Recurrent Vulvovaginal Candidosis and Cluster Analysis of Clinical Signs and Symptoms: A Laboratory-Based Investigation

 ,
,  ,
, 


Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Characteristics and Quality of Life (QoL) Assessment
2.2. Statistical Analysis
3. Results
Patients Characteristics and Laboratory Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Sobel, J.D. Vulvovaginal candidosis. Lancet 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- Bitew, A.; Abebaw, Y. Vulvovaginal candidiasis: Species distribution of Candida and their antifungal susceptibility pattern. BMC Womens Health 2018, 18, 9. [Google Scholar] [CrossRef] [PubMed]
- Cauchie, M.; Desmet, S.; Lagrou, K. Candida and its dual lifestyle as a commensal and a pathogen. Res. Microbiol. 2017, 168, 802–810. [Google Scholar] [CrossRef]
- Drell, T.; Lillsaar, T.; Tummeleht, L.; Simm, J.; Aaspõllu, A.; Väin, E.; Saarma, I.; Salumets, A.; Donders, G.G.G.; Metsis, M. Characterization of the vaginal micro- and mycobiome in asymptomatic reproductive-age Estonian women. PLoS ONE 2013, 8, e54379. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: A systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Tasić, S.; Miladinović-Tasić, N.; Tasić, A.; Zdravković, D.; Djordjević, J. Exogenic reinfection—A possible cause of recurrent genital candidosis in women. Acta Fac. Med. Naissensis 2008, 25, 107–111. [Google Scholar]
- Tasić, S.; Miladinović–Tasić, N.; Tasić, A. Endogenous reinfection as a cause of recurrent GC in women. Srp. Arh. Celok. Lek. 2003, 131, 149–155. [Google Scholar] [CrossRef]
- Blostein, F.; Levin-Sparenberg, E.; Wagner, J.; Foxman, B. Recurrent vulvovaginal candidiasis. Ann. Epidemiol. 2017, 27, 575–582. [Google Scholar] [CrossRef]
- Otašević, S.; Momčilović, S.; Trajkovic, A.; Arsic-Arsenijevic, V. Modelling of antifungal treatment with azoles and essential oils for non-albicans Candida spp. causing vulvo-vaginal infections. Presented at the 27th European Congress of Clinical Microbiology and Infectious Diseases, Vienna, Austria, 22–25 April 2017; Available online: https://www.escmid.org/escmid_publications/escmid_elibrary/material/?mid=52112 (accessed on 15 June 2019).
- Makanjuola, O.; Bongomin, F.; Fayemiwo, S.A. An update on the roles of non-albicans Candida species in vulvovaginitis. J. Fungi (Basel) 2018, 4, 121. [Google Scholar] [CrossRef]
- Papaemmanouil, V.; Georgogiannis, N.; Plega, M.; Lalaki, J.; Lydakis, D.; Dimitriou, M.; Papadimitriou, A. Prevalence and susceptibility of Saccharomyces cerevisiae causing vaginitis in Greek women. Anaerobe 2011, 17, 298–299. [Google Scholar] [CrossRef]
- Mendling, W.; Brasch, J.; Cornely, O.A.; Effendy, I.; Friese, K.; Ginter-Hanselmayer, G.; Hof, H.; Mayser, P.; Mylonas, I.; Ruhnke, M.; et al. Guideline: Vulvovaginal candidosis (AWMF 015/072), S2k (excluding chronic mucocutaneous candidosis). Mycoses 2015, 58, 1–15. [Google Scholar] [CrossRef] [PubMed]
- EuroQoL Group. EuroQoL—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2013. Available online: http://www.R-project.org/ (accessed on 15 June 2019).
