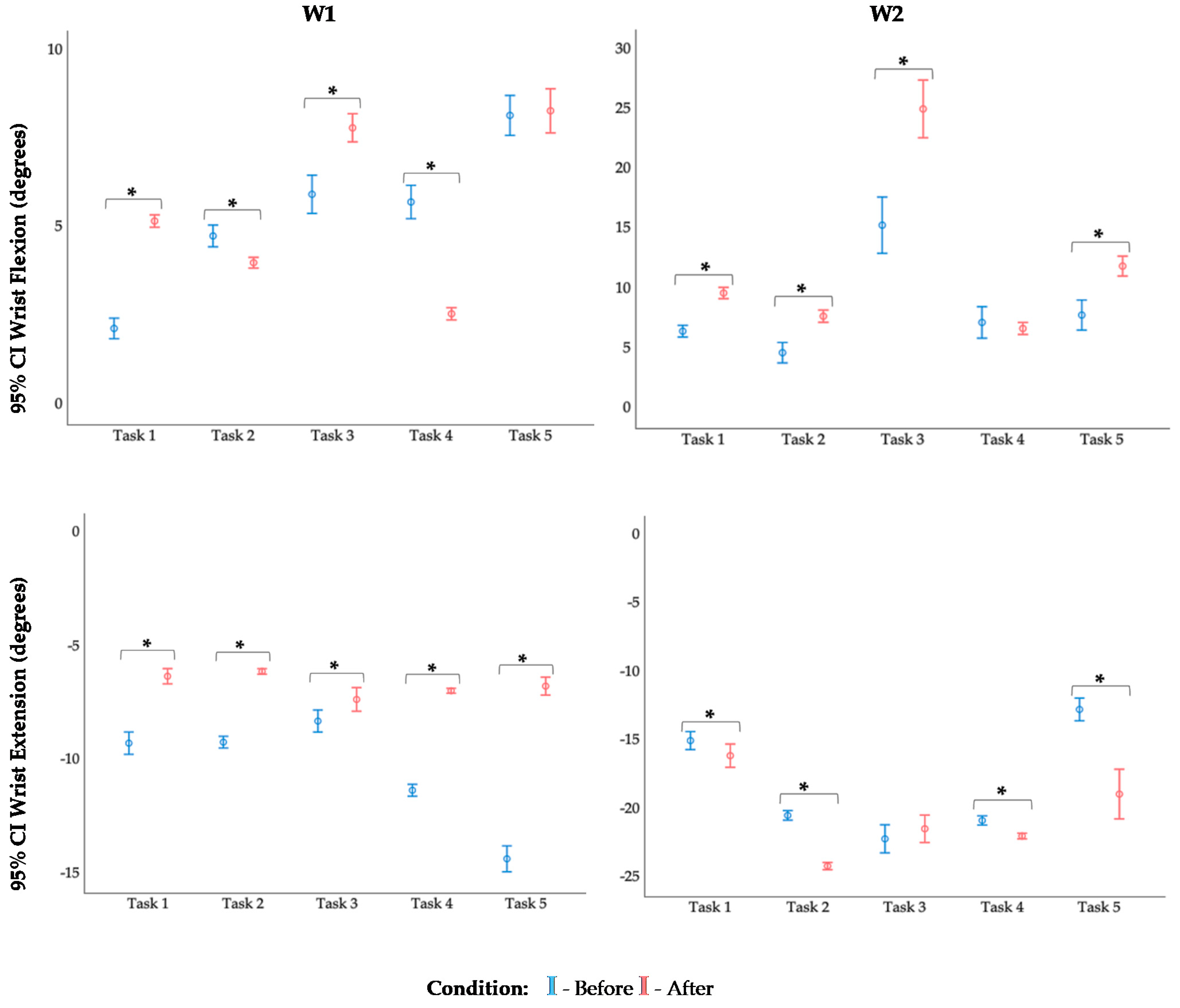
- To analyze wrist postures in detail during assembly tasks before and after the implementation;
- (iii)
- To highlight the importance of using this technology to assess musculoskeletal risk in real-industry manufacturing scenarios.
