1. Introduction
Work in the construction industry is highly labor-intensive and physically demanding, often involving heavy manual material handling and awkward postures. The construction sector is India’s second-largest industry after agriculture, employing a vast unorganized workforce [
1]. It is estimated that approximately 340 million workers (about 72% of India’s workforce) are in the unorganized sector, with nearly half of them engaged in construction activities [
2]. Construction projects encompass numerous hazardous operations, such as carrying heavy loads, working at heights, repetitive manual tasks, and prolonged stooping or kneeling [
1]. As a result, construction workers experience a high burden of work-related musculoskeletal disorders (WMSDs) and injuries, often exceeding that of other occupational groups [
3]. Globally, musculoskeletal disorders are among the leading causes of work-related illness, accounting for about one-third of occupational illnesses overall and up to 77% in construction workers [
4]. In India, community-based studies have estimated that the overall prevalence of musculoskeletal disorders (MSDs) in the general population is around 20% [
5]. In contrast, a study conducted among construction workers in Chennai found that 84% of them suffer from work-related musculoskeletal disorders [
2].
Despite the evident risks, there is a scarcity of detailed epidemiological data on ergonomic hazards and WMSDs among construction workers in India. A few studies have highlighted this issue: for instance, a cross-sectional study in South India reported that 33.8% of construction workers had musculoskeletal morbidity in at least one body part [
2]. However, that study relied on self-reported complaints without an in-depth ergonomic assessment of work tasks. Given the diversity of tasks (masonry, material transport, carpentry, etc.) and the largely unorganized nature of the construction workforce, there is a need for comprehensive research combining symptom surveys with quantitative ergonomic evaluation tools. The identification of specific work-related risk factors (e.g., heavy lifting, repetitive motions, awkward postures) is crucial for developing targeted interventions.
The present study was designed to fill this gap by assessing both the prevalence of WMSDs and the nature of work-related ergonomic hazards among construction workers in India by using validated tools. We used the Nordic Musculoskeletal Questionnaire (NMQ) to capture self-reported musculoskeletal symptoms across body regions [
6,
7,
8] and the Rapid Entire Body Assessment (REBA) tool to evaluate the postural risks associated with construction tasks [
9]. By integrating these approaches, this cross-sectional study aims to quantify the prevalence of WMSDs among construction workers in India and examine the nature of ergonomic risk factors associated with these disorders. We utilized the Rapid Entire Body Assessment (REBA) to evaluate postural risks during typical construction tasks, and we investigated personal and work-related factors (age, experience, job type, work hours) for their association with WMSDs. We hypothesize that WMSDs are highly prevalent in this population and are significantly associated with high REBA risk scores and other work exposure variables. The findings will help in understanding the ergonomic hazards in construction and inform targeted interventions to reduce musculoskeletal injuries in this sector.
2. Materials and Methods
2.1. Study Design and Setting
This study was based on a cross-sectional design and adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for transparent and standardized reporting of observational studies. The participants were recruited using stratified random sampling from active construction projects in a major city in India. Construction sites were first stratified based on criteria, such as project size and type of construction activity. Within each stratum, workers were randomly selected to ensure representation across the different work settings. The selected sites were typical of the regional construction industry, where work was manual-intensive with minimal mechanization.
2.2. Participants
A total of 250 participants were included in this study. The participants were evaluated for demographic assessment, the Nordic Musculoskeletal Questionnaire (NMQ), and the Rapid Entire Body Assessment (REBA). The study was completed within six months, from August 2024 to March 2025. Convenience sampling was used to recruit the participants. The inclusion criteria for the study were as follows: both male and female construction workers aged between 25 and 55 years with at least 3 years of work experience and a minimum of 8 h per day, 6 days a week. Subjects were excluded if they had any chronic disease or accidents that affected the musculoskeletal system.
Notably, certain personal factors, such as Body Mass Index (BMI), smoking status, physical fitness levels, and psychosocial stressors (e.g., deadline pressure), were not assessed due to field-based logistical constraints. These are acknowledged as limitations and recommended for inclusion in future studies.
