
Upper-Limb and Low-Back Load Analysis in Workers Performing an Actual Industrial Use-Case with and without a Dual-Arm Collaborative Robot

 , ,
, ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
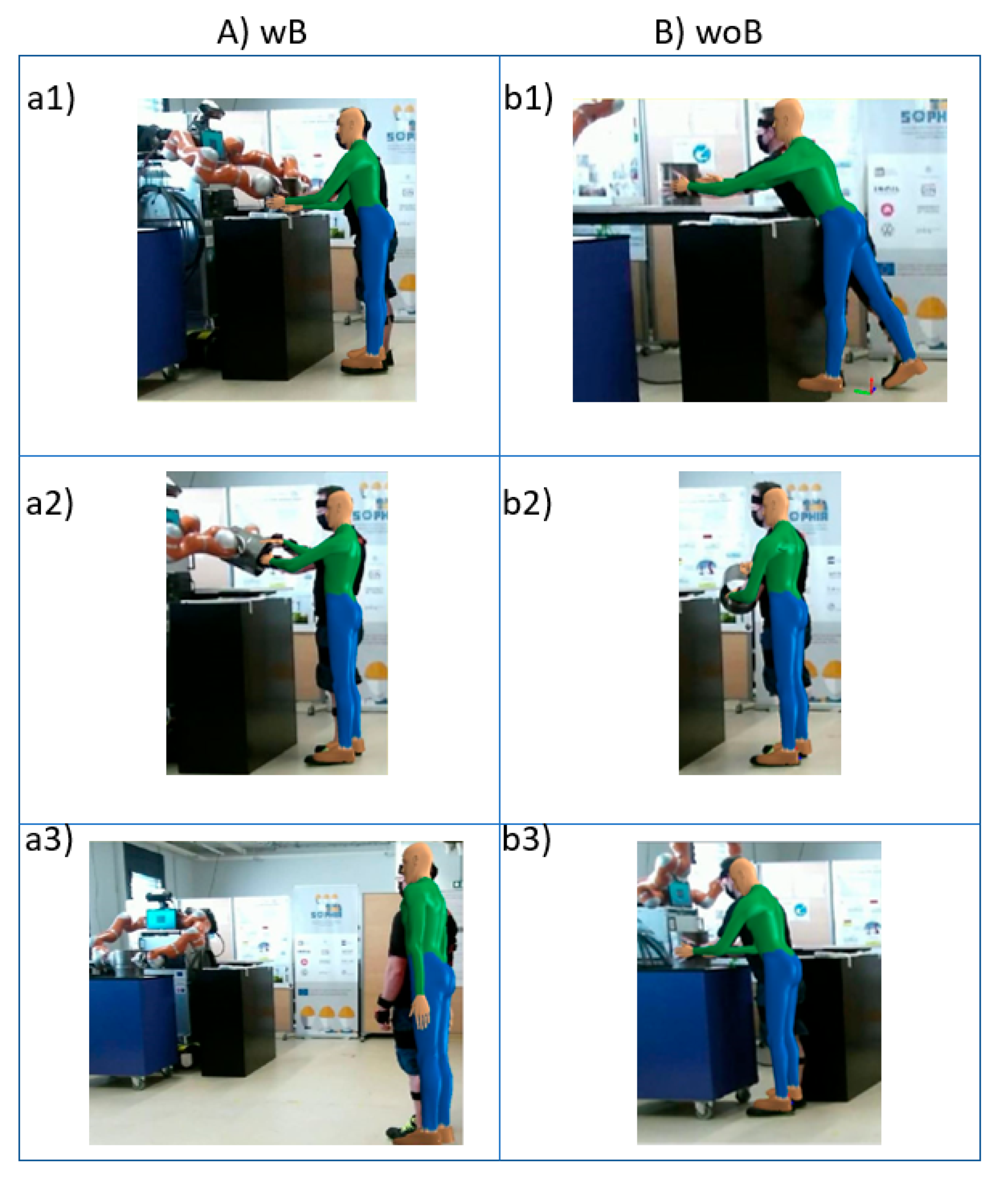
2.2. Task Analysis
2.3. 3D Static Strength Prediction Program (3DSSPP) v 7.1.3
2.3.1. Percentage of Maximum Voluntary Contraction (%MVC)
- Wrist flexion/extension (wrist flex/ext), ulnar/radial deviation (wrist uln/rad), and rotation (wrist rot);
- Elbow flexion/extension (elbow flex/ext);
- Shoulder humeral rotation (shoulder hum rot), backward/forward rotation (shoulder bk/fw), and abduction/adduction (shoulder abd/add);
- Neck flexion/extension (neck flex/ext);
- Trunk flexion/extension (trunk flex/ext).