2. Materials and Methods
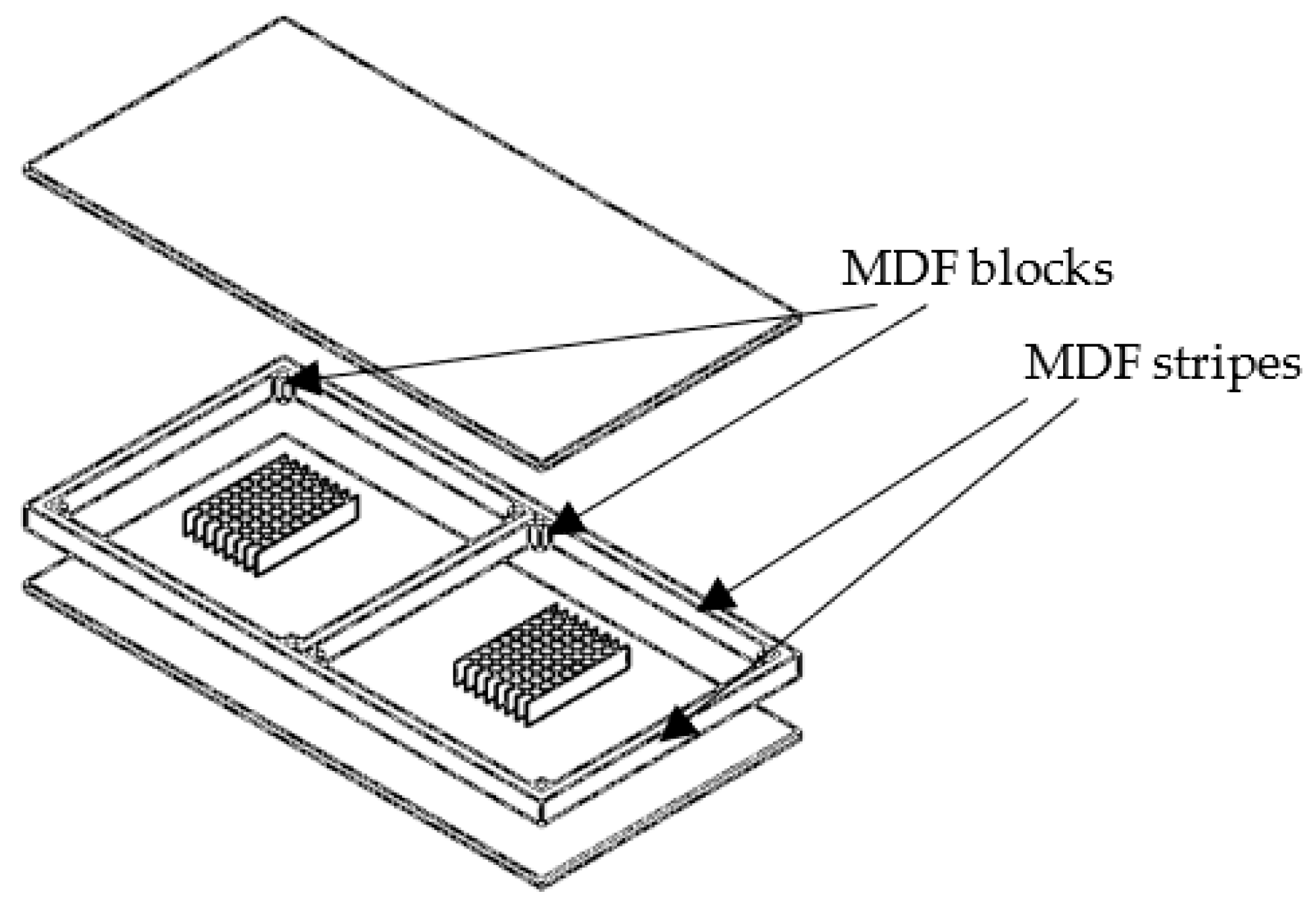
2.1. Participants and Assembly Workstation Description
2.2. Data Acquisition and Processing
2.3. Data Analysis
- (i)
- Flexion/Extension: z-axis;
- (ii)
- Ulnar/Radial deviation: x-axis;
- (iii)
- Pronation/Supination: y-axis.
