
Emergence and Genomic Characterization of Multidrug Resistant Candida auris in Nigeria, West Africa

 , and
, and
Abstract
1. Introduction
1.1. The Cases
1.1.1. Case 1
1.1.2. Case 2
1.1.3. Case 3
1.1.4. Case 4
2. Materials and Methods
2.1. DNA Extraction and Library Preparation
2.2. Whole Genome Sequencing and Bioinformatics Analysis
2.3. Phylogenetic Analysis
3. Results
3.1. Antifungal Susceptibility Test (AFST)
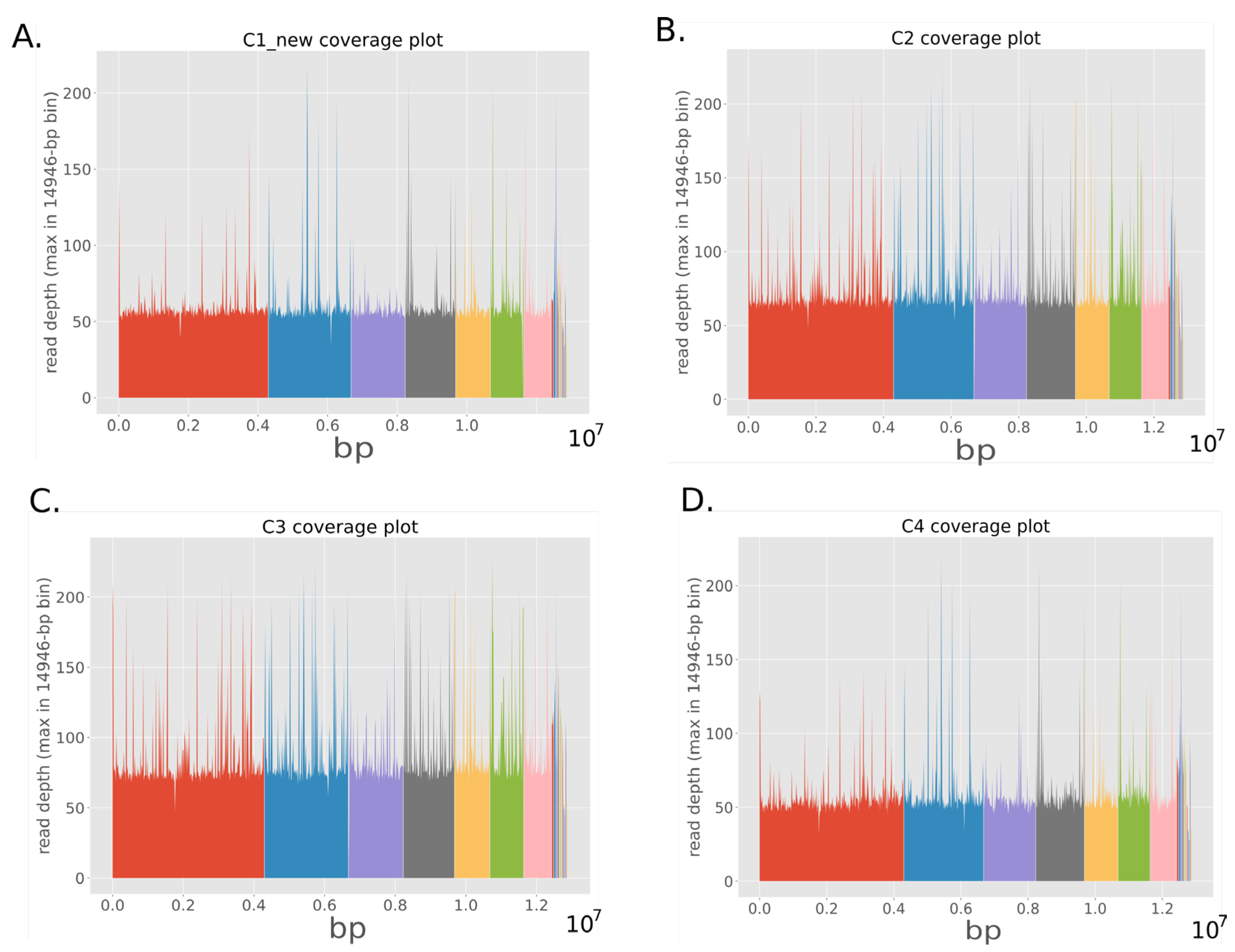
3.2. Genome Analysis
3.3. Variant Analysis
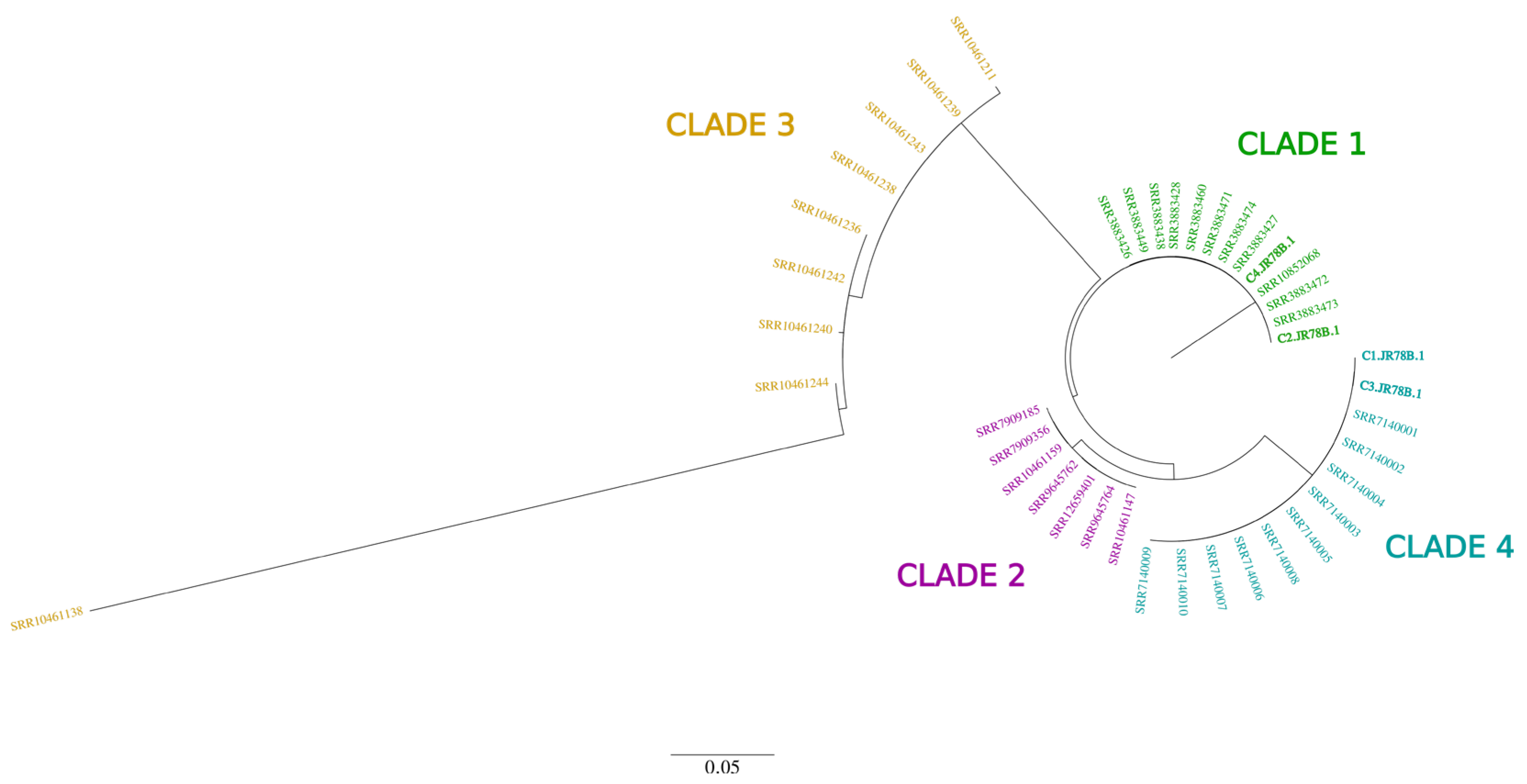
3.4. Phylogenetic Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, W.G.; Shin, J.H.; Uh, Y.; Kang, M.G.; Kim, S.H.; Park, K.H.; Jang, H.C. First three reported cases of nosocomial fungemia caused by Candida auris. J. Clin. Microbiol. 2011, 49, 3139–3142. [Google Scholar] [CrossRef] [PubMed]
- Calandra, T.; Roberts, J.A.; Antonelli, M.; Bassetti, M.; Vincent, J.L. Diagnosis and management of invasive candidiasis in the ICU: An updated approach to an old enemy. Crit. Care 2016, 20, 125. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, M.; Weber, T.; Denker, T.; Winterland, S.; Wichmann, D.; Rohde, H.; Ozga, A.K.; Fischer, M.; Kluge, S. Epidemiology, clinical characteristics, and outcome of candidemia in critically ill patients in Germany: A single-center retrospective 10-year analysis. Ann. Intensiv. Care 2020, 10, 142. [Google Scholar] [CrossRef] [PubMed]
- Jeffery-Smith, A.; Taori, S.K.; Schelenz, S.; Jeffery, K.; Johnson, E.M.; Borman, A. Candida auris: A review of the literature. Clin. Microbiol. Rev. 2018, 31, e00029-17. [Google Scholar] [CrossRef]
- Chow, N.A.; Muñoz, J.F.; Gade, L.; Berkow, E.L.; Li, X.; Welsh, R.M.; Forsberg, K.; Lockhart, S.R.; Adam, R.; Alanio, A.; et al. Tracing the evolutionary history and global expansion of Candida auris using population genomic analyses. Mbio 2020, 11, e03364-19. [Google Scholar] [CrossRef]
- Calvo, B.; Melo, A.S.; Perozo-Mena, A.; Hernandez, M.; Francisco, E.C.; Hagen, F.; Meis, J.F.; Colombo, A.L. First report of Candida auris in America: Clinical and microbiological aspects of 18 episodes of candidemia. J. Infect. 2016, 73, 369–374. [Google Scholar] [CrossRef]
