Abstract
Numerous hospital laboratories in Indonesia need to implement improved bio-risk management (BRM) systems. There are many potential biohazards in laboratory activities that can impact health and the environment, leading to laboratory incidents. To minimize the impact and occurrence of such incidents, it is necessary to evaluate the implementation of BRM in every hospital laboratory that uses biological agents. This study was conducted in eight COVID-19 reference hospitals in Indonesia in the regions of Sumatra, Kalimantan, and Java, which have committed to implementing BRM systems in their laboratory activities. This research employed a descriptive study design and quantitative methods, with the aim of analyzing and evaluating the implementation of BRM systems in laboratories by assessing the achievements and gap analysis obtained from each laboratory. This research utilized primary data in the form of checklist forms referencing ISO 35001:2019 for the laboratory BRM system. Then, the assessments were based on virtual interviews conducted by the researcher with laboratory personnel as the primary data. The evaluation conducted on gap analysis from the seven clauses in ISO 35001:2019 across all hospitals revealed large gaps, particularly in three clauses: leadership, support, and performance. However, the aspects concerning organization, improvement, and performance evaluation were relatively satisfactory. Hence, there is a need for further improvement in leadership, support, and performance evaluation clauses. Additionally, it is essential to highlight the importance of comprehensive performance assessment, including proactive audits and continuous enhancements to achieve optimal bio-risk management.
1. Introduction
In the face of unprecedented global challenges posed by infectious diseases, the significance of robust biosafety measures in healthcare settings cannot be overstated. The outbreak of COVID-19, caused by the novel coronavirus SARS-CoV-2, underscored the critical importance of stringent biosafety protocols in hospitals, particularly in designated COVID-19 referral centers. Indonesia, similar to many other countries, has faced significant impacts from this pandemic, necessitating a comprehensive evaluation of the biosafety measures implemented in its healthcare institutions. The hospital laboratories in Indonesia are wet laboratories, meaning they use chemical and biological materials in their activities. Typically, hospital laboratories are used for testing samples derived from the human body, such as fluids and tissues. Hospital laboratories play a crucial role in disease screening, diagnosis, and medical decision-making [1]. Additionally, hospital laboratories serve as the hub for public health investigations, aiming to provide services to clients and the community in public health programs with reference to evidence-based decision-making [2]. These activities can pose pathogen-related hazards that could endanger both humans and the surrounding environment [3] due to the types of potential hazards and the magnitude of occupational risk [1].
Workplace accidents can occur due to a lack of attention to biological safety. An example of a workplace accident involving biological materials was the exposure of laboratory workers when transferring biological material from one vial to another. The vial used in this instance cracked and broke, causing the contents to spill. Fortunately, the laboratory workers were equipped with complete personal protective equipment (PPE), and no infections resulted. This illustrates that risk assessment and the implementation of biosafety and biosecurity aspects are essential, as they form the foundation of the biosafety management system [4]. Risk assessment must be carried out to ensure the safe operation of all laboratory activities [1]. The assessment involves identifying potential hazards in the laboratory, such as biological materials and equipment; evaluating laboratory activities; determining the level of biosafety risk and its mitigation; evaluating personnel; and reviewing risk assessments [5].
Risk assessment can be conducted in accordance with a bio-risk management (BRM) system, which integrates aspects of biosafety and biosecurity. The BRM system focuses on the roles and responsibilities of individuals working in the laboratory and ensures that top management plays a central role in its implementation [2]. If the evaluation reveals any gaps, the laboratory must make improvements. Risk assessment should ideally be conducted by individuals who understand the characteristics of the biological materials, research procedures, equipment, and facilities in the laboratory.
In 2020, every country in the world faced a new emerging disease, namely the COVID-19 pandemic, caused by the SARS-CoV-2 virus. On 30 January 2020, the WHO declared that the coronavirus disease, now known as COVID-19, had become a global health emergency, eventually escalating to a pandemic. This respiratory illness was initially discovered in late 2019 in Wuhan, China, and later spread worldwide, including to Indonesia. The total number of infected individuals reached 194,261,519 people (as of 24 July 2021), resulting in the deaths of up to 4,164,100 people. In Indonesia alone, there were 3,127,826 confirmed cases of SARS-CoV-2 infection, with 82,013 deaths. During the pandemic, sample-testing demands increased, and laboratories faced challenges in engineering and administrative controls, standard operating procedures (SOPs), specimen handling, personal protective equipment (PPE), and occupational health and safety [6]. Laboratories were required to enhance their ability to provide fast and accurate services [7,8]. The COVID-19 pandemic provided a real-life picture of significant issues related to the challenges of implementing biosafety and biosecurity for both local and global communities. However, the biological safety aspects in laboratories have received limited attention. Areas such as the handling of biological materials and specimen waste need further analysis to determine their level of danger, both for laboratory personnel and the environment [9].
