
Clinical Outcomes of Radical Surgery and Antimicrobial Agents in Vascular Pythiosis: A Multicenter Prospective Study

 ,
,  , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients and Study Design
2.2. Beta-d-Glucan, Erythrocyte Sedimentation Rate, and C-Reactive Protein
2.3. In Vitro Susceptibility
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics and Treatment Modalities
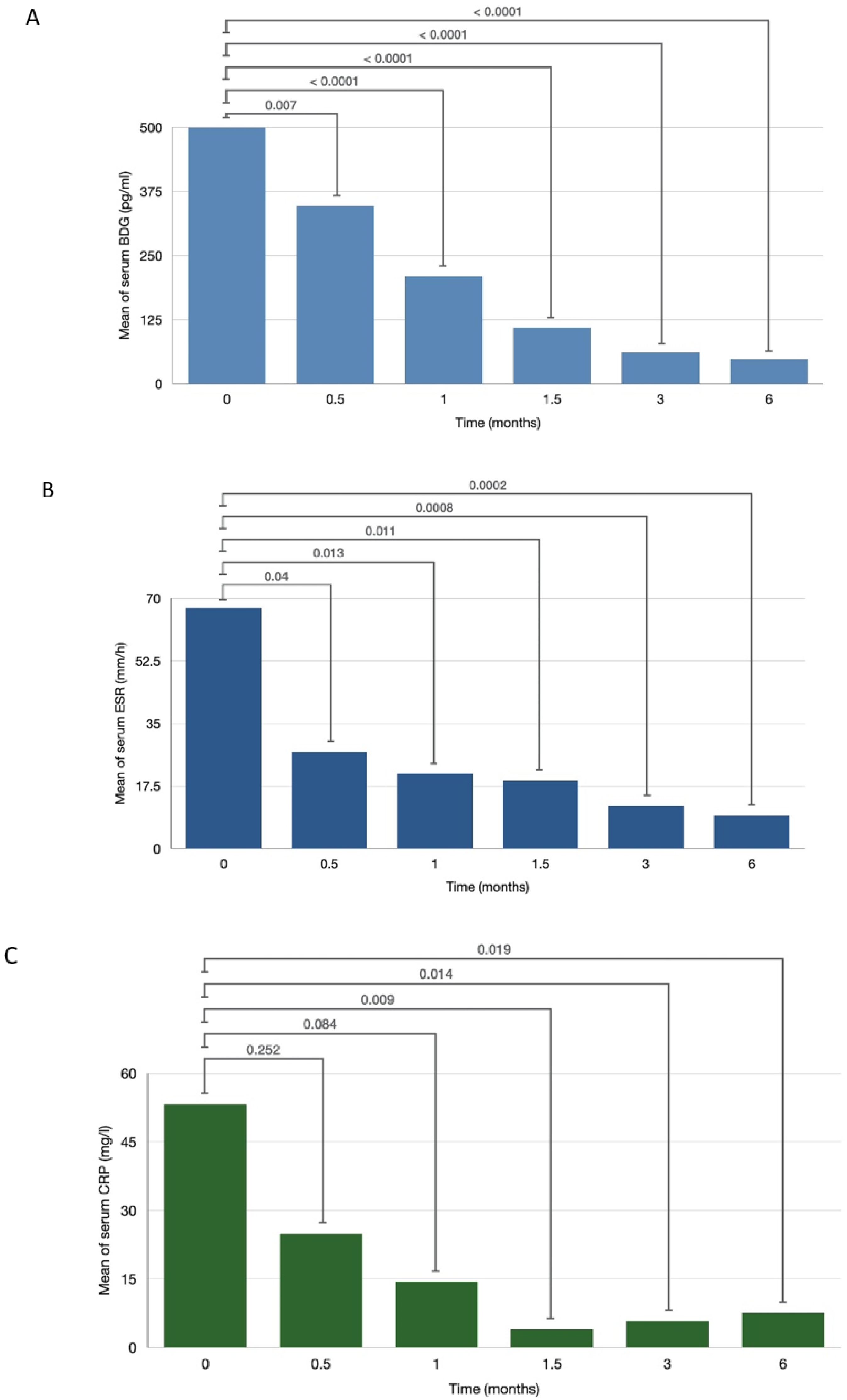
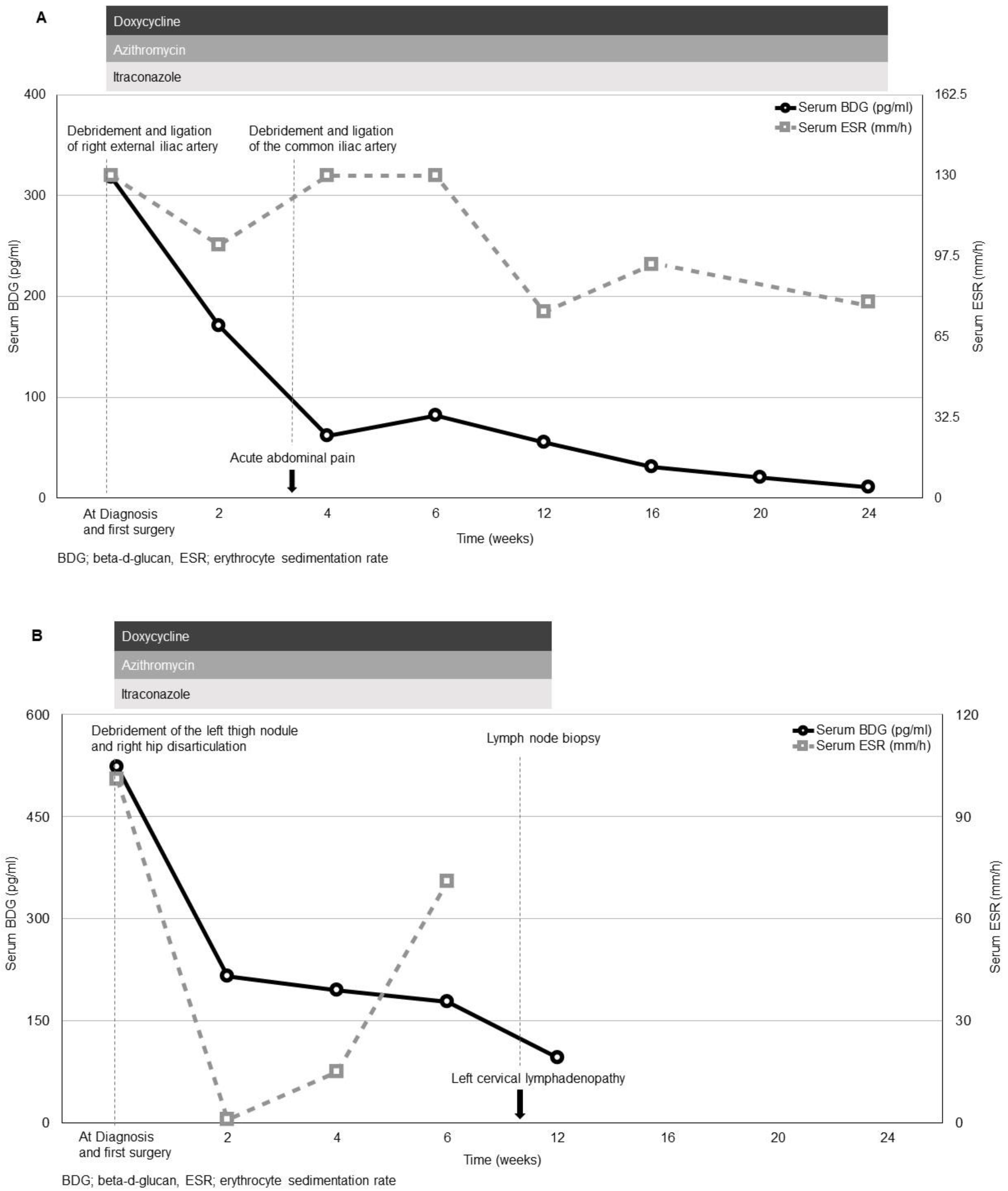
3.2. Serum Beta-d-Glucan, Erythrocyte Sedimentation Rate and C-Reactive Protein
3.3. In Vitro Susceptibility
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sathapatayavongs, B.; Leelachaikul, P.; Prachaktam, R.; Atichartakarn, V.; Sriphojanart, S.; Trairatvorakul, P.; Jirasiritham, S.; Nontasut, S.; Eurvilaichit, C.; Flegel, T. Human pythiosis associated with thalassemia hemoglobinopathy syndrome. J. Infect. Dis. 1989, 159, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Krajaejun, T.; Sathapatayavongs, B.; Pracharktam, R.; Nitiyanant, P.; Leelachaikul, P.; Wanachiwanawin, W.; Chaiprasert, A.; Assanasen, P.; Saipetch, M.; Mootsikapun, P.; et al. Clinical and epidemiological analyses of human pythiosis in Thailand. Clin. Infect. Dis. 2006, 43, 569–576. [Google Scholar] [CrossRef]
- Triscott, J.A.; Weedon, D.; Cabana, E. Human subcutaneous pythiosis. J. Cutan. Pathol. 1993, 20, 267–271. [Google Scholar] [CrossRef]
- HHe, H.; Liu, H.; Chen, X.; Wu, J.; He, M.; Zhong, X. Diagnosis and Treatment of Pythium Insidiosum Corneal Ulcer in a Chinese Child: A Case Report and Literature Review. Am. J. Case Rep. 2016, 17, 982–988. [Google Scholar] [CrossRef]
- Hilton, R.; Tepedino, K.; Glenn, C.J.; Merkel, K.L. Swamp cancer: A case of human pythiosis and review of the literature. Br. J. Dermatol. 2016, 175, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.; Leddin, D. Keratitis caused by Pythium insidiosum in an immunosuppressed patient with Crohn’s disease. Clin. Gastroenterol. Hepatol. 2014, 12, A21–A22. [Google Scholar] [CrossRef] [PubMed]
- FFranco, D.M.; Aronson, J.F.; Hawkins, H.K.; Gallagher, J.J.; Mendoza, L.; McGinnis, M.R.; Williams-Bouyer, N. Systemic Pythium insidiosum in a pediatric burn patient. Burn J. Int. Soc. Burn Inj. 2010, 36, e68–e71. [Google Scholar] [CrossRef]
