
Does Post-Transplant Cytomegalovirus Increase the Risk of Invasive Aspergillosis in Solid Organ Transplant Recipients? A Systematic Review and Meta-Analysis

 , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis

{kind=link}
{kind=link}
{kind=link}
| Study | Country | Number of Patients for Analysis | Study Design | Year of the Study | Type of Organ Transplantation | Age (Years) | CMV Definition | CMV Prophylaxis Protocols | Definition of Invasive Aspergillosis | Timing of Aspergillosis Post Transplantation (Days) |
|---|---|---|---|---|---|---|---|---|---|---|
| Desbois 2016 [27] | France | 62 | Case-control study | 2003–2013 | Kidney | IA: median 57.6 (IQR 47.7–68.2) No IA: median 56.8 (IQR 47.9–67.4) | No definition of CMV infection provided | VGCV 1.5 g was administered 4 times per day until 2006, and then VGCV 450 mg daily for 3 to 6 months. | IA was defined according to the EORTC/MSG criteria *. | Median 34 months (range 1–181 months) |
| Fortún 2002 [11] | Spain | 51 | Case-control study | 1994–2000 | Liver | IA: mean (±SD) 51 (±11) No IA: not reported | CMV disease was defined as a compatible picture associated with direct tissue culture or histologic evidence of invasive CMV disease, or when CMV viral syndrome was present; CMV infection was defined by the presence of detectable CMV by antigenemia shell vial culture of blood or by polymerase chain reaction regardless of clinical manifestation. | GCV was administered in CMV mismatch recipients for 14 days. | Proven aspergillosis: tissue histopathology showed septate, acute branching hyphae with or without a positive culture for Aspergillus spp. from the same site, or, in the absence of histopathology, a positive culture from tissue obtained by an invasive procedure- Probable aspergillosis: patients with a pulmonary disease with chest radiographic appearance of new nodules or cavities, and two sputum cultures or one bronchoalveolar lavage, washing, or brushing culture for Aspergillus spp. | Median 126 (range 22–1117) |
| Fortún 2003 [28] | Spain | 280 | Case-control study | 1994–2001 | Liver | Not reported | CMV antigenemia was defined by positive antigenemia >10 cells/200,000. | GCV was administered in CMV mismatch recipients for 14 days, followed by ACV for 3 months. | Proven aspergillosis was assigned when tissue histopathology showed septate, acute branching hyphae with or without a positive culture for Aspergillus spp. from the same site, or, in the absence of histopathology, a positive culture from tissue obtained by an invasive procedure. Probable aspergillosis applied only to patients with a pulmonary disease with chest radiographic appearance of new nodules or cavities, and two sputum cultures or one bronchoalveolar lavage, washing or brushing cultures for Aspergillus spp. In the absence of pulmonary infiltrates, the isolation of Aspergillus spp. in sputum and not confirmed in bronchoalveolar lavage was considered colonization. | Range 1–465 |
| Gavalda 2005 [12] | Spain | 468 | Case-control study | 1990–2001 | Liver, kidney, kidney-pancreas, heart, and lung | IA: mean 52 (range 14–76) No IA: not reported | CMV disease was defined by consistent clinical picture associated with direct tissue culture or histological evidence of invasive CMV disease or CMV syndrome; CMV Infection was defined by detectable CMV by antigen assay and shell vial culture of blood or by PCR, regardless of clinical manifestations. | - | IA was defined according to the EORTC/MSG criteria *; only proven and probable IA was included. | Mean 234 (range 2–3025) |
