
Opportunistic Diagnostics of Dental Implants in Routine Clinical Photon-Counting CT Acquisitions

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Image Acquisition and Reconstruction
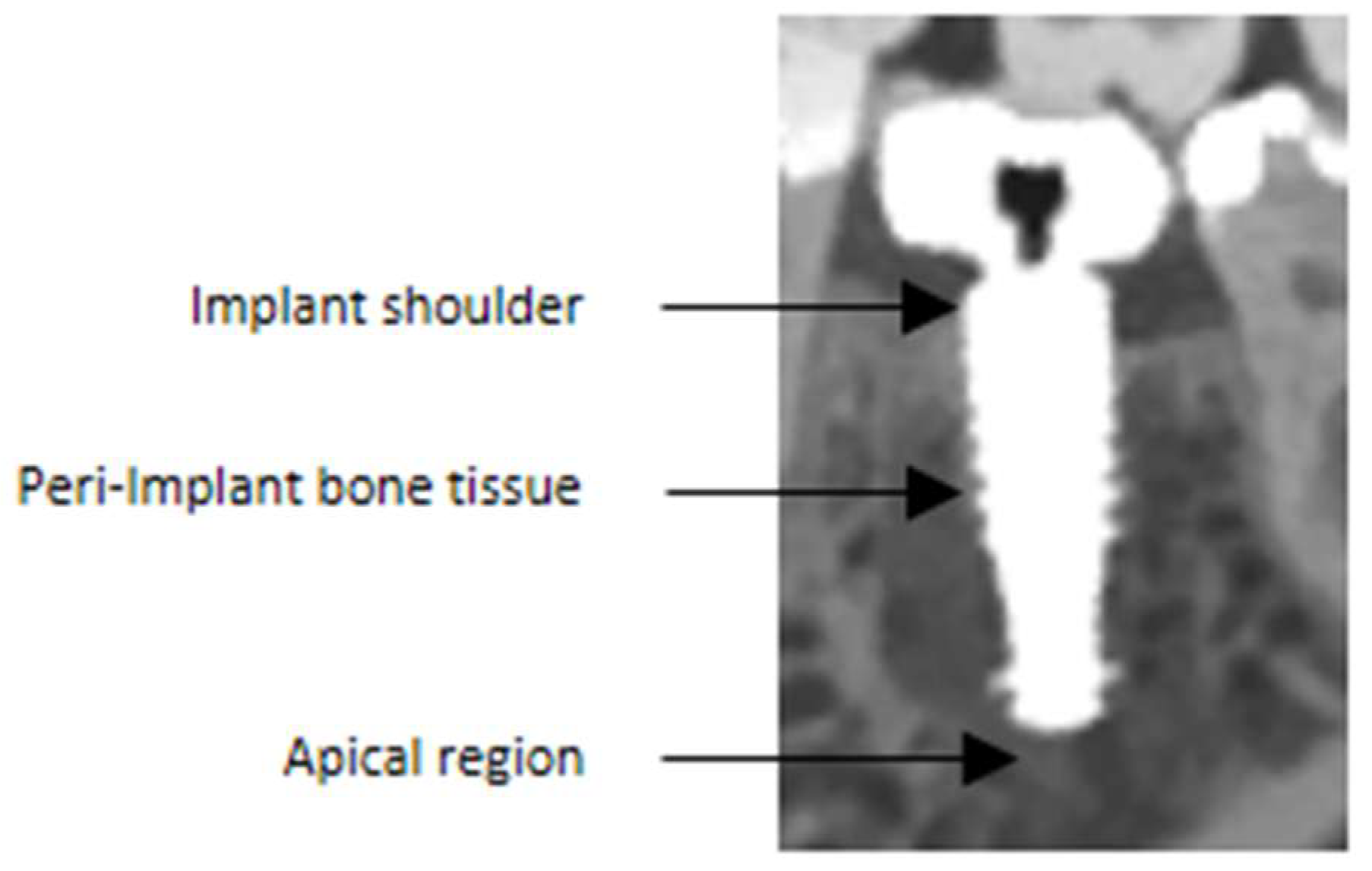
2.3. Qualitative and Quantitative Image Analysis
2.4. Statistical Evaluation
3. Results