2.4. Statistical Analysis
3. Results
4. Discussion
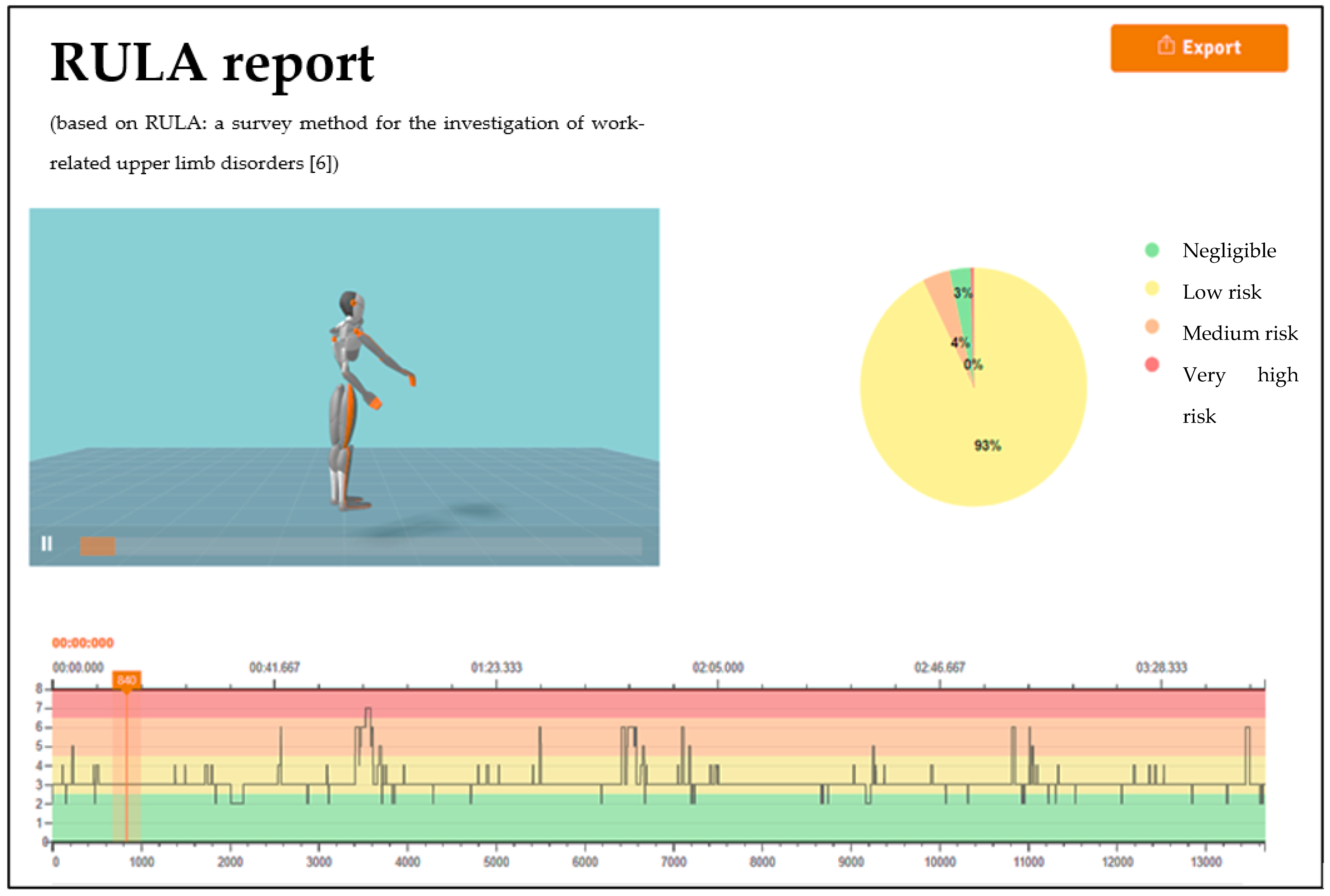
4.1. RULA Report
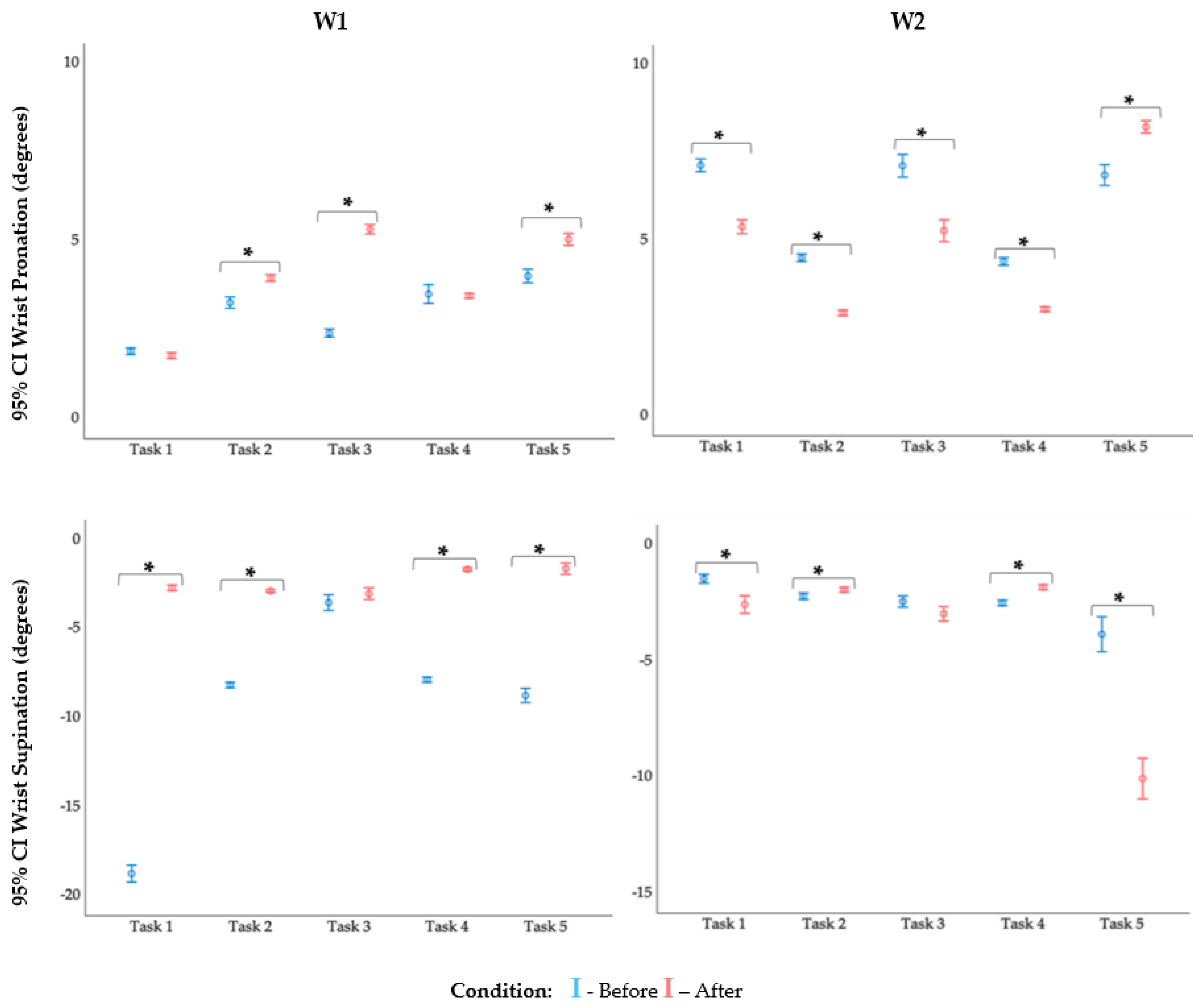
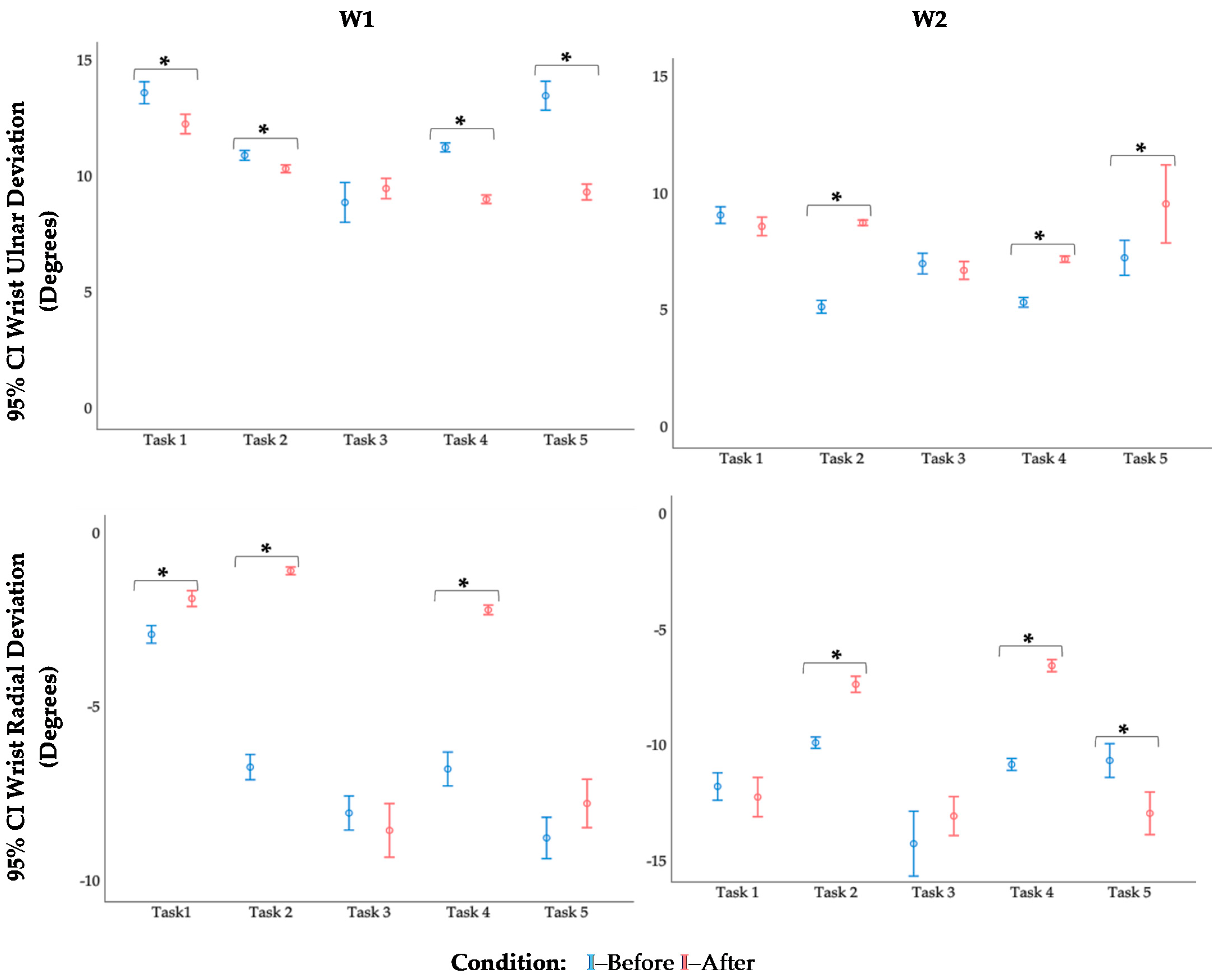
4.2. Kinematic Analysis of the Wrist
4.3. Limitations, Main Contributions, and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Petreanu, V.; Seracin, A.-M. Risk Factors for Musculoskeletal Disorders Development: Hand-Arm Tasks, Repetitive Work. Natl. Res.Dev. Heal. Safety Rom. 2017, 1–8. [Google Scholar]
- Guimarães, L.; Anzanello, M.J.; Ribeiro, J.L.D.; Saurin, T.A. Participatory Ergonomics Intervention for Improving Human and Production Outcomes of a Brazilian Furniture Company. Int. J. Ind. Ergon. 2015, 49, 97–107. [Google Scholar] [CrossRef]
- Colim, A.; Sousa, N.; Carneiro, P.; Costa, N.; Arezes, P.; Cardoso, A. Ergonomic Intervention on a Packing Workstation with Robotic Aid—Case Study at a Furniture Manufacturing Industry. Work. A J. Prev. Assess. Rehabil. 2020, 66, 229–237, article in press. [Google Scholar] [CrossRef] [PubMed]
- David, G. Ergonomic Methods for Assessing Exposure to Risk Factors for Work-Related Musculoskeletal Disorders. Occup. Med. 2005, 55, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Ellegast, R. Assessment of Physical Workloads to Prevent Work-Related MSDs; Institute for Occupational Safety and Health of the German Social Accident Insurance: Berlin, Germany, 2016. [Google Scholar]
- Hussain, I.; Park, S.J. Prediction of Myoelectric Biomarkers in Post-Stroke Gait. Sensors 2021, 21, 5334. [Google Scholar] [CrossRef]
- González, A.G.; Barrios-Muriel, J.; Romero-Sánchez, F.; Salgado, D.R.; Alonso, F.J. Ergonomic Assessment of a New Hand Tool Design for Laparoscopic Surgery Based on Surgeons’ Muscular Activity. Appl. Ergon. 2020, 88, 103161. [Google Scholar] [CrossRef]
- Colim, A.; Arezes, P.; Flores, P.; Monteiro, P.R.R.; Mesquita, I.; Braga, A.C. Obesity Effects on Muscular Activity during Lifting and Lowering Tasks. Int. J. Occup. Saf. Ergon. 2021, 27, 217–225. [Google Scholar] [CrossRef] [PubMed]
