

Biodegradable and Mechanically Resilient Recombinant Collagen/PEG/Catechol Cryogel Hemostat for Deep Non-Compressible Hemorrhage and Wound Healing


Abstract
1. Introduction
2. Results and Discussion
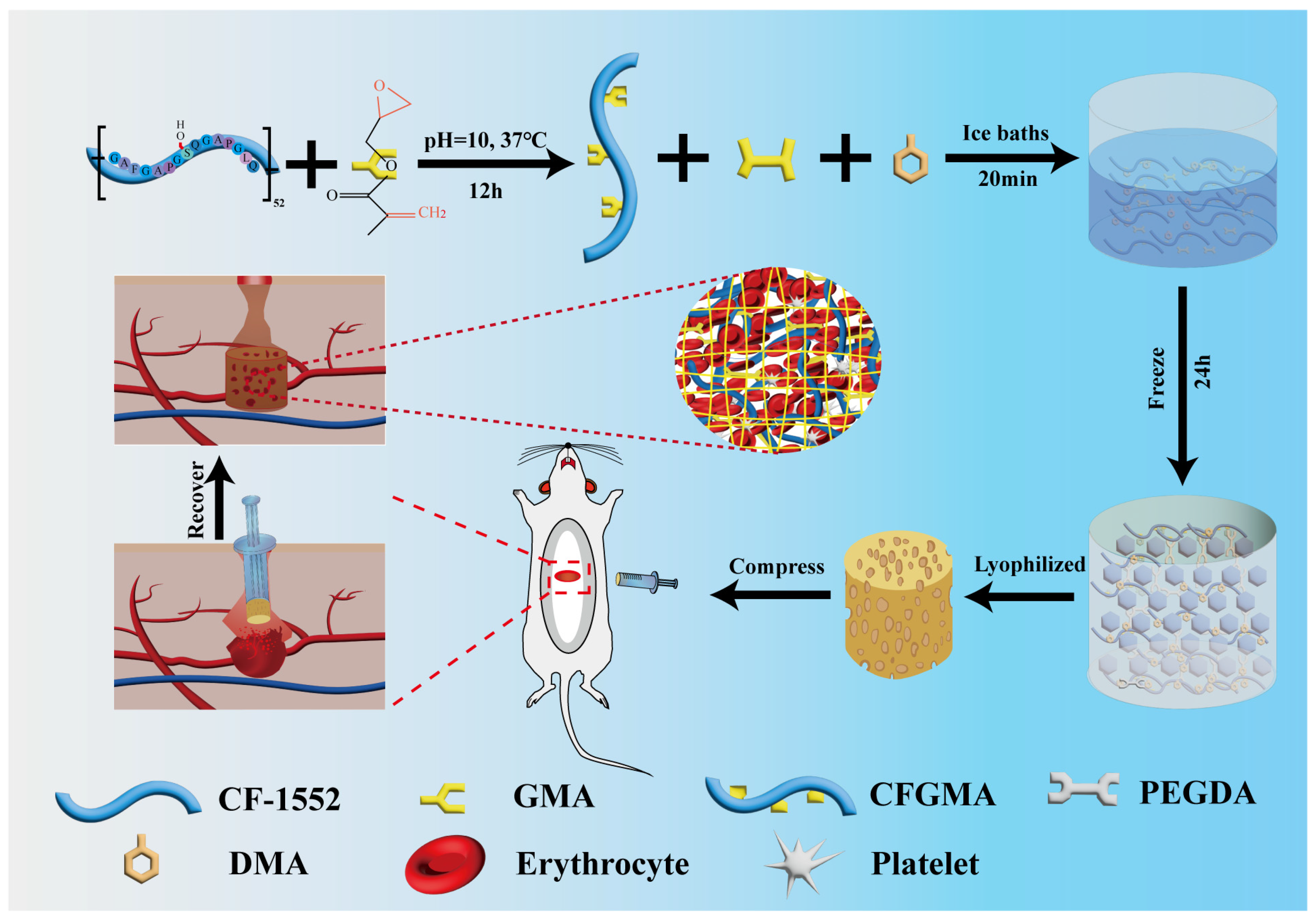
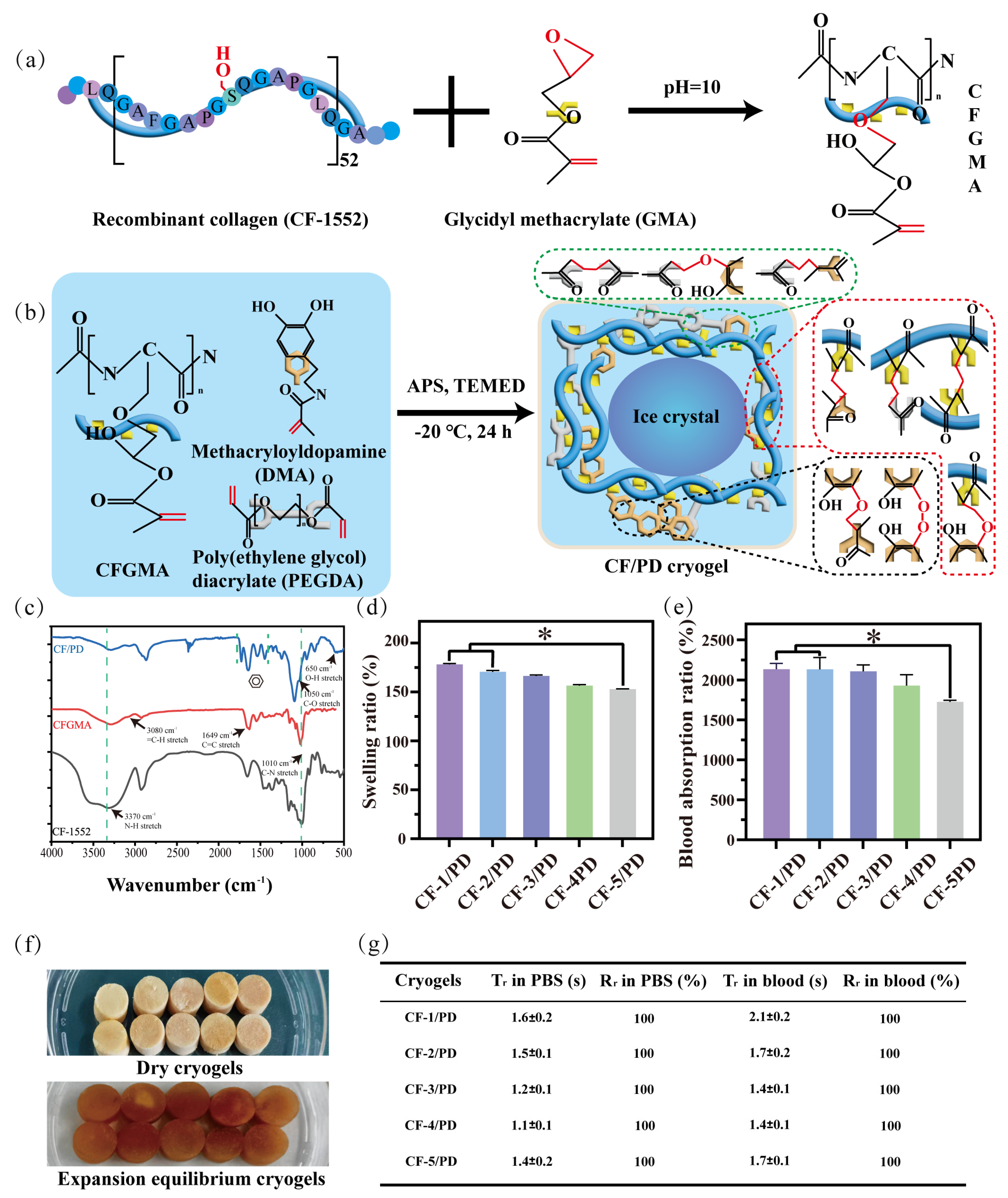
2.1. Synthesis and Characterization of CFGMA and CF/PD
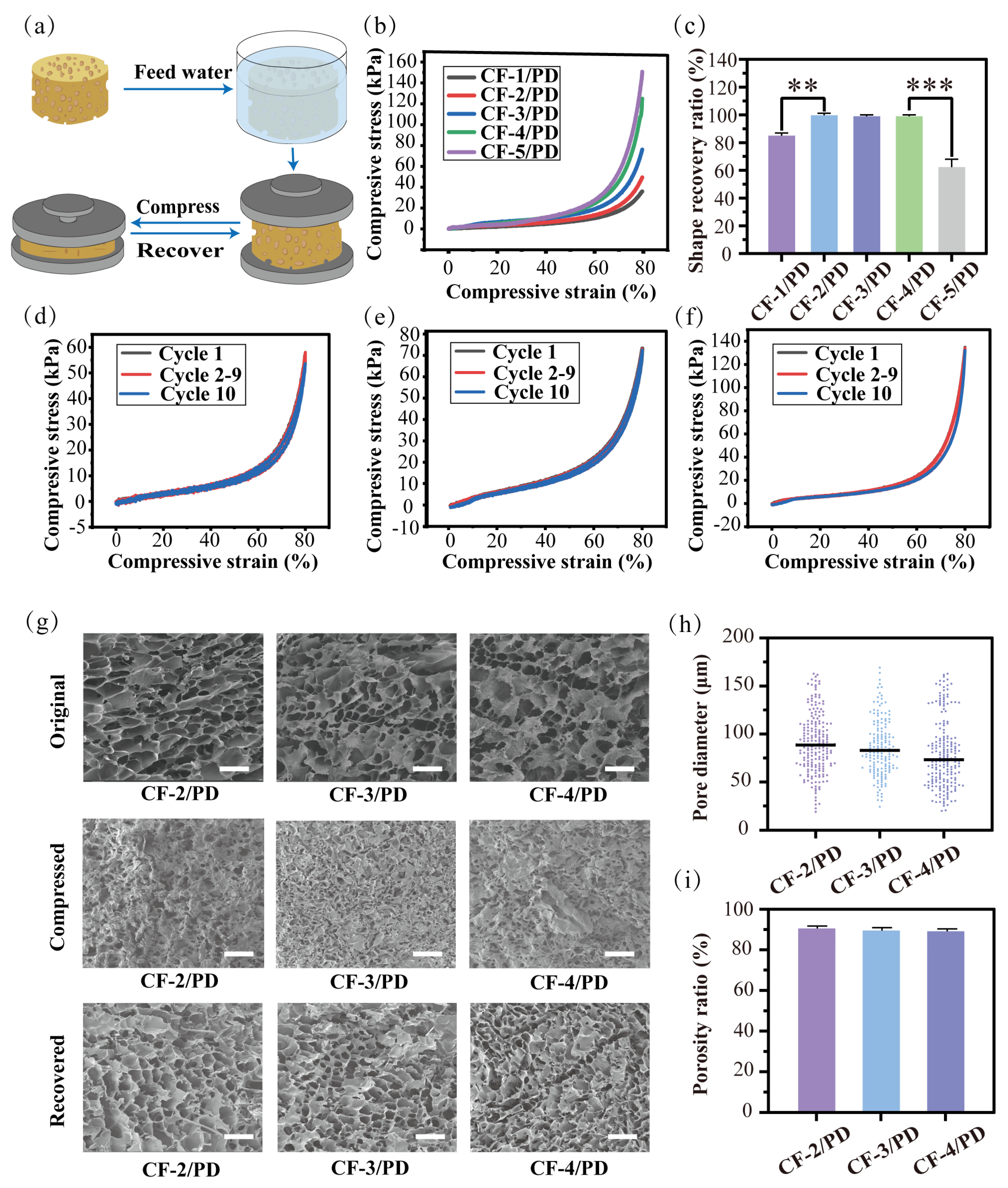
2.2. Shape Memory Properties of the Cryogels
2.3. Mechanical Property and Porosity of the Cryogels
2.4. Biocompatibility of the Cryogels
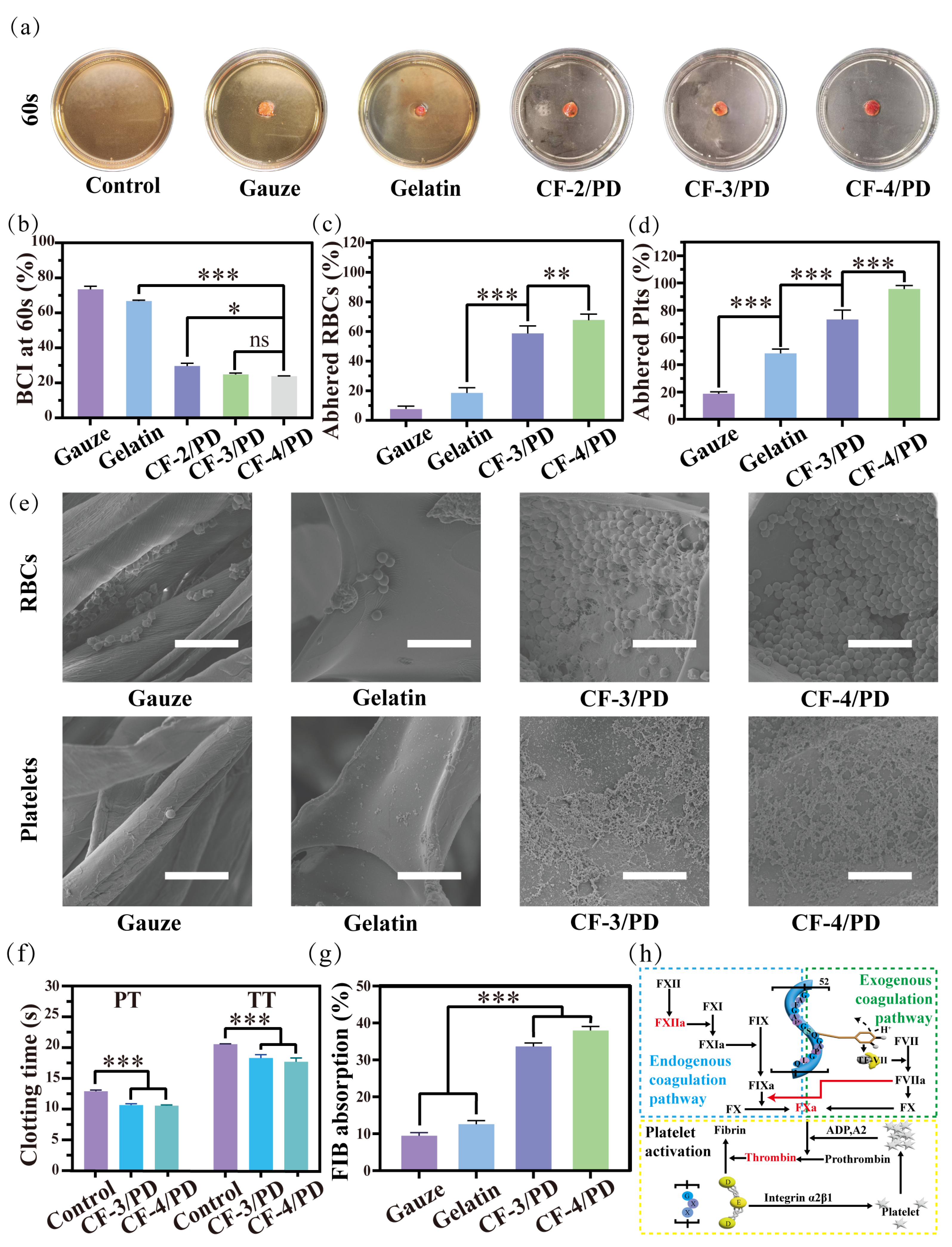
2.5. In Vitro Coagulation and Mechanisms of Hemostasis of the Cryogels
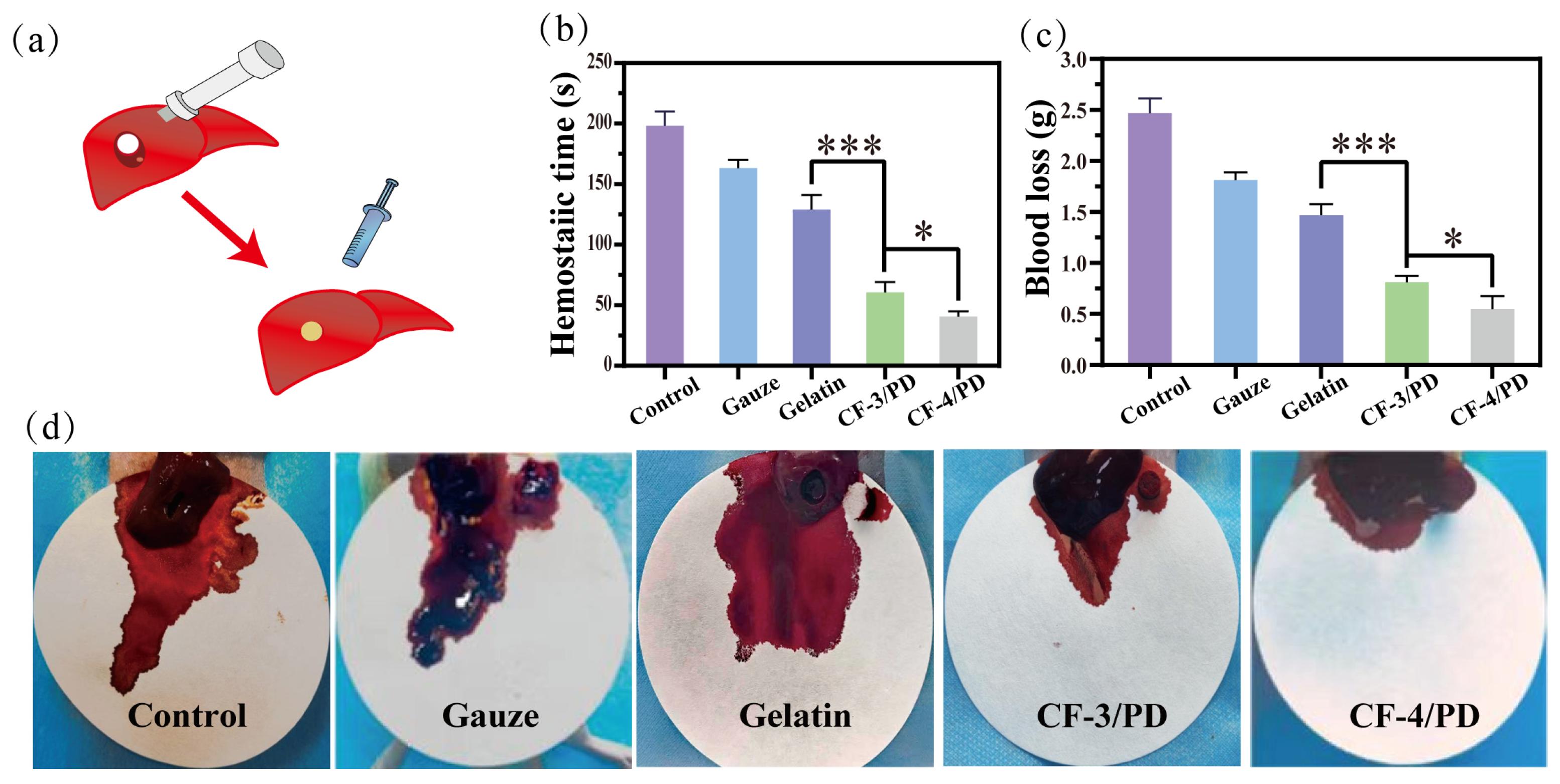
2.6. In Vivo Hemostasis of the Cryogels
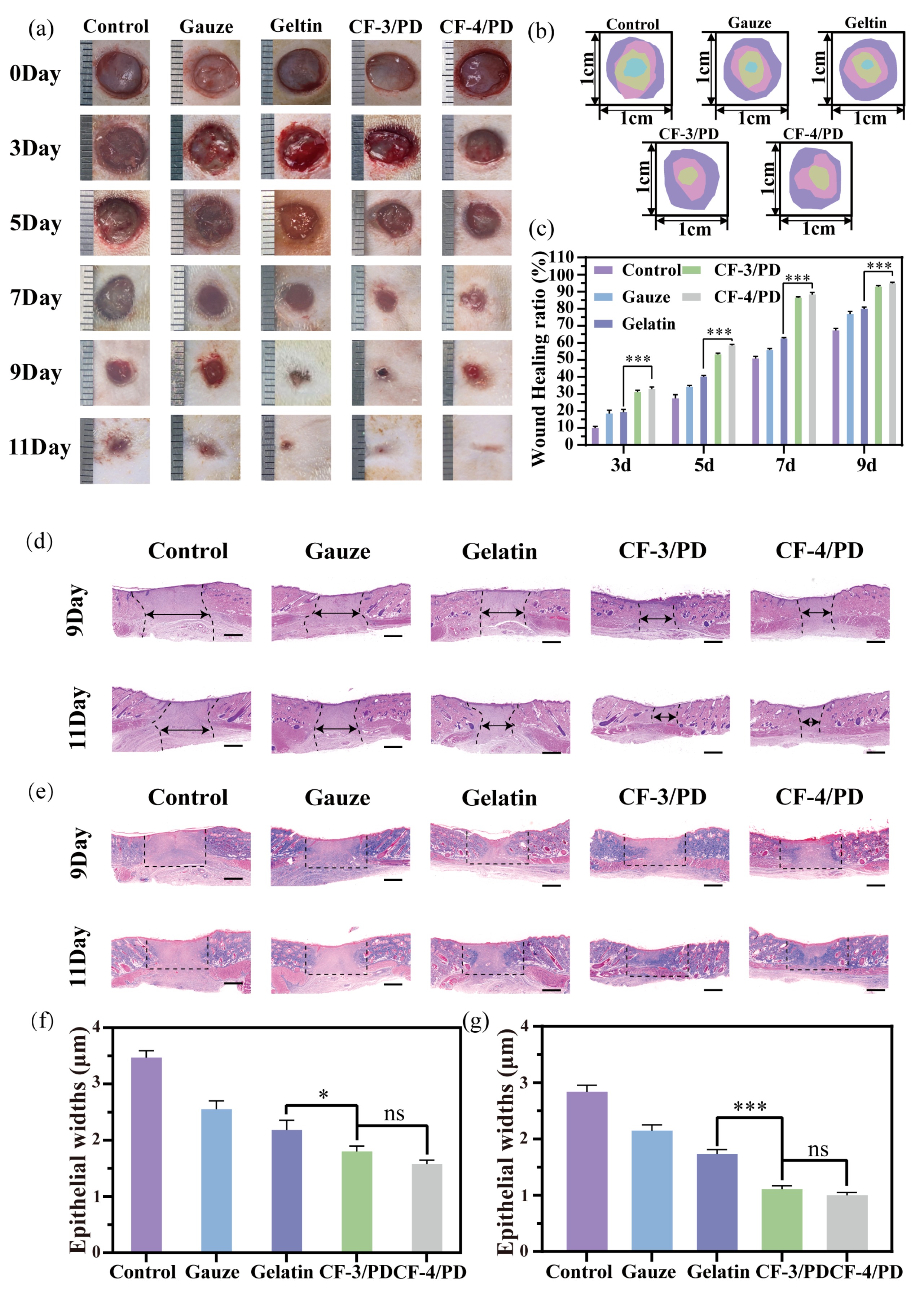
2.7. Wound Healing Study of the Cryogels
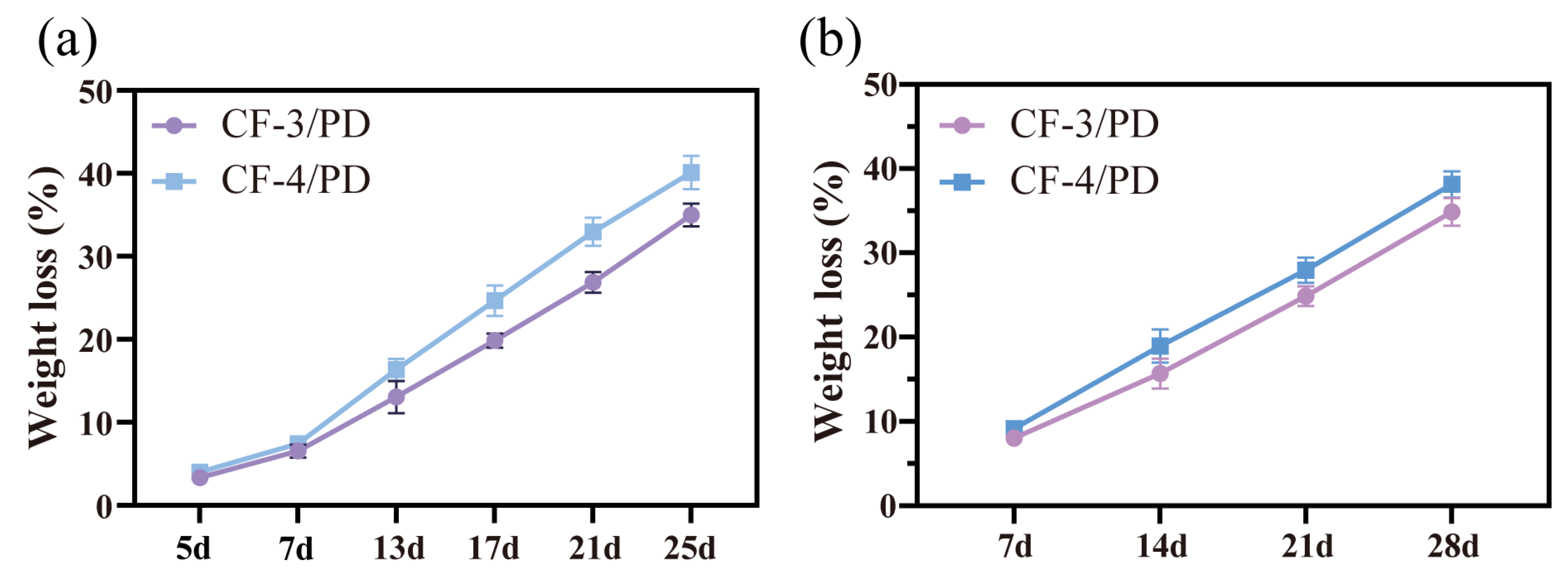
2.8. Degradability of the Cryogels
3. Conclusions
4. Materials and Methods
4.1. Materials
4.2. Synthesis of CFGMA and CF/PD
4.3. Characterization of CFGMA and CF/PD
4.4. Determination of Shape Recovery of Cryogels in Blood or Tissue Fluid
4.5. Characterization of the Physical Properties of Cryogels
4.6. Biocompatibility Assay of Cryogels
4.7. In Vitro Hemostatic Performance of Cryogels
4.8. Hemostatic Capacity and Hemostasis Mechanism Analysis of Cryogels
4.9. In Vivo Hemostasis of Cryogels
4.10. Wound Healing of Cryogels
4.11. Statistical Analysis
4.12. Statistics and Reproducibility
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chambers, J.A.; Seastedt, K.; Krell, R.; Caterson, E.; Levy, M.; Turner, N. “Stop the Bleed”: A U.S. Military Installation’s Model for Implementation of a Rapid Hemorrhage Control Program. Mil. Med. 2019, 184, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Katzenell, U.; Ash, N.; Tapia, A.L.; Campino, G.A.; Glassberg, E. Analysis of the Causes of Death of Casualties in Field Military Setting. Mil. Med. 2012, 177, 1065–1068. [Google Scholar] [CrossRef]
- Kauvar, D.S.; Lefering, R.; Wade, C.E. Impact of hemorrhage on trauma outcome: An overview of epidemiology, clinical presentations, and therapeutic considerations. J. Trauma 2006, 60, S3–S11. [Google Scholar] [CrossRef]
- Liu, C.; Li, Z.; Liu, L.; Qu, X.; Shi, Z.; Ma, Z.; Wang, X.; Huang, F. A thermal cross-linking approach to developing a reinforced elastic chitosan cryogel for hemostatic management of heavy bleeding. Carbohydr. Polym. 2024, 345, 122599. [Google Scholar] [CrossRef]
- Zhang, W.; Geng, X.; Qin, S.; Xie, Z.; Li, W.; Li, J. Research progress and application of chitosan dressings in hemostasis: A review. Int. J. Biol. Macromol. 2024, 282, 136421. [Google Scholar] [CrossRef]
- Raafat, A.I.; Ali, A.E.-H.; Hassan, A.A. Radiation development and hemostatic performance of innovative hydroxypropyl methyl cellulose-based sponge dressings for controlling severe hemorrhagic wounds. Int. J. Biol. Macromol. 2025, 292, 139132. [Google Scholar] [CrossRef]
- Thakur, P.; Anand Omar, R.; Talreja, N.; Chauhan, D.; Ashfaq, M. Waste-derived Ca and Zn-based bimetallic (Ca/Zn) nanorods encapsulated chitosan-based haemostatic dressing bandage: A step towards waste to bandages. J. Ind. Eng. Chem. 2025, 143, 327–338. [Google Scholar] [CrossRef]