2.3. Sample Size
The sample size was determined using the formula, where n = sample size, p = 50% (assuming maximum variability), with a power (1-β) set at 0.80 and an alpha level (α) of 0.05, corresponding to a 95% confidence interval, so Z score = 1.96, margin of error(d) = 10%, and non-response = 10%. The analysis aimed to achieve a minimum acceptable intraclass correlation coefficient (ICC) of 0.60. The outcome of the sample size determination indicated that a minimum of 220 participants were necessary to detect a statistically significant difference within the study parameters. To enhance our study′s robustness and mitigate the potential for type II errors, we elected to include 250 participants.
2.4. Ethical Considerations
This study was approved by the Institutional Review Board (IRB) (IEC/IIMSR/2024/86) and adhered to standard ethical procedures for research on human subjects. The study was registered under the Clinical Trial Registry India (CTRI) with the registration number CTRI/2024/11/047689. Informed consent was obtained from all participants after a thorough explanation of the study objectives, procedures, and potential risks. This study adhered to the ethical standards prescribed in the 1964 Declaration of Helsinki.
2.5. Outcome Measures
The participants were evaluated for demographic and work assessment, the Nordic Musculoskeletal Questionnaire (NMQ), and the Rapid Entire Body Assessment (REBA).
Demographic and work information:
Age, sex, years of construction work experience, typical daily work hours, and job role were collected using a structured questionnaire.
Nordic Musculoskeletal Questionnaire (NMQ):
We used the Standardized Nordic Musculoskeletal Questionnaire to assess self-reported musculoskeletal symptoms [
10]. This validated questionnaire documents the occurrence of musculoskeletal pain or discomfort in nine body regions (neck, shoulders, elbows, wrists/hands, upper back, lower back, hips/thighs, knees, and ankles/feet) over specified time frames [
11]. Each participant was asked if they had experienced musculoskeletal pain or ache in each body region in the last 12 months and in the last 7 days. Additional questions probed whether the pain in the last year prevented normal work or required medical treatment. The NMQ is a widely used tool for surveillance of WMSDs and has demonstrated reliability in various worker populations [
12]. For the purposes of this study, a positive response for a body region was defined as the presence of pain or discomfort in that region at least for one day in the past 12 months, and these were further detailed by 7-day period prevalence.
Rapid Entire Body Assessment (REBA):
An ergonomic risk assessment for each participant’s primary work activity was conducted using the REBA tool via the TuMeke (2.7.15) mobile application [
13,
14]. REBA is a systematic observational method used to evaluate working postures involving the neck, trunk, legs, arms, wrists, and load handling, ultimately generating a risk score that is indicative of musculoskeletal strain [
15]. Tasks were recorded under normal working conditions using a smartphone video from multiple angles and uploaded to TuMeke, which uses automated computer vision to analyze postures and calculate the REBA scores.
The tasks were recorded under normal working conditions using a smartphone video from multiple angles and then uploaded to TuMeke. This application employs automated computer vision to analyze postures and calculate the REBA scores. In prior studies, the TuMeke application has shown good validity and reliability in posture recognition and REBA scoring compared to traditional manual methods [
16]. Its computer vision algorithms are trained on diverse movement datasets, allowing consistent assessments across a variety of construction tasks.
The REBA scoring was performed by a single trained investigator to maintain consistency. To enhance reliability, standardized video recordings and photographs were used to evaluate posture. The TuMeke application provided automated REBA scoring based on validated computer vision algorithms, which have been shown to offer acceptable reliability in field settings [
16].
The investigator observed each participant during typical work tasks, including brick/block carrying (on the head or shoulder), mortar mixing, shoveling, bricklaying, bar bending, and overhead plastering. The worst posture observed during each task cycle was selected for REBA scoring based on variables such as joint angles, load handling, grip type, and activity frequency. Additionally, photographs (with informed consent) were taken to support postural analysis, and no personal identifiers were recorded.
The REBA scores range from 1 to 15, with higher scores reflecting greater ergonomic risk [
16]. For interpretation, we followed standard REBA action levels. Low risk (1–3): negligible or low risk; change may be needed. Medium risk (4–7): further investigation advised; changes should be considered. High risk (8–10): prompt investigation and changes required. Very high risk (≥11): immediate ergonomic intervention needed [
17].
