
Invasive Fusariosis in Pediatric Hematology/Oncology and Stem Cell Transplant Patients: A Report from the Israeli Society of Pediatric Hematology-Oncology

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Diagnostic Methods
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
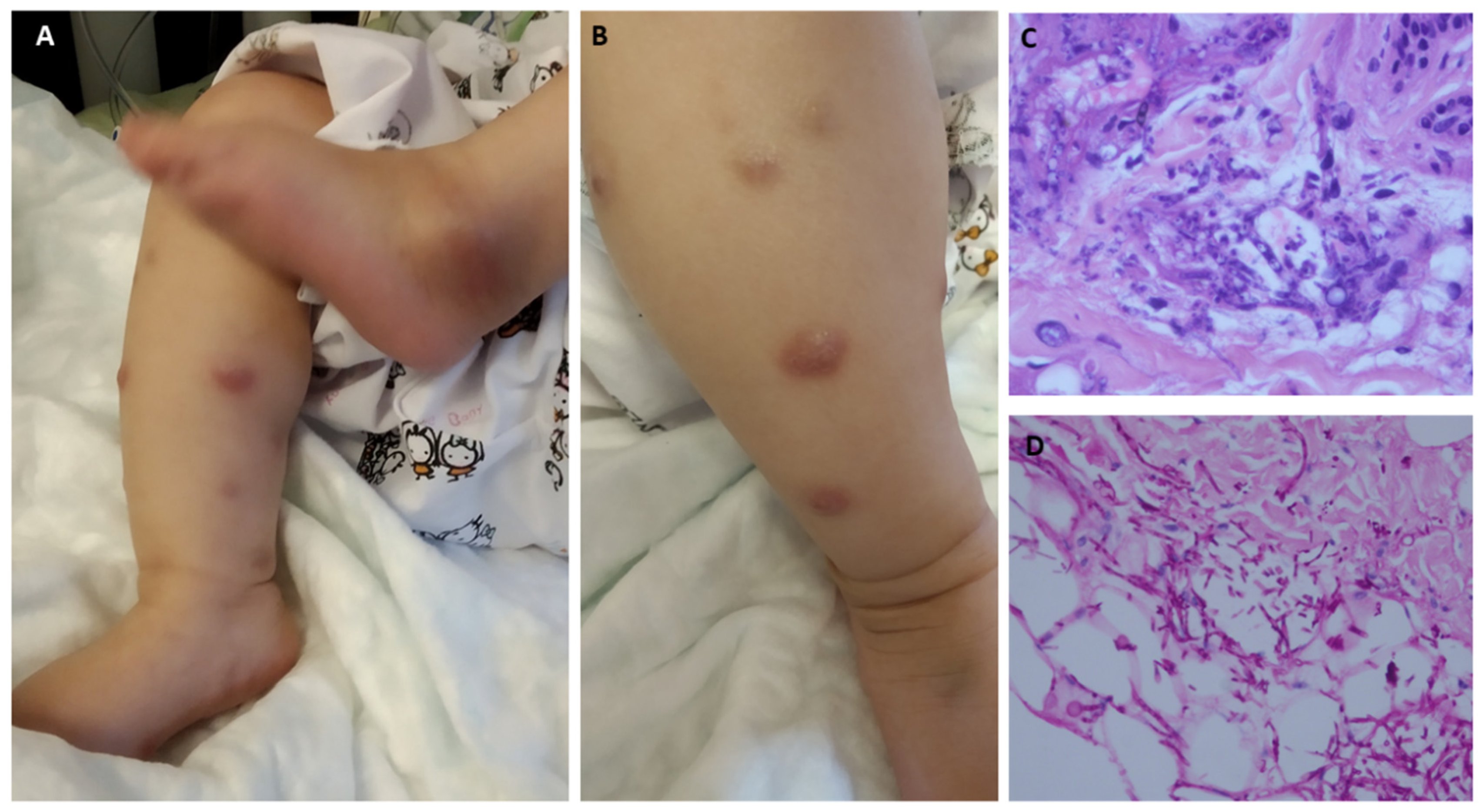
3.2. Infection Patterns and Pathogens
3.3. Treatment
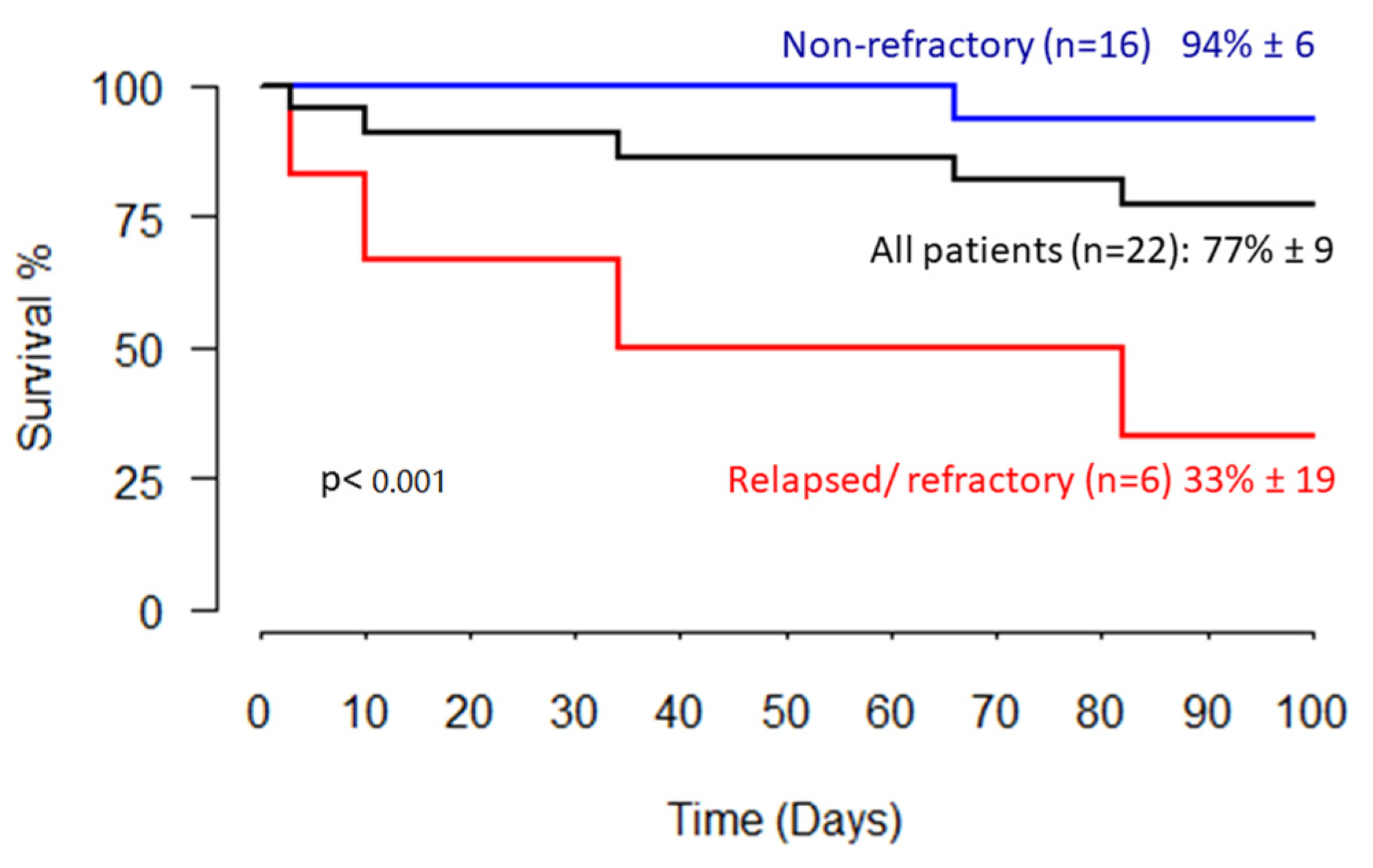
3.4. Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chamilos, G.; Luna, M.; Lewis, R.E.; Bodey, G.P.; Chemaly, R.; Tarrand, J.J.; Safdar, A.; Raad, K.D., II. Invasive fungal infections in patients with hematologic malignancies in a tertiary care cancer center: An autopsy study over a 15-year period (1989–2003). Haematologica 2006, 91, 986–989. [Google Scholar] [PubMed]
- Pagano, L.; Caira, M.; Candoni, A.; Offidani, M.; Fianchi, L.; Martino, B.; Pastore, D.; Picardi, M.; Bonini, A.; Chierichini, A.; et al. The epidemiology of fungal infections in patients with hematologic malignancies: The SEIFEM-2004 study. Haematologica 2006, 91, 1068–1075. [Google Scholar] [PubMed]
- Nucci, M.; Anaissie, E. Fusarium infections in immunocompromised patients. Clin. Microbiol. Rev. 2007, 20, 695–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nucci, M.; Barreiros, G.; Akiti, T.; Anaissie, E.; Nouér, S.A. Invasive fusariosis in patients with hematologic diseases. J. Fungi 2021, 7, 815. [Google Scholar] [CrossRef]
- Lamoth, F.; Damonti, L.; Alexander, B.D. Role of antifungal susceptibility testing in non-aspergillus invasive mold infections. J. Clin. Microbiol. 2016, 54, 1638–1640. [Google Scholar] [CrossRef] [Green Version]
- Castagnola, E.; Cesaro, S.; Giacchino, M.; Livadiotti, S.; Tucci, F.; Zanazzo, G.; Caselli, D.; Caviglia, I.; Parodi, S.; Rondelli, R.; et al. Fungal infections in children with cancer: A prospective, multicenter surveillance study. Pediatr. Infect. Dis. J. 2006, 25, 634–639. [Google Scholar] [CrossRef]
- Pana, Z.D.; Roilides, E.; Warris, A.; Groll, A.H.; Zaoutis, T. Epidemiology of Invasive Fungal Disease in Children. J. Pediatric Infect. Dis. Soc. 2017, 6, S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Hale, K.A.; Shaw, P.J.; Dalla-Pozza, L.; MacIntyre, C.R.; Isaacs, D.; Sorrell, T.C. Epidemiology of paediatric invasive fungal infections and a case-control study of risk factors in acute leukaemia or post stem cell transplant. Br. J. Haematol. 2010, 149, 263–272. [Google Scholar] [CrossRef]