- Rothwell, S.W.; Fudge, J.M.; Chen, W.-K.; Reid, T.J.; Krishnamurti, C. Addition of a propyl gallate-based procoagulant to a fibrin bandage improves hemostatic performance in a swine arterial bleeding model. Thromb. Res. 2002, 108, 335–340. [Google Scholar] [CrossRef]
- Ashfaq, M.; Wongpakham, T.; Talreja, N.; Chauhan, D.; Tharasanit, T.; Srituravanich, W. Synthesis of polymeric composite grafted with mineral particles/graphene oxide-based biomaterial: A promising robust hemostatic bandage. Mater. Today Commun. 2022, 33, 104786. [Google Scholar] [CrossRef]
- Fang, Y.; Chen, J.; Li, Q.; Chen, Q. Chitosan based Janus cryogel with anisotropic wettability, antibacterial activity, and rapid shape memory for effective hemostasis. Int. J. Biol. Macromol. 2024, 254, 127821. [Google Scholar] [CrossRef]
- Wen, J.; Weinhart, M.; Lai, B.; Kizhakkedathu, J.; Brooks, D.E. Reversible hemostatic properties of sulfabetaine/quaternary ammonium modified hyperbranched polyglycerol. Biomaterials 2016, 86, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, Y.; Min, Y.; Chen, J. Preparation of methacrylated hyaluronate/methacrylated collagen sponges with rapid shape recovery and orderly channel for fast blood absorption as hemostatic dressing. Int. J. Biol. Macromol. 2022, 222, 30–40. [Google Scholar] [CrossRef]
- Luo, Y.; Tao, F.; Wang, J.; Chai, Y.; Ren, C.; Wang, Y.; Wu, T.; Chen, Z. Development and evaluation of tilapia skin-derived gelatin, collagen, and acellular dermal matrix for potential use as hemostatic sponges. Int. J. Biol. Macromol. 2023, 253, 127014. [Google Scholar] [CrossRef]
- Yang, X.; Bi, S.; He, C.; Yuan, L.; Zhang, L.; Gu, J.; Yan, B.; He, J. Rapid Fluid-Induced-Expanding Chitosan-Derived Hemostatic Sponges with Excellent Antimicrobial and Antioxidant Properties for Incompressible Hemorrhage and Wound Healing. Biomacromolecules 2025, 26, 689–704. [Google Scholar] [CrossRef]
- Lei, D.; Zhao, J.; Zhu, C.; Jiang, M.; Ma, P.; Mi, Y.; Fan, D. Multifunct. Oxidized Dextran Cross-Linked Alkylat. Chitosan/Drug-Loaded Silver-Doped Mesoporous Bioact. Glass Cryogel Hemost. Noncompressible Wounds 2023, 9, 455. [Google Scholar]
- Zhu, Y.; Liu, H.; Qin, S.; Yang, C.; Lv, Q.; Wang, Z.; Wang, L. Antibacterial Sericin Cryogels Promote Hemostasis by Facilitating the Activation of Coagulation Pathway and Platelets. Adv. Healthc. Mater. 2022, 11, e2102717. [Google Scholar] [CrossRef]
- Ma, C.; Zhao, J.; Zhu, C.; Jiang, M.; Ma, P.; Mi, Y.; Fan, D. Oxidized dextran crosslinked polysaccharide/protein/polydopamine composite cryogels with multiple hemostatic efficacies for noncompressible hemorrhage and wound healing. Int. J. Biol. Macromol. 2022, 215, 675–690. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, X.; Zhang, Z.; Liang, Y.; Yin, Z.; Chen, B.; Bai, L.; Han, Y.; Guo, B. Degradable Gelatin-Based IPN Cryogel Hemostat for Rapidly Stopping Deep Noncompressible Hemorrhage and Simultaneously Improving Wound Healing. Chem. Mater. 2020, 32, 6595–6610. [Google Scholar] [CrossRef]
- Wang, T.; Yang, L.; Wang, G.; Han, L.; Chen, K.; Liu, P.; Xu, S.; Li, D.; Xie, Z.; Mo, X.; et al. Biocompatibility, hemostatic properties, and wound healing evaluation of tilapia skin collagen sponges. J. Bioact. Compat. Polym. 2020, 36, 44–58. [Google Scholar] [CrossRef]
