
Serological Changes in Anti-Aspergillus IgG Antibody and Development of Chronic Pulmonary Aspergillosis in Patients Treated for Pulmonary Tuberculosis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurement of Serum Anti-Aspergillus IgG Antibody Levels and Classification of Comparison Groups
2.3. Radiographic and Microbiological Evaluation
2.4. Diagnosis of CPA after PTB
2.5. Statistical Analysis
3. Results
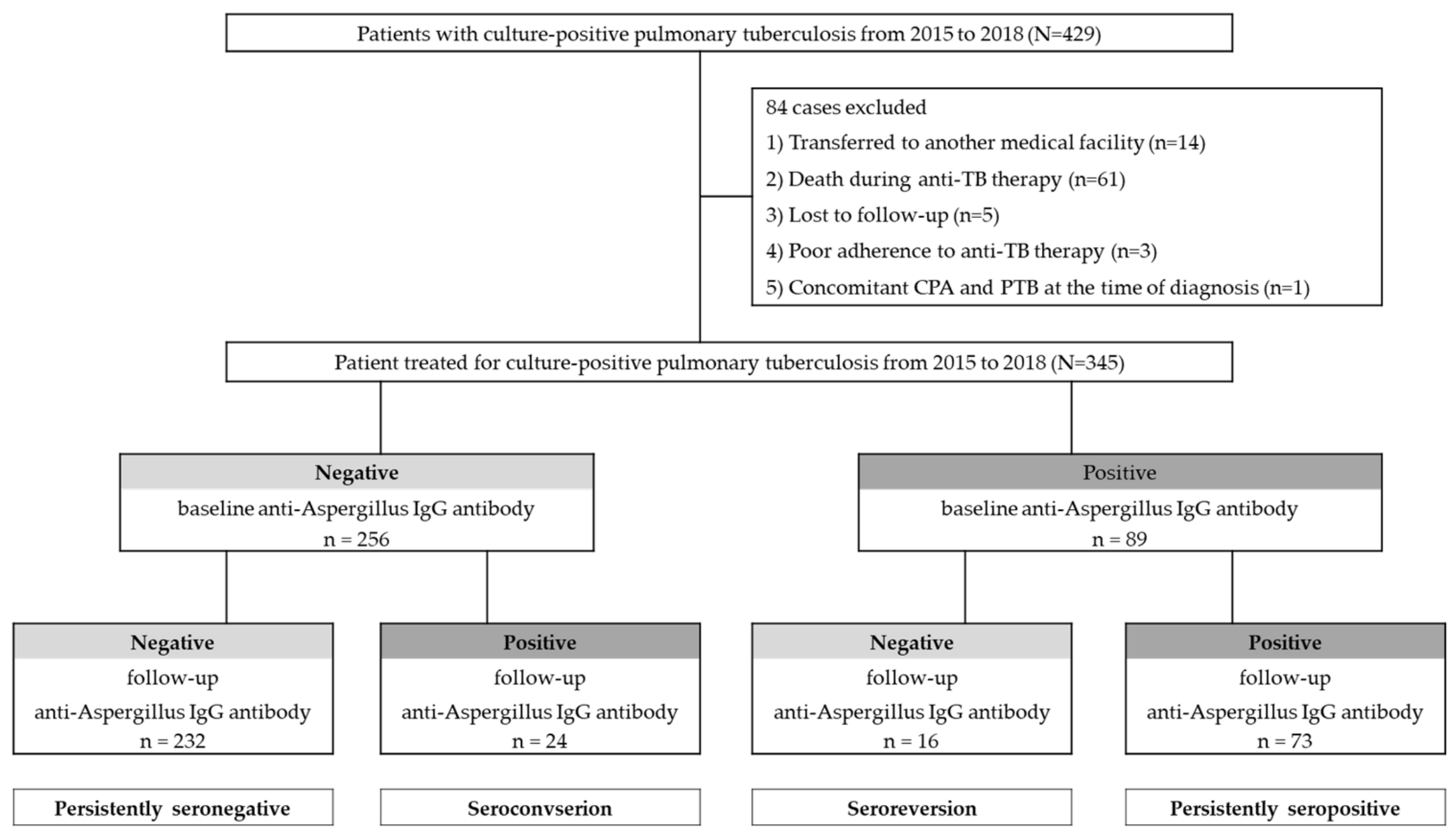
3.1. Study Population and Baseline Characteristics
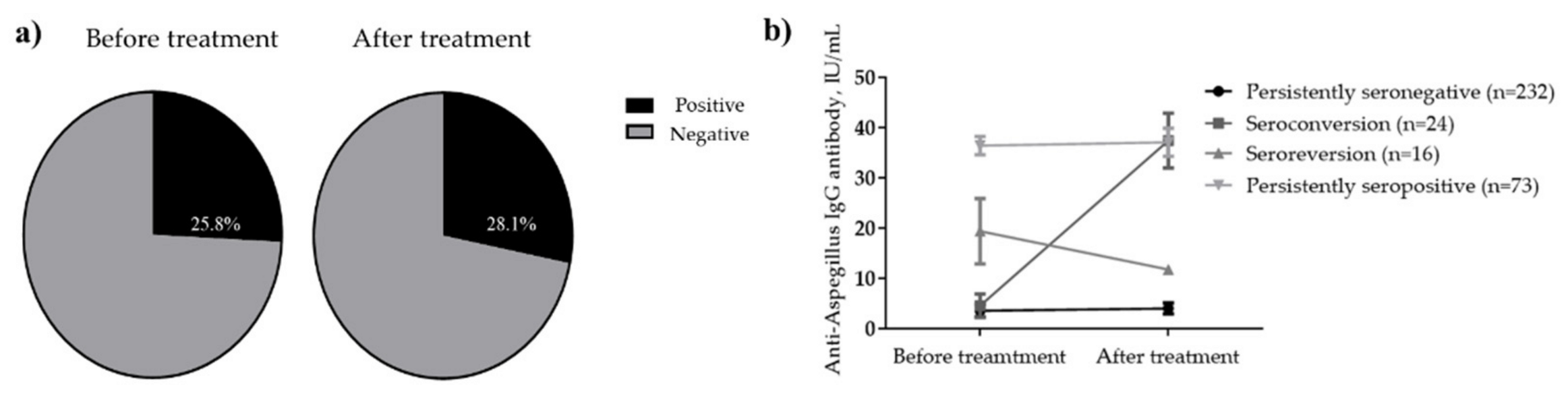
3.2. Serological Changes before and after Treatment of PTB
3.3. Comparison of Clinical Characteristics between Each Serological Group
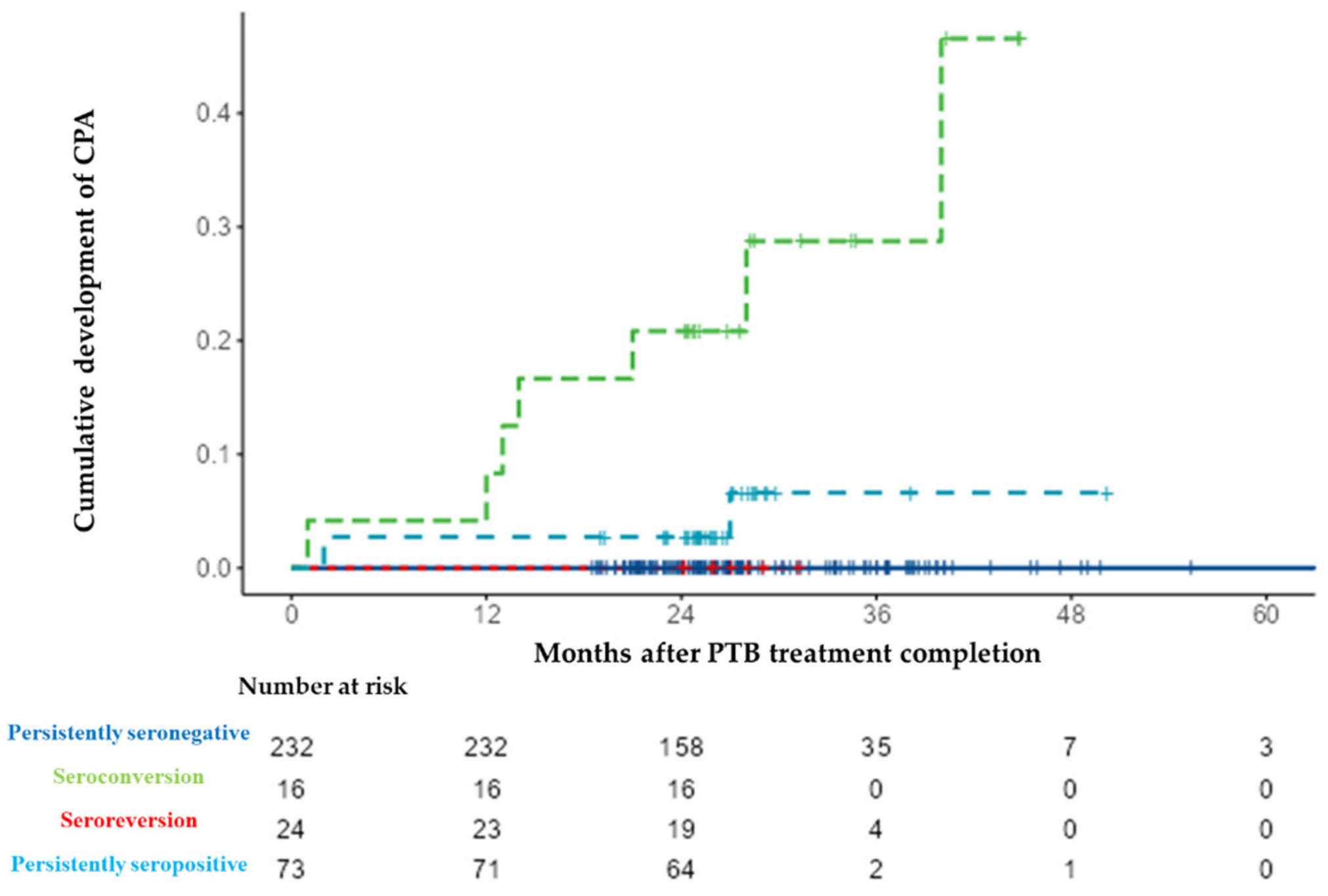
3.4. Follow-Up and Development of CPA according to Serotype
3.5. Risk Factors for Development of CPA after PTB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Oranization. Global Tuberculosis Report 2020. Available online: https://www.who.int/publications/i/item/9789240013131 (accessed on 24 January 2021).
- Allwood, B.W.; Byrne, A.; Meghji, J.; Rachow, A.; van der Zalm, M.M.; Schoch, O.D. Post-Tuberculosis Lung Disease: Clinical Review of an Under-Recognised Global Challenge. Respiration 2021, 100, 751–763. [Google Scholar] [CrossRef] [PubMed]
- Chakraborti, S.; Sarkar, J.; Pramanik, P.K.; Chakraborti, T. Role of proteases in lung disease: A brief overview. Proteases Hum. Dis. 2017, 333–374. [Google Scholar] [CrossRef]
- Allwood, B.W.; van der Zalm, M.M.; Amaral, A.F.S.; Byrne, A.; Datta, S.; Egere, U.; Evans, C.A.; Evans, D.; Gray, D.M.; Hoddinott, G.; et al. Post-tuberculosis lung health: Perspectives from the First International Symposium. Int. J. Tuberc. Lung Dis. 2020, 24, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef]
- Godet, C.; Alastruey-Izquierdo, A.; Flick, H.; Hennequin, C.; Mikilps-Mikgelbs, R.; Munteanu, O.; Page, I.; Seidel, D.; Salzer, H.J.F.; CPAnet. A CPAnet consensus statement on research priorities for chronic pulmonary aspergillosis: A neglected fungal infection that requires attention. J. Antimicrob. Chemother. 2018, 73, 280–286. [Google Scholar] [CrossRef]