| He 2013 [29] | China | 28 | Prospective Cohort | 2005–2011 | Lung | Not reported | No definition of CMV infection provided | - | IFI was defined according to the EORTC/MSG criteria *. | Median 211 (40–964) |
| Heylen 2015 [30] | Belgium | 123 | Case-control study | 1995–2013 | Kidney | IA: mean (±SD) 58 (±12) No IA: mean (±SD) 55 (±12) | No definition of CMV infection provided | GCV was given when the recipient and/or donor were CMV seropositive. | IA was defined according to the EORTC/MSG criteria *. | Median 141 (IQR 72–522 days) |
| Husni 1998 [31] | US | 101 | Case-control study | 1990–1995 | Lung | Not reported | CMV pneumonia was defined by recognition of cytomegalic inclusion bodies in tissue; CMV infection was by isolation of CMV from blood (viremia), respiratory secretions (bronchoalveolar lavage fluid), or urine in the absence of recognition of inclusion bodies in tissue. Types of CMV disease associated with IA included CMV pneumonia and CMV retinitis. | Prophylaxis for CMV infection was used for all lung transplant recipients except those with low-risk CMV (D-/R−). | Definitive IA was defined by positive culture along with positive histopathologic evidence of tissue invasion; probable pulmonary IA was defined by a characteristic clinical and radiographic picture with either histopathologic evidence of tissue invasion or culture of a respiratory tract specimen that yielded Aspergillus. | Mean 15 months (range 29 days–5 years) |
| Kato 2014 [32] | Japan | 30 | Retrospective cohort | 2008–2012 | Lung | IA: mean 51.4 (range 35–61) No IA: 44.2 (range 26–62) | No definition of CMV infection provided | - | IA was defined according to the EORTC/MSG criteria *. | Median 307 |
| López-Medrano 2016 [33] | Spain, US, Switzerland, Belgium, Brazil, Portugal, France, Mexico, Argentina, UK | 102 | Case-control study | 2000–2013 | Kidney | IA: mean (±SD) 57.3 (±15.6) No IA: mean (±SD) 54.4 (±14.5) | CMV disease was defined by viral syndrome and probable or definitive end-organ disease. | - | IA was defined according to the EORTC/MSG criteria *. | Median 91 (IQR 65–116) |
| López-Medrano 2018 [34] | Spain, US, Switzerland, Belgium, Brazil, Portugal, France, Mexico, Argentina, UK | 112 | Case-control study | 2000–2013 | Kidney | IA: mean (±SD) 54.6 (±14.2) No IA: mean (±SD) 48.6 (±15.5) | CMV disease was defined by viral syndrome and probable or definitive end-organ disease. | - | IA was defined according to the EORTC/MSG criteria *. | Median 34.4 months (IQR 11.8–78.5 months) |
| Monforte 2001 [35] | Spain | 55 | Retrospective cohort | 1990–1997 | Lung | IA: mean 43.7 (range 15–62) No IA: mean 42.8 (range 21–67) | Diagnosis of CMV infection was based on isolation or detection of the virus from any bodily fluid or tissue specimen or antigenemia; CMV disease included CMV viral syndrome and end-organ involvement; CMV viral syndrome was defined as persistent fever, with or without leukopenia and thrombocytopenia in patients with positive blood culture or antigenemia for CMV; CMV focal disease was defined as the isolation of CMV from any tissue or body fluid plus consistent histologic findings. | GCV was administered for 15 days in all patients post-transplantation. | Aspergillus infection was considered when the patient had clinical symptoms, 2 or more respiratory samples were positive for Aspergillus spp., and at least 1 of these was obtained by bronchoscopy; invasive pulmonary aspergillosis was diagnosed when Aspergillus spp. was found on lung histopathology or radiologic evidence of invasion. | Mean 8.8 months (range 0.3–41 months) |