- Zhang, X.; Cai, L.; Li, G. Bottom-up reconstitution design of a biomimetic atelocollagen microfibril for enhancing hemostatic, antibacterial, and biodegradable benefits. J. Mater. Chem. B 2024, 13, 2074–2090. [Google Scholar] [CrossRef]
- Wang, F.; Sun, J.; Shi, H.; Zhou, J.; Ma, X.; Song, X.; Su, X.; Liu, L. Multifunctionalized alginate/polydopamine cryogel for hemostasis, antibacteria and promotion of wound healing. Int. J. Biol. Macromol. 2023, 224, 1373–1381. [Google Scholar] [CrossRef]
- Yang, Q.; Zhao, Z.; Liu, R.; Yan, Z.; Yu, J.; Chen, L.; Li, X.; Cao, C.; Yao, F.; Zhang, H.; et al. Water-Triggered Self-Expanding Agarose/Chitosan-Gallate Hemostatic Sponge for Incompressible Wounds. ACS Appl. Polym. Mater. 2024, 6, 4114–4126. [Google Scholar] [CrossRef]
- Chunbo, W.; Yuqing, L.; Ying, H.; Meng, L.; Baolin, G. Porous photothermal antibacterial antioxidant dual–crosslinked cryogel based on hyaluronic acid/polydopamine for non-compressible hemostasis and infectious wound repair. J. Mater. Sci. Technol. 2022, 121, 207–219. [Google Scholar] [CrossRef]
- Zou, C.Y.; Han, C.; Xing, F.; Jiang, Y.L.; Xiong, M.; Li-Ling, J.; Xie, H.Q. Smart design in biopolymer-based hemostatic sponges: From hemostasis to multiple functions. Bioact. Mater. 2025, 45, 459–478. [Google Scholar] [CrossRef]
- Guo, X.; Ma, Y.; Wang, H.; Yin, H.; Shi, X.; Chen, Y.; Gao, G.; Sun, L.; Wang, J.; Wang, Y.; et al. Status and developmental trends in recombinant collagen preparation technology. Regen. Biomater. 2024, 11, rbad106. [Google Scholar] [CrossRef]
- Sowbhagya, R.; Muktha, H.; Ramakrishnaiah, T.N.; Surendra, A.S.; Sushma, S.M.; Tejaswini, C.; Roopini, K.; Rajashekara, S. Collagen as the extracellular matrix biomaterials in the arena of medical sciences. Tissue Cell 2024, 90, 102497. [Google Scholar] [CrossRef]
- Yang, X.; Yao, L.; Sun, X.; Wang, L.; Xiao, J. Low-temperature DLP 3D printing of low-concentration collagen methacryloyl for the fabrication of durable and bioactive personalized scaffolds. Chem. Eng. J. 2024, 497, 155650. [Google Scholar] [CrossRef]
- Wang, Q.; Yan, H.; Zhang, J.; Tian, B.; Li, W.; Xiao, J. Agarose-collagen composite microsphere implants: A biocompatible and robust approach for skin tissue regeneration. Int. J. Biol. Macromol. 2024, 277, 134510. [Google Scholar] [CrossRef]
- Chen, H.; Wang, Y.; Huang, Z.; Xiao, T.; Guo, T.; Wang, Y.; Wu, C.; Ren, Z. Elastic and recoverable sponges based on collagen/yeast β-glucan for quick hemostasis. Int. J. Biol. Macromol. 2024, 282, 137095. [Google Scholar] [CrossRef]
- Li, X.; Xu, Y.; Zhou, Z.; Tang, M.; Cui, J.; Han, W.; Li, J.; Dai, J.; Ren, X.; Jiang, H.; et al. Self-Cross-Linked Collagen Sponge from the Alosa sapidissima Scale for Hemostasis and Wound Healing Applications. Biomacromolecules 2025, 26, 405–414. [Google Scholar] [CrossRef]