- Lowes, D.; Al-Shair, K.; Newton, P.J.; Morris, J.; Harris, C.; Rautemaa-Richardson, R.; Denning, D.W. Predictors of mortality in chronic pulmonary aspergillosis. Eur. Respir. J. 2017, 49, 1601062. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., III; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Oladele, R.; Irurhe, N.; Foden, P.; Akanmu, A.S.; Gbaja-Biamila, T.; Nwosu, A.; Ekundayo, H.; Ogunsola, F.T.; Richardson, M.; Denning, D. Chronic pulmonary aspergillosis as a cause of smear-negative TB and/or TB treatment failure in Nigerians. Int. J. Tuberc. Lung Dis. 2017, 21, 1056–1061. [Google Scholar] [CrossRef]
- Page, I.D.; Byanyima, R.; Hosmane, S.; Onyachi, N.; Opira, C.; Richardson, M.; Sawyer, R.; Sharman, A.; Denning, D.W. Chronic pulmonary aspergillosis commonly complicates treated pulmonary tuberculosis with residual cavitation. Eur. Respir. J. 2019, 53, 1801184. [Google Scholar] [CrossRef]
- Jhun, B.W.; Jeon, K.; Eom, J.S.; Lee, J.H.; Suh, G.Y.; Kwon, O.J.; Koh, W.J. Clinical characteristics and treatment outcomes of chronic pulmonary aspergillosis. Med. Mycol. 2013, 51, 811–817. [Google Scholar] [CrossRef]
- Ohba, H.; Miwa, S.; Shirai, M.; Kanai, M.; Eifuku, T.; Suda, T.; Hayakawa, H.; Chida, K. Clinical characteristics and prognosis of chronic pulmonary aspergillosis. Respir. Med. 2012, 106, 724–729. [Google Scholar] [CrossRef] [Green Version]
- Denning, D.W.; Page, I.D.; Chakaya, J.; Jabeen, K.; Jude, C.M.; Cornet, M.; Alastruey-Izquierdo, A.; Bongomin, F.; Bowyer, P.; Chakrabarti, A.; et al. Case Definition of Chronic Pulmonary Aspergillosis in Resource-Constrained Settings. Emerg. Infect. Dis. 2018, 24, e171312. [Google Scholar] [CrossRef]
- Denning, D.W. Diagnosing pulmonary aspergillosis is much easier than it used to be: A new diagnostic landscape. Int. J. Tuberc. Lung Dis. 2021, 25, 525–536. [Google Scholar] [CrossRef]
