
Periprosthetic Joint Infections Caused by Candida Species—A Single-Center Experience and Systematic Review of the Literature

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Series
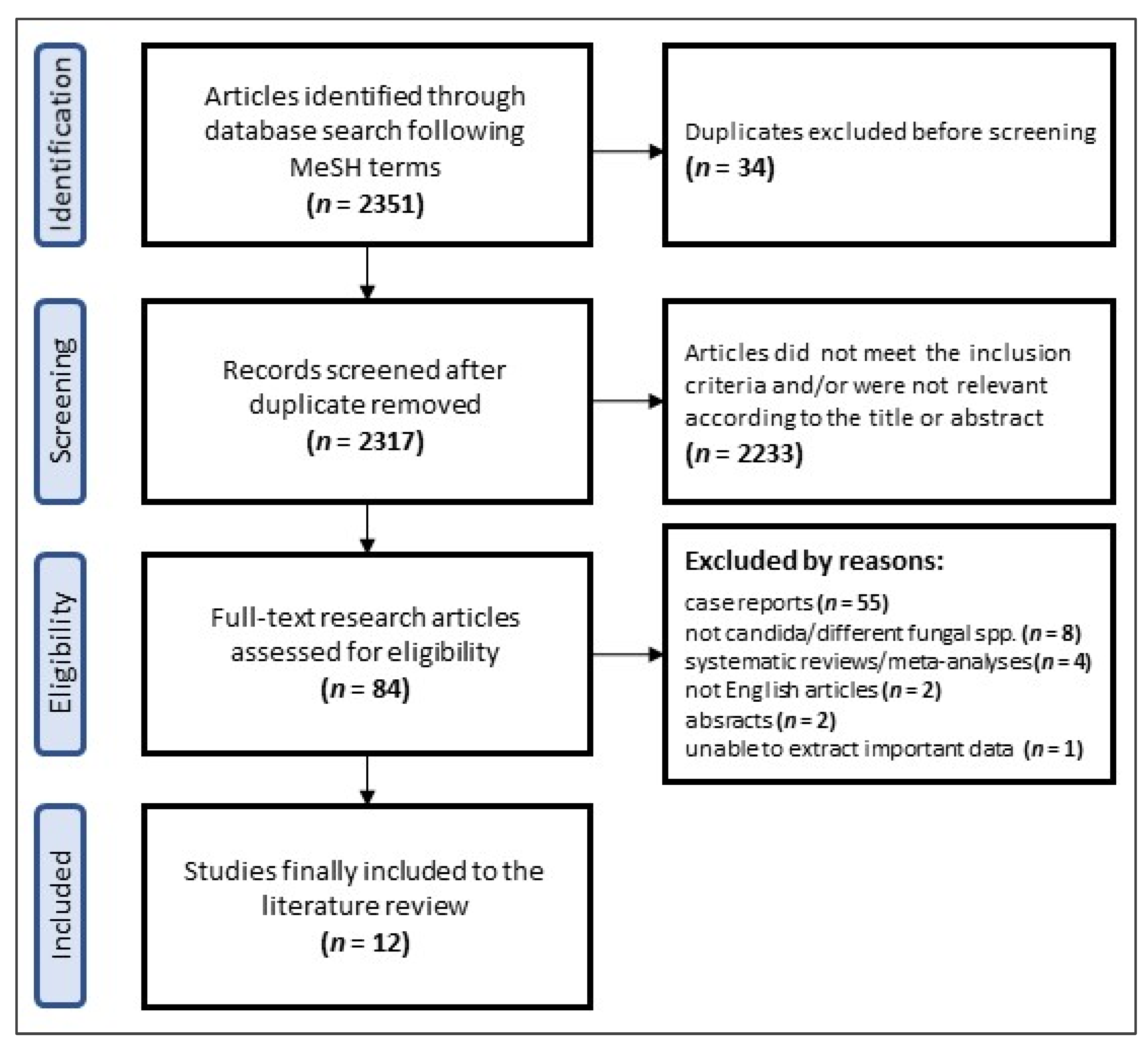
2.2. Literature Review
2.3. Statistical Analysis

3. Results
3.1. Case Series
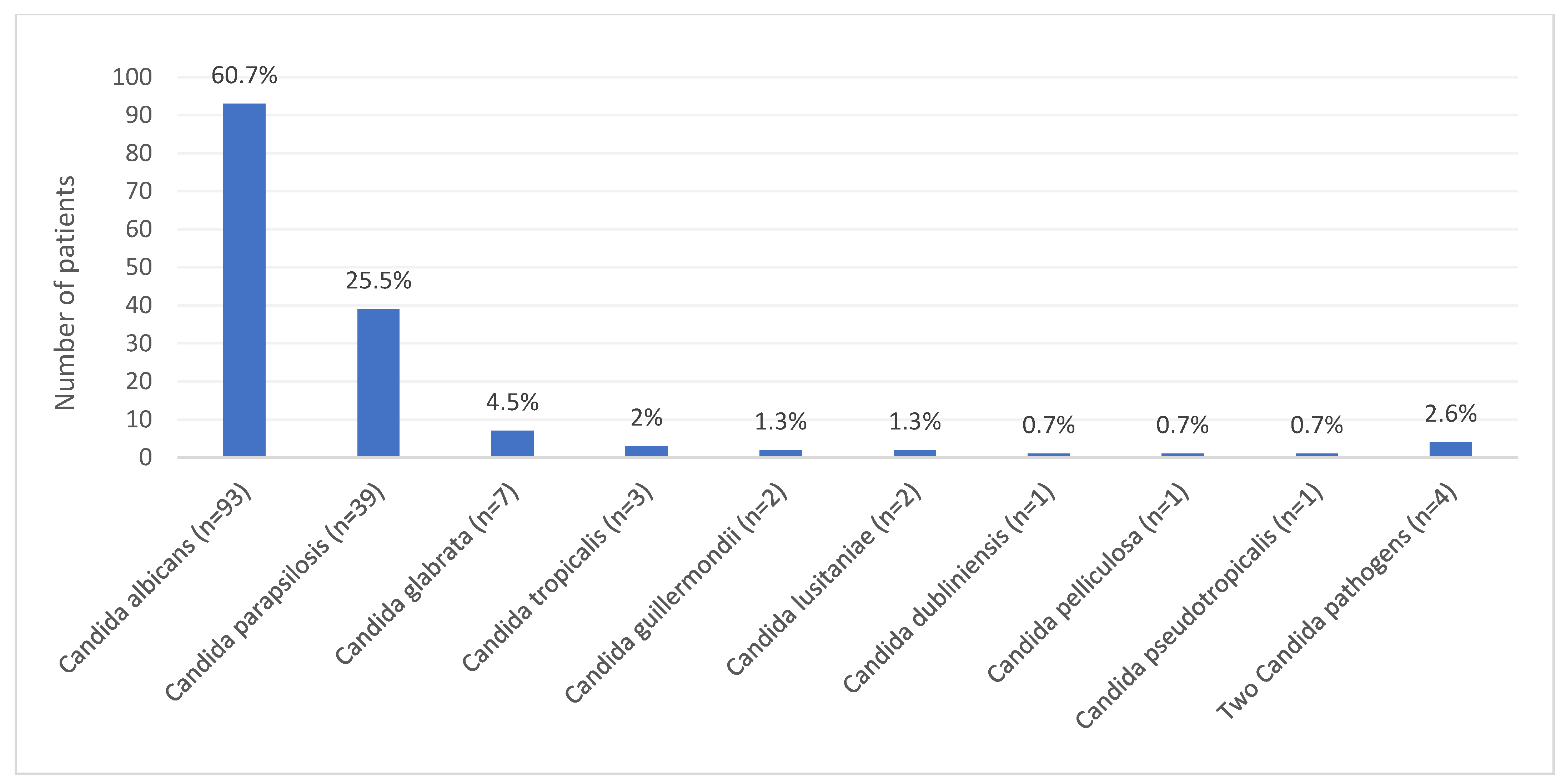
3.2. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, T.S.; Petis, S.M.; Osmon, D.R.; Mabry, T.M.; Berry, D.J.; Hanssen, A.D.; Abdel, M.P. Periprosthetic Joint Infection with Fungal Pathogens. J. Arthroplast. 2018, 33, 2605–2612. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.; Vrebos, M.; Boogaerts, M. Assessing risk factors for systemic fungal infections. Eur. J. Cancer Care 2001, 10, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-P.; Chen, Y.-Y.; Hsu, H.-S.; Wang, F.-D.; Chen, L.-Y.; Fung, C.-P. A risk factor analysis of healthcare-associated fungal infections in an intensive care unit: A retrospective cohort study. BMC Infect. Dis. 2013, 13, 10. [Google Scholar] [CrossRef] [Green Version]
- Kelesidis, T.; Tsiodras, S. Candida albicans prosthetic hip infection in elderly patients: Is fluconazole monotherapy an option? Scand. J. Infect. Dis. 2010, 42, 12–21. [Google Scholar] [CrossRef]
- Bosshard, P.P. Incubation of fungal cultures: How long is long enough? Mycoses 2011, 54, e539–e545. [Google Scholar] [CrossRef] [PubMed]
- Azzam, K.; Parvizi, J.; Jungkind, D.; Hanssen, A.; Fehring, T.; Springer, B.; Bozic, K.; Della Valle, C.; Pulido, L.; Barrack, R. Microbiological, Clinical, and Surgical Features of Fungal Prosthetic Joint Infections: A Multi-Institutional Experience. J. Bone Jt. Surg. 2009, 91 (Suppl. S6), 142–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, C.E.; Della Valle, C.J.; Rex, J.C.; Traven, S.A.; Durante, E.C. Fungal Periprosthetic Joint Infection: A Review of Demographics and Management. J. Arthroplast. 2021, 36, 1758–1764. [Google Scholar] [CrossRef] [PubMed]
- Escolà-Vergé, L.; Rodríguez-Pardo, D.; Lora-Tamayo, J.; Morata, L.; Murillo, O.; Vilchez, H.; Sorli, L.; Carrión, L.G.; Barbero, J.M.; Palomino-Nicás, J.; et al. Candida periprosthetic joint infection: A rare and difficult-to-treat infection. J. Infect. 2018, 77, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenny, J.Y.; Goukodadja, O.; Boeri, C.; Gaudias, J. May one-stage exchange for Candida albicans peri-prosthetic infection be successful? Orthop. Traumatol. Surg. Res. 2016, 102, 127–129. [Google Scholar] [CrossRef]