- He, Y.; Wang, C.; Wang, C.; Xiao, Y.; Lin, W. An Overview on Collagen and Gelatin-Based Cryogels: Fabrication, Classification, Properties and Biomedical Applications. Polymers 2021, 13, 2299. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, L.; Gallo, N.; Natali, M.L.; Campa, L.; Lunetti, P.; Madaghiele, M.; Blasi, F.S.; Corallo, A.; Capobianco, L.; Sannino, A. Marine collagen and its derivatives: Versatile and sustainable bio-resources for healthcare. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 113, 110963. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Fu, H.; Xu, Y.; Chen, T.; Liu, Z.; Liu, X.; Bing, W. Study on hemostatic and antibacterial properties of modified silicone rubber sponge. React. Funct. Polym. 2024, 203, 106020. [Google Scholar] [CrossRef]
- Thomas, D.P. Effect of Catecholamines on Platelet Aggregation caused by Thrombin. Nature 1967, 215, 298–299. [Google Scholar] [CrossRef]
- Puertas-Bartolomé, M.; Fernández-Gutiérrez, M.; García-Fernández, L.; Vázquez-Lasa, B.; San Román, J. Biocompatible and bioadhesive low molecular weight polymers containing long-arm catechol-functionalized methacrylate. Eur. Polym. J. 2018, 98, 47–55. [Google Scholar] [CrossRef]
- Yang, Y.; Liang, Y.; Chen, J.; Duan, X.; Guo, B. Mussel-inspired adhesive antioxidant antibacterial hemostatic composite hydrogel wound dressing via photo-polymerization for infected skin wound healing. Bioact. Mater. 2021, 8, 341–354. [Google Scholar] [CrossRef]
- Aarthy, M.; Hemalatha, T.; Suryalakshmi, P.; Vinoth, V.; Mercyjayapriya, J.; Shanmugam, G.; Ayyadurai, N. Biomimetic design of fibril-forming non-immunogenic collagen like proteins for tissue engineering. Int. J. Biol. Macromol. 2024, 266, 130999. [Google Scholar] [CrossRef]
- Jie, I.W.K.; Lee, K.W.A.; Yoon, S.E.; Song, J.K.; Chan, L.K.W.; Lee, C.H.; Jeong, E.; Kim, J.-H.; Yi, K.-H. Advancements in Clinical Utilization of Recombinant Human Collagen: An Extensive Review. Life 2025, 15, 582. [Google Scholar] [CrossRef]
- Jianlong, W.; Shuting, Z. Chitosan-based materials: Preparation, modification and application. J. Clean. Prod. 2022, 355, 131825. [Google Scholar] [CrossRef]
- Liu, Y.-M.; Cui, X.; Hao, C.-M.; Tao, F.-R.; Li, J.-Y. Modified gelatin with quaternary ammonium salts containing epoxide groups. Chin. Chem. Lett. 2014, 25, 1193–1197. [Google Scholar] [CrossRef]
- Kavitha Sankar, P.C.; Rajmohan, G.; Rosemary, M.J. Physico-chemical characterisation and biological evaluation of freeze dried chitosan sponge for wound care. Mater. Lett. 2017, 208, 130–132. [Google Scholar] [CrossRef]
- Budkov, Y.A.; Kolesnikov, A.L. Models of the Conformational Behavior of Polymers in Mixed Solvents. Polym. Sci. Ser. C 2018, 60, 148–159. [Google Scholar] [CrossRef]
- Strachota, B.; Matějka, L.; Sikora, A.; Spěváček, J.; Konefał, R.; Zhigunov, A.; Šlouf, M. Insight into the cryopolymerization to form a poly(N-isopropylacrylamide)/clay macroporous gel: Structure and phase evolution†. Soft Matter 2016, 13, 1244–1256. [Google Scholar] [CrossRef] [PubMed]
- Grenier, J.; Duval, H.; Barou, F.; Lv, P.; David, B.; Letourneur, D. Mechanisms of pore formation in hydrogel scaffolds textured by freeze-drying. Acta Biomater. 2019, 94, 195–203. [Google Scholar] [CrossRef]
- Sun, H.; Yang, X.; Zhang, Y.; Cheng, X.; Xu, Y.; Bai, Y.; Shao, L. Segregation-induced in situ hydrophilic modification of poly (vinylidene fluoride) ultrafiltration membranes via sticky poly (ethylene glycol) blending. J. Membr. Sci. 2018, 563, 22–30. [Google Scholar] [CrossRef]