- Uffredi, M.L.; Mangiapan, G.; Cadranel, J.; Kac, G. Significance of Aspergillus fumigatus isolation from respiratory specimens of nongranulocytopenic patients. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 457–462. [Google Scholar] [CrossRef]
- Wilopo, B.A.; Richardson, M.D.; Denning, D.W. Diagnostic Aspects of Chronic Pulmonary Aspergillosis: Present and New Directions. Curr. Fungal Infect. Rep. 2019, 13, 292–300. [Google Scholar] [CrossRef] [Green Version]
- Denning, D.W.; Riniotis, K.; Dobrashian, R.; Sambatakou, H. Chronic cavitary and fibrosing pulmonary and pleural aspergillosis: Case series, proposed nomenclature change, and review. Clin. Infect. Dis. 2003, 37 (Suppl. 3), S265–S280. [Google Scholar] [CrossRef] [Green Version]
- Smith, N.L.; Denning, D.W. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur. Respir. J. 2011, 37, 865–872. [Google Scholar] [CrossRef] [Green Version]
- Hedayati, M.T.; Azimi, Y.; Droudinia, A.; Mousavi, B.; Khalilian, A.; Hedayati, N.; Denning, D.W. Prevalence of chronic pulmonary aspergillosis in patients with tuberculosis from Iran. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1759–1765. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. 2017 Annual Report on the Notified Tuberculosis in Korea 2017; Korea Centers for Diseases Control and Prevention: Cheongju, Korea, 2018; pp. 10–52. (In Korean) [Google Scholar]
- Bongomin, F. Post-tuberculosis chronic pulmonary aspergillosis: An emerging public health concern. PLoS Pathog. 2020, 16, e1008742. [Google Scholar] [CrossRef]
- Salzer, H.J.; Cornely, O.A. Awareness of predictors of mortality may help improve outcome in chronic pulmonary aspergillosis. Eur. Respir. J. 2017, 49, 1602520. [Google Scholar] [CrossRef] [Green Version]
- Tuberculosis Association. Aspergilloma and residual tuberculous cavities. The results of a resurvey. Tuber. Lond. 1970, 51, 227–245. [Google Scholar] [CrossRef]