- Zerrouki, H.; Ibrahim, A.; Rebiahi, S.A.; Elhabiri, Y.; Benhaddouche, D.E.; de Groot, T.; Meis, J.F.; Rolain, J.M.; Bittar, F. Emergence of Candida auris in intensive care units in Algeria. Mycoses 2022, 65, 753–759. [Google Scholar] [CrossRef]
- Fayemiwo, S.A.; Makanjuola, O.B. Candida auris infection: How prepared is Nigeria for this emerging fungal agent? Afr. J. Clin. Exp. Microbiol. 2018, 19, 58–63. [Google Scholar] [CrossRef][Green Version]
- Centres of Disease Control and Prevention. Antifungal Susceptibility Testing and Interpretation. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html (accessed on 10 June 2021).
- Price, T.K.; Mirasol, R.; Ward, K.W.; Dayo, A.J.; Hilt, E.E.; Chandrasekaran, S.; Garner, O.B.; de St Maurice, A.; Yang, S. Genomic characterizations of clade III lineage of Candida auris, California, USA. Emerg. Infect. Dis. 2021, 27, 1223. [Google Scholar] [CrossRef]
- Chen, S.; Zhou, Y.; Chen, Y.; Gu, J. Fastp: An ultra-fast all-in-one FASTQ preprocessor. Bioinformatics 2018, 34, i884–i890. [Google Scholar] [CrossRef]
- Li, H. Aligning sequence reads, clone sequences and assembly contigs with BWA-MEM. arXiv 2013, arXiv:1303.3997. [Google Scholar] [CrossRef]
- Garrison, E.; Marth, G. Haplotype-based variant detection from short-read sequencing. arXiv 2012, arXiv:1207.3907. [Google Scholar] [CrossRef]
- Cingolani, P.; Platts, A.; Wang, L.L.; Coon, M.; Nguyen, T.; Wang, L.; Land, S.J.; Lu, X.; Ruden, D.M. A program for annotating and predicting the effects of single nucleotide polymorphisms, SnpEff: SNPs in the genome of Drosophila melanogaster strain w1118; iso-2; iso-3. Fly 2012, 6, 80–92. [Google Scholar] [CrossRef]
- Ruden, D.M.; Cingolani, P.; Patel, V.M.; Coon, M.; Nguyen, T.; Land, S.J.; Ruden, D.M.; Lu, X. Using Drosophila melanogaster as a model for genotoxic chemical mutational studies with a new program, SnpSift. Front. Genet. 2012, 3, 35. [Google Scholar]
- Li, H. A statistical framework for SNP calling, mutation discovery, association mapping and population genetical parameter estimation from sequencing data. Bioinformatics 2011, 27, 2987–2993. [Google Scholar] [CrossRef]
- Minh, B.Q.; Schmidt, H.A.; Chernomor, O.; Schrempf, D.; Woodhams, M.D.; Von Haeseler, A.; Lanfear, R. IQ-TREE 2: New models and efficient methods for phylogenetic inference in the genomic era. Mol. Biol. Evol. 2020, 37, 1530–1534. [Google Scholar] [CrossRef]