Given this background, a risk assessment was needed to understand the characteristics of the biological materials used and the risks they may pose. This study included eight laboratories that specifically handled samples for COVID-19 testing, which were derived from eight state-owned hospitals located in various cities in Indonesia. These hospitals had committed to implementing occupational health and safety procedures in all their activities, including laboratory work.
The evaluation of BRM implementation, based on ISO 35001:2019 [10] for the BRM system, constitutes the focus of this research. Promoting, coordinating, and disseminating biosafety knowledge is a shared responsibility. Furthermore, establishing a dedicated laboratory organization is imperative to both ensuring and assessing the efficacy of biosafety aspects. Bridging the existing gap involves implementing measures to strengthen these aspects and address any deficiencies identified during the evaluation. Therefore, evaluating the gaps in this research will be the basis for improving the implementation of the laboratory biorisk management system in the future.
2. Materials and Methods
2.1. Study Design
This study was a semi-quantitative descriptive study that analyzed the bio-risk implementation in the laboratories of eight referral hospitals in Indonesia. This study was performed during the period of May–November 2022. Primary data were collected through virtual interviews with the head of each laboratory and the staff using an instrument checklist for ISO 35001:2019. There were 8 laboratories (1 per hospital) that were assessed, represented by codes H1, H2, H3, H4, H5, H6, H7, and H8.
2.2. Ethical Considerations
The present study was approved by the ethics committee of the Research and Community Engagement of the Faculty of Public Health, Universitas Indonesia, under the ethical clearance no: Ket-212/UN2.F10.D.11/PPM.00.02/2022.
2.3. Instrument and Data Analysis
The criterion for choosing these laboratories was their use of PCR (Polymerase Chain Reaction) and antigen sample testing for COVID-19. Data collection was conducted using a specialized laboratory assessment checklist form for laboratories using biological materials. The checklist form was structured following ISO 35001:2019 and consisted of 211 questions [10]. This study employed primary data obtained through virtual interviews conducted by the researcher with laboratory personnel, including laboratory heads and/or technicians. Data processing was carried out by calculating each “yes”, “no”, and “N/A” responses with values of +1, −1, and 0, respectively. The total score was calculated using the following formula:
The maximum total score that could be obtained was 100%. The calculation process was performed using Microsoft Excel (Microsoft Office 365, Microsoft, Redmond, WA, USA). After the data for all the laboratories were processed, the gap analysis was carried out. The gap analysis considered the number of aspects that were not implemented out of the 211 questions and aimed to identify how many and what aspects were not implemented among the subclauses. The analysis in this study was based on a univariate analysis with a descriptive study, and each achievement met by the laboratory was presented by an element in a chart. The overall achievement was considered satisfactory when the laboratory achieved a cumulative score of 50% [5].
3. Results
Overall, the evaluation results were calculated from each laboratory from eight hospitals (H1–H8) as percentages and involved seven clauses based on ISO 35001:2019. The clauses included organizational context, leadership, planning, support, operations, performance evaluation, and improvement (Figure 1). Among these seven clauses, some clauses required improvement, namely, leadership, planning, and support based on their gap analysis on Table 1.
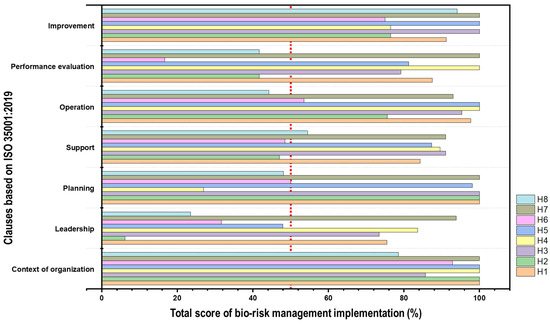
Figure 1.
Achievement results of the bio-risk management (BRM) system implementation in eight laboratory hospitals (H1–H8). The evaluation was conducted through gap analysis of the seven clauses in ISO 35001:2019. The result is the total implementation score, which is the sum of the values for each item from each laboratory hospital. The red dot indicates clauses that reach the implementation limit of up to 50%.

Table 1.
Gap analysis of laboratories from eight referral hospitals in Indonesia.