- Lee, W.; Lee, J.U.; Byun, J.-H. Catecholamine polymers as surface modifiers for enhancing interfacial strength of fiber-reinforced composites. Compos. Sci. Technol. 2015, 110, 53–61. [Google Scholar] [CrossRef]
- Lu, S.; Bian, S.; Jia, Y.; Guo, Y.; Xiao, H.; Zhang, M.; Liu, K.; Huang, L.; Chen, L.; Ni, Y.; et al. Catechol-functionalised dialdehyde cellulose-containing hydrogels with tissue adhesion, sensing and haemostatic properties for wound healing. Cellulose 2024, 31, 2355–2377. [Google Scholar] [CrossRef]
- Xiang, D.; Wang, K.; Wang, F.; Li, Y.; Hou, Y.; Hu, K.; Xu, Y. Coagulopathy-independent injectable catechol-functionalized chitosan shape-memory material to treat non-compressible hemorrhage. Carbohydr. Polym. 2024, 346, 122648. [Google Scholar] [CrossRef]
- A, W.; Du, F.; He, Y.; Wu, B.; Liu, F.; Liu, Y.; Zheng, W.; Li, G.; Wang, X. Graphene oxide reinforced hemostasis of gelatin sponge in noncompressible hemorrhage via synergistic effects. Colloids Surf. B Biointerfaces 2022, 220, 112891. [Google Scholar] [CrossRef]
- Xu, G.; Cao, S.; Dong, Y.; Huang, Z.; Chu, C. Strength enhanced expandable polyvinyl alcohol/chitosan cryogel for non-compressible hemostasis. Int. J. Biol. Macromol. 2024, 285, 138191. [Google Scholar] [CrossRef]
- Nepal, A.; Tran, H.D.N.; Nguyen, N.-T.; Ta, H.T. Advances in haemostatic sponges: Characteristics and the underlying mechanisms for rapid haemostasis. Bioact. Mater. 2023, 27, 231–256. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, X.; Wang, C.; Chen, J.; Liang, Y.; Li, Z.; Han, Y.; Guo, B. High-strength anti-bacterial composite cryogel for lethal noncompressible hemorrhage hemostasis: Synergistic physical hemostasis and chemical hemostasis. Chem. Eng. J. 2022, 427, 131977. [Google Scholar] [CrossRef]
- Zhao, X.; Liang, Y.; Guo, B.; Yin, Z.; Zhu, D.; Han, Y. Injectable dry cryogels with excellent blood-sucking expansion and blood clotting to cease hemorrhage for lethal deep-wounds, coagulopathy and tissue regeneration. Chem. Eng. J. 2020, 403, 126329. [Google Scholar] [CrossRef]
- Liu, Y.; Xu, K.; Chang, Q.; Darabi, M.A.; Lin, B.; Zhong, W.; Xing, M. Highly Flexible and Resilient Elastin Hybrid Cryogels with Shape Memory, Injectability, Conductivity, and Magnetic Responsive Properties. Adv. Mater. 2016, 28, 7758–7767. [Google Scholar] [CrossRef]
- Li, M.; Zhang, Z.; Liang, Y.; He, J.; Guo, B. Multifunctional Tissue-Adhesive Cryogel Wound Dressing for Rapid Nonpressing Surface Hemorrhage and Wound Repair. ACS Appl. Mater. Interfaces 2020, 12, 35856–35872. [Google Scholar] [CrossRef]
- Jones, D.W. What Is a Normal Blood Pressure? JAMA Cardiol. 2020, 5, 1018–1019. [Google Scholar] [CrossRef]
- Lüscher, T.F. What is a normal blood pressure? Eur. Heart J. 2018, 39, 2233–2240. [Google Scholar] [CrossRef]
- Nguyen, T.H.M.; Abueva, C.; Ho, H.V.; Lee, S.-Y.; Lee, B.-T. In vitro and in vivo acute response towards injectable thermosensitive chitosan/TEMPO-oxidized cellulose nanofiber hydrogel. Carbohydr. Polym. 2017, 180, 246–255. [Google Scholar] [CrossRef]
- Qiu, H.; Deng, X.; Zhang, D.; Zhang, H.; Li, W.; Tao, X.; Ye, D.; Yan, G.; Tang, R.; Yang, X. Antibacterial Chitin-Based Sponges with Enhanced Water Absorbency and Mechanical Properties for Hemostasis and Wound Healing. Langmuir 2025, 41, 7546–7558. [Google Scholar] [CrossRef]