- Tasić, S.; Miladinović-Tasić, N. Immunopathogenesis of recurrent GC in women. Med. Pregl. 2009, 62, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Tasić, S. Recurrent GC of Women—Microbiological and Immunological Aspects. PhD Thesis, University of Nis, Niš, Serbia, 1998. [Google Scholar]
- Echeverría-Irigoyen, M.J.; Eraso, E.; Cano, J.; Gomáriz, M.; Guarro, J.; Quindós, G. Saccharomyces cerevisiae vaginitis: Microbiology and in vitro antifungal susceptibility. Mycopathologia 2011, 172, 201–205. [Google Scholar] [CrossRef]
- Savini, V.; Catavitello, C.; Manna, A.; Talia, M.; Febbo, F.; Balbinot, A.; D’Antonio, F.; Di Bonaventura, G.; Celentano, C.; Liberati, M.; et al. Two cases of vaginitis caused by itraconazole-resistant Saccharomyces cerevisiae and a review of recently published studies. Mycopathologia 2008, 166, 47–50. [Google Scholar] [CrossRef]
- Liu, X.P.; Fan, S.R.; Peng, Y.T.; Zhang, H.P. Species distribution and susceptibility of Candida isolates from patient with vulvovaginal candidiasis in Southern China from 2003 to 2012. J. Mycol. Med. 2014, 24, 106–111. [Google Scholar] [CrossRef]
- Adjapong, G.; Hale, M.; Garrill, A. A comparative investigation of azole susceptibility in Candida isolates from vulvovaginal candidiasis and recurrent vulvovaginal candidiasis patients in Ghana. Med. Mycol. 2016, 55, 686–689. [Google Scholar]
- Richter, S.S.; Galask, R.P.; Messer, S.A.; Hollis, R.J.; Diekema, D.J.; Pfaller, M.A. Antifungal susceptibilities of Candida species causing vulvovaginitis and epidemiology of recurrent cases. J. Clin. Microbiol. 2005, 43, 2155–2162. [Google Scholar] [CrossRef]
- Hadrich, I.; Ayadi, A. Epidemiology of antifungal susceptibility: Review of literature. J. Mycol. Med. 2018, 28, 574–584. [Google Scholar] [CrossRef]
- Yano, J.; Sobel, J.D.; Nyirjesy, P.; Sobel, R.; Williams, V.L.; Yu, Q.; Noverr, M.C.; Fidel, P.L., Jr. Current patient perspectives of vulvovaginal candidiasis: Incidence, symptoms, management and post-treatment outcomes. BMC Womens Health 2019, 19, 48. [Google Scholar] [CrossRef]
- Sobel, J.D. Recurrent vulvovaginal candidiasis. Am. J. Obstet. Gynecol. 2016, 214, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Corsello, S.; Spinillo, A.; Osnengo, G.; Penna, C.; Guaschino, S.; Beltrame, A.; Blasi, N.; Festa, A. An epidemiological survey of vulvovaginal candidiasis in Italy. Eur J. Obstet. Gynecol. Reprod. Biol. 2003, 110, 66–72. [Google Scholar] [CrossRef]