| Muñoz 2004 [36] | Spain | 278 | Retrospective cohort | 1988–2002 | Heart | IA: mean (±SD) 55 (±8.6) No IA: mean (±SD) 53 (±9.7) | CMV infection was defined by the isolation or detection of the virus from any body fluids by shell vial assay or antigenemia; CMV disease was defined by detection of signs or symptoms attributable to this microorganism and included viral syndrome and CMV focal disease. | Hyperimmunegammaglobulin and GCV were given for 15 days for CMV mismatch recipient (CMV D+/R−). | IA was defined according to the EORTC/MSG criteria *. | Median 50 ± 63 |
| Nagao 2016 [37] | Japan | 279 | Case-control study | 2007–2014 | Liver | IA: mean (±SD) 51.8 (±8.8) No IA: mean (±SD) 53.5 (±10.8) | No definition of CMV infection provided | No routine CMV prophylaxis | IFI was defined according to the EORTC/MSG criteria *. | Median 79.5 (range 8–367) |
| Neofytos 2018 [38] | Switzerland | 2868 | Case-control study | 2008–2014 | Lung, heart, kidney, liver, and combined | IA: mean (±SD) 54.7 (±13.5) No IA: not reported | CMV infection and disease were defined based on the AST guidelines and the CMV definitions in transplant patients for use in a clinical trial. | - | IA was defined according to the EORTC/MSG criteria *. | Median 100 (IQR 15–275) |
| Osawa 2007 [39] | Japan | 430 | Case-control study | 1999–2002 | Liver | IA: mean (±SD) 47.5 (±4.6) No IA: mean (±SD) 44.8 (±11.7) | CMV antigenemia was defined by having at least 1 CMV pp65 antigen-positive cell/50,000 polymorphonuclear cells. | Preemptive GCV was administered in the presence of such CMV infection regardless of clinical manifestations. | IA was defined according to the EORTC/MSG criteria *. | Median 93 (range 14–333) |
| Rosenhagen 2009 [40] | Germany | 170 | Case-control study | 2001–2004 | Liver | IA: mean 54.7 (range 41–63) No IA: not reported | CMV infection was defined by positive pp65 antigenemia or at least 1 positive cell/10,000 leukocytes. | GCV was administered in CMV mismatch recipients. | IA was defined according to the EORTC/MSG criteria *. | Median 25 (range 3–282) |
3. Results
3.1. Study and Patient Characteristics
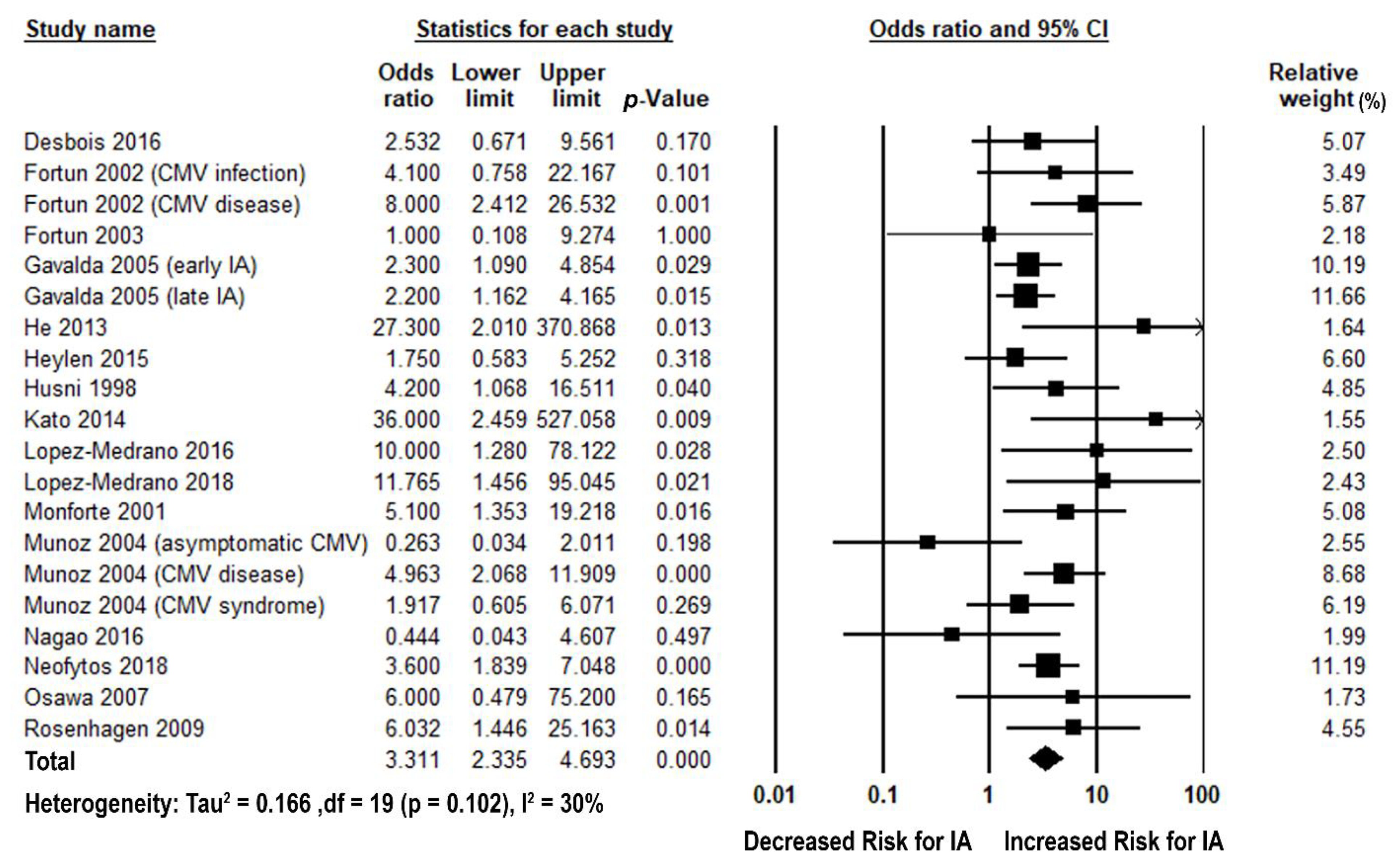
3.2. Cytomegalovirus and Invasive Aspergillosis
| Study | CMV Terminology Used in the Study | Number of Cases | Incidence by Risk Exposure, Number/Total | Confounding Risk Adjustment in Multivariable Analysis | Published Measure of Association | Published Measure of Association between CMV and IA | ||
|---|---|---|---|---|---|---|---|---|
| IA | No IA | Univariable (95% CI) | Multivariable (95% CI) | |||||
| Desbois 2016 [27] | CMV disease | 16 | 5/16 | 7/46 | - | - | - | - |
| Fortún 2002 [11] | CMV infection | 13 | 5/13 | 5/38 | - | OR (IA) | Overall 4.1 (0.78–22.8) Late IA 9.38 (1.21, 89.57) | - |
| CMV disease | 13 | 4/13 | 2/38 | - | OR (IA) | Overall 8.0 (7–77) Late IA 6.38 (0.76–58.0) | - | |
| Fortún 2003 [28] | CMV antigenemia | 13 | 8/13 | 22/118 | - | OR | 1.0 (0.1–8.6) | - |