2.6. Data Collection Procedure
On each site visit, the investigators first explained the study objectives and procedures to the workers in the local language. After obtaining informed consent, demographic and work information (age, sex, years of construction work experience, typical daily work hours, and job role/trade) were collected using a structured questionnaire. The investigator also inquired about any prior ergonomic training or use of assistive devices (though none had formal training). We used an NMQ to record the presence of musculoskeletal pain or discomfort in nine body regions (neck, shoulders, elbows, wrists/hands, upper back, lower back, hips/thighs, knees, ankles/feet) over the past 12 months. Participants indicated whether they had experienced work-related pain in each region. For analysis, a participant was considered to have a WMSD if they reported pain in one or more body parts. We also recorded the total number of body parts affected for each worker as an indicator of the extent of musculoskeletal morbidity. REBA was used for ergonomic risk assessment. Key tasks (such as bricklaying for masons, load carrying for laborers, pipe fitting for plumbers, painting at height for painters, etc.) were assessed. REBA scoring followed the standard methodology, yielding a REBA score for each worker’s predominant task posture. This score was categorized into REBA risk levels: low risk (score ≤ 3), medium risk (4–7), high risk (8–10), and very high risk (≥11), corresponding to increasing urgency of ergonomic intervention. For each participant, the highest REBA score observed among their tasks was recorded as representative of their ergonomic risk.
2.7. Statistical Analysis
The data were analyzed using IBM SPSS Statistics (Version 25). Descriptive statistics were used to summarize the sample characteristics, with continuous variables presented as mean ± standard deviation (SD) and categorical variables as frequency and percentage. WMSD prevalence by body region and job category is tabulated. Chi-square tests were used to examine associations between risk factors (age group, work experience, daily work hours, job type, and REBA risk category) and WMSD presence, with significance at p < 0.05. Factors with low cell counts were combined or analyzed using Fisher’s exact test. Multivariate logistic regression identified independent WMSD predictors using risk factors that showed significance in the univariate analysis. The binary outcome was the presence of WMSD (yes = 1, no = 0), with adjusted odds ratios (ORs), 95% CIs, and p-values reported.
3. Results
The demographic characteristics of the participants are presented in
Table 1. The sample consisted predominantly of males and encompassed a diverse array of construction occupations, with masons and general laborers representing the largest subgroup. The mean age of the participants was in the mid-thirties, indicative of a relatively young and active workforce. The majority of participants had less than 10 years of experience in construction, and nearly one-third reported working more than eight hours per day.
Figure 1 and