- Healey, K.R.; Kordalewska, M.; Jiménez Ortigosa, C.; Singh, A.; Berrío, I.; Chowdhary, A.; Perlin, D.S. Limited ERG11 mutations identified in isolates of Candida auris directly contribute to reduced azole susceptibility. Antimicrob. Agents Chemother. 2018, 62, e01427-18. [Google Scholar] [CrossRef]
- Naicker, S.D.; Maphanga, T.G.; Chow, N.A.; Allam, M.; Kwenda, S.; Ismail, A.; Govender, N.P. Clade distribution of Candida auris in South Africa using whole genome sequencing of clinical and environmental isolates. Emerg. Microbes Infect. 2021, 10, 1300–1308. [Google Scholar] [CrossRef]
- Escandón, P.; Cáceres, D.H.; Espinosa-Bode, A.; Rivera, S.; Armstrong, P.; Vallabhaneni, S.; Berkow, E.L.; Lockhart, S.R.; Chiller, T.; Jackson, B.R.; et al. Notes from the field: Surveillance for Candida auris—Colombia, September 2016–May 2017. Morb. Mortal. Wkly. Rep. 2018, 67, 459. [Google Scholar] [CrossRef]
- Ben-Ami, R.; Berman, J.; Novikov, A.; Bash, E.; Shachor-Meyouhas, Y.; Zakin, S.; Maor, Y.; Tarabia, J.; Schechner, V.; Adler, A.; et al. Multidrug-resistant Candida haemulonii and C. auris, Tel Aviv, Israel. Emerg. Infect. Dis. 2016, 23, 195. [Google Scholar]
- Vallabhaneni, S.; Kallen, A.; Tsay, S.; Chow, N.; Welsh, R.; Kerins, J.; Kemble, S.K.; Pacilli, M.; Black, S.R.; Landon, E.; et al. Investigation of the first seven reported cases of Candida auris, a globally emerging invasive, multidrug-resistant fungus—United States, May 2013–August 2016. Morb. Mortal. Wkly. Rep. 2016, 65, 1234–1237. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Duggal, S.; Agarwal, K.; Prakash, A.; Singh, P.K.; Jain, S.; Kathuria, S.; Randhawa, H.S.; Hagen, F.; et al. New clonal strain of Candida auris, Delhi, India. Emerg. Infect. Dis. 2013, 19, 1670–1673. [Google Scholar] [CrossRef] [PubMed]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob. Resist. Infect. Control 2016, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Recommendations for Identification of Candida auris. Available online: https://www.cdc.gov/fungal/diseases/candidiasis/recommendations.html (accessed on 18 June 2021).