- Agarwal, R.; Denning, D.W.; Chakrabarti, A. Estimation of the burden of chronic and allergic pulmonary aspergillosis in India. PLoS ONE 2014, 9, e114745. [Google Scholar] [CrossRef] [Green Version]
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef]
- Setianingrum, F.; Rozaliyani, A.; Adawiyah, R.; Syam, R.; Tugiran, M.; Sari, C.Y.; Nandipinto, F.; Arifin, A.; Handayani, D.; Burhan, E.; et al. A prospective longitudinal study of chronic pulmonary aspergillosis in pulmonary tuberculosis in Indonesia (APICAL). medRxiv 2021. [Google Scholar] [CrossRef] [PubMed]
- Volpe Chaves, C.E.; do Valle Leone de Oliveira, S.M.; Venturini, J.; Grande, A.J.; Sylvestre, T.F.; Poncio Mendes, R.; Mello Miranda Paniago, A. Accuracy of serological tests for diagnosis of chronic pulmonary aspergillosis: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0222738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwizera, R.; Parkes-Ratanshi, R.; Page, I.D.; Sekaggya-Wiltshire, C.; Musaazi, J.; Fehr, J.; Castelnuovo, B.; Kambugu, A.; Denning, D.W. Elevated Aspergillus-specific antibody levels among HIV infected Ugandans with pulmonary tuberculosis. BMC Pulm. Med. 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Setianingrum, F.; Rozaliyani, A.; Syam, R.; Adawiyah, R.; Tugiran, M.; Sari, C.Y.I.; Burhan, E.; Wahyuningsih, R.; Rautemaa-Richardson, R.; Denning, D.W. Evaluation and comparison of automated and manual ELISA for diagnosis of chronic pulmonary aspergillosis (CPA) in Indonesia. Diagn. Microbiol. Infect. Dis. 2020, 98, 115124. [Google Scholar] [CrossRef] [PubMed]
- Jhun, B.W.; Jung, W.J.; Hwang, N.Y.; Park, H.Y.; Jeon, K.; Kang, E.S.; Koh, W.J. Risk factors for the development of chronic pulmonary aspergillosis in patients with nontuberculous mycobacterial lung disease. PLoS ONE 2017, 12, e0188716. [Google Scholar] [CrossRef]
- Shin, S.H.; Kim, B.-G.; Kang, J.; Um, S.-W.; Kim, H.; Kim, H.K.; Kim, J.; Shim, Y.M.; Choi, Y.S.; Jeong, B.-H. Incidence and Risk Factors of Chronic Pulmonary Aspergillosis Development during Long-Term Follow-Up after Lung Cancer Surgery. J. Fungi 2020, 6, 271. [Google Scholar] [CrossRef]