{kind=link}
| Causative Agent of RVVC | n (%) |
|---|---|
| C. albicans | 236 (73.8) |
| C. glabrata | 44 (13.8) |
| C. krusei | 20 (6.3) |
| C. tropicalis | 7 (2.2) |
| C. parapsilosis | 4 (1.3) |
| C. kefyr | 3 (0.9) |
| S. cerevesiae | 6 (1.9) |
| Species | Antifungal Susceptibility Testing, n (%) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5-FC 2–32 µg/mL | AmB 0.5–8 µg/mL | ITZ 0.125–4 µg/mL | FCZ 8–64 µg/mL | VRZ 1 µg/mL | KCZ 0.5–4 µg/mL | MCZ 0.5–8 µg/mL | ||||||||||
| MIC ≤ 4 µg/mL | MIC = 8–16 µg/mL | MIC ≤ 0.5 µg/mL | MIC = 2 µg/mL | MIC > 2 µg/mL | MIC ≤ 0.125 µg/mL | MIC = 0.25–0.5 µg/mL | MIC ≤ 8 µg/mL | MIC = 16–32 µg/Ml | MIC > 32 µg/mL | MIC ≤ 1 µg/mL | MIC > 1 µg/mL | MIC < 0.5 µg/mL | MIC > 0.5 µg/mL | MIC < 0.5 µg/mL | MIC > 0.5 µg/mL | |
| S | I/ SDD | S | I/ SDD | R | S | I/ SDD | S | I/ SDD | R | S | I/ SDD | S | I/ SDD | S | I/ SDD | |
| C. albicans | 211 (89.4) | 25 (10.6) | 225 (95.3) | 11 (4.7) | 0 | 81 (34.3) | 155 (65.7) | 157 (66.5) | 79 (33.5) | 0 | 183 (77.5) | 53 (22.5) | 213 (90.3) | 23 (9.7) | 127 (53.8) | 109 (46.2) |
| C. glabrata | 43 (97.7) | 1 (2.3) | 44 (100) | 0 | 0 | 11 (25) | 33 (75) | 10 (22.7) | 33 (75) | 1 (2.3) | 31 (70.5) | 13 (29.5) | 39 (88.6) | 5 (11.4) | 12 (27.3) | 32 (72.7) |
| C. krusei | 19 (95) | 1 (5) | 18 (90) | 0 | 2 (10) | 5 (25) | 15 (75) | 0 | 0 | 20 (100) | 19 (95) | 1 (5) | 19 (95) | 1 (5) | 12 (60) | 8 (40) |
| C. tropicalis | 7 (100) | 0 | 7 (100) | 0 | 0 | 3 (42.9) | 4 (57.1) | 2 (28.6) | 5 (71.4) | 0 | 7(100) | 0 | 7 (100) | 0 | 2 (28.6) | 5 (71.4) |
| C. parapsilosis | 4 (100) | 0 | 4 (100) | 0 | 0 | 4 (100) | 0 | 4 (100) | 0 | 0 | 4 (100) | 0 | 4 (100) | 0 | 4 (100) | 0 |
| C. kefyr | 3 (100) | 0 | 3 (100) | 0 | 0 | 3 (100) | 0 | 3 (100) | 0 | 0 | 3 (100) | 0 | 4 (100) | 0 | 4 (100) | 0 |
| S. cerevesiae | 6 (100) | 0 | 4 (66.7) | 0 | 2 (33.3) | 4 (66.7) | 2 (33.3) | 4 (66.7) | 2 (33.3) | 0 | 4 (66.7) | 2 (33.3) | 4 (66.7) | 2 (33.3) | 4 (66.7) | 2 (33.3) |
| Characteristics | RVVC, n (%) | Control, n (%) | p* | ||
|---|---|---|---|---|---|
| Itching | |||||
| 0 | 216 | (67.5) | 98 | (89.9) | <0.001 |
| 1 | 104 | (32.5) | 11 | (10.1) | |
| Discharge | |||||
| 0 | 68 | (21.2) | 61 | (56.0) | <0.001 |
| 1 | 252 | (78.8) | 48 | (44.0) | |
| Odor | |||||