- Rudramurthy, S.M.; Chakrabarti, A.; Paul, R.A.; Sood, P.; Kaur, H.; Capoor, M.R.; Kindo, A.J.; Marak, R.S.; Arora, A.; Sardana, R.; et al. Candida auris candidaemia in Indian ICUs: Analysis of risk factors. J. Antimicrob. Chemother. 2017, 72, 1794–1801. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 2017, 64, 134–140. [Google Scholar] [CrossRef]
- Driemeyer, C.; Falci, D.R.; Oladele, R.O.; Bongomin, F.; Ocansey, B.K.; Govender, N.P.; Hoenigl, M.; Gangneux, J.P.; Lass-Flörl, C.; Cornely, O.A.; et al. The current state of clinical mycology in Africa: A european confederation of medical mycology and international society for human and animal mycology survey. Lancet Microbe 2022, 3, e464–e470. [Google Scholar] [CrossRef]
- De Groot, T.; Puts, Y.; Berrio, I.; Chowdhary, A.; Meis, J.F. Development of Candida auris short tandem repeat typing and its application to a global collection of isolates. MBio 2020, 11, e02971-19. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Date | February, 2021 | February, 2021 | March, 2021 | April, 2021 |
| Gender, age (years) | Male, 60 | Female, 67 | Male, 74 | Female, 48 |
| Underlying disease | Diabetes mellitus, Hypertension | Diabetes mellitus, Hypertension, COVID-19 | Prostate cancer | Systemic Lupus Erythematosus (SLE) |
| Country visited in the previous year | Unknown | Unknown | Dubai, UAE | No travel |
| Recent intake of broad-spectrum antibiotics | Yes | Yes | Yes | Yes |
| Vascular surgery | No | No | No | No |
| Total parenteral nutrition | No | No | No | Yes |
| Dialysis | Yes | No | No | Yes |
| Urinary catheterization | Yes | Yes | Yes | Yes |
| Postoperative drain placement | Yes | No | No | No |
| Type of invasive candidiasis infection | Bloodstream infection (also isolated from sputum and urine) | Bloodstream infection | Bloodstream (probable skin colonization) | Bloodstream |
| Antifungal Treatment | Voriconazole | None | None | Fluconazole, voriconazole |
| Outcome | Death | Death | Discharged | Death |
| Antifungal (Minimal Inhibitory Concentration mg/L) | |||||||
|---|---|---|---|---|---|---|---|
| Fluconazole | Voriconazole | Posaconazole | Amphotericin B | Caspofungin | Micafungin | Anidulafungin | |
| Tentative MIC breakpoints | ≥32 | NA * | NA * | ≥2 | ≥2 | ≥4 | ≥4 |
| Case 1 | 16 | 0.25 | 0.016 | 1 | 0.06 | 0.063 | 0.031 |
| Case 2 | 64 | 1 | 0.031 | 0.5 | 0.06 | 0.125 | 0.25 |