- Bosco, S.; Bagagli, E.; Araújo, J.P.; Candeias, J.M., Jr.; de Franco, M.F.; Alencar Marques, M.E.; Mendoza, L.; de Camargo, R.P.; Alencar Marques, S. Human pythiosis, Brazil. Emerg. Infect. Dis. 2005, 11, 715–718. [Google Scholar] [CrossRef]
- Tanhehco, T.Y.; Stacy, R.C.; Mendoza, L.; Durand, M.L.; Jakobiec, F.A.; Colby, K.A. Pythium insidiosum keratitis in Israel. Eye Contact Lens Sci. Clin. Pract. 2011, 37, 96–98. [Google Scholar] [CrossRef]
- Permpalung, N.; Worasilchai, N.; Plongla, R.; Upala, S.; Sanguankeo, A.; Paitoonpong, L.; Mendoza, L.; Chindamporn, A. Treatment outcomes of surgery, antifungal therapy and immunotherapy in ocular and vascular human pythiosis: A retrospective study of 18 patients. J. Antimicrob. Chemother. 2015, 70. [Google Scholar] [CrossRef] [PubMed]
- Reanpang, T.; Orrapin, S.; Orrapin, S.; Arworn, S.; Kattipatanapong, T.; Srisuwan, T.; Vanittanakom, N.; Lekawanvijit, S.P.; Rerkasem, K. Vascular Pythiosis of the Lower Extremity in Northern Thailand: Ten Years’ Experience. Int. J. Low Extrem. Wounds. 2015, 14, 245–250. [Google Scholar] [CrossRef]
- Sermsathanasawadi, N.; Praditsuktavorn, B.; Hongku, K.; Wongwanit, C.; Chinsakchai, K.; Ruangsetakit, C.; Hahtapornsawan, S.; Mutirangura, P. Outcomes and factors influencing prognosis in patients with vascular pythiosis. J. Vasc. Surg. 2016, 64, 411–417. [Google Scholar] [CrossRef]
- Worasilchai, N.; Permpalung, N.; Chongsathidkiet, P.; Leelahavanichkul, A.; Mendoza, A.L.; Palaga, T.; Reantragoon, R.; Finkelman, M.; Sutcharitchan, P.; Chindamporn, A. Monitoring Anti-Pythium insidiosum IgG Antibodies and (1→3)-β-d-Glucan in Vascular Pythiosis. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef]
- Permpalung, N.; Worasilchai, N.; Chindamporn, A. Human Pythiosis: Emergence of Fungal-Like Organism. Mycopathologia 2020, 185, 801–812. [Google Scholar] [CrossRef]
- de Sousa, M. Immune cell functions in iron overload. Clin. Exp. Immunol. 1989, 75, 1–6. [Google Scholar]
- Gordeuk, V.R.; Ballou, S.; Lozanski, G.; Brittenham, G.M. Decreased concentrations of tumor necrosis factor-alpha in supernatants of monocytes from homozygotes for hereditary hemochromatosis. Blood 1992, 79, 1855–1860. [Google Scholar] [CrossRef] [PubMed]
- Krajaejun, T.; Khositnithikul, R.; Lerksuthirat, T.; Lowhnoo, T.; Rujirawat, T.; Petchthong, T.; Yingyong, W.; Suriyaphol, P.; Smittipat, N.; Juthayothin, T.; et al. Expressed sequence tags reveal genetic diversity and putative virulence factors of the pathogenic oomycete Pythium insidiosum. Fungal Biol. 2011, 115, 683–696. [Google Scholar] [CrossRef] [PubMed]