- Elitzur, S.; Arad-Cohen, N.; Barg, A.; Litichever, N.; Bielorai, B.; Elhasid, R.; Fischer, S.; Fruchtman, Y.; Gilad, G.; Kapelushnik, J.; et al. Mucormycosis in children with haematological malignancies is a salvageable disease: A report from the Israeli Study Group of Childhood Leukemia. Br. J. Haematol. 2020, 189, 339–350. [Google Scholar] [CrossRef]
- Elitzur, S.; Fischer, S.; Arad-Cohen, N.; Barg, A.; Ben-Harosh, M.; Danino, D.; Elhasid, R.; Gefen, A.; Gilad, G.; Levy, I.; et al. Disseminated mucormycosis in immunocompromised children: Are new antifungal agents making a difference? A multicenter retrospective study. J. Fungi 2021, 7, 165. [Google Scholar] [CrossRef]
- Arnoni, M.V.; Paula, C.R.; Auler, M.E.; Simões, C.C.N.; Nakano, S.; Szeszs, M.W.; Melhem, M.D.S.C.; Pereira, V.B.R.; Garces, H.G.; Bagagli, E.; et al. Infections caused by fusarium species in pediatric cancer patients and review of published literature. Mycopathologia 2018, 183, 941–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassler, A.; Lieb, A.; Seidel, D.; Cesaro, S.; Greil, J.; Klimko, N.; Khostelidi, S.; Solopova, G.; Ogunc, D.; Graeff, L.D.; et al. Disseminated fusariosis in immunocompromised children—Analysis of recent cases identified in the global fungiscope registry. Pediatr. Infect. Dis. J. 2017, 36, 230–231. [Google Scholar] [CrossRef] [PubMed]
- Riojas Hernández, M.P.; Cisneros Saldaña, D.; Vaquera Aparicio, D.N.; Castillo Bejarano, J.I.; Mascareñas de los Santos, A.H.; Villanueva-Lozano, H.; Treviño-Rangel Rogelio de, J.; De la O Cavazos, M.E. Disseminated fusariosis in immunocompromised children: A case series and review of literature. J. Chemother. 2021, 33, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Biddeci, G.; Donà, D.; Geranio, G.; Spadini, S.; Petris, M.G.; Pillon, M.; Biffi, A.; Putti, M.C. Systemic fusariosis: A rare complication in children with acute lymphoblastic leukemia. J. Fungi 2020, 6, 212. [Google Scholar] [CrossRef]
- Litvinov, N.; da Silva, M.T.N.; van der Heijden, I.M.; Graça, M.G.; Marques de Oliveira, L.; Fu, L.; Giudice, M.; Zilda de Aquino, M.; Odone-Filho, V.; Marques, H.H.; et al. An outbreak of invasive fusariosis in a children’s cancer hospital. Clin. Microbiol. Infect. 2015, 21, 268.e1–268.e7. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, K.L.; Sheffield, H.; Richardson, S.E.; Sung, L.; Morris, S.K. Invasive fusariosis: A single pediatric center 15-Year experience. J. Pediatric Infect. Dis. Soc. 2015, 4, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Hiebert, R.M.; Welliver, R.C.; Yu, Z. Fusarium osteomyelitis in a patient with pearson syndrome: Case report and review of the literature. Open Forum Infect. Dis. 2016, 3, ofw183. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Almyroudis, N.G.; Battiwalla, M.; Bambach, B.J.; McCarthy, P.L.; Proefrock, A.D.; Ball, D.; Paplham, P.; Varma, A.; Kwon-Chung, J.; et al. Successful treatment of disseminated fusariosis with posaconazole during neutropenia and subsequent allogeneic hematopoietic stem cell transplantation. Transpl. Infect. Dis. 2007, 9, 156–160. [Google Scholar] [CrossRef]
- Morel, L.N.; Cid, P.M.; De Celada, R.M.A.; Rodríguez, M.F.; Merino, M.J.B.; Arias, Á.G.; Laguna, R.D.L. Disseminated fusariosis in a pediatric population. Pediatr. Dermatol. 2013, 30, 2012–2013. [Google Scholar] [CrossRef]
- Carlesse, F.; Amaral, A.P.C.; Gonçalves, S.S.; Xafranski, H.; Lee, M.L.M.; Zecchin, V.; Petrilli, A.S.; Al-Hatmi, A.M.; Hagen, F.; Meis, J.F.; et al. Outbreak of Fusarium oxysporum infections in children with cancer: An experience with 7 episodes of catheter-related fungemia. Antimicrob. Resist. Infect. Control 2017, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Velasco, E.; Martins, C.A.; Nucci, M. Successful treatment of catheter-related fusarial infection in immunocompromised children. Clin. Microbiol. Infect. Dis. 1995, 14, 697–699. [Google Scholar] [CrossRef] [PubMed]
- Peter Donnelly, J.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutati, E.I.; Anaissie, E.J. Fusarium, a significant emerging pathogen in patients with hematologic malignancy: Ten years’ experience at a cancer center and implications for management. Blood 1997, 90, 999–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nucci, M.; Marr, K.A.; Vehreschild, M.J.G.T.; de Souza, C.A.; Velasco, E.; Cappellano, P.; Carlesse, F.; Queiroz-Telles, F.; Sheppard, D.C.; Kindo, A.; et al. Improvement in the outcome of invasive fusariosis in the last decade. Clin. Microbiol. Infect. 2014, 20, 580–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nucci, M.; Anaissie, E.J.; Queiroz-Telles, F.; Martins, C.A.; Trabasso, P.; Solza, C.; Mangini, C.; Simões, B.P.; Colombo, A.L.; Vaz, J.; et al. Outcome predictors of 84 patients with hematologic malignancies and Fusarium infection. Cancer 2003, 98, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Tacke, D.; Cornely, O.A. Bone and joint infections by Mucorales, Scedosporium, Fusarium and even rarer fungi. Crit. Rev. Microbiol. 2016, 42, 158–171. [Google Scholar] [CrossRef]