- Wang, Q.J.; Shen, H.; Zhang, X.-L.; Jiang, Y.; Wang, Q.; Chen, Y.S.; Shao, J.-J. Staged reimplantation for the treatment of fungal peri-prosthetic joint infection following primary total knee arthro-plasty. Orthop. Traumatol. Surg. Res. 2015, 101, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Koutserimpas, C.; Samonis, G.; Velivassakis, E.; Iliopoulou-Kosmadaki, S.; Kontakis, G.; Kofteridis, D.P. Candida glabrata prosthetic joint infection, successfully treated with anidulafungin: A case report and review of the literature. Mycoses 2017, 61, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-K.; Lee, D.-Y.; Kang, D.-W.; Ro, D.-H.; Lee, M.C.; Han, H.-S. Efficacy of antifungal-impregnated cement spacer against chronic fungal periprosthetic joint infections after total knee arthroplasty. Knee 2018, 25, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Riaz, T.; Tande, A.J.; Steed, L.L.; Demos, H.A.; Salgado, C.D.; Osmon, D.R.; Marculescu, C.E. Risk Factors for Fungal Prosthetic Joint Infection. J. Bone Jt. Infect. 2020, 5, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Hwang, B.-H.; Yoon, J.-Y.; Nam, C.-H.; Jung, K.-A.; Lee, S.-C.; Han, C.-D.; Moon, S.-H. Fungal peri-prosthetic joint infection after primary total knee replacement. J. Bone Jt. Surg. Br. 2012, 94, 656–659. [Google Scholar] [CrossRef]
- Escola-Verge, L.; Rodríguez-Pardo, D.; Corona, P.S.; Pigrau, C. Candida Periprosthetic Joint Infection: Is It Curable? Antibiotics 2021, 10, 458. [Google Scholar] [CrossRef] [PubMed]
- Jakobs, O.; Schoof, B.; Klatte, T.O.; Schmidl, S.; Fensky, F.; Guenther, D.; Frommelt, L.; Gehrke, T.; Gebauer, M. Fungal periprosthetic joint infection in total knee arthroplasty: A systematic review. Orthop. Rev. 2015, 7, 5623. [Google Scholar] [CrossRef] [Green Version]