- Argenta, J.S.; Alves, S.H.; Silveira, F.; Maboni, G.; Zanette, R.A.; Cavalheiro, A.S.; Pereira, P.L.; Pereira, D.I.; Sallis, E.S.; Pötter, L.; et al. In vitro and in vivo susceptibility of two-drug and three-drug combinations of terbinafine, itraconazole, caspofungin, ibuprofen and fluvastatin against Pythium insidiosum. Vet. Microbiol. 2012, 157, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Cavalheiro, A.S.; Maboni, G.; De Azevedo, M.I.; Argenta, J.S.; Pereira, D.I.B.; Spader, T.B.; Alves, S.H.; Santurio, J.M. In Vitro activity of terbinafine combined with caspofungin and azoles against Pythium insidiosum. Antimicrob. Agents Chemother. 2009, 53, 2136–2138. [Google Scholar] [CrossRef]
- Shenep, J.L.; English, B.K.; Kaufman, L.; Pearson, T.A.; Thompson, J.W.; Kaufman, R.A.; Frisch, G.; Rinaldi, M.G. Successful medical therapy for deeply invasive facial infection due to Pythium insidiosum in a child. Clin. Infect. Dis. 1998, 27, 1388–1393. [Google Scholar] [CrossRef]
- Permpalung, N.; Worasilchai, N.; Manothummetha, K.; Torvorapanit, P.; Ratanawongphaibul, K.; Chuleerarux, N.; Plongla, R.; Chindamporn, A. Clinical outcomes in ocular pythiosis patients treated with a combination therapy protocol in Thailand: A prospective study. Med. Mycol. 2019, 57, 923–928. [Google Scholar] [CrossRef]
- Worasilchai, N.; Chindamporn, A.; Plongla, R.; Torvorapanit, P.; Manothummetha, K.; Chuleerarux, N.; Permpalung, N. In Vitro Susceptibility of Thai Pythium insidiosum Isolates to Antibacterial Agents. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef]
- Susaengrat, N.; Torvorapanit, P.; Plongla, R.; Chuleerarux, N.; Manothummetha, K.; Tuangsirisup, J.; Worasilchai, N.; Chindamporn, A.; Permpalung, N. Adjunctive antibacterial agents as a salvage therapy in relapsed vascular pythiosis patients. Int. J. Infect. Dis. 2019, 88, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Vilela, R.; Mendoza, L. Lacazia, Lagenidium, Pythium, and Rhinosporidium. In Manual of Clinical Microbiology; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015; pp. 2196–2208. [Google Scholar] [CrossRef]
- Chindamporn, A.; Vilela, R.; Hoag, K.A.; Mendoza, L. Antibodies in the sera of host species with pythiosis recognize a variety of unique immunogens in geographically divergent Pythium insidiosum strains. Clin. Vaccine Immunol. 2008, 16, 330–336. [Google Scholar] [CrossRef]