| Gavalda 2005 [12] | CMV disease | 156 | - | - | The effect of CMV disease for early IA development was adjusted by CMV mismatch, use of vascular amines for >24 h, additional ICU stay, post-transplantation renal failure, post-transplantation hemodialysis, >1 episode of bacterial infection, and OKT3 use | OR (IA) | Early IA 2.1 (1.1–3.8) Late IA 2.2 (1.2–4.3) | Early IA 2.3 (1.1–4.9) Late IA - |
| He 2013 [29] | CMV infection | 8 | 5/7 | 3/21 | - | OR (IA) | 27.3 (2.0–369.1) | - |
| Heylen 2015 [30] | CMV infection | 41 | 8/41 | 12/82 | - | OR (IA) | 1.750 (0.583–5.251) | - |
| Husni 1998 [31] | Cytomegalovirus disease and/or cytomegalovirus infection | 14 | 8/14 | 17/57 | - | OR (IA) | 4.2 (1.1–17) | - |
| Kato 2014 [32] | CMV infection | 5 | 3/5 | 1/25 | - | - | - | - |
| López-Medrano 2016 [33] | CMV disease | 51 | 11/51 | 2/51 | - | OR (IA) | 10.0 (1.28–78.12) | - |
| López-Medrano 2018 [34] | CMV disease | 61 | 10/61 | 1/61 | - | - | - | - |
| Monforte 2001 [35] | CMV disease | 18 | 11/18 | 9/37 | - | OR (IA) | - | 5.1 (1.35–19.17) |
| Muñoz 2004 [36] | Asymptomatic CMV infection | 24 | 1/24 | 36/254 | - | - | - | - |
| CMV disease | 24 | 11/24 | 37/254 | CMV disease was adjusted by re-operation, post-transplant hemodialysis, itraconazole prophylaxis, and another case of IA in the heart transplant program 2 months before or after the transplant date | RR (IA) | - | 5.2 (2–13.9) | |
| CMV syndrome | 24 | 4/24 | 24/254 | - | - | - | - | |
| Nagao 2016 [37] | CMV viremia | 10 | 1/5 | 9/25 | - | - | - | - |
| Neofytos 2018 [38] | CMV infection | - | - | - | - | OR (IA) | 3.6 (1.8–6.9) | - |
| Osawa 2007 [39] | CMV infection | 5 | 4/5 | 4/10 | - | OR (IA) | 6.0 (0.48–75.4) | - |
| Rosenhagen 2009 [40] | CMV infection | 14 | 8/14 | 45/181 | CMV infection was adjusted by dialysis, leukocytopenia, and retransplantation | OR (IA) | - | 6.032 (1.446–25.163) |
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AST IDCOP | American Society of Transplantation Infectious Diseases Community of Practice |
| CI | Confidence interval |
| CMV | Cytomegalovirus |
| EORTC/MSG | European Organization for Research and Treatment of Cancer/Mycoses Study Group |
| HRs | Hazard ratios |
| HSCT | Hematopoietic stem cell transplant recipients |
| IA | Invasive aspergillosis |
| IC | Invasive candidiasis |
| IFI | Invasive fungal infection |
| ORs | Odds ratios |
| PCP | Pneumocystis carinii pneumonia |
| RRs | Relative risks |
| SOT | Solid-organ transplant |
| TRANSNET | Transplant Associated Infection Surveillance Network |
References
- Gandhi, M.K.; Khanna, R. Human cytomegalovirus: Clinical aspects, immune regulation, and emerging treatments. Lancet Infect. Dis. 2004, 4, 725–738. [Google Scholar] [CrossRef]
- Gane, E.; Saliba, F.; Valdecasas, G.J.; O’Grady, J.; Pescovitz, M.D.; Lyman, S.; Robinson, C.A. The Oral Ganciclovir International Transplantation Study Group. Randomised trial of efficacy and safety of oral ganciclovir in the prevention of cytomegalovirus disease in liver-transplant recipients. Lancet 1997, 350, 1729–1733. [Google Scholar] [CrossRef]
- Lowance, D.; Neumayer, H.H.; Legendre, C.M.; Squifflet, J.P.; Kovarik, J.; Brennan, P.J.; Norman, D.; Mendez, R.; Keating, M.R.; Lee, I.C.; et al. International Valacyclovir Cytomegalovirus Prophylaxis Transplantation Study Group. Valacyclovir for the prevention of cytomegalovirus disease after renal transplantation. N. Engl. J. Med. 1999, 340, 1462–1470. [Google Scholar] [CrossRef]