2.3.2. Maximum Allowed Static (Continuous) Exertion Time (MaxST)
- Wrist flexion/extension, ulnar/radial deviation, and rotation;
- Elbow flexion/extension;
- Shoulder humeral rotation, backward/forward rotation, and abduction/adduction;
- Neck flexion/extension;
- Trunk flexion/extension.
2.3.3. Low-Back Spine Compression Forces (L4Ort)
2.3.4. Strength Percent Capable (SPC) Parameter
2.4. Statistical Analysis
3. Results
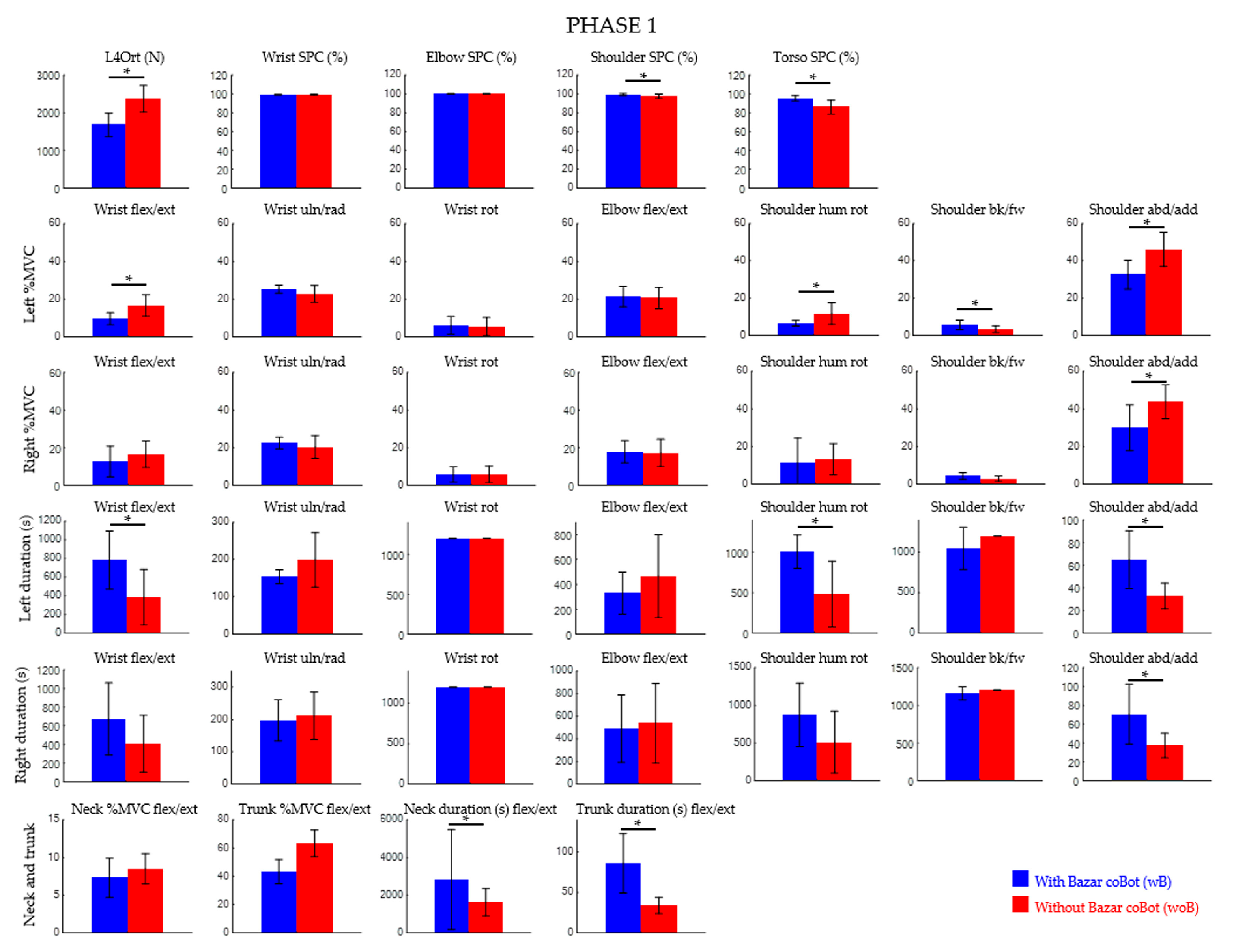
3.1. Phase 1
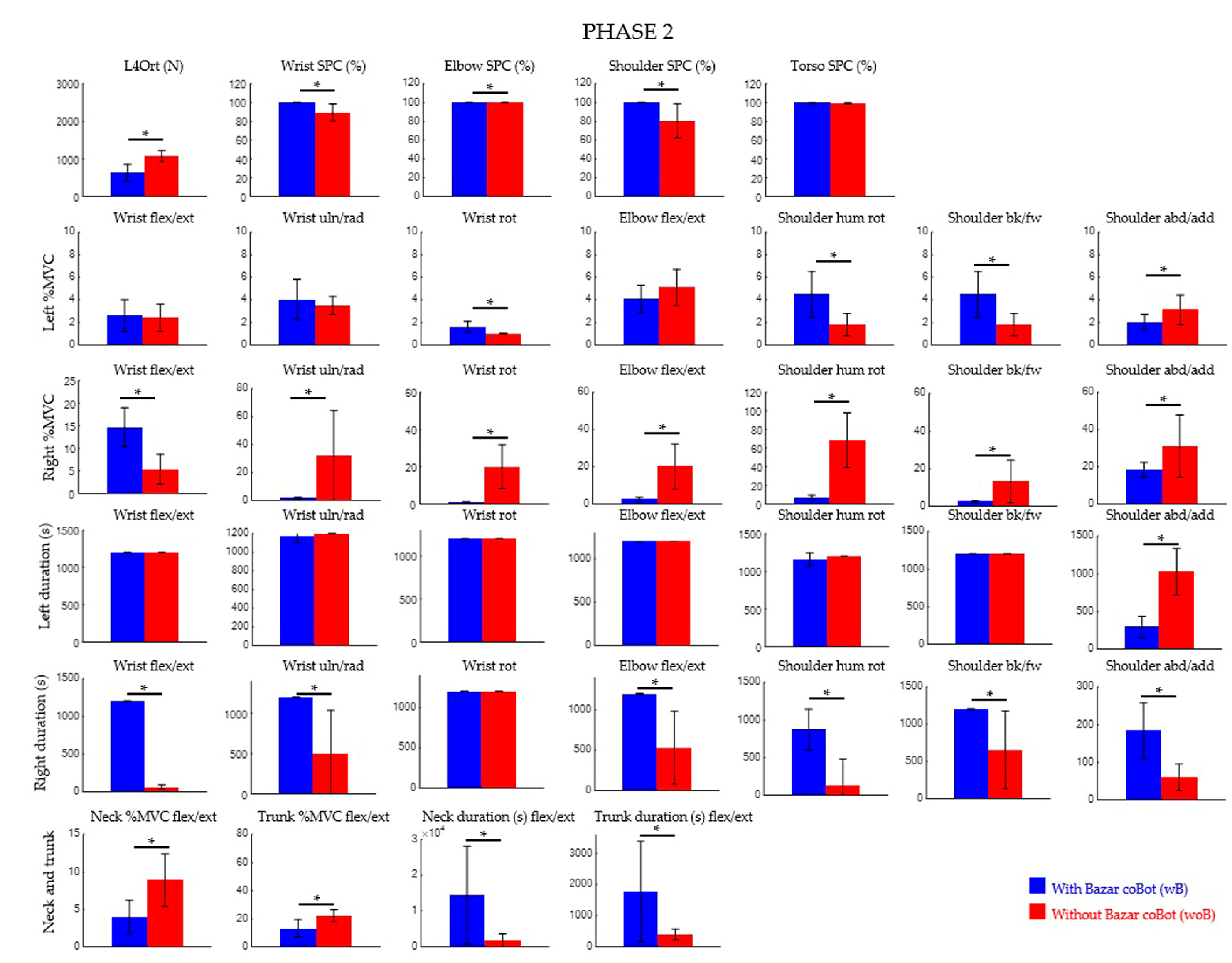
3.2. Phase 2
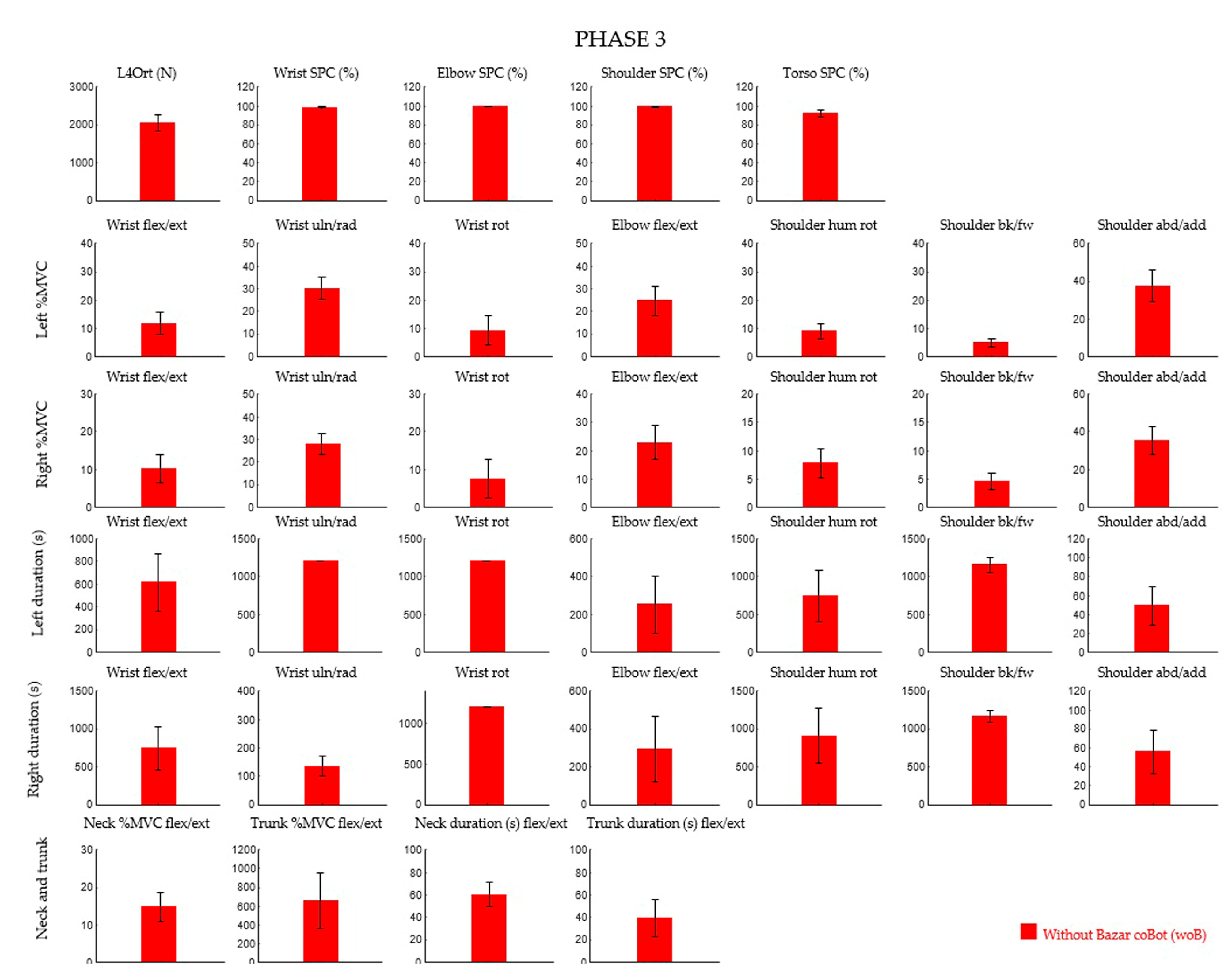
3.3. Phase 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, N.; Fong, D.Y.T.; Wong, J.Y.H. Health and Economic Outcomes Associated with Musculoskeletal Disorders Attributable to High Body Mass Index in 192 Countries and Territories in 2019. JAMA Netw. Open 2023, 6, e2250674. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- National Research Council (US) and Institute of Medicine (US) Panel on Musculoskeletal Disorders and the Workplace. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- National Research Council (US) Steering Committee for the Workshop on Work-Related Musculoskeletal Injuries: The Research Base. Work-Related Musculoskeletal Disorders: Report, Workshop Summary, and Workshop Papers; National Academies Press: Washington, DC, USA, 1999. [Google Scholar] [PubMed]
- Ajoudani, A.; Albrecht, P.; Bianchi, M.; Cherubini, A.; Del Ferraro, S.; Fraisse, P.; Fritzsche, L.; Garabini, M.; Ranavolo, A.; Rosen, P.H.; et al. Smart collaborative systems for enabling flexible and ergonomic work practices [industry activities]. IEEE Robot. Autom. Mag. 2020, 27, 169–176. [Google Scholar] [CrossRef]
- Thoben, K.; Wiesner, S.; Wuest, T. “Industrie 4.0” and smart manufacturing-a review of research issues and application examples. Int. J. Autom. Technol. 2017, 11, 4–16. [Google Scholar] [CrossRef]
- Gualtieri, L.; Rauch, E.; Vidoni, R. Emerging research fields in safety and ergonomics in industrial collaborative robotics: A systematic literature review. Robot. Comput.-Integr. Manuf. 2021, 67, 101998. [Google Scholar] [CrossRef]
- ISO 11228-1:2021; Ergonomics—Manual Handling—Part 1: Lifting, Lowering and Carrying. International Organization for Standardization: Geneva, Switzerland, 2021.
