

Antifungal Testing of Vaginal Candida Isolates in Pregnant Women: A Retrospective, Single-Center Study in Adana, Türkiye

 , , , , , , , , and
, , , , , , , , and 
Abstract
1. Introduction
2. Materials and Methods
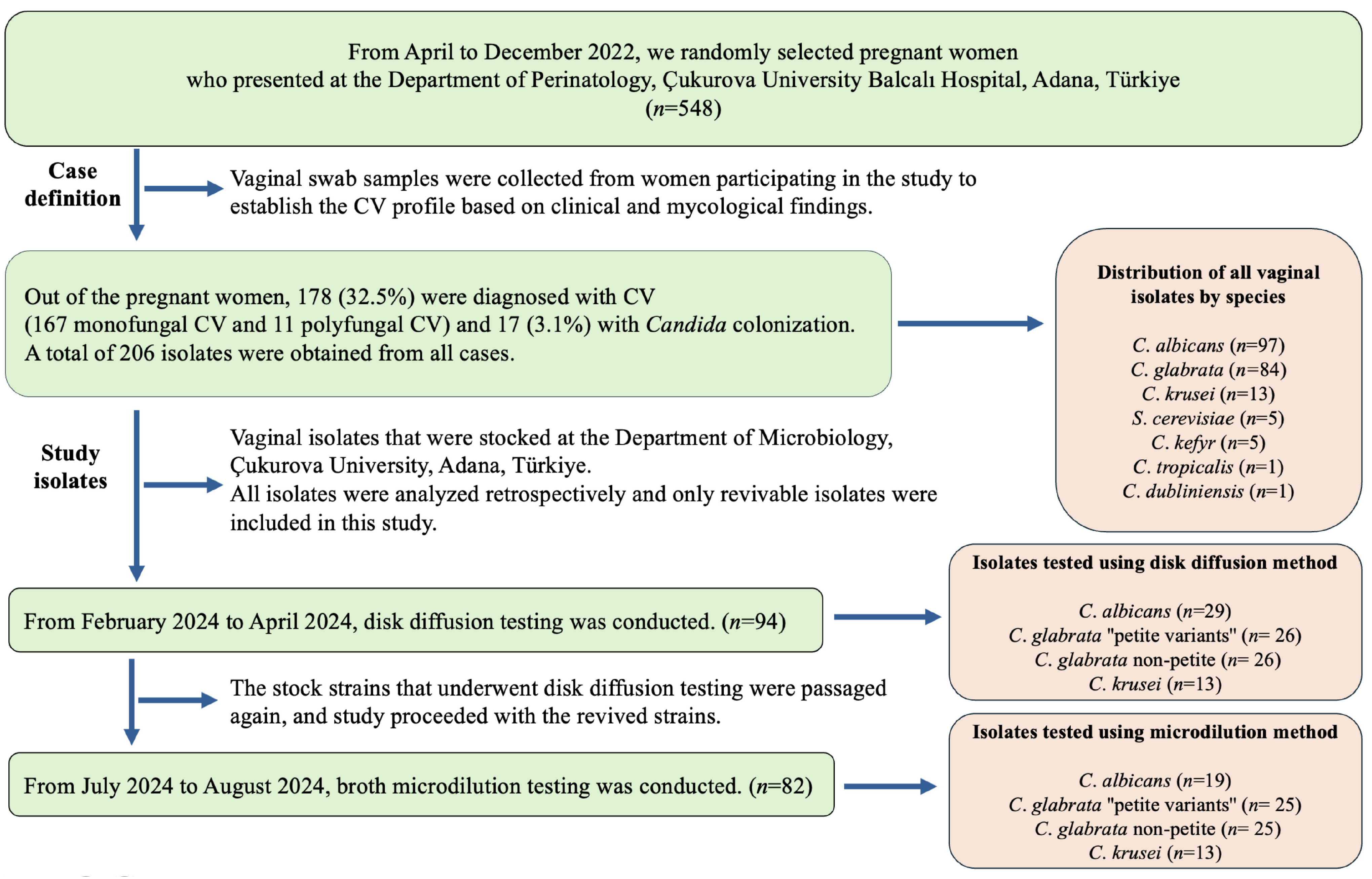
2.1. Study Group and Identification of Isolates
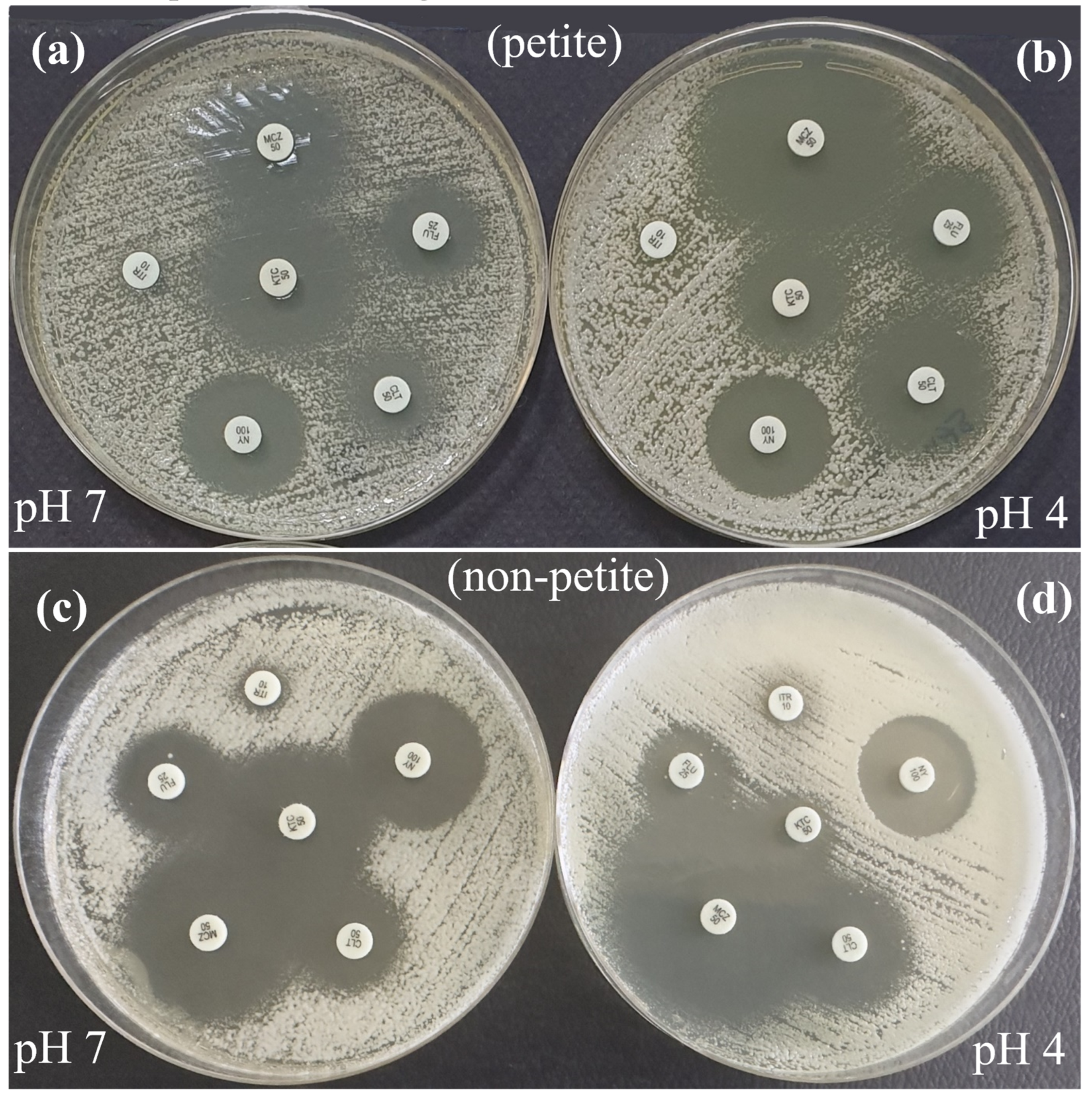
2.2. Candida glabrata “Petite Variants”
2.3. Antifungal Testing
2.3.1. Disk Diffusion Method
2.3.2. Broth Microdiution Method
2.4. Statistical Analysis
2.5. Ethics Statement
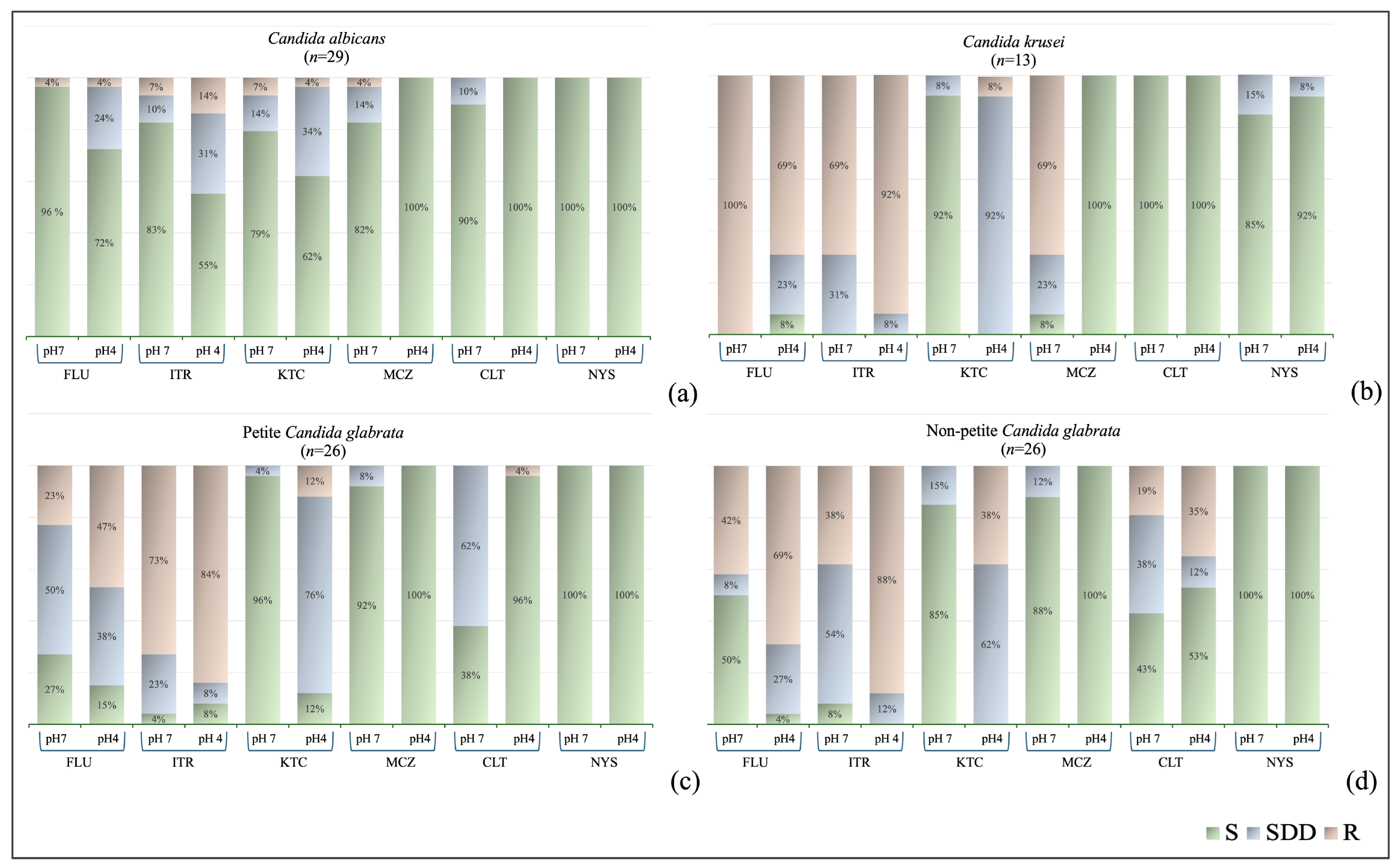
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sobel, J.D. Vulvovaginal candidosis. Lancet 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- Sobel, J.D. Recurrent vulvovaginal candidiasis. Am. J. Obstet. Gynecol. 2016, 214, 15–21. [Google Scholar] [CrossRef]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: A systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Foxman, B.; Muraglia, R.; Dietz, J.P.; Sobel, J.D.; Wagner, J. Prevalence of recurrent vulvovaginal candidiasis in 5 European countries and the United States: Results from an internet panel survey. J. Low. Genit. Tract. Dis. 2013, 17, 340–345. [Google Scholar] [CrossRef]
- Danby, C.S.; Boikov, D.; Rautemaa, R.; Sobel, J.D. Effect of pH on in vitro susceptibility of Candida glabrata and Candida albicans to eleven antifungal agents—Implications for clinical use. Antimicrob. Agents Chemother. 2012, 56, 1403–1406. [Google Scholar] [CrossRef]