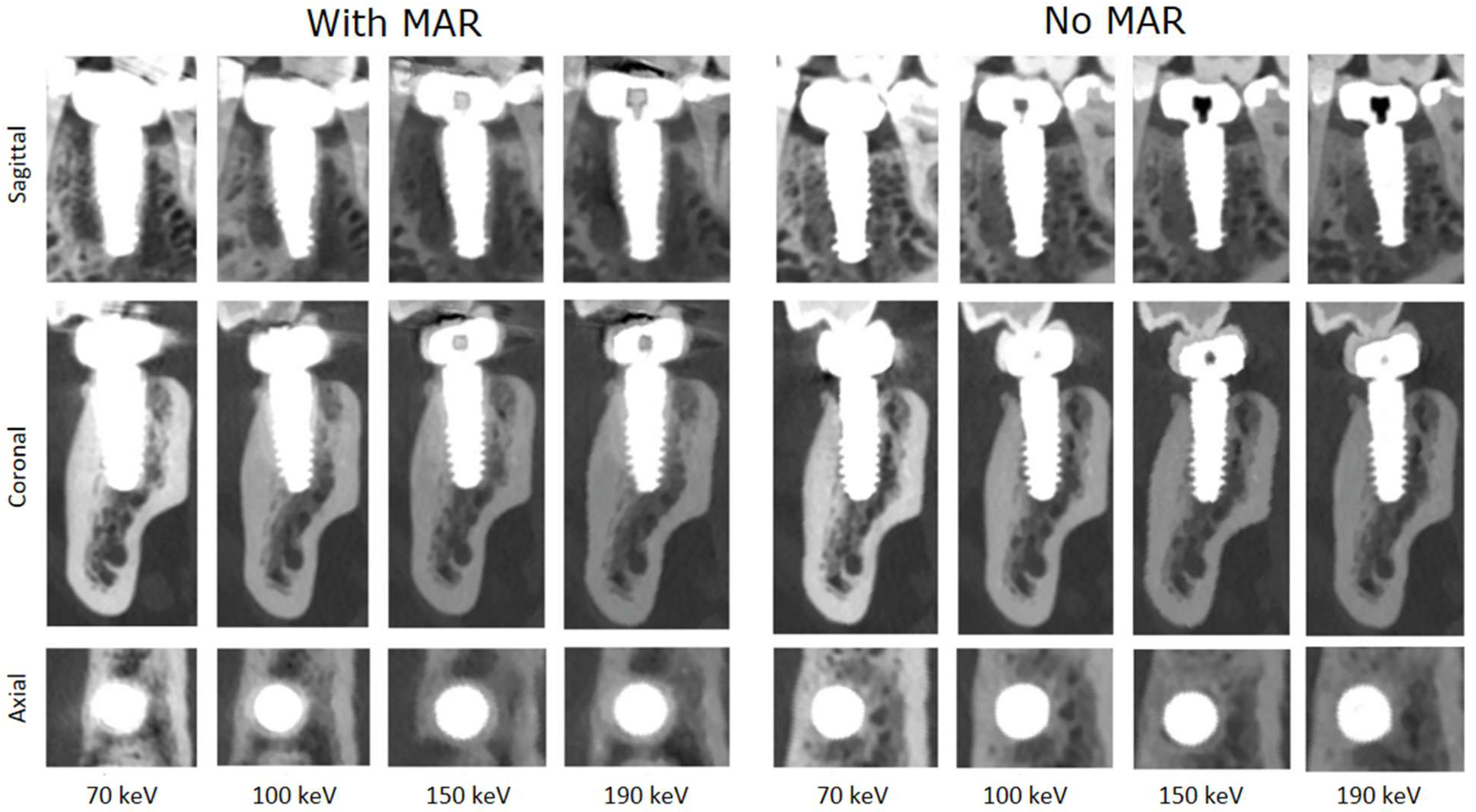
3.1. Image Quality Quantification and Metal Artifact Reduction
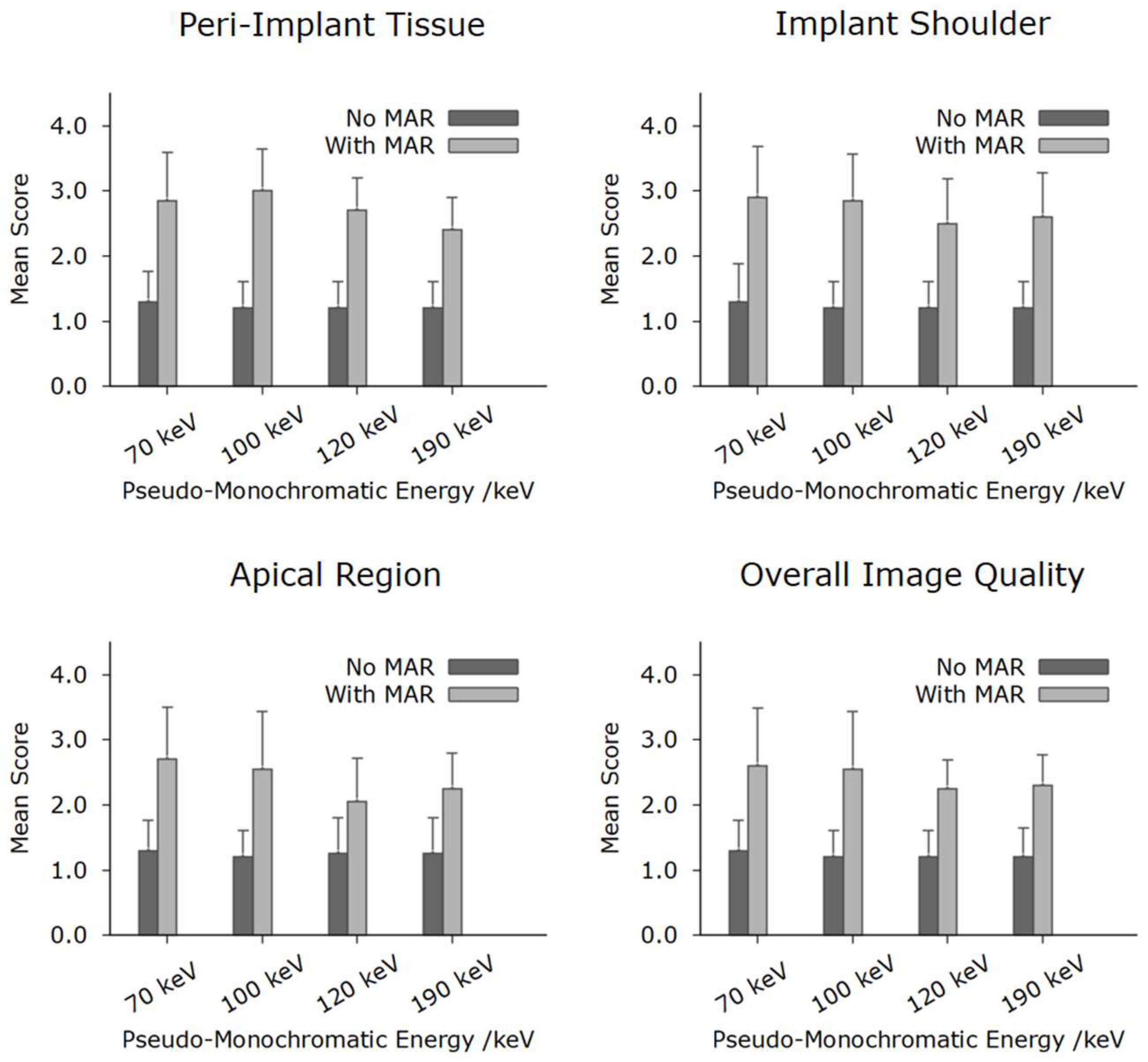
3.2. Qualitative Analysis
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CNR | contrast-to-noise ratio |
| CT | computed tomography |
| CTDI | CT dose index |
| CBCT | cone beam computed tomography |
| FOV | field of view |
| PCCT | photon-counting CT |
| QIR | Quantum Iterative Reconstruction |
| MAR | metal artefact reduction |
References
- Strahlenschutz, B.f. 2022. Available online: https://www.bfs.de/DE/themen/ion/anwendung-medizin/diagnostik/roentgen/haeufigkeit-exposition.html (accessed on 10 May 2025).