- ISO 11228-2:2007; Ergonomics—Manual Handling—Part 2: Pushing and Pulling. International Organization for Standardization: Geneva, Switzerland, 2007.
- ISO 11228-3:2007; Ergonomics—Manual Handling—Part 3: Handling of Low Loads at High Frequency. International Organization for Standardization: Geneva, Switzerland, 2007.
- Silvetti, A.; Ranavolo, T.; Varrecchia, G.; Chini, A.; Papale, L.; Fiori, A.; Fiorelli, A.; Tatarelli, R.; Trovato, F. Draicchio. Biomechanical overload risk assessment in Industry 4.0. Saf. Health Work. 2022, 13, 147. [Google Scholar] [CrossRef]
- Armstrong, T.J.; Burdorf, A.; Descatha, A.; Farioli, A.; Graf, M.; Horie, S.; Marras, W.S.; Potvin, J.R.; Rempel, D.; Spatari, G.; et al. Scientific basis of ISO standards on biomechanical risk factors. Scand. J. Work Environ. Health 2018, 44, 323–329. [Google Scholar] [CrossRef]
- Armstrong, T.J.; Burdorf, A.; Descatha, A.; Farioli, A.; Graf, M.; Horie, S.; Marras, W.S.; Potvin, J.R.; Rempel, D.; Spatari, G.; et al. Authors’ response: Letter to the Editor concerning OCRA as preferred method in ISO standards on biomechanical risk factors. Scand. J. Work Environ. Health 2018, 44, 439–440. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Muzammil, M. Revised NIOSH lifting equation: A critical evaluation. Int. J. Occup. Saf. Ergon. 2023, 29, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, A.; Colim, A.; Bicho, E.; Braga, A.C.; Menozzi, M.; Arezes, P. Ergonomics and Human Factors as a Requirement to Implement Safer Collaborative Robotic Workstations: A Literature Review. Safety 2021, 7, 71. [Google Scholar] [CrossRef]
- Colim, A.; Faria, C.; Cunha, J.; Oliveira, J.; Sousa, N.; Rocha, L.A. Physical Ergonomic Improvement and Safe Design of an Assembly Workstation through Collaborative Robotics. Safety 2021, 7, 14. [Google Scholar] [CrossRef]
- Ranavolo, A.; Ajoudani, A.; Cherubini, A.; Bianchi, M.; Fritzsche, L.; Iavicoli, S.; Sartori, M.; Silvetti, A.; Vanderborght, B.; Varrecchia, T.; et al. The Sensor-Based Biomechanical Risk Assessment at the Base of the Need for Revising of Standards for Human Ergonomics. Sensors 2020, 20, 5750. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alberto, R.; Draicchio, F.; Varrecchia, T.; Silvetti, A.; Iavicoli, S. Wearable Monitoring Devices for Biomechanical Risk Assessment at Work: Current Status and Future Challenges-A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2001, Erratum in Int. J. Environ. Res. Public Health 2018, 15, 2001. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- CWA 17938:2023; Guideline for Introducing and Implementing Real-Time Instrumental-Based Tools for Biomechanical Risk Assessment. CEN-CENELEC Management Centre: Brussels, Belgium, 2023.
- Chini, G.; Varrecchia, T.; Tatarelli, A.; Silvetti, A.; Fiori, L.; Draicchio, F.; Ranavolo, A. Trunk muscle co-activation and activity in one- and two-person lifting. Int. J. Ind. Ergon. 2022, 89, 103297. [Google Scholar] [CrossRef]
- Varrecchia, T.; Conforto, S.; De Nunzio, A.M.; Draicchio, F.; Falla, D.; Ranavolo, A. Trunk Muscle Coactivation in People with and without Low Back Pain during Fatiguing Frequency-Dependent Lifting Activities. Sensors 2022, 22, 1417. [Google Scholar] [CrossRef] [PubMed]
- Colombini, D. Risk Assessment and Management of Repetitive Movements and Exertions of Upper Limbs: Job Analysis, Ocra Risk Indicies, Prevention Strategies and Design Principles; Elsevier: Amsterdam, The Netherlands, 2002; Volume 2. [Google Scholar]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Varrecchia, T.; Chini, G.; Tarbouriech, S.; Navarro, B.; Cherubini, A.; Draicchio, F.; Ranavolo, A. The assistance of BAZAR robot promotes improved upper limb motor coordination in workers performing an actual use-case manual material handling. Ergonomics 2023, 66, 1950–1967. [Google Scholar] [CrossRef] [PubMed]
- Arjmand, N.; Plamondon, A.; Shirazi-Adl, A.; Larivière, C.; Parnianpour, M. Predictive equations to estimate spinal loads in symmetric lifting tasks. J. Biomech. 2011, 44, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Mientjes, M.I.; Norman, R.W.; Wells, R.P.; McGill, S.M. Assessment of an EMG-based method for continuous estimates of low back compression during asymmetrical occupational tasks. Ergonomics 1999, 42, 868–879. [Google Scholar] [CrossRef] [PubMed]