Table 2 present the prevalence of musculoskeletal pain categorized according to body region and occupational type. Overall, 48% of the workers reported experiencing lower back pain, which was the most affected region, followed by knee pain (45%) and shoulder pain (40%). Within specific trades, 60% of the laborers and 55% of the masons reported lower back pain, suggesting a significant correlation with tasks involving heavy manual handling. Neck pain was most prevalent among electricians (60%) and painters (50%) and was likely attributable to prolonged overhead work. Carpenters demonstrated the highest prevalence of wrist and hand pain at 40%, which aligns with the precision and repetitive nature of tool use in their work.
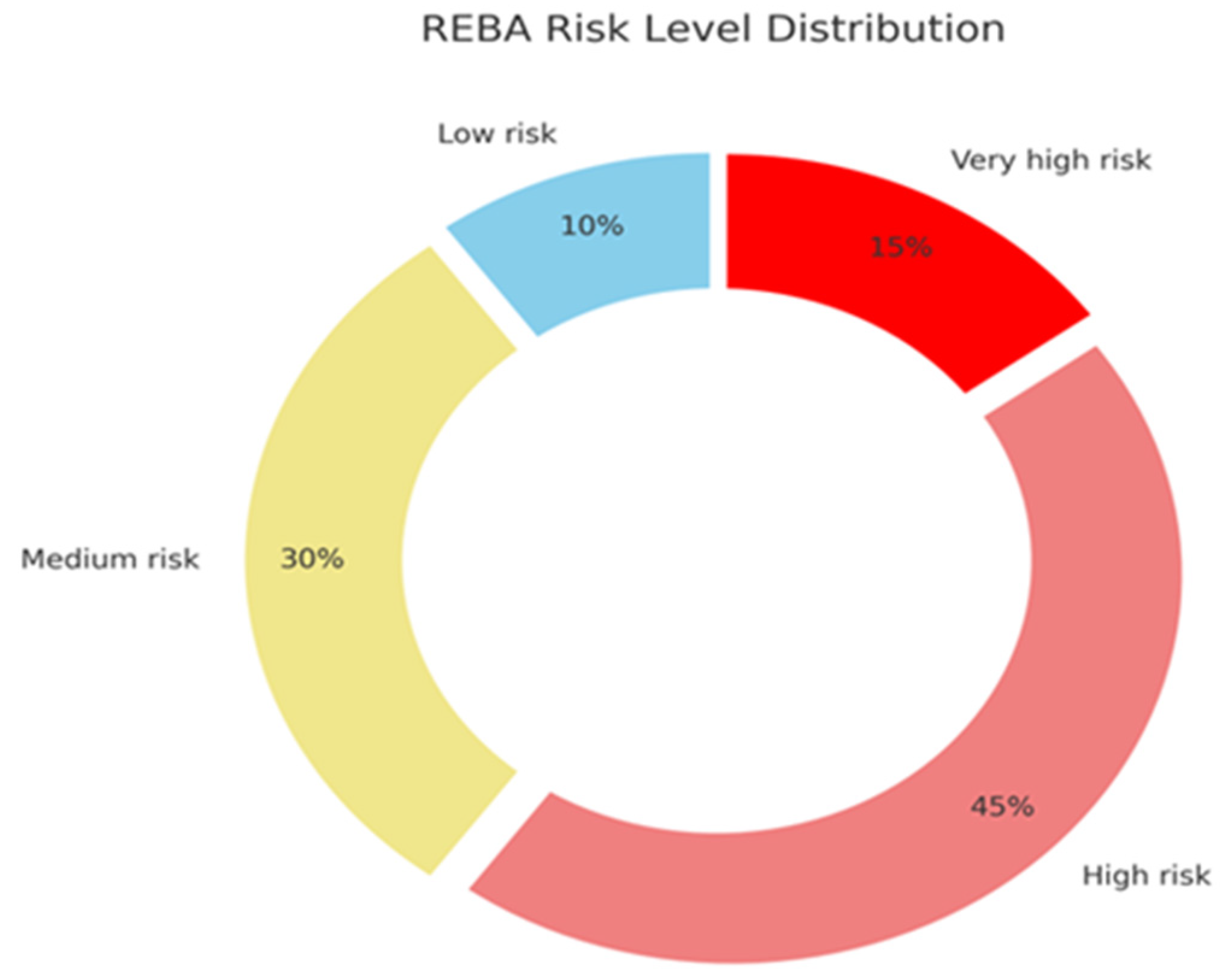
Figure 2 and
Table 3 present the distribution of the REBA risk categories among construction workers. A significant proportion of participants were classified into high- and very high-risk categories, collectively comprising over 60% of the sample. This indicates that the majority of tasks involved postures assessed as high or extreme risk, requiring urgent or immediate ergonomic intervention. The REBA scoring system evaluates individual body regions and task components to determine the overall risk level, with higher scores indicating more biomechanically demanding or unsafe postures. These scores reflect cumulative ergonomic strain rather than a single momentary posture. In contrast, only a small percentage (10%) of workers were identified in the low-risk category, highlighting the prevalent exposure to ergonomic hazards within this occupational group.
Table 4 illustrates the association between the selected risk factors and the incidence of work-related musculoskeletal disorders (WMSDs), as determined by chi-square analysis. Significant associations were observed for age (
p = 0.005), work experience (
p = 0.010), work hours per day (
p = 0.040), job type (
p = 0.020), and REBA risk category (
p < 0.001). These results indicate that older workers, those with more work experience, longer work hours, and those in manual labor roles were more likely to report WMSDs. Notably, ergonomic risk level (REBA score) exhibited the strongest association, with 80% of WMSD prevalence in the high/very high-risk group compared to 40% in the low/medium-risk group. This highlights the predictive value of ergonomic risk in WMSD occurrence. Sex was not significantly associated with WMSDs (
p = 0.200).
As shown in
Table 5, multivariate logistic regression confirmed that high/very high REBA scores (adjusted OR = 4.5, 95% CI: 1.8–11.2,
p = 0.001) and age > 40 years (OR = 3.5, 95% CI: 1.2–10.2,
p = 0.02) were the strongest independent predictors of WMSDs. Longer work hours (>8 per day) showed a borderline significant association (OR = 1.9, 95% CI: 1.0–3.6,
p = 0.05), while job type was not statistically significant (
p = 0.30). All odds ratios are reported with their 95% confidence intervals to support interpretation of the model estimates. Although a sensitivity analysis was not performed due to sample size limitations, we acknowledge this as a limitation and recommend it for future research to validate model robustness. These findings emphasize that ergonomic exposure and age are key drivers of WMSDs in this population.