- Fleischmann, D.; Boas, F.E. Computed tomography—Old ideas and new technology. Eur. Radiol. 2011, 21, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Schlemmer, H.-P. The Eye of the CT Scanner: The story of learning to see the invisible or from the fluorescent screen to the photon-counting detector. RoFo 2021, 193, 1034–1049. [Google Scholar] [CrossRef] [PubMed]
- Lell, M.; Kachelrieß, M. Computed Tomography 2.0: New Detector Technology, AI, and Other Developments. Investig. Radiol. 2023, 58, 587–601. [Google Scholar] [CrossRef] [PubMed]
- Lell, M.; Kachelrieß, M. Recent and Upcoming Technological Developments in Computed Tomography: High Speed, Low Dose, Deep Learning, Multienergy. Investig. Radiol. 2020, 55, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Ruetters, M.; Sen, S.; Gehrig, H.; Bruckner, T.; Kim, T.-S.; Lux, C.J.; Schlemmer, H.-P.; Heinze, S.; Maier, J.; Kachelrieß, M.; et al. Dental imaging using an ultra-high resolution photon-counting CT system. Sci. Rep. 2022, 12, 7125. [Google Scholar] [CrossRef] [PubMed]
- Sawall, S.; Maier, J.; Sen, S.; Gehrig, H.; Kim, T.-S.; Schlemmer, H.-P.; Schönberg, S.O.; Kachelrieß, M.; Rütters, M. Dental imaging in clinical photon-counting CT at a quarter of DVT dose. J. Dent. 2024, 142, 104859. [Google Scholar] [CrossRef] [PubMed]
- Fontenele, R.C.; Picoli, F.F.; Pinto, J.C.; Coudyzer, W.; Vasconcelos, K.d.F.; Gomes, A.F.; Binst, J.; Jacobs, R. Feasibility of photon-counting computed tomography as a novel imaging modality for challenging endodontic diagnostic tasks. Sci. Rep. 2023, 13, 6266. [Google Scholar] [CrossRef] [PubMed]
- Husain, A.A.-H.; Mergen, V.; Valdec, S.; Husain, N.A.-H.; Stadlinger, B.; Essig, H.; Frauenfelder, T.; Kessler, P.; Lie, S.A.N.; Alkadhi, H.; et al. Comparison of cone-beam computed tomography with photon-counting detector computed tomography for dental implant surgery. Int. J. Implant. Dent. 2025, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Listl, S.; Galloway, J.; Mossey, P.; Marcenes, W. Global Economic Impact of Dental Diseases. J. Dent. Res. 2015, 94, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Gala, d.l.H. Bekanntmachung der Aktualisierten Diagnostischen Referenzwerte für Diagnostische und Interventionelle Röntgenanwendungen; Bundesamt für Strahlenschutz: Salzgitter, Germany, 2022; p. 7. [Google Scholar]
- Aissa, J.; Boos, J.; Sawicki, L.M.; Heinzler, N.; Krzymyk, K.; Sedlmair, M.; Kröpil, P.; Antoch, G.; Thomas, C. Iterative metal artefact reduction (MAR) in postsurgical chest CT: Comparison of three iMAR-algorithms. Br. J. Radiol. 2017, 90, 20160778. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.; Raupach, R.; Lell, M.; Schmidt, B.; Kachelrieß, M. Frequency split metal artifact reduction (FSMAR) in computed tomography. Med. Phys. 2012, 39, 1904–1916. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.; Raupach, R.; Lell, M.; Schmidt, B.; Kachelrieß, M. Normalized metal artifact reduction (NMAR) in computed tomography. Med. Phys. 2010, 37, 5482–5493. [Google Scholar] [CrossRef] [PubMed]