- Chen, Z.; Fan, D.; Shang, L. Exploring the potential of the recombinant human collagens for biomedical and clinical applications: A short review. Biomed. Mater. 2020, 16, 012001. [Google Scholar] [CrossRef]
- Liu, C.-C.; Leclair, P.; Pedari, F.; Mahdis, M.; Sly, L.; Reid, G.S.D.; Lim, C.J. Integrin Activity Reduces Immunogenic Cell Death By Inhibiting Cell Surface Presentation of ERp57 and Calreticulin. Blood 2018, 132, 3927. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, W.; Gan, B.; Wang, Y.; Fan, Z.; Yang, Y.; Xiong, X.; Li, Y.; Chen, H.; Yu, M.; et al. Non-cross-linked collagen type I microfibers for improved hemostasis and wound healing. J. Mater. Sci. 2022, 57, 13570–13585. [Google Scholar] [CrossRef]
- Huang, J.; Zheng, Y.; Ma, W.; Han, Y.; Xue, J.; Huan, Z.; Wu, C.; Zhu, Y. SiO2-based inorganic nanofiber aerogel with rapid hemostasis and liver wound healing functions. Acta Biomater. 2025, 194, 483–497. [Google Scholar] [CrossRef]
- Qi, L.; Mu, L.; Guo, X.; Liu, A.; Chen, C.; Ye, Q.; Zhong, Z.; Shi, X. Fast Expandable Chitosan-Fibers Cryogel from Ambient Drying for Noncompressible Bleeding Control and In Situ Tissue Regeneration. Adv. Funct. Mater. 2023, 33, 2212231. [Google Scholar] [CrossRef]
- Sun, L.; Yin, H.; Liu, M.; Xu, G.; Zhou, X.; Ge, P.; Yang, H.; Mao, Y. Impaired albumin function: A novel potential indicator for liver function damage? Ann. Med. 2019, 51, 333–344. [Google Scholar] [CrossRef]
- Cvirn, G.; Kutschera, J.; Wagner, T.; Ferstl, U.; Vrecko, K.; Hallstrom, S.; Juergens, G.; Koestenberger, M. Collagen/Endogenous Thrombin-Induced Platelet Aggregation in Cord versus Adult Whole Blood. Neonatology 2009, 95, 187–192. [Google Scholar] [CrossRef]
- Fang, Y.; Zhang, L.; Chen, Y.; Wu, S.; Weng, Y.; Liu, H. Polysaccharides based rapid self-crosslinking and wet tissue adhesive hemostatic powders for effective hemostasis. Carbohydr. Polym. 2023, 312, 120819. [Google Scholar] [CrossRef]
- Horbett, T.A. Fibrinogen adsorption to biomaterials. J. Biomed. Mater. Res. Part A 2018, 106, 2777–2788. [Google Scholar] [CrossRef]
- Risman, R.A.; Belcher, H.A.; Ramanujam, R.K.; Weisel, J.W.; Hudson, N.E.; Tutwiler, V. Comprehensive Analysis of the Role of Fibrinogen and Thrombin in Clot Formation and Structure for Plasma and Purified Fibrinogen. Biomolecules 2024, 14, 230. [Google Scholar] [CrossRef]
- Hathcock, J.J.; Rusinova, E.; Nemerson, Y. Factor Xa Control of the Extrinsic Pathway: A Different View of the Regulation of Coagulation. Blood 2006, 108, 546. [Google Scholar] [CrossRef]
- Misenheimer, T.M.; Kumfer, K.T.; Bates, B.E.; Nettesheim, E.R.; Schwartz, B.S. A candidate activation pathway for coagulation factor VII. Biochem. J. 2019, 476, 2909–2926. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Sun, Z.; Chen, L.; Zhang, X.; Guo, X.; Li, G. Co-assembled biomimetic fibrils from collagen and chitosan for performance-enhancing hemostatic dressing. Biomater. Sci. 2024, 13, 236–249. [Google Scholar] [CrossRef] [PubMed]