- Krajaejun, T.; Kunakorn, M.; Niemhom, S.; Chongtrakool, P.; Pracharktam, R. Development and evaluation of an in-house enzyme-linked immunosorbent assay for early diagnosis and monitoring of human pythiosis. Clin. Vaccine Immunol. 2002, 9, 378–382. [Google Scholar] [CrossRef]
- Worasilchai, N.; Chaumpluk, P.; Chakrabarti, A.; Chindamporn, A. Differential diagnosis for pythiosis using thermophilic helicase DNA amplification and restriction fragment length polymorphism (tHDA-RFLP). Med. Mycol. 2017, 56, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Worasilchai, N.; Permpalung, N.; Chindamporn, A. High-resolution melting analysis: A novel approach for clade differentiation in Pythium insidiosum and pythiosis. Med. Mycol. 2017, 56, 868–876. [Google Scholar] [CrossRef]
- Kammarnjesadakul, P.; Palaga, T.; Sritunyalucksana, K.; Mendoza, L.; Krajaejun, T.; Vanittanakom, N.; Tongchusak, S.; Denduangboripant, J.; Chindamporn, A. Phylogenetic analysis of Pythium insidiosum Thai strains using cytochrome oxidase II (COX II) DNA coding sequences and internal transcribed spacer regions (ITS). Med. Mycol. 2011, 49, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Pickering, J.W.; Sant, H.W.; Bowles, C.A.P.; Roberts, W.L.; Woods, G.L. Evaluation of a (1->3)-beta-D-glucan assay for diagnosis of invasive fungal infections. J. Clin. Microbiol. J. Clin. Microbiol. 2005, 43, 5957–5962. [Google Scholar] [CrossRef]
- Tran, T.; Beal, S.G. Application of the 1,3-β-D-Glucan (Fungitell) Assay in the Diagnosis of Invasive Fungal Infections. Arch. Pathol. Lab. Med. 2016, 140, 181–185. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi, Approved Standard, 3rd ed.; Document M45; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017. [Google Scholar]
- Jesus, F.P.K.; Loreto, E.S.; Ferreiro, L.; Alves, S.H.; Driemeier, D.; Souza, S.O.; França, R.T.; Lopes, S.T.A.; Pilotto, M.B.; Ludwig, A.; et al. In Vitro and In Vivo Antimicrobial Activities of Minocycline in Combination with Azithromycin, Clarithromycin, or Tigecycline against Pythium insidiosum. Antimicrob. Agents Chemother. 2016, 60, 87–91. [Google Scholar] [CrossRef]
- Loreto, É.S.; Mario, D.A.N.; Denardi, L.B.; Alves, S.H.; Santurio, J.M. In vitro susceptibility of Pythium insidiosum to macrolides and tetracycline antibiotics. Antimicrob. Agents Chemother. 2011, 55, 3588–3590. [Google Scholar] [CrossRef] [PubMed]