- Patzer, T.S.; Kunz, A.S.; Huflage, H.; Gruschwitz, P.; Pannenbecker, P.; Afat, S.; Herrmann, J.; Petritsch, B.; Bley, T.A.; Grunz, J.-P. Combining virtual monoenergetic imaging and iterative metal artifact reduction in first-generation photon-counting computed tomography of patients with dental implants. Eur. Radiol. 2023, 33, 7818–7829. [Google Scholar] [CrossRef] [PubMed]
- Schreck, J.; Niehoff, J.H.; Saeed, S.; Kroeger, J.R.; Lennartz, S.; Laukamp, K.R.; Borggrefe, J.; Michael, A.E. Dental implant artifacts: Evaluation of photon counting CT-derived virtual monoenergetic images in combination with iterative metal artifact reduction algorithms. Eur. J. Radiol. 2025, 187, 112117. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S237–S248. [Google Scholar] [CrossRef] [PubMed]
- Rajpurkar, P.; Chen, E.; Banerjee, O.; Topol, E.J. AI in health and medicine. Nat. Med. 2022, 28, 31–38. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trajectory | Spiral |
| CT Dose Index | 13.2 mGy (CTDI32cm) |
| Tube Voltage | 120 kV |
| Reconstruction | QIR(3) |
| Voxel Size | 156 µm |
| Slice Thickness | 400 µm |
| Slice Increment | 200 µm |
| Kernel | Qr64 |
| With Metal Artifact Reduction | ||||
|---|---|---|---|---|
| 70 keV | 100 keV | 150 keV | 190 keV | |
| Peri-Implant Tissue | 0.914 | 0.795 | 1.000 | 1.000 |
| Implant Shoulder | 0.846 | 0.914 | 1.000 | 0.916 |
| Apical Region | 0.851 | 0.818 | 0.899 | 0.842 |
| Overall Image Quality | 0.815 | 0.818 | 0.757 | 1.000 |
| Without Metal Artifact Reduction | ||||
| 70 keV | 100 keV | 150 keV | 190 keV | |
| Peri-Implant Tissue | 1.000 | 1.000 | 1.000 | 1.000 |
| Implant Shoulder | 1.000 | 1.000 | 1.000 | 1.000 |
| Apical Region | 1.000 | 1.000 | 0.842 | 0.842 |
| Overall Image Quality | 1.000 | 1.000 | 1.000 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruetters, M.; Gehrig, H.; Mertens, C.; Sen, S.; Kim, T.-S.; Schlemmer, H.-P.; Ziener, C.H.; Schoenberg, S.; Froelich, M.; Kachelrieß, M.; et al. Opportunistic Diagnostics of Dental Implants in Routine Clinical Photon-Counting CT Acquisitions. J. Imaging 2025, 11, 215. https://doi.org/10.3390/jimaging11070215
Ruetters M, Gehrig H, Mertens C, Sen S, Kim T-S, Schlemmer H-P, Ziener CH, Schoenberg S, Froelich M, Kachelrieß M, et al. Opportunistic Diagnostics of Dental Implants in Routine Clinical Photon-Counting CT Acquisitions. Journal of Imaging. 2025; 11(7):215. https://doi.org/10.3390/jimaging11070215
Chicago/Turabian StyleRuetters, Maurice, Holger Gehrig, Christian Mertens, Sinan Sen, Ti-Sun Kim, Heinz-Peter Schlemmer, Christian H. Ziener, Stefan Schoenberg, Matthias Froelich, Marc Kachelrieß, and et al. 2025. "Opportunistic Diagnostics of Dental Implants in Routine Clinical Photon-Counting CT Acquisitions" Journal of Imaging 11, no. 7: 215. https://doi.org/10.3390/jimaging11070215
APA StyleRuetters, M., Gehrig, H., Mertens, C., Sen, S., Kim, T.-S., Schlemmer, H.-P., Ziener, C. H., Schoenberg, S., Froelich, M., Kachelrieß, M., & Sawall, S. (2025). Opportunistic Diagnostics of Dental Implants in Routine Clinical Photon-Counting CT Acquisitions. Journal of Imaging, 11(7), 215. https://doi.org/10.3390/jimaging11070215