| 0 | 284 | (88.8) | 100 | (91.7) | 0.484 |
| 1 | 36 | (11.2) | 9 | (8.3) | |
| Burning | |||||
| 0 | 232 | (72.5) | 104 | (95.4) | <0.001 |
| 1 | 88 | (27.5) | 5 | (4.6) | |
| Erythema | |||||
| 0 | 260 | (81.2) | 104 | (95.4) | <0.001 |
| 1 | 60 | (18.8) | 5 | (4.6) | |
| Whitish discharge | |||||
| 0 | 92 | (28.8) | 63 | (57.8) | <0.001 |
| 1 | 228 | (71.2) | 46 | (42.2) | |
| Edema | |||||
| 0 | 288 | (90.0) | 108 | (99.1) | 0.004 |
| 1 | 32 | (10.0) | 1 | (0.9) | |
| Soreness/tenderness | |||||
| 0 | 224 | (70.0) | 99 | (90.8) | <0.001 |
| 1 | 96 | (30.0) | 10 | (9.2) | |
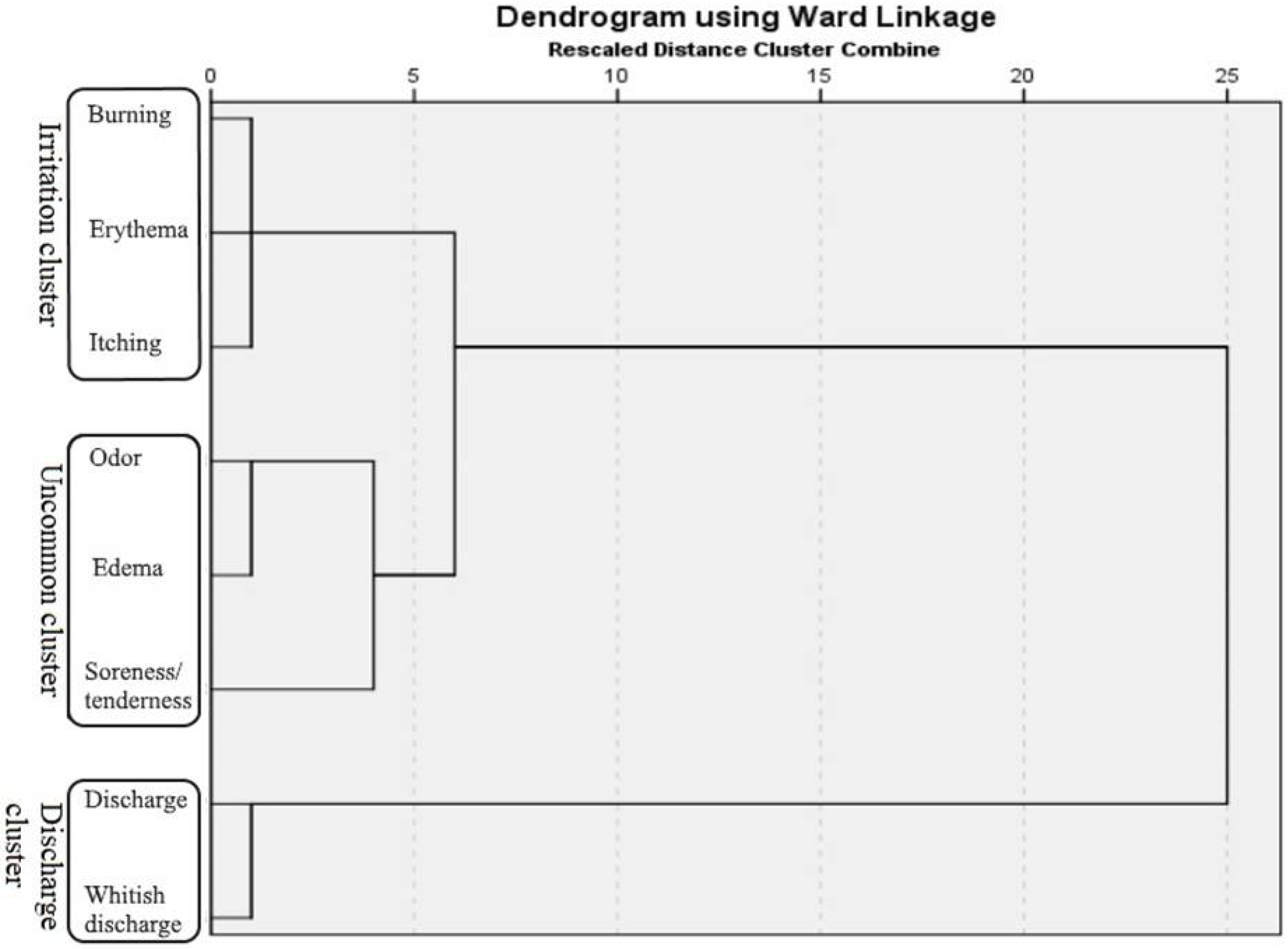
| Signs and Symptoms | Irritation Cluster, n (%) | Uncommon Cluster, n (%) | Discharge Cluster, n (%) | |||
|---|---|---|---|---|---|---|
| None | 188 | (58.8) | 200 | (62.5) | 48 | (15) |
| Some | 84 | (25.5) | 116 | (36.3) | 64 | (20) |
| All | 48 | (15) | 4 | (1.3) | 208 | (65) |
| 320 | (100) | 320 | (100) | 320 | (100) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ignjatović, A.; Arsić-Arsenijević, V.; Golubović, M.; Đenić, S.; Momčilović, S.; Trajković, A.; Ranđelović, M.; Ćirić, V.; Otašević, S. Recurrent Vulvovaginal Candidosis and Cluster Analysis of Clinical Signs and Symptoms: A Laboratory-Based Investigation. J. Fungi 2020, 6, 113. https://doi.org/10.3390/jof6030113
Ignjatović A, Arsić-Arsenijević V, Golubović M, Đenić S, Momčilović S, Trajković A, Ranđelović M, Ćirić V, Otašević S. Recurrent Vulvovaginal Candidosis and Cluster Analysis of Clinical Signs and Symptoms: A Laboratory-Based Investigation. Journal of Fungi. 2020; 6(3):113. https://doi.org/10.3390/jof6030113
Chicago/Turabian StyleIgnjatović, Aleksandra, Valentina Arsić-Arsenijević, Milan Golubović, Saša Đenić, Stefan Momčilović, Aleksandra Trajković, Marina Ranđelović, Vojislav Ćirić, and Suzana Otašević. 2020. "Recurrent Vulvovaginal Candidosis and Cluster Analysis of Clinical Signs and Symptoms: A Laboratory-Based Investigation" Journal of Fungi 6, no. 3: 113. https://doi.org/10.3390/jof6030113
APA StyleIgnjatović, A., Arsić-Arsenijević, V., Golubović, M., Đenić, S., Momčilović, S., Trajković, A., Ranđelović, M., Ćirić, V., & Otašević, S. (2020). Recurrent Vulvovaginal Candidosis and Cluster Analysis of Clinical Signs and Symptoms: A Laboratory-Based Investigation. Journal of Fungi, 6(3), 113. https://doi.org/10.3390/jof6030113