- Mahl, D.L.; De Jesus, F.P.K.; Loreto, É.S.; Zanette, R.A.; Ferreiro, L.; Ben Pilotto, M.; Alves, S.H.; Santurio, J.M. In vitro susceptibility of Pythium insidiosum isolates to aminoglycoside antibiotics and tigecycline. Antimicrob. Agents Chemother. 2012, 56, 4021–4023. [Google Scholar] [CrossRef]
- Jensen, A.G.; Espersen, F.; Skinhøj, P.; Frimodt-Møller, N. Bacteremic Staphylococcus aureus spondylitis. Arch. Intern. Med. 1998, 158, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Siemionow, K.; Steinmetz, M.; Bell, G.; Ilaslan, H.; McLain, R.F. Identifying serious causes of back pain: Cancer, infection, fracture. Clevel. Clin. J. Med. 2008, 75, 557–566. [Google Scholar] [CrossRef]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, J.V.G.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef]
- Berbari, E.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M.; Petermann, G.W.; et al. Executive Summary: 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin. Infect. Dis. 2015, 61, 859–863. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Case | Age (Years) /Sex | Occupation | Clinical Presentations | Arterial Involvement | Surgery | Duration from First Medical Visit to Surgery (Days) | Free Surgical Margins Achievement | Antimicrobial Agents | Follow-Up Duration (Months) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 53/M | Farmer | Left leg pain 2 weeks | Left popliteal artery | Left AKA | 5 | No | Itraconazole Azithromycin | 6 |
| 2 | 52/M | Driver | Right leg pain, groin mass, cold skin, numbness 3 days | Right common iliac artery | Right AKA | 5 | No | Itraconazole Azithromycin Doxycycline | 6 |
| 3 | 69/M | Farmer | Left leg pain 2 weeks | Left tibial artery and left popliteal artery | Left AKA | 5 | Yes | Itraconazole Azithromycin | 6 |
| 4 | 34/M | Merchant | Right ankle swelling and tenderness 2 days | Right popliteal artery | Right BKA | 25 | Yes | Itraconazole Azithromycin | 8 |
| 5 | 50/F | Farmer | Right leg chronic wound 2 months | Right popliteal artery | Right BKA | 21 | Yes | Itraconazole Azithromycin | 8 |
| 6 | 53/M | Farmer | Left leg pain 1 day | Left femoral artery | Left AKA | 1 | Yes | Itraconazole Azithromycin Doxycycline | 6 |
| 7 | 49/M | Security guard | Left leg chronic wound 3 years | Cutaneous vessels | Left wide excision | 11 | Yes | Itraconazole Azithromycin Doxycycline | 6 |