- Razonable, R.R.; Blumberg, E.A. It’s not too late: A proposal to standardize the terminology of “late-onset” cytomegalovirus infection and disease in solid organ transplant recipients. Transpl. Infect. Dis. 2015, 17, 779–784. [Google Scholar] [CrossRef]
- Razonable, R.R.; Humar, A. Cytomegalovirus in solid organ transplant recipients-Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13512. [Google Scholar] [CrossRef] [PubMed]
- Reischig, T.; Jindra, P.; Švecová, M.; Kormunda, S.; Opatrný, K.; Třeška, V. The impact of cytomegalovirus disease and asymptomatic infection on acute renal allograft rejection. J. Clin. Virol. 2006, 36, 146–151. [Google Scholar] [CrossRef]
- Freeman, R.B., Jr. The ‘indirect’ effects of cytomegalovirus infection. Am. J. Transplant. 2009, 9, 2453–2458. [Google Scholar] [CrossRef]
- Kamar, N.; Mengelle, C.; Rostaing, L. Alteration of direct and indirect effects of cytomegalovirus. Exp. Clin. Transplant. 2007, 5, 727–730. [Google Scholar]
- Solano, C.; Navarro, D. Clinical virology of cytomegalovirus infection following hematopoietic transplantation. Future Virol. 2009, 5, 111–124. [Google Scholar] [CrossRef]
- Kusne, S.; Furukawa, H.; Abu-Elmagd, K.; Irish, W.; Rakela, J.; Fung, J.; Starzl, T.E.; Todo, S. Infectious complications after small bowel transplantation in adults: An update. Transplant. Proc. 1996, 28, 2761–2762. [Google Scholar] [PubMed]
- Fortun, J.; Martin-Davila, P.; Moreno, S.; de Vicente, E.; Nuno, J.; Candelas, A.; Barcena, R.; Garcia, M. Risk factors for invasive aspergillosis in liver transplant recipients. Liver Transplant. 2002, 8, 1065–1070. [Google Scholar] [CrossRef]
- Gavalda, J.; Len, O.; San Juan, R.; Aguado, J.M.; Fortun, J.; Lumbreras, C.; Moreno, A.; Munoz, P.; Blanes, M.; Ramos, A.; et al. Risk factors for invasive aspergillosis in solid-organ transplant recipients: A case-control study. Clin. Infect. Dis. 2005, 41, 52–59. [Google Scholar] [CrossRef]
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Ito, J.; et al. Invasive fungal infections among organ transplant recipients: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Farmakiotis, D.; Kontoyiannis, D.P. Emerging issues with diagnosis and management of fungal infections in solid organ transplant recipients. Am. J. Transplant. 2015, 15, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.A.; Gans, H. Pneumocystis jiroveci in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13587. [Google Scholar] [CrossRef] [PubMed]
- Hosseini-Moghaddam, S.M.; Krishnan, R.J.; Guo, H.; Kumar, D. Cytomegalovirus infection and graft rejection as risk factors for pneumocystis pneumonia in solid organ transplant recipients: A systematic review and meta-analysis. Clin. Transplant. 2018, 32, e13339. [Google Scholar] [CrossRef] [PubMed]
- Permpalung, N.; Kittipibul, V.; Mekraksakit, P.; Rattanawong, P.; Nematollahi, S.; Zhang, S.X.; Mehta Steinke, S. A Comprehensive Evaluation of Risk Factors for Pneumocystis Jirovecii Pneumonia in Adult Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis. Transplantation 2020. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ Br. Med. J. 2015, 349, g7647. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2019, 71, 1367–1376. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Published 2019. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 19 March 2021).