- McAtamney, L.; Corlett, N. RULA: A Survey Method for the Investigation of Work-Related Upper Limb Disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Plantard, P.; Shum, H.; Le Pierres, A.; Multon, F. Validation of an Ergonomic Assessment Method Using Kinect Data in Real Workplace Conditions. Appl. Ergon. 2017, 65, 562–569. [Google Scholar] [CrossRef]
- Abobakr, A.; Nahavandi, D.; Hossny, M.; Iskander, J.; Attia, M.; Nahavandi, S.; Smets, M. RGB-D Ergonomic Assessment System of Adopted Working Postures. Appl. Ergon. 2019, 80, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Colim, A.; Morgado, R.; Carneiro, P.; Costa, N.; Faria, C.; Sousa, N.; Rocha, A.; Arezes, P. Lean Manufacturing and Ergonomics Integration: Defining Productivity and Wellbeing Indicators in a Human—Robot Workstation. Sustainability 2021, 13, 1931. [Google Scholar] [CrossRef]
- Humadi, A.; Nazarahari, M.; Ahmad, R.; Rouhani, H. In-Field Instrumented Ergonomic Risk Assessment: Inertial Measurement Units versus Kinect V2. Int. J. Ind. Ergon. 2021, 84, 103147. [Google Scholar] [CrossRef]
- Savino, M.M.; Battini, D.; Riccio, C. Visual Management and Artificial Intelligence Integrated in a New Fuzzy-Based Full Body Postural Assessment. Comput. Ind. Eng. 2017, 111, 596–608. [Google Scholar] [CrossRef]
- Zhang, J.T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent Validation of Xsens MVN Measurement of Lower Limb Joint Angular Kinematics. Physiol. Meas. 2013, 34, N63. [Google Scholar] [CrossRef] [PubMed]
- Cigrovski, V.; Rupčić, T.; Bon, I.; Očić, M.; Krističević, T. How Can Xsens Kinematic Suit Add to Our Understanding of a Slalom Turn: A Case Study in Laboratory and Field Conditions. Kinesiology 2020, 52, 187–195. [Google Scholar] [CrossRef]
- Schepers, M.; Giuberti, M.; Bellusci, G. Xsens MVN: Consistent Tracking of Human Motion Using Inertial Sensing. Xsens Technol. 2018, 1–8. [Google Scholar] [CrossRef]
- Wang, F. Analysis of Human Mechanics Structure in National Tai Chi Movement. Int. J. Adv. Robot. Syst. 2020, 17, 15069. [Google Scholar] [CrossRef]
- Salas, E.A.; Vi, P.; Reider, V.L.; Moore, A.E. Factors Affecting the Risk of Developing Lower Back Musculoskeletal Disorders (MSDs) in Experienced and Inexperienced Rodworkers. Appl. Ergon. 2016, 52, 62–68. [Google Scholar] [CrossRef]