| 8 | 45/M | Merchant | Right leg pain and chronic wound 2 months | Right femoral artery | Ligation of right external iliac artery | 6 | Yes | Itraconazole Azithromycin Doxycycline | 6 |
| 9 | 51/M | Potter | Right leg pain 2 months | Right femoral artery | Right hip disarticulation | 60 | No | Itraconazole Azithromycin Doxycycline | 5 |
| 10 | 53/M | Farmer | Left leg pain 2 months | Left anterior tibial artery | Left AKA | 7 | Yes | Itraconazole Azithromycin Doxycycline | 6 |
| Minimum Inhibitory Concentrations (mg/L) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Case 1 | Case 2 | Case 3 | Case 5 | Case 6 | Case 8 | Case 9 | Case 10 | ||
| Tetracyclines | Doxycycline | 4 | 1 | 4 | 2 | 2 | 4 | 4 | 2 |
| Minocycline | 1 | 1 | 0.5 | 1 | 0.25 | 1 | 1 | 2 | |
| Tigecycline | 1 | 1 | 0.5 | 1 | 1 | 1 | 2 | 1 | |
| Macrolides | Azithromycin | 4 | 2 | 2 | 2 | 2 | 2 | 2 | 4 |
| Clarithromycin | 2 | 1 | 1 | 1 | 0.125 | 1 | 2 | 1 | |
| Beta-lactams | Cefazolin | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 |
| ceftriaxone | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 | |
| Ceftazidime | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 | |
| Meropenem | 32 | 32 | >32 | 32 | 32 | >32 | >32 | >32 | |
| Oxazolidinone | Linezolid | 4 | 8 | 4 | 8 | 4 | 4 | 8 | 4 |
| Glycopeptide | Vancomycin | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 |
| Aminoglycosides | Amikacin | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 |
| Gentamicin | 32 | >32 | 16 | 32 | >32 | >32 | >32 | >32 | |
| Neomycin | 32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 | |
| Streptomycin | 32 | >32 | >32 | 32 | 32 | 16 | >32 | 32 | |
| Tobramycin | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 | |
| Quinolones | Ciprofloxacin | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 |
| Levofloxacin | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 | |
| Moxifloxacin | 32 | 16 | >32 | 16 | 32 | 32 | >32 | 16 | |
| Polymyxins | Colistin (Polymyxin E) | 8 | 8 | 4 | 8 | >32 | 16 | 16 | 16 |
| Polymyxin B | >32 | >32 | >32 | >32 | >32 | >32 | >32 | >32 | |
| Combination | Azithromycin/Minocycline | S | S | S | S | S | S | S | S |
| Azithromycin/Tigecycline | S | S | S | S | S | S | S | S | |
| Clarithromycin/Minocycline | S | S | S | S | S | S | S | S | |