- Patsopoulos, N.A.; Evangelou, E.; Ioannidis, J.P. Sensitivity of between-study heterogeneity in meta-analysis: Proposed metrics and empirical evaluation. Int. J. Epidemiol. 2008, 37, 1148–1157. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- The United States Food and Drug Administration (US FDA). Vfend (Voriconazole) Tablets & Injection Approval Letter. Approval Date: 24 May 2002. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2002/21-266_VFEND_Approv.pdf (accessed on 16 December 2020).
- The United States Food and Drug Administration (US FDA). Valcyte (Valganciclovir) Approval Letter. Approval Date: 9 December 2003. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2003/021304_S001_VALCYTE.pdf (accessed on 16 December 2020).
- Desbois, A.C.; Poiree, S.; Snanoudj, R.; Bougnoux, M.E.; Sberro-Soussan, R.; Lanternier, F.; Legendre, C.; Lortholary, O.; Scemla, A. Prognosis of Invasive Aspergillosis in Kidney Transplant Recipients: A Case-Control Study. Transplant. Direct 2016, 2, e90. [Google Scholar] [CrossRef] [PubMed]
- Fortún, J.; Martín-Dávila, P.; Moreno, S.; Bárcena, R.; de Vicente, E.; Honrubia, A.; García, M.; Nuño, J.; Candela, A.; Uriarte, M.; et al. Prevention of invasive fungal infections in liver transplant recipients: The role of prophylaxis with lipid formulations of amphotericin B in high-risk patients. J. Antimicrob. Chemother. 2003, 52, 813–819. [Google Scholar] [CrossRef]
- He, X.; Dai, H.P.; Chen, Q.R.; Miao, J.B.; Sun, B.; Bao, N.; Hu, B.; Li, H.; Wu, A.S.; Ban, C.J.; et al. Pneumonia relevant to lung transplantation and pathogen distribution. Chin. Med. J. 2013, 126, 3209–3214. [Google Scholar]
- Heylen, L.; Maertens, J.; Naesens, M.; Van Wijngaerden, E.; Lagrou, K.; Bammens, B.; Claes, K.; Evenepoel, P.; Meijers, B.; Kuypers, D.; et al. Invasive aspergillosis after kidney transplant: Case-control study. Clin. Infect. Dis. 2015, 60, 1505–1511. [Google Scholar] [CrossRef]
- Husni, R.N.; Gordon, S.M.; Longworth, D.L.; Arroliga, A.; Stillwell, P.C.; Avery, R.K.; Maurer, J.R.; Mehta, A.; Kirby, T. Cytomegalovirus infection is a risk factor for invasive aspergillosis in lung transplant recipients. Clin. Infect. Dis. 1998, 26, 753–755. [Google Scholar] [CrossRef]
- Kato, K.; Nagao, M.; Nakano, S.; Yunoki, T.; Hotta, G.; Yamamoto, M.; Matsumura, Y.; Ito, Y.; Takakura, S.; Chen, F.; et al. Itraconazole prophylaxis for invasive Aspergillus infection in lung transplantation. Transpl. Infect. Dis. 2014, 16, 340–343. [Google Scholar] [CrossRef]
- Lopez-Medrano, F.; Fernandez-Ruiz, M.; Silva, J.T.; Carver, P.L.; van Delden, C.; Merino, E.; Perez-Saez, M.J.; Montero, M.; Coussement, J.; Mazzolin, M.D.; et al. Multinational case-control study of risk factors for the development of late invasive pulmonary aspergillosis following kidney transplantation. Clin. Microbiol. Infect. 2018, 24, 192–198. [Google Scholar] [CrossRef]