- Arechavala, A.; Negroni, R.; Santiso, G.; Depardo, R.; Bonvehi, P. Chronic recurrent vulvovaginitis is not only due to Candida. Rev. Iberoam. Micol. 2021, 38, 132–137. [Google Scholar] [CrossRef]
- Sobel, J.D.; Sobel, R. Current treatment options for vulvovaginal candidiasis caused by azole-resistant Candida species. Expert Opin. Pharmacother. 2018, 19, 971–977. [Google Scholar] [CrossRef]
- Fernandes, Â.; Azevedo, N.; Valente, A.; Dias, M.; Gomes, A.; Nogueira-Silva, C.; Henriques, M.; Silva, S.; Gonçalves, B. Vulvovaginal candidiasis and asymptomatic vaginal colonization in Portugal: Epidemiology, risk factors and antifungal pattern. Med. Mycol. 2022, 60, myac029. [Google Scholar] [CrossRef]
- Dunaiski, C.M.; Kock, M.M.; Chan, W.Y.; Ismail, A.; Peters, R.P.H. Molecular epidemiology and antimicrobial resistance of vaginal Candida glabrata isolates in Namibia. Med. Mycol. 2024, 62, myae009. [Google Scholar] [CrossRef]
- Sobel, J.D.; Chaim, W.; Nagappan, V.; Leaman, D. Treatment of vaginitis caused by Candida glabrata: Use of topical boric acid and flucytosine. Am. J. Obstet. Gynecol. 2003, 189, 1297–1300. [Google Scholar] [CrossRef]
- Sobel, J.D. Treatment of vaginitis caused by non-albicans Candida species. Expert Rev. Anti Infect. Ther. 2024, 22, 289–296. [Google Scholar] [CrossRef]
- Linhares, I.M.; Summers, P.R.; Larsen, B.; Giraldo, P.C.; Witkin, S.S. Contemporary perspectives on vaginal pH and lactobacilli. Am. J. Obstet. Gynecol. 2011, 204, 120.e1–120.e5. [Google Scholar] [CrossRef]