- Sierra-Hoffman, M.; Paltiyevich-Gibson, S.; Carpenter, J.L.; Hurley, D.L. Fusarium osteomyelitis: Case report and review of the literature. Scand. J. Infect. Dis. 2005, 37, 237–240. [Google Scholar] [CrossRef]
- Edupuganti, S.; Rouphael, N.; Mehta, A.; Eaton, M.; Heller, J.G.; Bressler, A.; Brandt, M.; O’Donnell, K. Fusarium falciforme vertebral abscess and osteomyelitis: Case report and molecular classification. J. Clin. Microbiol. 2011, 49, 2350–2353. [Google Scholar] [CrossRef] [Green Version]
- Mader, J.T.; Shirtliff, M.; Calhoun, J.H. The host and the skeletal infection: Classification and pathogenesis of acute bacterial bone and joint sepsis. Baillieres Best Pract. Res. Clin. Rheumatol. 1999, 13, 1–20. [Google Scholar] [CrossRef]
- Lortholary, O.; Obenga, G.; Biswas, P.; Caillot, D.; Chachaty, E.; Bienvenu, A.L.; Cornet, M.; Greene, J.; Herbrecht, R.; Lacroix, C.; et al. International retrospective analysis of 73 cases of invasive fusariosis treated with voriconazole. Antimicrob. Agents Chemother. 2010, 54, 4446–4450. [Google Scholar] [CrossRef] [Green Version]
- Campo, M.; Lewis, R.E.; Kontoyiannis, D.P. Invasive fusariosis in patients with hematologic malignancies at a cancer center: 1998–2009. J. Infect. 2010, 60, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Stempel, J.M.; Hammond, S.P.; Sutton, D.A.; Weiser, L.M.; Marty, F.M. Invasive Fusariosis in the Voriconazole Era: Single-Center 13-Year Experience. Open Forum Infect. Dis. 2015, 2, ofv099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinel-Ingroff, A.; Colombo, A.L.; Cordoba, S.; Dufresne, P.J.; Fuller, J.; Ghannoum, M.; Gonzalez, G.M.; Guarro, J.; Kidd, S.E.; Meis, J.F.; et al. International evaluation of MIC distributions and epidemiological cutoff value (ECV) definitions for Fusarium species identified by molecular methods for the CLSI broth microdilution method. Antimicrob. Agents Chemother. 2016, 60, 1079–1084. [Google Scholar] [CrossRef] [Green Version]