- López-Medrano, F.; Silva, J.T.; Fernández-Ruiz, M.; Carver, P.L.; van Delden, C.; Merino, E.; Pérez-Saez, M.J.; Montero, M.; Coussement, J.; de Abreu Mazzolin, M.; et al. Risk Factors Associated With Early Invasive Pulmonary Aspergillosis in Kidney Transplant Recipients: Results From a Multinational Matched Case–Control Study. Am. J. Transplant. 2016, 16, 2148–2157. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Monforte, V.; Roman, A.; Gavalda, J.; Bravo, C.; Tenorio, L.; Ferrer, A.; Maestre, J.; Morell, F. Nebulized amphotericin B prophylaxis for Aspergillus infection in lung transplantation: Study of risk factors. J. Heart Lung Transplant. 2001, 20, 1274–1281. [Google Scholar] [CrossRef]
- Munoz, P.; Rodriguez, C.; Bouza, E.; Palomo, J.; Yanez, J.F.; Dominguez, M.J.; Desco, M. Risk factors of invasive aspergillosis after heart transplantation: Protective role of oral itraconazole prophylaxis. Am. J. Transplant. 2004, 4, 636–643. [Google Scholar] [CrossRef]
- Nagao, M.; Fujimoto, Y.; Yamamoto, M.; Matsumura, Y.; Kaido, T.; Takakura, S.; Uemoto, S.; Ichiyama, S. Epidemiology of invasive fungal infections after liver transplantation and the risk factors of late-onset invasive aspergillosis. J. Infect. Chemother. 2016, 22, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Neofytos, D.; Chatzis, O.; Nasioudis, D.; Boely Janke, E.; Doco Lecompte, T.; Garzoni, C.; Berger, C.; Cussini, A.; Boggian, K.; Khanna, N.; et al. Epidemiology, risk factors and outcomes of invasive aspergillosis in solid organ transplant recipients in the Swiss Transplant Cohort Study. Transpl. Infect. Dis. 2018, 20, e12898. [Google Scholar] [CrossRef]
- Osawa, M.; Ito, Y.; Hirai, T.; Isozumi, R.; Takakura, S.; Fujimoto, Y.; Iinuma, Y.; Ichiyama, S.; Tanaka, K.; Mishima, M. Risk factors for invasive aspergillosis in living donor liver transplant recipients. Liver Transplant. 2007, 13, 566–570. [Google Scholar] [CrossRef]
- Rosenhagen, M.; Feldhues, R.; Schmidt, J.; Hoppe-Tichy, T.; Geiss, H.K. A Risk Profile for Invasive Aspergillosis in Liver Transplant Recipients. Infection 2009, 37, 313–319. [Google Scholar] [CrossRef]
- Singh, N.; Avery, R.K.; Munoz, P.; Pruett, T.L.; Alexander, B.; Jacobs, R.; Tollemar, J.G.; Dominguez, E.A.; Yu, C.M.; Paterson, D.L.; et al. Trends in risk profiles for and mortality associated with invasive aspergillosis among liver transplant recipients. Clin. Infect. Dis. 2003, 36, 46–52. [Google Scholar] [CrossRef]
- Brown, R.S.J.; Lake, J.R.; Katzman, B.A.; Ascher, N.L.; Somberg, K.A.; Emond, J.C.; Roberts, J.P. Incidence and significance of aspergillus cultures following liver and kidney transplantation. Transplantation 1996, 61, 666–669. [Google Scholar] [CrossRef]
- Paterson, D.L.; Singh, N. Invasive aspergillosis in transplant recipients. Medicine 1999, 78, 123–138. [Google Scholar] [CrossRef]
- Atalla, A.; Garnica, M.; Maiolino, A.; Nucci, M. Risk factors for invasive mold diseases in allogeneic hematopoietic cell transplant recipients. Transpl. Infect. Dis. 2015, 17, 7–13. [Google Scholar] [CrossRef] [PubMed]