- Boikov, D.A.; Locke, J.B.; James, K.D.; Bartizal, K.; Sobel, J.D. In vitro activity of the novel echinocandin CD101 at pH 7 and 4 against Candida spp. isolates from patients with vulvovaginal candidiasis. J. Antimicrob. Chemother. 2017, 72, 1355–1358. [Google Scholar] [CrossRef]
- Sobel, J.D.; Borroto-Esoda, K.; Azie, N.; Angulo, D. In vitro pH activity of ibrexafungerp against fluconazole-susceptible and -resistant Candida isolates from women with vulvovaginal candidiasis. Antimicrob. Agents Chemother. 2021, 65, e0056221. [Google Scholar] [CrossRef]
- Sobel, J.D.; Akins, R. Determining susceptibility in Candida vaginal isolates. Antimicrob. Agents Chemother. 2022, 66, e0236621. [Google Scholar] [CrossRef]
- Sobel, J.D.; Sebastian, S.; Boikov, D.A. A longitudinal study on fluconazole resistance in Candida albicans vaginal isolates. Mycoses 2023, 66, 563–565. [Google Scholar] [CrossRef]
- Sobel, J.D. Resistance to fluconazole of Candida albicans in vaginal isolates: A 10-year study in a clinical referral center. Antimicrob. Agents Chemother. 2023, 67, e0018123. [Google Scholar] [CrossRef]
- Saxon, C.; Edwards, A.; Rautemaa-Richardson, R.; Owen, C.; Nathan, B.; Palmer, B.; Wood, C.; Ahmed, H. British Association for Sexual Health and HIV national guideline for the management of vulvovaginal candidiasis (2019). Int. J. STD AIDS 2020, 31, 1124–1144. [Google Scholar] [CrossRef]
- Posteraro, B.; Tumbarello, M.; La Sorda, M.; Spanu, T.; Trecarichi, E.M.; De Bernardis, F.; Scoppettuolo, G.; Sanguinetti, M.; Fadda, G. Azole resistance of Candida glabrata in a case of recurrent fungemia. J. Clin. Microbiol. 2006, 44, 3046–3047. [Google Scholar] [CrossRef]