- Fusini, F.; Aprato, A.; Massè, A.; Bistolfi, A.; Girardo, M.; Artiaco, S. Candida periprosthetic infection of the hip: A systematic review of surgical treatments and clinical outcomes. Int. Orthop. 2020, 44, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Li, X.; Du, Y.; Peng, Y.; Wu, W.; Zhou, Y. Success Rate of Fungal Peri-Prosthetic Joint Infection Treated by 2-Stage Revision and Potential Risk Factors of Treatment Failure: A Retrospective Study. Med. Sci. Monit. 2018, 24, 5549–5557. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.-C.; Goswami, K.; Shohat, N.; Blevins, K.; Rondon, A.J.; Parvizi, J. Two-Stage Exchange Arthroplasty Is a Favorable Treatment Option Upon Diagnosis of a Fungal Periprosthetic Joint Infection. J. Arthroplast. 2018, 33, 3555–3560. [Google Scholar] [CrossRef] [PubMed]
- Belden, K.; Cao, L.; Chen, J.; Deng, T.; Fu, J.; Guan, H.; Jia, C.; Kong, X.; Kuo, F.-C.; Li, R.; et al. Hip and Knee Section, Fungal Periprosthetic Joint Infection, Diagnosis and Treatment: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2018, 34 (Suppl. S2), S387–S391. [Google Scholar] [CrossRef] [PubMed]
- Ji, B.; Zhang, X.; Xu, B.; Guo, W.; Mu, W.; Cao, L. Single-Stage Revision for Chronic Fungal Periprosthetic Joint Infection: An Average of 5 Years of Follow-Up. J. Arthroplast. 2017, 32, 2523–2530. [Google Scholar] [CrossRef] [PubMed]
- Klatte, T.O.; Kendoff, D.; Kamath, A.F.; Jonen, V.; Rueger, J.M.; Frommelt, L.; Gebauer, M.; Gehrke, T. Single-stage revision for fungal peri-prosthetic joint infection: A single-centre experience. Bone Jt. J. 2014, 96, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Enz, A.; Mueller, S.; Warnke, P.; Ellenrieder, M.; Mittelmeier, W.; Klinder, A. Periprosthetic Fungal Infections in Severe Endoprosthetic Infections of the Hip and Knee Joint—A Retrospective Analysis of a Certified Arthroplasty Centre of Excellence. J. Fungi 2021, 7, 404. [Google Scholar] [CrossRef] [PubMed]
- Karczewski, D.; Ren, Y.; Andronic, O.; Akgün, D.; Perka, C.; Müller, M.; Kienzle, A. Candida periprosthetic joint infections—Risk factors and outcome between albicans and non-albicans strains. Int. Orthop. 2022, 46, 449–456. [Google Scholar] [CrossRef]
- Saconi, E.S.; de Carvalho, V.C.; de Oliveira, P.R.G.; Lima, A.L.L.M. Prosthetic joint infection due to Candida species: Case series and review of literature. Medicine 2020, 99, e19735. [Google Scholar] [CrossRef]