4. Discussion
This cross-sectional study examined the prevalence and factors associated with work-related musculoskeletal disorders (WMSDs) among construction workers in India. The study found that over 60% of the workers reported at least one WMSD in the past year, indicating a significant health burden in this population. The most affected body parts were the lower back, knees, shoulders, and neck, consistent with the physical demands and repetitive movements in construction work.
A key finding of this study was the association between poor ergonomic posture and WMSDs. Using the Rapid Entire Body Assessment (REBA) tool, this study showed that workers exposed to high-risk postures had significantly higher odds of experiencing musculoskeletal pain. Workers with higher REBA scores often reported pain in multiple body regions, suggesting a cumulative effect of the ergonomic strain. The presence of WMSDs was not merely associated with job title (e.g., laborers vs. skilled trades), but with the physical nature of the tasks performed. This underscores that the biomechanical demands of work, not occupational labels, are key determinants of musculoskeletal risk.
The prevalence of WMSDs (60.4%) reported in this study aligns with recent literature on construction workers in India. A systematic review estimated a pooled 12-month WMSD prevalence of 76% among Indian occupational groups, with common pain sites including the lower back (~60%), neck (~40%), and shoulders (~36%) [
18,
19]. In this study, LBP, neck pain, and shoulder pain prevalence were 48%, 30%, and 40%, respectively. These results align with the broader epidemiological trends, suggesting that the construction sector remains vulnerable. The lower back pain rate compared to the pooled estimates may reflect variations in worker demographics or job activities. The high prevalence of knee disorders (45%) in our sample is noteworthy and slightly exceeds the rates reported in previous studies. Previous studies documented knee pain prevalence between 34% and 37% among Indian construction workers [
20,
21]. Similar findings have been observed internationally, such as in a study by Boakey et al. in the UK [
22]. Comparable patterns have also been reported in other low- and middle-income countries—for instance, a Bangladeshi study among manual construction workers highlighted similar musculoskeletal risks, particularly affecting the lower back and knees, while a community-based study in Nepal observed a one-year low back pain prevalence of 52%, with knee strain also noted among labor-intensive occupations. These findings underscore the consistency of ergonomic risk exposure across construction sectors globally [
23,
24]. These variations may stem from differences in the populations studied, data collection methods, and knee pain definitions. Future research should aim to standardize these factors to enable more accurate comparisons across different regions and demographic groups. The elevated prevalence of knee pain may reflect the nature of specific tasks commonly performed by the workers in our sample, particularly masons, plumbers, and floor workers, who often engage in squatting, kneeling, and working on uneven surfaces without adequate protective aids. This may also indicate gaps in ergonomic adaptation or work rotation practices in the local construction industry. The WMSD distribution across trades shows how specific tasks correspond to different musculoskeletal strains. Painters and electricians, who frequently perform overhead work, have higher rates of neck and shoulder pain, whereas laborers and masons, engaged in heavy lifting and bending, report lower back problems. These findings align with ergonomic literature which indicates that elevated arms and extended neck positions increase neck and shoulder disorder risks, while frequent stooping and lifting of heavy loads contribute to low back pain [
25].
The REBA scores confirmed the ergonomic nature of the construction. Most workers fell into the medium- or high-risk category. The study demonstrated a correlation between REBA risk levels and WMSD prevalence, suggesting a dose–response relationship. Higher REBA scores were associated with more musculoskeletal complaints, thus supporting the predictive validity of the tool. These findings align with those of Zare et al., who reported significant correlations between REBA scores and musculoskeletal symptoms in various body regions [
26,
27]. Among personal risk factors, older age and longer work experience were significantly associated with higher WMSD prevalence. Workers over 40 had 3.5 times higher odds of reporting WMSDs than younger workers. Those with five or more years of work experience had a higher prevalence of WMSDs. These results support the hypothesis of cumulative biomechanical wear, which suggests that prolonged physical strain leads to increased musculoskeletal complaints. Similar findings were reported by Reddy et al., who showed that individuals with over 11 years of construction experience had 2.8 times higher risk of WMSDs than those with shorter tenures [
2,
27].