- Arastehfar, A.; Daneshnia, F.; Hovhannisyan, H.; Fuentes, D.; Cabrera, N.; Quinteros, C.; Ilkit, M.; Ünal, N.; Hilmioğlu-Polat, S.; Jabeen, K.; et al. Overlooked Candida glabrata petites are echinocandin tolerant, induce host inflammatory responses, and display poor in vivo fitness. mBio 2023, 14, e0118023. [Google Scholar] [CrossRef]
- Badrane, H.; Cheng, S.; Dupont, C.L.; Hao, B.; Driscoll, E.; Morder, K.; Liu, G.; Newbrough, A.; Fleres, G.; Kaul, D.; et al. Genotypic diversity and unrecognized antifungal resistance among populations of Candida glabrata from positive blood cultures. Nat. Commun. 2023, 14, 5918. [Google Scholar] [CrossRef]
- Garcia-Rubio, R.; Jimenez-Ortigosa, C.; DeGregorio, L.; Quinteros, C.; Shor, E.; Perlin, D.S. Multifactorial role of mitochondria in echinocandin tolerance revealed by transcriptome analysis of drug-tolerant cells. mBio 2021, 12, e0195921. [Google Scholar] [CrossRef]
- Karakoyun, A.S.; Unal, N.; Sucu, M.; Bingöl, O.; Unal, I.; Ilkit, M. Integrating clinical and microbiological expertise to improve vaginal candidiasis management. Mycopathologia 2024, 189, 96. [Google Scholar] [CrossRef]
- Pincus, D.H.; Orenga, S.; Chatellier, S. Yeast identification—Past, present, and future methods. Med. Mycol. 2007, 45, 97–121. [Google Scholar] [CrossRef]
- Guzel, A.B.; Ilkit, M.; Burgut, R.; Urunsak, I.F.; Ozgunen, F.T. An evaluation of risk factors in pregnant women with Candida vaginitis and the diagnostic value of simultaneous vaginal and rectal sampling. Mycopathologia 2011, 172, 25–36. [Google Scholar] [CrossRef]