- Nucci, M.; Jenks, J.; Thompson, G.R.; Hoenigl, M.; Dos Santos, M.C.; Forghieri, F.; Rico, J.C.; Bonuomo, V.; Lopez-Soria, L.; Lass-Florl, C.; et al. Do high MICs predict the outcome in invasive fusariosis? J. Antimicrob. Chemother. 2021, 76, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Groll, A.H.; Pana, D.; Lanternier, F.; Mesini, A.; Ammann, R.A.; Averbuch, D.; Castagnola, E.; Cesaro, S.; Engelhard, D.; Garcia-Vidal, C.; et al. 8th European Conference on Infections in Leukaemia: 2020 guidelines for the diagnosis, prevention, and treatment of invasive fungal diseases in paediatric patients with cancer or post-haematopoietic cell transplantation. Lancet Oncol. 2021, 22, e254–e269. [Google Scholar] [CrossRef]
- Hoenigl, M.; Salmanton-García, J.; Walsh, T.J.; Nucci, M.; Neoh, C.F.; Jenks, J.D.; Lackner, M.; Sprute, R.; Al-Hatmi, A.M.S.; Bassetti, M.; et al. Global guideline for the diagnosis and management of rare mould infections: An initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology and the American Society for Microbiolo. Lancet Infect. Dis. 2021, 21, e246–e257. [Google Scholar] [CrossRef]
- Neely, M.; Rushing, T.; Kovacs, A.; Jelliffe, R.; Hoffman, J. Voriconazole pharmacokinetics and pharmacodynamics in children. Clin. Infect. Dis. 2010, 50, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Kadri, S.S.; Remy, K.E.; Strich, J.R.; Gea-Banacloche, J.; Leitman, S.F. Role of granulocyte transfusions in invasive fusariosis: Systematic review and single-center experience. Transfusion 2015, 55, 2076–2085. [Google Scholar] [CrossRef] [Green Version]
- Roden, M.M.; Zaoutis, T.E.; Buchanan, W.L.; Knudsen, T.A.; Sarkisova, T.A.; Schaufele, R.L.; Sein, M.; Sein, T.; Chiou, C.C.; Chu, J.H.; et al. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin. Infect. Dis. 2005, 41, 634–653. [Google Scholar] [CrossRef] [Green Version]
- Kontoyiannis, D.P.; Bodey, G.P.; Hanna, H.; Hachem, R.; Boktour, M.; Girgaway, E.; Mardani, M.; Raad, I. Outcome determinants of fusariosis in a tertiary care cancer center: The impact of neutrophil recovery. Leuk. Lymphoma 2004, 45, 139–141. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All (n = 22) n (%) | Death ≤ 90 d (n = 5) n (%) | Alive ≤ 90 d (n = 17) n (%) | p Value * | ||
|---|---|---|---|---|---|---|
| Sex | Male | 14 (64) | 4 (80) | 10 (59) | 0.61 | |
| Female | 8 (36) | 1 (20) | 7 (41) | |||
| Age (years) | <10 | 9 (41) | 1 (20) | 8 (47) | 0.36 | |
| ≥10 | 13 (59) | 4 (80) | 9 (53) | |||
| Median (range) | 10.8 (0.4–18) | 13.2 (8.1–18) | 10.5 (0.4–16) | |||