- Bazrgari, B.; Shirazi-Adl, A.; Arjmand, N. Analysis of squat and stoop dynamic liftings: Muscle forces and internal spinal loads. Eur. Spine J. 2007, 16, 687–699. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, H.K.; Zhang, Y. Estimation of lumbar spinal loading and trunk muscle forces during asymmetric lifting tasks: Application of whole-body musculoskeletal modelling in OpenSim. Ergonomics 2017, 60, 563–576. [Google Scholar] [CrossRef] [PubMed]
- Van Dieën, J.H.; Kingma, I. Total trunk muscle force and spinal compression are lower in asymmetric moments as compared to pure extension moments. J. Biomech. 1999, 32, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Von Arx, M.; Liechti, M.; Connolly, L.; Bangerter, C.; Meier, M.L.; Schmid, S. From Stoop to Squat: A Comprehensive Analysis of Lumbar Loading among Different Lifting Styles. Front. Bioeng. Biotechnol. 2021, 9, 769117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Feola, E.; Refai, M.I.M.; Costanzi, D.; Sartori, M.; Calanca, A. A Neuromechanical Model-Based Strategy to Estimate the Operator’s Payload in Industrial Lifting Tasks. IEEE Trans Neural Syst. Rehabil Eng. 2023, 31, 4644–4652. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, D.G.; Besier, T.F. An EMG-driven musculoskeletal model to estimate muscle forces and knee joint moments in vivo. J. Biomech. 2003, 36, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Moya-Esteban, A.; van der Kooij, H.; Sartori, M. Robust estimation of lumbar joint forces in symmetric and asymmetric lifting tasks via large-scale electromyography-driven musculoskeletal models. J. Biomech. 2022, 144, 111307. [Google Scholar] [CrossRef] [PubMed]
- Moya-Esteban, A.; Durandau, G.; van der Kooij, H.; Sartori, M. Real-time lumbosacral joint loading estimation in exoskeleton-assisted lifting conditions via electromyography-driven musculoskeletal models. J. Biomech. 2023, 157, 111727. [Google Scholar] [CrossRef] [PubMed]
- Sartori, M.; Reggiani, M.; Pagello, E.; Lloyd, D.G. Modeling the human knee for assistive technologies. IEEE Trans. Biomed. Eng. 2012, 59, 2642–2649. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chaffin, D.B.; Andersson, G.B.J.; Martin, B.J. Occupational Biomechanics, 4th ed.; John Wiley & Sons: New York, NY, USA, 2006. [Google Scholar]
- Chaffin, D.B. Biomechanical Modeling for Simulation of 3D Static Human Exertions. In Computer Applications in Ergonomics, Occupational Safety and Health; Elsevier Publishers B.V.: Amsterdam, The Netherlands, 1992. [Google Scholar]
- Tokarski, T.M.; Roman-Liu, D. Assessment of load on the lumbar spine using two computerised packages and REBA method. Acta Bioeng. Biomech. 2020, 22, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Ghezelbash, F.; Shirazi-Adl, A.; Plamondon, A.; Arjmand, N. Comparison of different lifting analysis tools in estimating lower spinal loads-Evaluation of NIOSH criterion. J. Biomech. 2020, 112, 110024. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.J.; Winnemuller, L.; Camp, J.E.; Johnson, P.W. Comparing the results of five lifting analysis tools. Appl. Ergon. 2007, 38, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Rajaee, M.A.; Arjmand, N.; Shirazi-Adl, A.; Plamondon, A.; Schmidt, H. Comparative evaluation of six quantitative lifting tools to estimate spine loads during static activities. Appl. Ergon. 2015, 48, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela-Gómez, S.A.; Rey-Galindo, J.A.; Aceves-Gonzlez, C. Analyzing working conditions for classical guitarists: Design guidelines for new supports and guitar positioning. Work 2020, 65, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Wiggermann, N. Biomechanical Evaluation of a Bed Feature to Assist in Turning and Laterally Repositioning Patients. Hum. Factors 2016, 58, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.; Ghassemieh, E. Risk assessment of patient handling with ambulance stretcher systems (ramp/(winch), easi-loader, tail-lift) using biomechanical failure criteria. Med. Eng. Phys. 2007, 29, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, M.; Monzó, J. Prevalence of low back disorders among female workers and biomechanical limits on the handling of load and patients. Work 2012, 41, 2364–2369. [Google Scholar] [CrossRef] [PubMed]