- Normand, A.C.; Gabriel, F.; Riat, A.; Cassagne, C.; Bourgeois, N.; Huguenin, A.; Chauvin, P.; De Geyter, D.; Bexkens, M.; Rubio, E.; et al. Optimization of MALDI-ToF mass spectrometry for yeast identification: A multicenter study. Med. Mycol. 2020, 58, 639–649. [Google Scholar] [CrossRef]
- CLSI M44-A2; Method for Antifungal Disk Diffusion Susceptibility Testing of Yeasts. 2nd ed. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2009.
- Liu, W.; Zhang, X.; Liu, Z.; Luo, X. Impact of pH on the antifungal susceptibility of vaginal Candida albicans. Int. J. Gynaecol. Obstet. 2011, 114, 278–280. [Google Scholar] [CrossRef]
- Dota, K.F.D.; Freitas, A.R.; Consolaro, M.E.L.; Svidzinski, T.I.E. A challenge for clinical laboratories: Detection of antifungal resistance in Candida species causing vulvovaginal candidiasis. Lab. Med. 2011, 42, 87–93. [Google Scholar] [CrossRef]
- Khan, M.; Ahmed, J.; Gul, A.; Ikram, A.; Lalani, F.K. Antifungal susceptibility testing of vulvovaginal Candida species among women attending antenatal clinic in tertiary care hospitals of Peshawar. Infect. Drug Resist. 2018, 11, 447–456. [Google Scholar] [CrossRef]
- CLSI M27-A3; Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts. 3rd ed. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008.
- CLSI M60; Performance Standards for Antifungal Susceptibility Testing of Yeasts. 1st ed. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017.
- CLSI M27-S4; Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts. 4th Supp. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2012.