3.1. Context of Organizations
The organizational context clause consisted of seven questions, which were divided into four parts, including understanding the organization and its context, the needs and expectations of interested parties, defining the scope of the biosafety management system, and the biosafety management system itself. From the survey results, it was evident that none of the laboratories had implemented a biosafety management system (Table 2). In reality, they had implemented one but had not formalized and documented it. Activities related to biosafety were being carried out, but they did not comply with existing standards or had been implemented but without written standard operating procedures (SOPs). Documents related to the biosafety management system were also nonexistent. It can be seen that the lowest score (50%) was found in the subclause of understanding the organization and its context (H3) and the bio-risk management system in H6 and H8.
Table 2.
The percentage of performance clauses regarding context and organization implementation from each hospital laboratory.
3.2. Leadership
Many laboratories had not yet adequately fulfilled the leadership clause. Among 50 questions, only about 16% to 28% were met. This clause is divided into three parts: leadership and commitment, policies, and roles, responsibilities, and organizational authority. Only three laboratories had established good implementation in the subclause of policy. The policies had still been created in a general sense, specifically policies related to laboratory health and safety, but they were not specific to biosafety. In policy development, the initial step is to identify the hazards and risks present in the laboratory because policy content should align with the nature and scale of risks associated with the laboratory facilities and activities. These policies are then compiled into a document that is similar to existing policies. However, there will be differences in terms of personnel protection and the risk of release of biological materials and/or toxins present in the laboratory. Once policy development is completed, the policy document must be signed by top management and other relevant parties if necessary. Top management must clearly state the overall objectives of the BRM and a commitment to enhancing BRM performance. Table 3 shows the lowest scores for implementations in all subclauses.
Table 3.
The percentage of leadership clause performance implementation from each hospital laboratory.
3.3. Planning
The planning clause consists of 11 questions divided into two parts. The first part involves actions to address risks and opportunities, and the second part pertains to the objectives and biosafety management planning for achieving them. In the first part, questions revolve around risk management in the laboratory, while the second part relates to quality objectives and biosafety-related information. Table 4 shows that the implementation of each subclause was good in three of the hospital laboratories, but two laboratories required further improvement, with implementation scores of 50% or below.
Table 4.
The percentage of planning clause implementation from each hospital laboratory.
3.4. Support
The support clause consists of 55 questions divided into eight sections, namely resources, competencies, commitment, communication, documented information, security and surveillance, personal safety, and supplier control. Table 5 shows that the levels of awareness, communication, and documentation of its implementation were still mostly below 50%.
Table 5.
The percentage of performance clause implementation regarding support from each hospital laboratory.
3.5. Operation
The operations clause consisted of 43 questions divided into 10 sections, namely operational planning, and control; commissioning and decommissioning; maintenance, control, calibration, certification, and validation; physical security; inventory of biological materials; good microbiological techniques; decontamination and waste management; emergency response and emergency planning; and transportation of biological materials. The achievement of all laboratories in this clause was good. This was evident from the achievement scores being above 50%, although one hospital laboratory required improvement in emergency response and contingency planning (Table 6).
Table 6.
The percentage of operation clause implementation from each hospital laboratory.
3.6. Performance Evaluation
The performance evaluation clause generally describes the laboratory assessment process, which includes monitoring, measurement, analysis, and evaluation, as well as internal audits and management review. The achievement of this clause was still relatively poor, as almost all laboratories had not conducted specific internal audits for the BRM system (Table 7).
Table 7.
The percentage of performance clause evaluation implementation from each hospital laboratory.
3.7. Improvement
The improvement clause describes how the laboratories implement improvements based on the assessments conducted. This clause consists of three main aspects: general improvements; incidents, non-conformities, and corrective actions; and continuous improvement. The achievements in this clause varied greatly (Table 8). Hospital 2 (H-2) had the lowest score in terms of continual improvement, while H6 scored below 100% on all subclauses.
Table 8.
The percentage of improvement clause implementation from each hospital laboratory.
4. Discussion
In this study, we assessed the biosafety management systems in eight hospital laboratories, focusing on seven key clauses: organizational context, leadership, planning, support, operations, performance evaluation, and improvement. The results revealed significant variations in the implementation of these clauses among the surveyed laboratories. Biosafety is a primary concern in every laboratory globally and especially in developing countries. However, despite established guidelines, biosafety in laboratories often remains an overlooked domain in terms of its implementation in hospitals.