- Maurer-Grubinger, C.; Haenel, J.; Fraeulin, L.; Holzgreve, F.; Wanke, E.M.; Groneberg, D.A.; Ohlendorf, D. The Movement Profile of Habitual Vacuuming as a Cyclic Movement—a Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 8793. [Google Scholar] [CrossRef]
- Callihan, M.L.; Eyer, J.C.; McCoy, C.J.; Dailey, A.M.; Diket, K.M.; Robinson, A.T.; Kaylor, S. Development and Feasibility Testing of a Contextual Patient Movement Intervention. J. Emerg. Nurs. 2021, 47, 101–112.e1. [Google Scholar] [CrossRef]
- Iranzo, S.; Piedrabuena, A.; Iordanov, D.; Martinez-Iranzo, U.; Belda-Lois, J.M. Ergonomics Assessment of Passive Upper-Limb Exoskeletons in an Automotive Assembly Plant. Appl. Ergon. 2020, 87, 103120. [Google Scholar] [CrossRef] [PubMed]
- Merino, G.; da Silva, L.; Mattos, D.; Guimarães, B.; Merino, E. Ergonomic Evaluation of the Musculoskeletal Risks in a Banana Harvesting Activity through Qualitative and Quantitative Measures, with Emphasis on Motion Capture (Xsens) and EMG. Int. J. Ind. Ergon. 2019, 69, 80–89. [Google Scholar] [CrossRef]
- Kim, W.; Peternel, L.; Lorenzini, M.; Babič, J.; Ajoudani, A. A Human-Robot Collaboration Framework for Improving Ergonomics During Dexterous Operation of Power Tools. Robot. Comput. Integr. Manuf. 2021, 68, 102084. [Google Scholar] [CrossRef]
- Xsens Technologies, B.V. Xsens MVN RULA Report: The Use of Inertial Motion Capture for Cloud Based Reporting of RULA Parameters; Xsens Technologies B.V.: Enschede, The Netherlands, 2021. [Google Scholar]
- Colim, A.; Faria, C.; Sousa, N.; Rocha, A. Physical Ergonomic Improvement and Safe Design of an Assembly Workstation through Collaborative Robotics. Safety 2021, 7, 14. [Google Scholar] [CrossRef]
- Colim, A.; Faria, C.; Braga, A.C.; Sousa, N.; Rocha, L.; Carneiro, P.; Costa, N.; Arezes, P. Towards an Ergonomic Assessment Framework for Industrial Assembly Workstations—A Case Study. Appl. Sci. 2020, 10, 3048. [Google Scholar] [CrossRef]