- Pfaller, M.A.; Espinel-Ingroff, A.; Canton, E.; Castanheira, M.; Cuenca-Estrella, M.; Diekema, D.J.; Fothergill, A.; Fuller, J.; Ghannoum, M.; Jones, R.N.; et al. Wild-type MIC distributions and epidemiological cutoff values for amphotericin B, flucytosine, and itraconazole and Candida spp. as determined by CLSI broth microdilution. J. Clin. Microbiol. 2012, 50, 2040–2046. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Hazen, K.C.; Messer, S.A.; Boyken, L.; Tendolkar, S.; Hollis, R.J.; Diekema, D.J. Comparison of results of fluconazole disk diffusion testing for Candida species with results from a central reference laboratory in the ARTEMIS global antifungal surveillance program. J. Clin. Microbiol. 2004, 42, 3607–3612. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Diekema, D.J.; Messer, S.A.; Boyken, L.; Hollis, R.J. Activities of fluconazole and voriconazole against 1586 recent clinical isolates of Candida species determined by broth microdilution, disk diffusion, and Etest methods: Report from the ARTEMIS Global Antifungal Susceptibility Program, 2001. J. Clin. Microbiol. 2003, 41, 1440–1446. [Google Scholar] [CrossRef]
- Kalkanci, A.; Güzel, A.B.; Khalil, I.I.; Aydin, M.; Ilkit, M.; Kuştimur, S. Yeast vaginitis during pregnancy: Susceptibility testing of 13 antifungal drugs and boric acid and the detection of four virulence factors. Med. Mycol. 2012, 50, 585–593. [Google Scholar] [CrossRef]
- Kwizera, R.; Abdolrasouli, A.; Garcia-Effron, G.; Denning, D.W. Antifungal susceptibility testing: Applicability of methods and strategies for improving access in resource-constrained settings. Lancet Infect. Dis. 2024, 24, e782–e793. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Fluconazole | Itraconazole | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| MIC Range | MIC50 | MIC90 | GM | MIC Range | MIC50 | MIC90 | GM | ||
| pH 7 | C. albicans (n = 19) | <0.125–4 | 2 | 4 | 0.89 | <0.03–2 | 0.25 | 2 | 0.18 |
| Petite C. glabrata (n = 25) | 2–>64 | 16 | 64 | 16.95 | 0.25–>16 | 1 | 16 | 1.63 | |
| Non-petite C. glabrata (n = 25) | 0.5–>64 | 8 | 16 | 6.41 | 0.03–2 | 0.5 | 1 | 0.50 | |
| C. krusei (n = 13) | 16–>64 | 32 | 32 | 30.33 | 0.25–1 | 0.5 | 0.5 | 0.42 | |
| pH 4 | C. albicans (n = 19) | <0.125–8 | 0.5 | 1 | 0.60 | 0.125–0.5 | 0.25 | 0.25 | 0.26 |
| Petite C. glabrata (n = 25) | 8–>64 | >64 | >64 | 49.87 | 2–>16 | 16 | >16 | 10.85 | |
| Non-petite C. glabrata (n = 25) | 8–>64 | 64 | 64 | 39.95 | 1–>16 | 8 | 16 | 7.57 | |
| C. krusei (n = 13) | 16–>64 | 32 | 32 | 28.76 | 0.5–1 | 1 | 1 | 0.85 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sucu, M.; Ünal, N.; Karakoyun, A.S.; Şahin, İ.; Bingöl, O.; Hüner, F.; İşlek Uzay, F.; Ünal, İ.; Metin, D.Y.; Ilkit, M. Antifungal Testing of Vaginal Candida Isolates in Pregnant Women: A Retrospective, Single-Center Study in Adana, Türkiye. J. Fungi 2025, 11, 92. https://doi.org/10.3390/jof11020092
Sucu M, Ünal N, Karakoyun AS, Şahin İ, Bingöl O, Hüner F, İşlek Uzay F, Ünal İ, Metin DY, Ilkit M. Antifungal Testing of Vaginal Candida Isolates in Pregnant Women: A Retrospective, Single-Center Study in Adana, Türkiye. Journal of Fungi. 2025; 11(2):92. https://doi.org/10.3390/jof11020092
Chicago/Turabian StyleSucu, Mete, Nevzat Ünal, Ayşe Sultan Karakoyun, İrem Şahin, Oğuzhan Bingöl, Fatih Hüner, Fatma İşlek Uzay, İlker Ünal, Dilek Yeşim Metin, and Macit Ilkit. 2025. "Antifungal Testing of Vaginal Candida Isolates in Pregnant Women: A Retrospective, Single-Center Study in Adana, Türkiye" Journal of Fungi 11, no. 2: 92. https://doi.org/10.3390/jof11020092
APA StyleSucu, M., Ünal, N., Karakoyun, A. S., Şahin, İ., Bingöl, O., Hüner, F., İşlek Uzay, F., Ünal, İ., Metin, D. Y., & Ilkit, M. (2025). Antifungal Testing of Vaginal Candida Isolates in Pregnant Women: A Retrospective, Single-Center Study in Adana, Türkiye. Journal of Fungi, 11(2), 92. https://doi.org/10.3390/jof11020092