| Underlying condition | Hematological malignancies | 16 (73) | 5 (100) | 11 (65) | 0.27 | |
| ALL | 8 | 4 | 4 | |||
| AML | 8 | 1 | 7 | |||
| Solid tumors | 2 (9) | 0 | 2 | |||
| Neuroblastoma | 1 | 0 | 1 | |||
| Medulloblastoma | 1 | 0 | 1 | |||
| Non-malignant hematological conditions | 4 (18) | 0 | 4 | |||
| Aplastic anemia | 2 | 0 | 2 | |||
| Beta-thalassemia post-SCT | 1 | 0 | 1 | |||
| Congenital neutropenia due to ADA2 deficiency | 1 | 0 | 1 | |||
| Disease status | Relapsed/refractory malignancy Non-refractory | 6 (27) 16 (73) | 4 (80) 1 (20) | 2 (12) 15 (88) | 0.009 | |
| Preceding corticosteroid therapy | Yes | 7 (32) | 3 | 4 | 0.27 | |
| No | 15 (68) | 2 | 13 | |||
| Preceding treatment | SCT | 9(41) | 4 (80) | 5 (29) | 0.12 | |
| Allogeneic SCT | 8 | 4 | 4 | |||
| Autologous SCT | 1 | 0 | 1 | |||
| Concurrent GVHD | 0 | 0 | 0 | |||
| Time from SCT, days Median (range) | 35 (1–1174) | 122 (35–1174) | 8 (1–194) | |||
| Other | Chemotherapy | 9 (41) | 1 (20) | 8 (47) | ||
| Immunotherapy | 2 (9) | 0 | 2 | |||
| None | 2 (9) | 0 | 2 | |||
| Neutropenia | Yes | New-onset | 17 (77) | 4 | 13 | 1.00 |
| Congenital | 2 (9) | 0 | 2 | |||
| None | 3 (14) | 1 | 2 | |||
| Blood cultures | Positive Negative | 8 (36) 14 (64) | 2 3 | 6 11 | 1.00 | |
| Pattern of infection | Disseminated | 16 (73) | 5 | 11 | 0.27 | |
| Local | 5 (23) | 0 | 5 | |||
| Isolated fungemia | 1 (4) | 0 | 1 | |||
| Category (EORTC/MSG criteria) | Proven | 19 (82) | 5 | 14 | - | |
| Probable | 3 (18) | 0 | 3 | |||
| Antifungal therapy | Combination therapy | 19 (86) | 4 | 15 | - | |
| L-AmB -azole combination a | 11 | 0 | 13 | |||
| AmB-voriconazole combination | 7 | 3 | 4 | |||
| Other b | 1 | 1 | 0 | |||
| Single-agent therapy | 3 (14) | 1 | 2 | |||
| Antifungal prophylaxis | Yes | 19 (86) | 5 | 14 | - | |
| Fluconazole | 10 | 2 | 8 | |||
| Itraconazole | 7 | 2 | 5 | |||
| Voriconazole | 1 | 0 | 1 | |||
| Caspofungin | 1 | 1 | 0 | |||
| No | 3 (14) | 0 | 3 |
| Patient No. * | Pathogen | Source | EORTC Classification | Amphotericin B | Voriconazole | Fluconazole | Itraconazole | Posaconazole | Caspofungin | Anidulafungin | Isavuconazole |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F. solani | Skin, blood-cultures. BAL-PCR. | Proven | 2 | >16 | >16 | >16 | >8 | >16 | ||
| 4 | F. solani | Skin, blood-culture and PCR | Proven | 2 | 3 | ||||||
| 6 | Fusarium sp. | Skin, sinus, blood-cultures | Proven | 2 | 2 | 2 | |||||