- Silvetti, A.; Papale, A.; Cipolloni, L.; Vittorio, S.; Draicchio, F. Biomechanical Risk Assessment of Pathologists in the Morgue. In Advances in Social and Occupational Ergonomics, AHFE 2018. Advances in Intelligent Systems and Computing; Goossens, R., Ed.; Springer: Cham, Switzerland, 2019; Volume 792. [Google Scholar] [CrossRef]
- Silvetti, A.; Munafò, E.; Fiorelli, A.; Fiori, L.; Tatarelli, A.; Ranavolo, A.; Draicchio, F. Ergonomic Risk Assessment of Sea Fisherman Part IV: Tunisian Chapter. In Advances in Physical, Social & Occupational Ergonomics, AHFE 2021, Lecture Notes in Networks and Systems; Goonetilleke, R.S., Xiong, S., Kalkis, H., Roja, Z., Karwowski, W., Murata, A., Eds.; Springer: Cham, Switzerland, 2021; Volume 273. [Google Scholar] [CrossRef]
- Silvetti, A.; Fiori, L.; Tatarelli, A.; Ranavolo, A.; Draicchio, F. Back and Shoulder Biomechanical Load in Curbside Waste Workers. In Advances in Physical, Social & Occupational Ergonomics, AHFE 2020, Advances in Intelligent Systems and Computing; Karwowski, W., Goonetilleke, R., Xiong, S., Goossens, R., Murata, A., Eds.; Springer: Cham, Switzerland, 2020; Volume 1215. [Google Scholar] [CrossRef]
- Çakit, E. Ergonomic assessment of airport shuttle driver tasks using an ergonomic analysis toolset. Int. J. Occup. Saf. Ergon. 2018, 24, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Tafazzol, A.; Aref, S.; Mardani, M.; Haddad, O.; Parnianpour, M. Epidemiological and biomechanical evaluation of airline baggage handling. Int. J. Occup. Saf. Ergon. 2016, 22, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, P.S.; Punnett, L.; Moir, S.; Kuhn, S.; Buchholz, B. Does drywall installers’ innovative idea reduce the ergonomic exposures of ceiling installation: A field case study. Appl. Ergon. 2016, 55, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Hassani, M.; Hesampour, R.; Bartnicka, J.; Monjezi, N.; Ezbarami, S.M. Evaluation of working conditions, work postures, musculoskeletal disorders and low back pain among sugar production workers. Work 2022, 73, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Hassani, M.; Kabiesz, P.; Hesampour, R.; Ezbarami, S.M.; Bartnicka, J. Prevalence of musculoskeletal disorders, working conditions, and related risk factors in the meat processing industry: Comparative analysis of Iran-Poland. Work 2023, 74, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Alderson, J.; Hopper, L.; Elliott, B.; Ackland, T. Risk factors for lower back injury in male dancers performing ballet lifts. J. Danc. Med. Sci. 2009, 13, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Ziaei, M.; Choobineh, A.; Ghaem, H.; Abdoli-Eramaki, M. Evaluation of a passive low-back support exoskeleton (Ergo-Vest) for manual waste collection. Ergonomics 2021, 64, 1255–1270. [Google Scholar] [CrossRef] [PubMed]
- Larson, R.E.; Johnson, A.W.; Bruening, D.A.; Ridge, S.T.; Mitchell, U.H. The influence of bed height as a percentage of participant height on low back forces when boosting a patient up in bed. Work 2023, 75, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Van Der Beek, A.J.; Dennerlein, J.T.; Huysmans, M.A.; Mathiassen, S.E.; Burdorf, A.; Van Mechelen, W.; Van Dieën, J.H.; Frings-Dresen, M.H.; Holtermann, A.; Janwantanakul, P.; et al. A Research Framework for the Development and Implementation of Interventions Preventing Work-Related Musculoskeletal Disorders. Scand. J. Work. Environ. Health 2017, 43, 526–539. [Google Scholar] [CrossRef] [PubMed]
- Eurofound 2015. Eurofound: Brussels, Belgium, 2019. European Working Conditions Survey. Available online: https://www.eurofound.europa.eu/data/european-working-conditions-survey (accessed on 9 March 2023).