Table 1 shows the gap analysis, which is the sum of points that were not implemented from 211 questions. Gap analysis can identify which aspects are still lacking, allowing them to be prioritized for improvement. From the results of the gap analysis, the three aspects with the most significant gaps were leadership, support, and performance evaluation. The planning and operation aspect also needed attention. Actions to address risks and opportunities for objectives and biosafety management planning to achieve them need to be improved. Within the leadership clause, the greatest gap existed in policies and roles, responsibilities, and organizational authority. The policies in laboratory biosafety and bio-risk refer to the established guidelines and principles governing the safe and secure handling of biological materials within a laboratory setting. These policies are designed to mitigate potential risks associated with biological agents, ensuring the protection of laboratory personnel, the environment, and the surrounding community, which should receive the attention of the leader. The smallest gap was in the organizational context, planning, operations, and improvement clauses. However, these results need further examination, as the number of questions in these clauses was not the same as that in the other clauses.
The gap analysis carried out in our study found that there were differences or “gaps” between the current state of each clause in each hospital laboratory and the requirements outlined in ISO 35001:2019 regarding the bio-risk management standard. Therefore, there is a need for specialized education, learning materials, and relevant training to enhance capacity in laboratories around biosafety and biosecurity [6,11]. In various industries, including healthcare, pharmaceuticals, and manufacturing, assessing and controlling bio-risk are crucial. It is essential to minimize bio-risk, especially in contexts where sterility is critical, such as medical devices, pharmaceutical products, and certain laboratory processes [12,13,14]. Reducing bio-risk helps prevent microbial contamination, which can compromise the integrity and effectiveness of products or lead to health risks in healthcare settings. In this context, these gaps represent areas where an organization does not fully comply with the standard’s requirements. The results of the gap analysis should serve as the basis for planning and implementing the necessary changes for the organization to achieve compliance with ISO 35001 and enhance its bio-risk management [6,15].
The organizational context, which includes understanding the organization and its context, understanding the needs and expectations of interested parties, and defining the biosafety management system, showed deficiencies in formal documentation across all laboratories. While activities related to biosafety were being practiced, formalization through written standard operating procedures (SOPs) was lacking. Similarly, the leadership clause exhibited notable gaps, especially in policies and roles. Based on the assessment, only three laboratories had specific biosafety-related policies (H1, H4, H7), and those in existence were often general and not tailored to the unique risks associated with biological materials. To establish a laboratory biosafety management system, an organization must be able to develop and enhance the system in place by setting objectives and goals. Commitment should also be fostered by top management through providing adequate resources and prioritizing communication regarding biosafety regulations, incorporating biosafety management into the organizational system, and identifying improvements and prevention related to incidents caused by biological materials [4].
Unfortunately, policies are still created in a general sense, specifically policies related to laboratory health and safety, but they are often not specific to biosafety [3]. In policy development, the initial step is to identify the hazards and risks present in the laboratory because policy content should align with the nature and scale of risks associated with laboratory facilities and activities. These policies are then compiled into a document that is similar to existing policies. However, there will be differences in terms of personnel protection and the risk of release of biological materials and/or toxins present in the laboratory. Once policy development is completed, the policy document must be signed by top management and other relevant parties if necessary. Top management must clearly state the overall objectives of the BRM and their commitment to enhancing BRM performance.
The planning of the BRM, which involves risk management and setting biosafety objectives, was inadequately implemented in two laboratories. These aspects are critical for ensuring personnel safety and effective biosafety practices. This is closely related to the implementation of the BRM system. In its implementation, various approaches are needed, such as dialogue, partnerships, and consultations with relevant parties [4]. The term “relevant parties” in this context refers to international organizations, regional organizations, national organizations, institutions, and at the lowest level, laboratory personnel [12]. The appointment of personnel according to their competencies is also essential, including the formation of a BRM committee consisting of scientific managers, additional scientific specialists, BRM advisors, security managers, and healthcare professionals. The scientific manager holds the primary responsibility among these pertinent parties, as they are typically the ones most actively involved in the direct management of the laboratory. It is essential to designate individuals responsible for supervising various aspects of the facility’s scientific program to ensure clarity regarding each staff member’s roles and responsibilities [12]. Besides this, the presence of biosafety officers is also necessary to support the implementation of BMR in the laboratory. A biosafety officer is a professional responsible for managing and ensuring the safety and security of biological materials, as well as assessing and mitigating risks associated with their handling and use. Appointments for a biosafety officer should be based on experience, educational background, and the ability to handle biological hazards in the laboratory.