This study did not observe a protective effect of older age, unlike findings from Chennai, where workers over 40 years of age reported lower WMSD prevalence (10%) compared to younger groups (33–60%). The Chennai study attributed this to the “healthy worker effect,” where older workers remaining employed are in less demanding roles or represent hardier individuals who withstood physical rigors [
2]. However, in this study, older workers still performed physically demanding tasks because of economic necessity and informal labor markets. Thus, age was associated with accumulated injury risk rather than resilience, emphasizing the need for ergonomic support for older workers.
The influence of job type and work hours was also explored. While bivariate analysis showed a higher WMSD prevalence among laborers and masons, these differences were not significant in multivariate analysis after adjusting for REBA scores. This finding suggests that job title is not an independent risk factor when ergonomic exposure is considered. Reddy et al. found that laborers had 4.4 times higher odds of developing WMSDs than other occupations [
2], but their analysis did not control for ergonomic risk using REBA. The findings emphasize that the ergonomic nature of work—posture, force, and repetition—matters more than occupational label. This insight is critical for workplace interventions as it highlights the need to target high-risk tasks across job types. Work hours remained a borderline significant factor in WMSD prevalence after adjusting for ergonomic risk. Workers exceeding eight hours per day showed higher rates of musculoskeletal complaints, indicating that prolonged physical strain increases the risk of injury. This suggests that limiting work hours or ensuring adequate breaks could help reduce WMSDs. In contrast, Reddy’s study found no significant differences related to work hours, possibly due to the homogeneity of work duration in their sample [
2]. The current study’s greater variability in daily work hours (with approximately 30% working overtime) likely allowed for the detection of this association.
To address these findings, we recommend specific ergonomic interventions, such as mechanical lifting devices, anti-fatigue flooring, adjustable scaffolding to prevent prolonged overhead work, and ergonomic tool designs, such as angled handles for masons and electricians. These targeted measures are supported by systematic reviews that confirm the effectiveness of task-specific interventions in reducing the WMSD risk across construction trades [
28,
29,
30].
This study highlights the burden of WMSDs among Indian construction workers and underscores the ergonomic risk factors. The REBA tool validated the link between posture and musculoskeletal pain, thereby offering a framework for identifying high-risk workers. These findings support a shift to preventive ergonomic strategies, including introducing mechanical lifting aids (e.g., trolleys, hoists), redesigning hand tools to reduce wrist strain (e.g., angled handles, cushioned grips), implementing task rotation systems to limit repetitive strain, providing knee pads and anti-fatigue mats, and delivering targeted ergonomic training sessions focused on safe lifting and posture techniques. Policymakers should also consider regulating working hours to prevent overuse.
Moreover, the low proportion of female participants (8%) limits the generalizability of our findings to female construction workers whose physiological and task-related ergonomic risks may differ. Additionally, personal characteristics such as Body Mass Index (BMI), smoking status, physical fitness levels, and psychosocial stressors (e.g., deadline pressure) were not assessed due to logistical constraints. Their exclusion may have influenced observed associations and should be incorporated in future longitudinal studies for a more comprehensive risk profile.
In future research, integrating emerging technologies such as deep learning and hybrid AI models could significantly enhance ergonomic risk assessments. For example, combining natural language processing (NLP) with sensor data has been effectively utilized in the mining and quarry sectors to automate task classification and predict injury risk. Tools such as the NLP-based risk assessment system developed for marble quarries illustrate how these technologies can be adapted to high-risk construction environments. By incorporating these tools, it may become possible to achieve real-time monitoring, automated posture analysis, and personalized interventions, moving beyond traditional observational scoring methods, such as REBA.
The study strengths include comprehensive methodology, diverse participant samples, and robust statistical analysis linking ergonomic assessments to health outcomes. Limitations include the cross-sectional design, self-reported data, underrepresentation of female workers, and lack of psychosocial and fitness variables. In addition, potential confounders such as Body Mass Index (BMI) and smoking status were not collected or controlled for in the analysis, which may influence the observed associations with WMSDs. Future research should use longitudinal designs, including diverse populations, and test interventions, such as wearable exoskeletons or task redesigns. Integrating machine learning algorithms, motion tracking systems, or biomechanical sensors could further enhance ergonomic evaluation and injury prevention strategies.





{kind=link}
{kind=link}