| Case 3 | 1 | 0.016 | <0.016 | 0.25 | 0.06 | 0.125 | 0.25 |
| Case 4 | 32 | 1 | 0.031 | 0.5 | 0.06 | 0.125 | 0.25 |
| Isolate | Change | Type of Change | Gene ID | Ortholog |
|---|---|---|---|---|
| Case 1 | a1004g | Asn335Ser | snp; missense | CJI97_001156 | ERG11 |
| a1029c | Glu343Asp | snp; missense | CJI97_001156 | ERG11 | |
| Case 2 | a395t | Tyr132Phe | snp; missense | CJI97_001156 | ERG11 |
| ctc374_376ttt | Leu125Phe | complex; missense | CJI97_001156 | ERG11 | |
| c4453a | Leu148Ile | snp; missense | CJI97_000983 | FKS1 | |
| a2811t | Arg937Ser | snp; missense | CJI97_000983 | FKS1 | |
| ca2100ag | Ile701Val | indel; missense | CJI97_000983 | FKS1 | |
| a2080g | Ile694Val | snp; missense | CJI97_000983 | FKS1 | |
| Case 3 | a530g | Lys177Arg | snp; missense | CJI97_001156 | ERG11 |
| a1004g | Asn335Ser | snp; missense | CJI97_001156 | ERG11 | |
| a1029c | Glu343Asp | snp; missense | CJI97_001156 | ERG11 | |
| Case 4 | ctc374_376ttt | Leu125Phe | complex; missense | CJI97_001156 | ERG11 |
| a395t | Tyr132Phe | snp; missense | CJI97_001156 | ERG11 | |
| a117c | Glu39Asp | snp; missense | CJI97_005027 | ERG2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oladele, R.; Uwanibe, J.N.; Olawoye, I.B.; Ettu, A.-W.O.; Meis, J.F.; Happi, C.T. Emergence and Genomic Characterization of Multidrug Resistant Candida auris in Nigeria, West Africa. J. Fungi 2022, 8, 787. https://doi.org/10.3390/jof8080787
Oladele R, Uwanibe JN, Olawoye IB, Ettu A-WO, Meis JF, Happi CT. Emergence and Genomic Characterization of Multidrug Resistant Candida auris in Nigeria, West Africa. Journal of Fungi. 2022; 8(8):787. https://doi.org/10.3390/jof8080787
Chicago/Turabian StyleOladele, Rita, Jessica N. Uwanibe, Idowu B. Olawoye, Abdul-Wahab O. Ettu, Jacques F. Meis, and Christian T. Happi. 2022. "Emergence and Genomic Characterization of Multidrug Resistant Candida auris in Nigeria, West Africa" Journal of Fungi 8, no. 8: 787. https://doi.org/10.3390/jof8080787
APA StyleOladele, R., Uwanibe, J. N., Olawoye, I. B., Ettu, A.-W. O., Meis, J. F., & Happi, C. T. (2022). Emergence and Genomic Characterization of Multidrug Resistant Candida auris in Nigeria, West Africa. Journal of Fungi, 8(8), 787. https://doi.org/10.3390/jof8080787