- Potvin, J. Predicting maximum acceptable efforts for repetitive tasks: An equation based on duty cycle. Hum. Factors 2012, 54, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Potvin, J. An equation to predict maximum acceptable loads for repetitive tasks based on duty cycle: Evaluation with lifting and lowering tasks. Work 2012, 41, 397–400. [Google Scholar] [CrossRef] [PubMed]
- ACGIH. Upper Limb Localized Fatigue: TLV(R) Physical Agents 7th Edition Documentation; Report number 7DOC-782; ACGIH: Cincinnati, OH, USA, 2016. [Google Scholar]
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH Equation for the Design and Evaluation of Manual Lifting Tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef]
- National Institute for Occupational Safety and Health. Work Practices Guide for Manual Lifting; Technical Report Number: 81-122; U.S. Department of Health and Human Services (NIOSH): Cincinnati, OH, USA, 1981. [Google Scholar]
- Zelik, K.E.; Nurse, C.A.; Schall, M.C., Jr.; Sesek, R.F.; Marino, M.C.; Gallagher, S. An ergonomic assessment tool for evaluating the effect of back exoskeletons on injury risk. Appl. Ergon. 2022, 99, 103619. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jäger, M. Extended compilation of autopsy-material measurements on lumbar ultimate compressive strength for deriving reference values in ergonomic work design: The Revised Dortmund Recommendations. EXCLI J. 2018, 17, 362–385. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.D.; La Delfa, N.J.; Loma, C.; Potvin, J.R. A comparison between measured female linear arm strengths and estimates from the 3D Static Strength Prediction Program (3DSSPP). Appl. Ergon. 2021, 94, 103415. [Google Scholar] [CrossRef]
- Diraneyya, M.M.; Ryu, J.; Abdel-Rahman, E.; Haas, C.T. Inertial Motion Capture-Based Whole-Body Inverse Dynamics. Sensors 2021, 21, 7353. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- INAIL. Relazione Annuale 202 del Presidente. Appendice Statistica. Rome 4 October 2023. Available online: https://www.inail.it/portale/it/inail-comunica/pubblicazioni/rapporti-e-relazioni-inail/rapporti-e-relazioni-inail-dettaglio.2023.09.relazione-annuale-2022.html (accessed on 2 August 2024).
- International Federation of Robotics. (IFR)–Position Paper “Artificial Intelligence in Robotics”. Available online: https://ifr.org/papers/artificial-intelligence-in-robotics (accessed on 1 August 2024).
- Maslej, N.; Fattorini, L.; Perrault, R.; Parli, V.; Reuel, A.; Brynjolfsson, E.; Etchemendy, J.; Ligett, K.; Lyons, T.; Manyika, J.; et al. The AI Index 2024 Annual Report, AI Index Steering Committee, Institute for Human-Centered AI; Stanford University: Stanford, CA, USA, 2024; Available online: https://aiindex.stanford.edu/report/ (accessed on 1 August 2024).
- Kuijer, P.P.F.M.; van der Wilk, S.; Evanoff, B.; Viikari-Juntura, E.; Coenen, P. What have we learned about risk assessment and interventions to prevent work-related musculoskeletal disorders and support work participation? Scand. J. Work Environ. Health 2024, 50, 317–328. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Horsak, B.; Eichmann, A.; Lauer, K.; Prock, K.; Krondorfer, P.; Siragy, T.; Dumphart, B. Concurrent validity of smartphone-based markerless motion capturing to quantify lower-limb joint kinematics in healthy and pathological gait. J. Biomech. 2023, 159, 111801. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silvetti, A.; Varrecchia, T.; Chini, G.; Tarbouriech, S.; Navarro, B.; Cherubini, A.; Draicchio, F.; Ranavolo, A. Upper-Limb and Low-Back Load Analysis in Workers Performing an Actual Industrial Use-Case with and without a Dual-Arm Collaborative Robot. Safety 2024, 10, 78. https://doi.org/10.3390/safety10030078
Silvetti A, Varrecchia T, Chini G, Tarbouriech S, Navarro B, Cherubini A, Draicchio F, Ranavolo A. Upper-Limb and Low-Back Load Analysis in Workers Performing an Actual Industrial Use-Case with and without a Dual-Arm Collaborative Robot. Safety. 2024; 10(3):78. https://doi.org/10.3390/safety10030078
Chicago/Turabian StyleSilvetti, Alessio, Tiwana Varrecchia, Giorgia Chini, Sonny Tarbouriech, Benjamin Navarro, Andrea Cherubini, Francesco Draicchio, and Alberto Ranavolo. 2024. "Upper-Limb and Low-Back Load Analysis in Workers Performing an Actual Industrial Use-Case with and without a Dual-Arm Collaborative Robot" Safety 10, no. 3: 78. https://doi.org/10.3390/safety10030078
APA StyleSilvetti, A., Varrecchia, T., Chini, G., Tarbouriech, S., Navarro, B., Cherubini, A., Draicchio, F., & Ranavolo, A. (2024). Upper-Limb and Low-Back Load Analysis in Workers Performing an Actual Industrial Use-Case with and without a Dual-Arm Collaborative Robot. Safety, 10(3), 78. https://doi.org/10.3390/safety10030078