In risk management, laboratories are required to prepare risk assessments for each activity. Some laboratories in this study had already undertaken this task, particularly those that had participated in risk assessment training. However, several of the laboratories were unaware of how to document the risk assessments. According to Gribble et al. [4], factors driving an organization to conduct risk assessments include the use of infectious materials, toxins, and other hazardous materials; the existence of standard operating procedures (SOPs) for practical work and research; new laboratory equipment and personnel; how to provide the personal protective equipment (PPE); and third-party waste management; workplace accidents and theft; disease outbreaks and pandemics; and also changes in infrastructure, such as electrical and plumbing systems. Risk assessments for each activity in a laboratory setting involve a systematic evaluation of potential hazards associated with specific tasks or processes. The goal is to identify, analyze, and prioritize risks to implement appropriate controls and mitigation strategies [1,2]. These acts will affect the planning and the appropriate procedures in each hospital.
Risk assessments are considered very important because their results can be used for budget planning in the following year, for instance, in planning laboratory design renovations, including facility adjustments and required equipment. Furthermore, risk assessment documents can also be used to evaluate and validate emergency response plans [10]. The hospital with the lowest implementation percentage, H4 (10%), did not show enough evidence regarding the implementation of risk assessment. Meanwhile, hospitals with implementation percentages above 80% provided evidence of periodically reviewing and updating risk assessments, particularly when there were changes in procedures, equipment, or personnel. Through systematic risk assessments for every laboratory activity and the implementation of effective controls, organizations can improve overall safety, reduce incidents, and establish a secure working environment for personnel. Assessing and managing risk are fundamental components of an effective biosafety and biosecurity program. Risk assessment involves identifying and evaluating potential hazards associated with biological agents and activities, while risk management entails implementing measures to mitigate or control these risks. These processes are essential for ensuring the safety of personnel, the environment, and the public in laboratories and other facilities working with biological materials [4]. This process includes job-desk analysis determination, risk management design, occupational health and safety-related standard operating procedures (SOPs), and the compilation and documentation of a list of hazardous materials (B3) and of guidelines for the management of hazardous materials (B3) [6].
Ideally, laboratories should define quality objectives and goals from the outset. Top management, such as the hospital director, should periodically monitor progress to ensure the achievement of these objectives. As an initial step in implementing a laboratory bio-risk management system, the approaches discussed earlier can be employed. Additionally, there should be a socialization process related to the laboratory bio-management system, targeting top management and laboratory personnel. Among all the laboratories, the largest gap was found in the resources section, particularly in the subsections of worker vaccination, competence in personnel reliability actions, and documented information. Through this socialization process, awareness of the risks and biohazards present in the laboratory and the materials used should be increased [6].
Communication was generally implemented well in all laboratories. Communication between laboratory workers and the laboratory head and/or head researcher was shown to be established. This was evident by the presence of effective communication guidelines and the delivery of information and education to patients. Regular meetings to discuss laboratory activities and address any challenges or issues faced in the laboratory were also noted. Challenges included equipment damage or maintenance, procurement of materials, personnel training needs, issues with vendors, and documentation completeness related to biosafety health and safety and other relevant information.
The operations clause generally showed good implementation across laboratories. However, there were shortcomings in emergency response and contingency planning, indicating a need for improvement in handling unexpected biosafety incidents. Previous studies have also reported a need for improvement in emergency response and emergency planning, and in this study, not all laboratories had a specific emergency response program for biosafety [16]. Emergency response programs have only been established for natural disasters, fires, and chemical spills. There is no specific training related to biosafety emergency responses. Conducting training would aim to increase the laboratory personnel’s awareness of biosafety issues, including the relevance of human factors in biosafety management [17,18]. Organizations must ensure that facilities, equipment, and processes are designed, operated, and managed safely and comfortably in relation to bioburden management. Bioburden encompasses the total microbial load, including bacteria, fungi, viruses, and other microorganisms, present on surfaces, equipment, or raw materials.
In practice, emergency responses can be challenging because they require support from various parties, such as campus security units, hospitals and/or healthcare facilities at the university, fire departments, police, and so on [5]. However, local emergency drills or desktop exercises can be done as the alternative to support the facilities. This once again highlights the importance of commitment from top management, as the overall responsibility for biosafety management lies with top management, who manage the facility and can support the implementation of a bio-risk management system [4].