- Longo, A.; Haid, T.; Meulenbroek, R.; Federolf, P. Biomechanics in Posture Space: Properties and Relevance of Principal Accelerations for Characterizing Movement Control. J. Biomech. 2019, 82, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Roetenberg, D.; Luinge, H.; Slycke, P. Xsens MVN: Full 6DOF Human Motion Tracking Using Miniature Inertial Sensors; Xsens Motion Technol. BV: Enschede, The Netherlands, 2009; pp. 1–7. [Google Scholar]
- Corbeil, P.; Plamondon, A.; Handrigan, G.; Vallée-Marcotte, J.; Laurendeau, S.; Ten Have, J.; Manzerolle, N. Biomechanical Analysis of Manual Material Handling Movement in Healthy Weight and Obese Workers. Appl. Ergon. 2019, 74, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Effect of Local Magnetic Field Disturbances on Inertial Measurement Units Accuracy. Appl. Ergon. 2017, 63, 123–132. [Google Scholar] [CrossRef]
- Igelmo, V.; Syberfeldt, A.; Högberg, D.; Rivera, F.; Luque, E. Aiding Observational Ergonomic Evaluation Methods Using MOCAP Systems Supported by AI-Based Posture Recognition. Adv. Transdiscipl. Eng. 2020, 11, 419–429. [Google Scholar] [CrossRef]
- Silva, V.; Fonseca, P.; Pinho, M.E.; Góis, J.; Vaz, M.; Reis-Campos, J. Biomechanical Study of Dentists’ Posture When Using a Conventional Chair versus a Saddle-Seat Chair. Rev. Port. Estomatol. Med. Dent. Cir. Maxilofac. 2017, 58, 39–45. [Google Scholar] [CrossRef][Green Version]
- Ertem, K.; Harma, A.; Cetin, A.; Elmali, N.; Yologlu, S.; Bostan, H.; Sakarya, B. An Investigation of Hand Dominance, Average versus Maximum Grip Strength, Body Mass Index and Ages as Determinants for Hand Evaluation. Isokinet. Exerc. Sci. 2005, 13, 223–227. [Google Scholar] [CrossRef]
- Gil Coury, H.J.C.; Kumar, S.; Rodgher, S.; Narayan, Y. Measurements of Shoulder Adduction Strength in Different Postures. Int. J. Ind. Ergon. 1998, 22, 195–206. [Google Scholar] [CrossRef]
- Grzywiński, W.; Wandycz, A.; Tomczak, A.; Jelonek, T. The Prevalence of Self-Reported Musculoskeletal Symptoms among Loggers in Poland. Int. J. Ind. Ergon. 2014, 52, 12–17. [Google Scholar] [CrossRef]
- Cherubini, A.; Passama, R.; Crosnier, A.; Lasnier, A.; Fraisse, P. Collaborative Manufacturing with Physical Human-Robot Interaction. Robot. Comput. Integr. Manuf. 2016, 40. [Google Scholar] [CrossRef]