- Theil, C.; Schmidt-Braekling, T.; Gosheger, G.; Idelevich, E.A.; Moellenbeck, B.; Dieckmann, R. Fungal prosthetic joint infection in total hip or knee arthroplasty: A retrospective single-centre study of 26 cases. Bone Jt. J. 2019, 101, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.R.; Kim, H.J.; Lee, E.J.; Sohn, J.W.; Kim, M.J.; Yoon, Y.K. Prosthetic Joint Infections Caused by Candida Species: A Systematic Review and a Case Series. Mycopathologia 2019, 184, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Jt. J. 2013, 95, 1450–1452. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success After Treatment of Periprosthetic Joint Infection: A Delphi-based International Multidisciplinary Consensus. Clin. Orthop. Relat. Res. 2013, 471, 2374–2382. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Darouiche, R.O.; Hamill, R.J.; Musher, D.M.; Young, E.J.; Harris, R.L. Periprosthetic Candidal Infections Following Arthroplasty. Clin. Infect. Dis. 1989, 11, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Phelan, D.M.; Osmon, D.R.; Keating, M.R.; Hanssen, A.D. Delayed Reimplantation Arthroplasty for Candidal Prosthetic Joint Infection: A Report of 4 Cases and Review of the Literature. Clin. Infect. Dis. 2002, 34, 930–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutronc, H.; Dauchy, F.A.; Cazanave, C.; Rougie, C.; Lafarie-Castet, S.; Couprie, B.; Fabre, T.; Dupon, M. Candida prosthetic infections: Case series and literature review. Scand. J. Infect. Dis. 2010, 42, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Ueng, S.W.N.; Lee, C.-Y.; Hu, C.-C.; Hsieh, P.-H.; Chang, Y. What is the success of treatment of hip and knee candidal periprosthetic joint infection? Clin. Orthop. Relat. Res. 2013, 471, 3002–3009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuiper, J.W.P.; van den Bekerom, M.P.J.; van der Stappen, J.; Nolte, P.A.; Colen, S. 2-stage revision recommended for treatment of fungal hip and knee prosthetic joint infections. Acta Orthop. 2013, 84, 517–523. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| No. | Age (Years) | Sex | Joint | BMI (kg/m2) | Risk Factors | Time from TJA to PJI Diagnosis (Months) | Preoperative CRP (mg/L) | Preoperative ESR (mm/h) | Pathogen | Material for Mycological Culturing | Surgical Protocol | Intravenous Antibacterial/Antifungal Agents | Oral Antibacterial/Antifungal Agents | Follow-Up (after Definitive Procedure) [Months] | Final Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 83 | F | Knee | 37.39 | None | 74 | 5.4 | 10 | Candida parapsilosis, MSCNS | Tissues (+) Synovial fluid (+) Sonication (+) | Two-stage | CFX + AMC | FLU + CFX | 18 | Nail arthrodesis |
| 2 | 68 | F | Knee | 30.47 | Sepsis due to renal failure before the PJI | 28 | 1.9 | 22 | Candida glabrata | Tissues (+) Synovial fluid (+) Sonication (+) | Two-stage | VAN + AMB + MYC | ITR | 10 | Prosthesis replantation |
| 3 | 79 | F | Knee | 30.48 | Psoriathic arthritis | 150 | 64.6 | 103 | Candida albicans | Tissues (+) Synovial fluid (−) Sonication (+) | Two-stage | AMC + CEF + FLU | FLU + AMO/CLA | 37 | Nail arthrodesis |
| 4 | 63 | M | Hip | 30.99 | Alcohilizm | 158 | 6.2 | 10 | Candida albicans | Tissues (+) Synovial fluid (−) Sonication (−) | One-stage | CFX + AMC | FLU | 2 (lost follow-up) | Prosthesis replantation |
| 5 | 77 | F | Knee | 25.65 | None | 9 | 19 | 44 | Candida albicans | Tissues (+) Synovial fluid (−) Sonication (+) | Two-stage | CFX + AMC | FLU | 22 | Prosthesis replantation |
| 6 | 84 | M | Hip | 31.07 | None | 10 | 86.3 | 135 | Candida krusei | Tissues (+) Synovial fluid (−) Sonication (+) | Two-stage | CFX + AMC | ITR | 10 | Resection arthroplasty |
| 7 | 51 | F | Knee | 24.01 | Rheumatoid arthritis | 26 | 5.5 | 42 | Candida parapsilosis | Tissues (+) Synovial fluid (−) Sonication (n/d) | Two-stage | CFX + AMC | KET | 36 | Nail arthrodesis |
| 8 | 58 | M | Knee | 35.44 | After yersinia and chlamydia infections | 12 | 10.4 | 40 | Candida parapsilosis | Tissues (+) Synovial fluid (−) Sonication (+) | Two-stage | AMB + MYC | ITR | 6 | Prosthesis replantation |
| Country | Number of Patients (Male/Female) | Mean Age (Years) | Joint | Mean Preoperative CRP (mg/L) | Bacterial Co-Infection | Risk Factors | Mean Follow-Up (Months) | Therapeutic Success/ Treatment Protocol (n/m) % | Overall Success Rate ** | |
|---|---|---|---|---|---|---|---|---|---|---|
| Darouiche et al. (1989) [32] | USA | 4 (3/1) | 63.5 | K—1 (25%) H—3 (75%) | N/A | Yes—0 No—4 (100%) | Yes—2 (50%) No—2 (50%) | 13.8 | Resection arthroplasty—(0/4) 0% | 0% |