Performance evaluation, involving internal audits and management reviews, was found to be lacking in all of the studied laboratories. This deficiency highlights the need for regular assessments to ensure the effectiveness of biosafety measures. Usually, audits are only performed for general occupational health and safety [4]. Regular inspections or audits are crucial in laboratory management, especially facility and equipment inspections, as routine maintenance and checks are needed to ensure that equipment is being used in accordance with standards. This helps to reduce risks and hazards to the lowest level [19]. To encourage laboratories to conduct routine inspections and audits, awareness of their importance must be increased [20]. An awareness campaign should target the top-level management in laboratories so that future budgets can be allocated for audits. During these awareness campaigns, it is crucial to emphasize that routine inspections or audits can significantly improve laboratory design, construction, operational processes, and management systems [21]. Additionally, routine inspections or audits help top management identify deficiencies in the laboratory, providing a basis for gradual improvements [22]. If a laboratory conducts internal audits, it will have specific records, such as monitoring results, measurements, and audit findings, to serve as the basis for improvement [4,18].
Organizations must continually improve the effectiveness of their BRM systems via the use of policies, objectives, self-audit programs, audit results, data analysis, risk assessments, corrective and preventive actions, and management reviews [23]. Corrective actions must be taken in the event of an incident, including identifying personnel responsible for the accident/incident reporting system. The accident and incident investigation process should preferably utilize the available data, such as risk assessments, standard operating procedures (SOPs), emergency response plans, accident reports, interviews with relevant individuals, inspections, and staff training records [24]. The organization should strive to implement the development and improvement of the system to ensure that enhancements are identified and applied [8]. This can be achieved through goal setting and targets placed on the management system working within the facility and through monitoring progress to ensure that objectives can be achieved.
One method that can be employed to enhance biosafety aspects in laboratory activities is using the plan–do–check–act (PDCA) methodology. In the plan phase, objectives and processes are established to achieve results in alignment with the ISO 35,001 standard. This involves defining the scope of the management system, identifying relevant risks and opportunities, and subsequently developing a plan to address the identified risks and opportunities. Following this, the management can allocate necessary resources, encompassing personnel, technology, and finances. During the do phase, the planned processes are implemented. It is essential to ensure that personnel are cognizant of their roles and responsibilities concerning ISO 35001 compliance. Employee training on pertinent procedures and requirements is conducted, and the outlined processes in the plan are executed.
For the check phase, the laboratory can monitor and measure processes and services against the ISO 35001 requirements. Relevant data are collected and analyzed to evaluate the effectiveness of the management system. Internal audits are conducted to ensure compliance, and the system’s performance is assessed against key performance indicators. In the act phase, corrective actions are taken to address any identified non-conformities or areas for improvement. Continuous efforts are made to identify opportunities for enhancement. The management system, policies, and procedures are adjusted based on the results of monitoring and evaluation. Any changes are communicated to relevant stakeholders [1,2,4,25].
The results of this study highlight the significance of establishing clear and specific biosafety guidelines for laboratories, tailored to their individual risks. It is crucial to address deficiencies in leadership, planning, and support. Laboratories should concentrate on developing precise biosafety protocols, refining risk management techniques, enhancing communication, and guaranteeing sufficient resources. Additionally, regular internal audits and management reviews are essential to monitoring and improving biosafety management systems over time. Furthermore, efforts should be directed toward enhancing emergency response and contingency planning in order to handle unforeseen biosafety incidents as effectively as possible.
5. Conclusions
This study emphasized the current state of BRM systems within the healthcare facility environment, specifically in eight COVID-19 referral hospitals in Indonesia. The results of this study indicated that most laboratories in these hospitals generally still have gaps between biosafety standards and the implementation of their BRM systems. This research highlights the need for improvements in the BRM system in every hospital laboratory based on the gap analysis. The aspects with the greatest gaps were leadership, planning, and support. These aspects need to be addressed to ensure that the bio-risk management systems in the laboratories are effective. To improve BRM implementation, we can use a familiar model approach: the PDCA (plan–do–check–act) model. This model is popular as a concept that can guide organizations in achieving sustainable processes and improvements. The improvements that should be considered include policies and procedures, operational practices, education and training, resources, and monitoring and evaluation according to the standard’s requirements. Closing these gaps is vital, not only to meet standards, but more significantly, to safeguard the well-being of laboratory staff and the wider community. Subsequent studies and efforts should focus on specialized training, creation of policies, and ongoing evaluation to promote a culture of excellent biosafety practices in hospital laboratories.