- Maurice, P.; Padois, V.; Measson, Y.; Bidaud, P. Human-Oriented Design of Collaborative Robots. Int. J. Ind. Ergon. 2017, 57, 88–102. [Google Scholar] [CrossRef]
- Gualtieri, L.; Palomba, I.; Merati, F.A.; Rauch, E.; Vidoni, R. Design of Human-Centered Collaborative Assembly Workstations for the Improvement of Operators’ Physical Ergonomics and Production Efficiency: A Case Study. Sustainability 2020, 12, 3606. [Google Scholar] [CrossRef]
- Haque, S.; Khan, A.A. Effects of Ulnar Deviation of the Wrist Combined with Flexion/Extension on the Maximum Voluntary Contraction of Grip. J. Hum. Ergol. 2009, 38, 1–9. [Google Scholar] [CrossRef]
- Garg, A.; Moore, J.; Kapellusch, J. The Revised Strain Index: An Improved Upper Extremity Exposure Assessment Model. Ergonomics 2017, 60, 912–922. [Google Scholar] [CrossRef]
- Kee, D.; Karwowski, W. LUBA: An Assessment Technique for Postural Loading on the Upper Body Based on Joint Motion Discomfort and Maximum Holding Time. Appl. Ergon. 2001, 32, 357–366. [Google Scholar] [CrossRef]
- Roman-Liu, D. Repetitive Task Indicator as a Tool for Assessment of Upper Limb Musculoskeletal Load Induced by Repetitive Task. Ergonomics 2007, 50, 1740–1760. [Google Scholar] [CrossRef] [PubMed]
- Rempel, D.M.; Keir, P.J.; Bach, J.M. Effect of Wrist Posture on Carpal Tunnel Pressure While Typing. J. Orthop. Res. 2008, 26, 1269–1273. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Arellano, J.L.; Serratos-Perez, J.N.; de la Torre, A.; Maldonado-Macias, A.A.; Garcia-Alcaraz, J.L. Design Proposal of an Adjustable Workstation for Very Short and Very Tall People. Procedia Manuf. 2015, 3, 5699–5706. [Google Scholar] [CrossRef][Green Version]
- Pavlovic-Veselinovic, S.; Hedge, A.; Veselinovic, M. An Ergonomic Expert System for Risk Assessment of Work-Related Musculo-Skeletal Disorders. Int. J. Ind. Ergon. 2016, 53, 130–139. [Google Scholar] [CrossRef]
- Manghisi, V.M.; Uva, A.E.; Fiorentino, M.; Bevilacqua, V.; Trotta, G.F.; Monno, G. Real Time RULA Assessment Using Kinect v2 Sensor. Appl. Ergon. 2017, 65, 481–491. [Google Scholar] [CrossRef]