| Clarithromycin/Tigecycline | S | S | S | S | S | S | S | S | |
| Minocycline/Tigecycline | S | S | S | S | S | S | S | S | |
| Doxycycline/Azithromycin | S | S | S | S | S | S | S | S | |
| Doxycycline/Clarithromycin | S | S | S | S | S | S | S | S | |
| Doxycycline/Tigecycline | S | S | S | S | S | S | S | S | |
| Antifungal agents | Amphotericin B | 4 | 8 | 8 | 8 | 8 | 8 | 4 | 4 |
| Voriconazole | 2 | 4 | 2 | 2 | 4 | 4 | 8 | 4 | |
| Itraconazole | 2 | 2 | 1 | 1 | 2 | 2 | 4 | 4 | |
| Fluconazole | 2 | 4 | 2 | 2 | 4 | 2 | 4 | 8 | |
| Anidulafungin | 4 | 2 | 4 | 8 | 4 | 2 | 8 | 8 | |
| Caspofungin | 4 | 2 | 4 | 4 | 4 | 2 | 4 | 8 | |
| Terbinafine | 2 | 4 | 2 | 2 | 4 | 2 | 4 | 4 | |
| Voriconazole/Terbinafine | I | I | I | I | I | I | I | I | |
| Itraconazole/Terbinafine | I | I | I | I | I | I | I | I | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torvorapanit, P.; Chuleerarux, N.; Plongla, R.; Worasilchai, N.; Manothummetha, K.; Thongkam, A.; Langsiri, N.; Diewsurin, J.; Kongsakpaisan, P.; Bansong, R.; et al. Clinical Outcomes of Radical Surgery and Antimicrobial Agents in Vascular Pythiosis: A Multicenter Prospective Study. J. Fungi 2021, 7, 114. https://doi.org/10.3390/jof7020114
Torvorapanit P, Chuleerarux N, Plongla R, Worasilchai N, Manothummetha K, Thongkam A, Langsiri N, Diewsurin J, Kongsakpaisan P, Bansong R, et al. Clinical Outcomes of Radical Surgery and Antimicrobial Agents in Vascular Pythiosis: A Multicenter Prospective Study. Journal of Fungi. 2021; 7(2):114. https://doi.org/10.3390/jof7020114
Chicago/Turabian StyleTorvorapanit, Pattama, Nipat Chuleerarux, Rongpong Plongla, Navaporn Worasilchai, Kasama Manothummetha, Achitpol Thongkam, Nattapong Langsiri, Jaruwan Diewsurin, Prasopchai Kongsakpaisan, Ratiporn Bansong, and et al. 2021. "Clinical Outcomes of Radical Surgery and Antimicrobial Agents in Vascular Pythiosis: A Multicenter Prospective Study" Journal of Fungi 7, no. 2: 114. https://doi.org/10.3390/jof7020114
APA StyleTorvorapanit, P., Chuleerarux, N., Plongla, R., Worasilchai, N., Manothummetha, K., Thongkam, A., Langsiri, N., Diewsurin, J., Kongsakpaisan, P., Bansong, R., Susaengrat, N., Wattanasoontornsakul, W., Chindamporn, A., & Permpalung, N. (2021). Clinical Outcomes of Radical Surgery and Antimicrobial Agents in Vascular Pythiosis: A Multicenter Prospective Study. Journal of Fungi, 7(2), 114. https://doi.org/10.3390/jof7020114