Author Contributions
Conceptualization, A.B., W.H. and F.L.; methodology, W.H., A.K., S.A.S. and D.L.; software, A.K. and S.A.S.; validation, W.H., A.K. and S.A.S.; formal analysis, W.H., A.K., S.A.S., F.L., A.B. and S.G.; investigation, A.K., D.L. and S.A.S.; resources, A.Z.A.; data curation, A.Z.A.; writing—original draft preparation, W.H., A.B., F.L., A.K., S.A.S., D.L. and A.Z.A.; writing—review and editing, W.H., A.B., F.L., A.K., S.A.S., D.L., A.Z.A. and S.G.; visualization, A.K.; supervision, A.B., F.L. and S.G.; project administration, A.Z.A.; funding acquisition, W.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Directorate of Research and Development, Universitas Indonesia, Under Hibah PUTI Q2 [grant number NKB-1311/UN2.RST/HKP.05.00/2022].
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (or Ethics Committee) of the Research and Community Engagement of Faculty of Public Health, Universitas Indonesia, under ethical clearance no. Ket-212/UN2.F10.D.11/PPM.00.02/2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
Data are contained within the article.
Acknowledgments
The authors would like to thank the directors, laboratory managers, and laboratory staff from hospitals H1–H8 for participating in this study. For the support given to complete this study, the authors also thank the Faculty of Mathematics and Natural Sciences, Universitas Indonesia; the Faculty of Public Health Universitas Indonesia; and the Disaster and Risk Reduction Centre, Universitas Indonesia.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lestari, F.; Kadir, A.; Miswary, T.; Maharani, C.F.; Bowolaksono, A.; Paramitasari, D. Implementation of Bio-Risk Management System in a National Clinical and Medical Referral Centre Laboratories. Int. J. Environ. Res. Public Health 2021, 18, 2308. [Google Scholar] [CrossRef] [PubMed]
- Bowolaksono, A.; Lestari, F.; Satyawardhani, S.A.; Kadir, A.; Maharani, C.F.; Paramitasari, D. Analysis of Bio-Risk Management System Implementation in Indonesian Higher Education Laboratory. Int. J. Environ. Res. Public Health 2021, 18, 5076. [Google Scholar] [CrossRef] [PubMed]
- Bakanidze, L.; Imnadze, P.; Perkins, D. Biosafety and Biosecurity as Essential Pillars of International Health Security and Cross-Cutting Elements of Biological Nonproliferation. BMC Public Health 2010, 10 (Suppl. S1), S12. [Google Scholar] [CrossRef] [PubMed]
- Salerno, R.M.; Gaudioso, J. Laboratory Biorisk Management: Biosafety and Biosecurity, 1st ed.; CRC Press: Boca Raton, FL, USA, 2015; Volume 19, ISBN 978-1-4665-9365-7. [Google Scholar]
- Naroeni, A.; Bachtiar, E.W.; Ibrahim, F.; Bela, B.; Kusminanti, Y.; Pujiriani, I.; Lestari, F. Challenges in Implementing a Biorisk Management Program at Universitas Indonesia: A Checklist Tool for Biorisk Management. Health Secur. 2016, 14, 375–381. [Google Scholar] [CrossRef]
- Callihan, D.R.; Downing, M.; Meyer, E.; Ochoa, L.A.; Petuch, B.; Tranchell, P.; White, D. Considerations for Laboratory Biosafety and Biosecurity during the Coronavirus Disease 2019 Pandemic: Applying the ISO 35001:2019 Standard and High-Reliability Organizations Principles. Appl. Biosaf. 2021, 26, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Putri, Z.T.; Fahma, F.; Sutopo, W.; Zakaria, R. A Framework to Measure Readiness Level of Laboratory for Implementing ISO/IEC 17025: A Case Study. IOP Conf. Ser. Mater. Sci. Eng. 2019, 495, 012011. [Google Scholar] [CrossRef]
- Tamil, S.M.; Srinivas, A. Evaluation of Quality Management Systems Implementation in Medical Diagnostic Laboratories Benchmarked for Accreditation. J. Med. Lab. Diagn. 2015, 6, 27–35. [Google Scholar] [CrossRef]
- Qasmi, S.A.; Khan, B.A. Survey of Suspected Laboratory-Acquired Infections and Biosafety Practices in Research, Clinical, and Veterinary Laboratories in Karachi, Pakistan. Health Secur. 2019, 17, 372–383. [Google Scholar] [CrossRef]
- ISO 35001:2019; Biorisk Management for Laboratories and Other Related Organisations, 1st ed. The International Organization for Standardization: Geneva, Switzerland, 2019; pp. 7–25.