| 7 | Fusarium sp. | Skin culture | Proven | 0.5 | >16 | >16 | >16 | >8 | >16 | >16 | |
| 8 | Fusarium sp. | Sinus culture | Probable | 2 | >16 | >16 | >16 | >8 | >8 | ||
| 15 | Fusarium sp. | Blood culture, and histopathology from skin lesion | Proven | 24 | 0.75 | 192 | 32 | 0.38 | |||
| 17 | F. moniliforme | Culture and PCR from sinus, histopathology from skin lesions | Proven | 16 | 0.75 | ||||||
| 18 | F. solani | Culture, histopathology and PCR from sinus | Proven | 1.5 | 0.75 | 256 | 32 | ||||
| 20 | Fusarium sp. | Culture, histopathology and PCR from sinus | Proven | 4 | 4 | 128 | 16 | >8 | |||
| 21 | Fusarium sp. | Blood culture | Proven | 4 | 0.47 | ||||||
| 22 | Fusarium sp. | Culture and histopathology from sinus | Proven | 2 | 4 | 128 | 16 | 2 | >8 | >8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benish, M.; Elitzur, S.; Arad-Cohen, N.; Barg, A.A.; Ben-Harosh, M.; Bielorai, B.; Fischer, S.; Gilad, G.; Levy, I.; Rosenfeld-Keidar, H.; et al. Invasive Fusariosis in Pediatric Hematology/Oncology and Stem Cell Transplant Patients: A Report from the Israeli Society of Pediatric Hematology-Oncology. J. Fungi 2022, 8, 387. https://doi.org/10.3390/jof8040387
Benish M, Elitzur S, Arad-Cohen N, Barg AA, Ben-Harosh M, Bielorai B, Fischer S, Gilad G, Levy I, Rosenfeld-Keidar H, et al. Invasive Fusariosis in Pediatric Hematology/Oncology and Stem Cell Transplant Patients: A Report from the Israeli Society of Pediatric Hematology-Oncology. Journal of Fungi. 2022; 8(4):387. https://doi.org/10.3390/jof8040387
Chicago/Turabian StyleBenish, Marganit, Sarah Elitzur, Nira Arad-Cohen, Assaf Arie Barg, Miriam Ben-Harosh, Bella Bielorai, Salvador Fischer, Gil Gilad, Itzhak Levy, Hila Rosenfeld-Keidar, and et al. 2022. "Invasive Fusariosis in Pediatric Hematology/Oncology and Stem Cell Transplant Patients: A Report from the Israeli Society of Pediatric Hematology-Oncology" Journal of Fungi 8, no. 4: 387. https://doi.org/10.3390/jof8040387
APA StyleBenish, M., Elitzur, S., Arad-Cohen, N., Barg, A. A., Ben-Harosh, M., Bielorai, B., Fischer, S., Gilad, G., Levy, I., Rosenfeld-Keidar, H., Shachor-Meyouhas, Y., Soen-Grisaru, G., Weinreb, S., Nirel, R., & Elhasid, R. (2022). Invasive Fusariosis in Pediatric Hematology/Oncology and Stem Cell Transplant Patients: A Report from the Israeli Society of Pediatric Hematology-Oncology. Journal of Fungi, 8(4), 387. https://doi.org/10.3390/jof8040387