- Lv, C.; Zhou, X.; Wang, P.; Li, J.; Wu, Z.; Jiao, Z.; Guo, M.; Wang, Z.; Wang, Y.; Wang, L.; et al. Biodegradable alginate-based sponge with antibacterial and shape memory properties for penetrating wound hemostasis. Compos. Part B Eng. 2022, 247, 110263. [Google Scholar] [CrossRef]
- Lv, S.; Cai, M.; Leng, F.; Jiang, X. Biodegradable carboxymethyl chitin-based hemostatic sponges with high strength and shape memory for non-compressible hemorrhage. Carbohydr. Polym. 2022, 288, 119369. [Google Scholar] [CrossRef]
- Hixon, K.R.; Lu, T.; Sell, S.A. A comprehensive review of cryogels and their roles in tissue engineering applications. Acta Biomater. 2017, 62, 29–41. [Google Scholar] [CrossRef]
- Gil-Cifuentes, L.; Jiménez, R.A.; Fontanilla, M.R. Evaluation of collagen type I scaffolds including gelatin-collagen microparticles and Aloe vera in a model of full-thickness skin wound. Drug Deliv. Transl. Res. 2018, 9, 25–36. [Google Scholar] [CrossRef]
- Hwang, J.; Kiick, K.L.; Sullivan, M.O. Modified hyaluronic acid-collagen matrices trigger efficient gene transfer and prohealing behavior in fibroblasts for improved wound repair. Acta Biomater. 2022, 150, 138–153. [Google Scholar] [CrossRef]
- Ding, C.; Yang, Q.; Tian, M.; Guo, C.; Deng, F.; Dang, Y.; Zhang, M. Novel collagen-based hydrogels with injectable, self-healing, wound-healing properties via a dynamic crosslinking interaction. Polym. Int. 2020, 69, 858–866. [Google Scholar] [CrossRef]
- Kong, X.; Fu, J.; Shao, K.; Wang, L.; Lan, X.; Shi, J. Biomimetic hydrogel for rapid and scar-free healing of skin wounds inspired by the healing process of oral mucosa. Acta Biomater. 2019, 100, 255–269. [Google Scholar] [CrossRef]
- Bourgot, I.; Primac, I.; Louis, T.; Noël, A.; Maquoi, E. Reciprocal Interplay Between Fibrillar Collagens and Collagen-Binding Integrins: Implications in Cancer Progression and Metastasis. Front. Oncol. 2020, 10, 1488. [Google Scholar] [CrossRef]
- McAndrews, K.M.; Miyake, T.; Ehsanipour, E.A.; Kelly, P.J.; Becker, L.M.; McGrail, D.J.; Sugimoto, H.; LeBleu, V.S.; Ge, Y.; Kalluri, R. Dermal αSMA+ myofibroblasts orchestrate skin wound repair via β1 integrin and independent of type I collagen production. EMBO J. 2022, 41, e109470. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, K.; Togo, S.; Okamoto, R.; Idiris, A.; Kumagai, H.; Miyagi, Y. Collective cancer cell invasion in contact with fibroblasts through integrin-α5β1/fibronectin interaction in collagen matrix. Cancer Sci. 2020, 111, 4381–4392. [Google Scholar] [CrossRef] [PubMed]
- Eigel, D.; Werner, C.; Newland, B. Cryogel biomaterials for neuroscience applications. Neurochem. Int. 2021, 147, 105012. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.O.; Williams, L.; Boam, T.; Kalmet, M.; Oguike, C.; Hatton, F.L. Cryogels: Recent applications in 3D-bioprinting, injectable cryogels, drug delivery, and wound healing. Beilstein J. Org. Chem. 2021, 17, 2553–2569. [Google Scholar] [CrossRef]
- Razavi, M.; Qiao, Y.; Thakor, A.S. Three-dimensional cryogels for biomedical applications. J. Biomed. Mater. Res. Part A 2019, 107, 2736–2755. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, J.; Jin, Y.; Yin, M. Gelatin methacrylate based liquid dressing with antibacterial and hemostasis properties. Colloids Surf. A Physicochem. Eng. Asp. 2024, 689, 133749. [Google Scholar] [CrossRef]