| Phelan et al. (2002) [33] | USA | 4 (2/2) | 72.3 | K—1 (25%) H—3 (75%) | N/A | Yes—0 No—4 (100%) | Yes—4 (100%) No—0 | 52.8 | Two-stage—(4/4) 100% | 100% |
| Dutronc et al. (2010) [34] | France | 7 (3/4) | 72 | K—4 (57.1%) H—3 (42.9%) | 98.1 | Yes—0 No—7 (100%) | Yes—5 (71.4%) No—2 (28.6%) | 30 | No surgery—(0/1) 0% DIAR (1/1)—100% Two-stage—(1/3) 33.3% Arthrodesis—(0/1) 0% Resection arthroplasty—(1/1) 100% | 42.9% |
| Ueng et al. (2013) [35] | Taiwan | 16 (12/4) | 55.4 | K—9 (52.9%) H—7 (47.1%) | N/A | Yes—8 (50%) No—8 (50%) | Yes—11 (68.8%) No—5 (31.2%) | 41 | Two-stage—(8/9) 88.9% Resection arthroplasty—(3/7) 42.9% | 68.8% |
| Kuiper et al. (2013) [36] | Netherland | 8 (2/6) | 72.8 | H—8 (100%) | 47 | Yes—0 No—8 (100%) | Yes—7 (87.5%) No—1 (12.5%) | 30.4 | Two-stage—(2/7) 28.6% *** | 28.6% *** |
| Klatte et al. (2014) [22] | Germany | 10 (6/4) | 67.8 | K—4 (40%) H—6 (60%) | 22 | Yes—6 (60%) No—4 (40%) | Yes—7 (70%) No—3 (30%) | 72 | One-stage—(9/10) 90% | 90% |
| Ji et al. (2017) [21] | China | 11 (4/7) | 66.5 | K—7 (63.6%) H—4 (36.4%) | N/A | Yes—8 (72.7%) No—3 (27.3%) | Yes—6 (54.5%) No—5 (45.5%) | 60 | One-stage—(9/11) 81.8% | 81.8% |
| Kim et al. (2018) [12] | South Korea | 9 (1/8) | 76 | K—9 (100%) | 22.6 | Yes—7 (77.8%) No—2 (22.2%) | Yes—4 (44.4%) No—5 (55.6%) | 66 | Two-stage—(9/9) 100% | 100% |
| Theil et al. (2019) [26] | Germany | 26 (10/16) | 71.9 | K—8 (30.8%) H—18 (69.2%) | N/A | Yes—13 (50%) No—13 (50%) | Yes—24 (92.3%) No—2 (7.7%) | 33 * | One-stage—(0/2) 0% Two-stage—(10/24) 41.7% | 38.5% |
| Saconi et al. (2020) [25] | Brazil | 11 (5/6) | 65.1 | K—5 (45.5%) H—6 (54.5%) | 312 | Yes—6 (54.5%) No—5 (45.5%) | Yes—7 (63.6%) No—4 (36.4%) | 41.7 | DAIR—(1/1) 100% *** One-stage—(2/3) 66.7% *** Two-stage—(1/1) 100% Resection arthroplasty—(4/4) 100% | 88.9% *** |
| Enz et al. (2021) [23] | Germany | 18 (N/A) | 70.2 | K—4 (22.2%) H—14 (77.8%) | N/A | Yes—14 (22.2%) No—4 (77.8%) | N/A | N/A | DAIR—(1/1) 100% **** Two-stage—(5/7) 71.4% **** Resection arthroplasty—(3/5) 60% **** | 72.2% **** |
| Karczewski et al. (2022) [24] | Germany | 29 (13/16) | 71 | K—15 (51.7%) H—14 (48.3%) | 51.7 | Yes—22 (68.2%) No—7 (31.8%) | N/A | 33 | DIAR— (1/2) 50% One-stage—(1/2) 50% Two-stage—(7/8) 87.5% Three-stage—(9/12) 75% Resection arthroplasty—(3/5) 60% | 72.4% |