- Kang, N.; Park, J.; Jhun, B.W. Clinical Characteristics and Treatment Outcomes of Pathologically Confirmed Aspergillus Nodules. J. Clin. Med. 2020, 9, 2185. [Google Scholar] [CrossRef]
- Im, Y.; Jhun, B.W.; Kang, E.-S.; Koh, W.-J.; Jeon, K. Impact of treatment duration on recurrence of chronic pulmonary aspergillosis. J. Infect. 2021, 83, 490–495. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 345) |
|---|---|
| Age, years Male sex, % Height, cm Body weight, kg BMI, kg/m2 | 55.0 (37.0–69.0) 230 (66.7) 166.0 (160.0–171.9) 59.0 (52.3–66.0) 21.6 (19.6–23.8) |
| Comorbidity | |
| COPD or asthma Thyroid disease Cardiovascular disease Malignancy Hematologic disease Chronic liver disease Rheumatic disease CKD Diabetes Neurologic disease Cerebrovascular disease KTP | 46 (13.3) 3 (0.9) 20 (5.8) 12 (3.5) 4 (1.2) 24 (7.0) 13 (3.8) 15 (4.3) 72 (20.9) 10 (2.9) 12 (3.5) 2 (0.6) |
| Combined TB at another site | |
| PTB only PTB with EPTB | 302 (87.5) 43 (12.5) |
| Smoking status | |
| Never smoker Former smoker Current smoker Cessation of smoking after diagnosis of PTB | 150 (43.5) 72 (20.9) 123 (35.7) 71/123 (57.7) |
| Alcohol use (heavy alcoholics) | 21 (9.5) |
| New cases Previously treated cases | 297 (86.1) 48 (13.9) |
| Radiographic features | |
| Cavity (before treatment) Remaining cavity (after treatment) Extent of lung lesion, multilobar involvement | 96 (27.8) 41 (11.9) 166 (48.1) |
| AFB smear status, positive | 129 (37.4) |
| DST profiles | |
| Resistant to INH Resistant to RIF Resistant to INH and RIF | 21 (6.1) 5 (1.4) 2 (0.6) |
| Treatment duration, months | 6.5 (6.1–9.3) |
| Persistently Seronegative (n = 232) | Seroconversion (n = 24) | Seroreversion (n = 24) | Persistently Seropositive (n = 73) | p-Value | |
|---|---|---|---|---|---|