- Zhang, W.; Li, M.; Chen, J.; Chen, Y.; Liu, C.; Wu, X. A Review of Modified Gelatin: Physicochemical Properties, Modification Methods, and Applications in the Food Field. J. Agric. Food Chem. 2024, 72, 20705–20721. [Google Scholar] [CrossRef]
- Salmanipour, S.; Rezaie, A.; Alipour, N.; Ghahremani-Nasab, M.; Zakerhamidi, M.S.; Akbari-Gharalari, N.; Mehdipour, A.; Salehi, R.; Jarolmasjed, S. Development of Polyphosphate/Nanokaolin-Modified Alginate Sponge by Gas-Foaming and Plasma Glow Discharge Methods for Ultrarapid Hemostasis in Noncompressible Bleeding. ACS Appl. Mater. Interfaces 2024, 16, 34684–34704. [Google Scholar] [CrossRef]
- Yao, L.; Gao, H.; Lin, Z.; Dai, Q.; Zhu, S.; Li, S.; Liu, C.; Feng, Q.; Li, Q.; Wang, G.; et al. A shape memory and antibacterial cryogel with rapid hemostasis for noncompressible hemorrhage and wound healing. Chem. Eng. J. 2021, 428, 131005. [Google Scholar] [CrossRef]
- Sang, F.; Pan, L.; Ji, Z.; Zhang, B.; Meng, Z.; Cao, L.; Zhang, J.; Li, X.; Yang, X.; Shi, C. Polydopamine functionalized polyurethane shape memory sponge with controllable expansion performance triggered by near-infrared light for incompressible hemorrhage control. Colloids Surf. B Biointerfaces 2023, 232, 113590. [Google Scholar] [CrossRef]
- Sneha Letha, S.; Shukla, S.K.; Haridas, N.; Smitha, R.P.; Sidharth Mohan, M.; Archana, V.; Rosemary, M.J. In vitro and In vivo Biocompatibility Evaluation of Freeze Dried Gelatin Haemostat. Fibers Polym. 2021, 22, 621–628. [Google Scholar] [CrossRef]
- Takizawa, K.; Okazaki, D.; Takegawa, Y.; Koga, Y.; Sagata, M.; Michishita, K.; Shinya, N. Evaluation of the hemostatic effect of a combination of hemostatic agents and fibrin glue in a rabbit venous hemorrhage model. BMC Neurol. 2021, 21, 270. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cryogel | CFGMA (%, w/v) | PEGDA (%, v/v) | DMA (%, w/v) |
|---|---|---|---|
| CF-1/PD | 1.00 | 4.0 | 0.50 |
| CF-2/PD | 1.25 | 4.0 | 0.50 |
| CF-3/PD | 1.50 | 4.0 | 0.50 |
| CF-4/PD | 1.75 | 4.0 | 0.50 |
| CF-5/PD | 2.00 | 4.0 | 0.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Yao, T.; Xu, R.; Ma, P.; Zhao, J.; Mi, Y. Biodegradable and Mechanically Resilient Recombinant Collagen/PEG/Catechol Cryogel Hemostat for Deep Non-Compressible Hemorrhage and Wound Healing. Gels 2025, 11, 445. https://doi.org/10.3390/gels11060445
Zhang Y, Yao T, Xu R, Ma P, Zhao J, Mi Y. Biodegradable and Mechanically Resilient Recombinant Collagen/PEG/Catechol Cryogel Hemostat for Deep Non-Compressible Hemorrhage and Wound Healing. Gels. 2025; 11(6):445. https://doi.org/10.3390/gels11060445
Chicago/Turabian StyleZhang, Yuanzhe, Tianyu Yao, Ru Xu, Pei Ma, Jing Zhao, and Yu Mi. 2025. "Biodegradable and Mechanically Resilient Recombinant Collagen/PEG/Catechol Cryogel Hemostat for Deep Non-Compressible Hemorrhage and Wound Healing" Gels 11, no. 6: 445. https://doi.org/10.3390/gels11060445
APA StyleZhang, Y., Yao, T., Xu, R., Ma, P., Zhao, J., & Mi, Y. (2025). Biodegradable and Mechanically Resilient Recombinant Collagen/PEG/Catechol Cryogel Hemostat for Deep Non-Compressible Hemorrhage and Wound Healing. Gels, 11(6), 445. https://doi.org/10.3390/gels11060445