- George, M.J.; Snydman, D.R.; Werner, B.G.; Griffith, J.; Falagas, M.E.; Dougherty, N.N.; Rubin, R.H. The independent role of cytomegalovirus as a risk factor for invasive fungal disease in orthotopic liver transplant recipients. Boston Center for Liver Transplantation CMVIG-Study Group. Cytogam, MedImmune, Inc. Gaithersburg, Maryland. Am. J. Med. 1997, 103, 106–113. [Google Scholar] [CrossRef]
- Salzberger, B.; Bowden, R.A.; Hackman, R.C.; Davis, C.; Boeckh, M. Neutropenia in Allogeneic Marrow Transplant Recipients Receiving Ganciclovir for Prevention of Cytomegalovirus Disease: Risk Factors and Outcome. Blood 1997, 90, 2502–2508. [Google Scholar] [CrossRef]
- Venton, G.; Crocchiolo, R.; Fürst, S.; Granata, A.; Oudin, C.; Faucher, C.; Coso, D.; Bouabdallah, R.; Berger, P.; Vey, N.; et al. Risk factors of Ganciclovir-related neutropenia after allogeneic stem cell transplantation: A retrospective monocentre study on 547 patients. Clin. Microbiol. Infect. 2014, 20, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Laursen, A.L.; Mogensen, S.C.; Andersen, H.M.; Andersen, P.L.; Ellermann-Eriksen, S. The impact of CMV on the respiratory burst of macrophages in response to Pneumocystis carinii. Clin. Exp. Immunol. 2001, 123, 239–246. [Google Scholar] [CrossRef]
- Bochud, P.-Y.; Chien, J.W.; Marr, K.A.; Leisenring, W.M.; Upton, A.; Janer, M.; Rodrigues, S.D.; Li, S.; Hansen, J.A.; Zhao, L.P.; et al. Toll-like receptor 4 polymorphisms and aspergillosis in stem-cell transplantation. N. Engl. J. Med. 2008, 359, 1766–1777. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chuleerarux, N.; Thongkam, A.; Manothummetha, K.; Nematollahi, S.; Dioverti-Prono, V.; Torvorapanit, P.; Langsiri, N.; Worasilchai, N.; Plongla, R.; Chindamporn, A.; et al. Does Post-Transplant Cytomegalovirus Increase the Risk of Invasive Aspergillosis in Solid Organ Transplant Recipients? A Systematic Review and Meta-Analysis. J. Fungi 2021, 7, 327. https://doi.org/10.3390/jof7050327
Chuleerarux N, Thongkam A, Manothummetha K, Nematollahi S, Dioverti-Prono V, Torvorapanit P, Langsiri N, Worasilchai N, Plongla R, Chindamporn A, et al. Does Post-Transplant Cytomegalovirus Increase the Risk of Invasive Aspergillosis in Solid Organ Transplant Recipients? A Systematic Review and Meta-Analysis. Journal of Fungi. 2021; 7(5):327. https://doi.org/10.3390/jof7050327
Chicago/Turabian StyleChuleerarux, Nipat, Achitpol Thongkam, Kasama Manothummetha, Saman Nematollahi, Veronica Dioverti-Prono, Pattama Torvorapanit, Nattapong Langsiri, Navaporn Worasilchai, Rongpong Plongla, Ariya Chindamporn, and et al. 2021. "Does Post-Transplant Cytomegalovirus Increase the Risk of Invasive Aspergillosis in Solid Organ Transplant Recipients? A Systematic Review and Meta-Analysis" Journal of Fungi 7, no. 5: 327. https://doi.org/10.3390/jof7050327
APA StyleChuleerarux, N., Thongkam, A., Manothummetha, K., Nematollahi, S., Dioverti-Prono, V., Torvorapanit, P., Langsiri, N., Worasilchai, N., Plongla, R., Chindamporn, A., Sanguankeo, A., & Permpalung, N. (2021). Does Post-Transplant Cytomegalovirus Increase the Risk of Invasive Aspergillosis in Solid Organ Transplant Recipients? A Systematic Review and Meta-Analysis. Journal of Fungi, 7(5), 327. https://doi.org/10.3390/jof7050327