| Age, years Male sex, % Height, cm Body weight, kg BMI, kg/m2, | 57.0 (41.8–73.3) 153 (65.9) 166.0 (159.0–171.0) 58.1 (53.2–64.5) 21.6 (19.5–23.5) | 46.0 (34.0–56.3) 19 (79.2) 166.0 (162.0–172.4) 55.4 (50.5–63.9) 20.3 (17.8–22.9) | 43.5 (27.3–67.8) 11 (68.8) 164.0 (158.2.0–175.3) 59.0 (50.4–80.1) 22.5 (20.4–24.2) | 50.0 (34.0–66.5) 47 (64.4) 167.1 (160.8–174.5) 62.1 (51.9–68.0) 22.0 (20.1–24.7) | 0.003 0.609 0.383 0.118 0.087 |
| before treatment | |||||
| BMI, kg/m2, | 22.2 (20.6–24.5) | 20.8 (19.7–23.5) | 23.2 (20.7–24.4) | 22.6 (20.4–24.7) | 0.221 |
| after treatment | |||||
| AFB smear status, positive | 81 (34.9) | 18 (75.0) | 5 (31.3) | 25 (34.2) | 0.002 |
| Radiographic feature | |||||
| Cavity (before treatment) Cavity (after treatment) | 58 (25.0) 14 (6.0) | 15 (62.5) 9 (37.5) | 1 (6.3) 1 (6.3) | 22 (30.1) 17 (23.3) | <0.001 <0.001 |
| Extent of lung lesion, | |||||
| Multilobar involvement | 110 (47.4) | 20 (83.3) | 7 (43.8) | 29 (39.7) | 0.002 |
| New cases Previously treated cases | 206 (88.8) 26 (11.2) | 23 (95.8) 1 (4.2) | 15 (93.8) 1 (6.3) | 53 (72.6) 20 (27.4) | <0.001 <0.001 |
| Smoking status, | |||||
| ever smoker | 128 (55.2) | 18 (75.0) | 6 (37.5) | 43 (58.9) | 0.111 |
| Seronegative | Seropositive | p-Value | |
|---|---|---|---|
| n = 248 | n = 97 | ||
| Age, years | 57.0 (39.8–73.0) | 49.0 (34.0–62.0) | 0.002 |
| Male sex, % | 164 (66.1) | 66 (68.0) | 0.800 |
| Height, cm | 166.0 (159.0–171.0) | 167.0 (162.0–173.5) | 0.082 |
| Body weight, kg | 58.3 (52.9–64.9) | 60.3 (51.6–68.0) | 0.289 |
| BMI, kg/m2, before treatment | 21.7 (19.6–23.7) | 21.4 (19.5–23.9) | 0.788 |
| BMI, kg/m2, after treatment | 22.2 (20.6–24.5) | 22.4 (20.0–24.7) | 0.536 |
| AFB smear status, positive | 86 (34.7) | 43 (44.3) | 0.108 |
| Radiographic feature | |||
| Cavity (before treatment) | 59 (23.8) | 37 (38.1) | 0.011 |
| Cavity (after treatment) | 15 (6.0) | 26 (26.8) | <0.001 |
| Extent of lung lesion, multilobar involvement | 117 (47.2) | 49 (50.5) | 0.632 |
| New cases | 221 (89.1) | 76 (78.4) | 0.015 |