| Candida albicans | Candida parapsilosis | p-Value | |
|---|---|---|---|
| Males/Females (#) | 33/24 | 17/18 | 0.4 * |
| Hip/Knee | 50/23 | 9/27 | <0.01 * |
| Median age (years) | 73 (62–79) | 71 (65–77) | 0.88 ** |
| Bacterial co-infection (%) | 43 (58.9%) | 17 (47.2%) | 0.3 * |
| Risk factors (no. of patients; %) (##) | 32 (78%) | 13 (52%) | 0.03 * |
Type of risk factors (##)
| 7 2 2 1 1 1 - - 18 9 | 6 - - - 1 1 1 1 3 12 | |
Treatment protocol [no. of patients] (#)
| 2 14 20 5 16 | 0 8 18 3 6 | |
| Overall success rate (n; %) | 44/72 (60.3%) —one patient lost to follow-up | 30/36 (83.3%) | 0.03 * |
Success rate depending on treatment protocol [no. of patients, (%)] (#)
| 1 (50%) 12 (85.7%) 13 (65%) 4 (80%) 2 (66.7%)—one patient lost to follow-up | - 4 (50%) 17 (94.4%) 2 (66.7%) 6 (100%) | - 0.14 * 0.04 * - - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grzelecki, D.; Grajek, A.; Dudek, P.; Olewnik, Ł.; Zielinska, N.; Fulin, P.; Czubak-Wrzosek, M.; Tyrakowski, M.; Marczak, D.; Kowalczewski, J. Periprosthetic Joint Infections Caused by Candida Species—A Single-Center Experience and Systematic Review of the Literature. J. Fungi 2022, 8, 797. https://doi.org/10.3390/jof8080797
Grzelecki D, Grajek A, Dudek P, Olewnik Ł, Zielinska N, Fulin P, Czubak-Wrzosek M, Tyrakowski M, Marczak D, Kowalczewski J. Periprosthetic Joint Infections Caused by Candida Species—A Single-Center Experience and Systematic Review of the Literature. Journal of Fungi. 2022; 8(8):797. https://doi.org/10.3390/jof8080797
Chicago/Turabian StyleGrzelecki, Dariusz, Aleksandra Grajek, Piotr Dudek, Łukasz Olewnik, Nicol Zielinska, Petr Fulin, Maria Czubak-Wrzosek, Marcin Tyrakowski, Dariusz Marczak, and Jacek Kowalczewski. 2022. "Periprosthetic Joint Infections Caused by Candida Species—A Single-Center Experience and Systematic Review of the Literature" Journal of Fungi 8, no. 8: 797. https://doi.org/10.3390/jof8080797
APA StyleGrzelecki, D., Grajek, A., Dudek, P., Olewnik, Ł., Zielinska, N., Fulin, P., Czubak-Wrzosek, M., Tyrakowski, M., Marczak, D., & Kowalczewski, J. (2022). Periprosthetic Joint Infections Caused by Candida Species—A Single-Center Experience and Systematic Review of the Literature. Journal of Fungi, 8(8), 797. https://doi.org/10.3390/jof8080797