- Susanti, I.; Susilarini, N.K.; Setiawaty, V. Assessment of Biorisk Management Implementation in NIHRD Laboratory as National Referral Laboratory of Emerging Infectious Diseases in Indonesia. Health Sci. J. Indones. 2018, 9, 70–75. [Google Scholar] [CrossRef]
- Castriciones, E.V.; Vijayan, V. Biosecurity Risk Mapping and Gap Analysis in South East Asia. J. Biosaf. Biosecurity 2020, 2, 36–43. [Google Scholar] [CrossRef]
- Oladeinde, B.H.; Omoregie, R.; Odia, I.; Osakue, E.O.; Imade, O.S. Biorisk Assessment of Medical Diagnostic Laboratories in Nigeria. Saf. Health Work 2013, 4, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Kagirita, A.A.; Owalla, T.J.; Okwalinga, P.; Opio, J.; Baguma, A.; Mugasha, R.; Kakooza, F.; Ojwiya, A.; Aisu, S.; Eragu, R.; et al. Biorisk Management Practices in Public and Private Laboratories in Uganda: A Nationwide Baseline Survey. J. Bioterror. Biodef. 2018, 9, 1–7. [Google Scholar] [CrossRef]
- Zaki, A.N. Biosafety and Biosecurity Measures: Management of Biosafety Level 3 Facilities. Int. J. Antimicrob. Agents 2010, 36, S70–S74. [Google Scholar] [CrossRef] [PubMed]
- Arfin Qasmi, S.; Pirzada, S.; Ghani, A.; Mohsin, S. Survey on Proper and Safe Use of Biological Safety Cabinets (BSCs) in Research, Bio-Medical and Animal Laboratories in Karachi, Pakistan a Cross Sectional Study. J. Biosaf. Biosecurity 2020, 2, 77–80. [Google Scholar] [CrossRef]
- Ali, K.; Kabir, F.; Meyer, E. Editorial: Biorisk Management, Laboratory Acquired Infections and Clinical Containment. Front. Public Health 2023, 11, 1127856. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Laboratory Biorisk Management: Strategic Framework for Action 2012–2016; World Health Organization: Geneva, Switzerland, 2012; p. 16. [Google Scholar]
- Li, N.; Hu, L.; Jin, A.; Li, J. Biosafety Laboratory Risk Assessment. J. Biosaf. Biosecurity 2019, 1, 90–92. [Google Scholar] [CrossRef]
- Jucan, M.S.; Jucan, C.N. The Power of Science Communication. Procedia Soc. Behav. Sci. 2014, 149, 461–466. [Google Scholar] [CrossRef]
- Zhai, P.; Wang, R.; Zhou, Y.; Hu, D.; Li, J.; Zhou, Y. Enhancing the Capabilities of Biosafety Laboratories through the Established Accreditation System: Development of the Biosafety Laboratory Accreditation System in China. J. Biosaf. Biosecurity 2019, 1, 86–89. [Google Scholar] [CrossRef]
- Blacksell, S.D.; Dhawan, S.; Kusumoto, M.; Le, K.K.; Summermatter, K.; O’Keefe, J.; Kozlovac, J.; Almuhairi, S.S.; Sendow, I.; Scheel, C.M.; et al. The Biosafety Research Road Map: The Search for Evidence to Support Practices in Human and Veterinary Laboratories. Appl. Biosaf. 2023, 28, 64–71. [Google Scholar] [CrossRef]
- Muhammad, J.; Sarwar, S.; Khan, T.; Qasmi, S.A.; Ikram, A.; Ahmad, G.; Zahid, M.; Durrani, R.H.; Ahmed, F. A Cross-Sectional Survey to Assess Biorisk Management System in Research and Diagnostic Laboratories in Khyber Pakhtunkhwa, Pakistan. Front. Public Health 2021, 9, 766162. [Google Scholar] [CrossRef]
- International Labour Organization. Technical Guidelines on Biological Hazards; International Labour Organization: Geneva, Switzerland, 2022; pp. 20–24. ISBN 978-92-2-037717-8. [Google Scholar]
- Fruchtnicht, E.; Eaker, N.; Fellers, J.; Urbanczyk, B.; Robertson, C.; Dhakal, M.; Colman, S.; Freas-Lutz, D.; Patterson, H.; Bazan, C.; et al. Plan-do-Check-Act: A University Laboratory Equipment Decontamination Case Study. Prof. Saf. 2019, 64, 43–51. Available online: https://www.jstor.org/stable/48689819 (accessed on 29 January 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).