| Previously treated cases | 27 (10.9) | 21 (21.6) | 0.009 |
| Smoking status, ever smoker | 134 (54.0) | 61 (62.9) | 0.085 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age, years | 1.03 (0.97–1.39) | 0.371 | ||
| BMI, kg/m2 | 1.16 (0.97–1.39) | 0.107 | ||
| AFB smear status, positive | 6.25 (1.32–29.55) | 0.021 | ||
| Cavity (before treatment) | 65,772,095.37 (0.35–infinity) | 0.999 | ||
| Cavity (after treatment) | 731,976,139.68 (0.00–infinity) | 0.998 | ||
| Extent of PTB, multilobar involvement | 2.23 (0.57–8.71) | 0.249 | ||
| Seroconversion | 27.97 (7.11–109.86) | <0.001 | 25.21 (6.11–103.99) | <0.001 |
| Seropositive in treatment completion | 324.70 (0.342–308,700.74) | 0.098 | ||
| Previously treated cases | 1.38 (0.29–6.54) | 0.862 | ||
| Chronic liver disease | 9.05 (2.54–32.19) | 0.003 | ||
| Diabetes | 5.81 (1.64–20.61) | 0.007 | 7.54 (1.93–29.50) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.; Moon, J.-W.; Park, Y.-B.; Ko, Y. Serological Changes in Anti-Aspergillus IgG Antibody and Development of Chronic Pulmonary Aspergillosis in Patients Treated for Pulmonary Tuberculosis. J. Fungi 2022, 8, 130. https://doi.org/10.3390/jof8020130
Kim C, Moon J-W, Park Y-B, Ko Y. Serological Changes in Anti-Aspergillus IgG Antibody and Development of Chronic Pulmonary Aspergillosis in Patients Treated for Pulmonary Tuberculosis. Journal of Fungi. 2022; 8(2):130. https://doi.org/10.3390/jof8020130
Chicago/Turabian StyleKim, Changwhan, Jin-Wook Moon, Yong-Bum Park, and Yousang Ko. 2022. "Serological Changes in Anti-Aspergillus IgG Antibody and Development of Chronic Pulmonary Aspergillosis in Patients Treated for Pulmonary Tuberculosis" Journal of Fungi 8, no. 2: 130. https://doi.org/10.3390/jof8020130
APA StyleKim, C., Moon, J.-W., Park, Y.-B., & Ko, Y. (2022). Serological Changes in Anti-Aspergillus IgG Antibody and Development of Chronic Pulmonary Aspergillosis in Patients Treated for Pulmonary Tuberculosis. Journal of Fungi, 8(2), 130. https://doi.org/10.3390/jof8020130