- Health and Safety (HSE). Assessment of Repetitive Tasks of the Upper Limbs (the ART Tool ); HSE: London, UK, 2010. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Personal Data | W1 | W2 |
|---|---|---|
| Age (years) | 46 | 36 |
| Stature (cm) | 155 | 170 |
| Dominant hand | Right | Right |
| WMSD diagnosed | Carpal tunnel syndrome | Lumbar disc herniation |
| RULA Score | WMSD Risk Level | Action Level | Meaning |
|---|---|---|---|
| 1 or 2 | Negligible | 1 | The posture is acceptable if it is not maintained or repeated for long periods. |
| 3 or 4 | Low risk | 2 | Further investigation is needed and changes may be required. |
| 5 or 6 | Medium risk | 3 | Investigation and changes are required soon. |
| 7 | Very high risk | 4 | Investigation and changes are required immediately. |
| Before | After | |
|---|---|---|
| W1 | 30%Low risk 63%Medium risk 7%High risk | 1%Negligible 52%Low risk 42%Medium risk 5%High risk |
| W2 | 100% Medium risk | 3%Negligible 93%Low risk 4% Medium risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colim, A.; Cardoso, A.; Arezes, P.; Braga, A.C.; Peixoto, A.C.; Peixoto, V.; Wolbert, F.; Carneiro, P.; Costa, N.; Sousa, N. Digitalization of Musculoskeletal Risk Assessment in a Robotic-Assisted Assembly Workstation. Safety 2021, 7, 74. https://doi.org/10.3390/safety7040074
Colim A, Cardoso A, Arezes P, Braga AC, Peixoto AC, Peixoto V, Wolbert F, Carneiro P, Costa N, Sousa N. Digitalization of Musculoskeletal Risk Assessment in a Robotic-Assisted Assembly Workstation. Safety. 2021; 7(4):74. https://doi.org/10.3390/safety7040074
Chicago/Turabian StyleColim, Ana, André Cardoso, Pedro Arezes, Ana Cristina Braga, Ana Carolina Peixoto, Vítor Peixoto, Felix Wolbert, Paula Carneiro, Nélson Costa, and Nuno Sousa. 2021. "Digitalization of Musculoskeletal Risk Assessment in a Robotic-Assisted Assembly Workstation" Safety 7, no. 4: 74. https://doi.org/10.3390/safety7040074
APA StyleColim, A., Cardoso, A., Arezes, P., Braga, A. C., Peixoto, A. C., Peixoto, V., Wolbert, F., Carneiro, P., Costa, N., & Sousa, N. (2021). Digitalization of Musculoskeletal Risk Assessment in a Robotic-Assisted Assembly Workstation. Safety, 7(4), 74. https://doi.org/10.3390/safety7040074