
Aspergillus Outbreak in an Intensive Care Unit: Source Analysis with Whole Genome Sequencing and Short Tandem Repeats


 ,
,  , ,
, ,
Abstract
1. Introduction
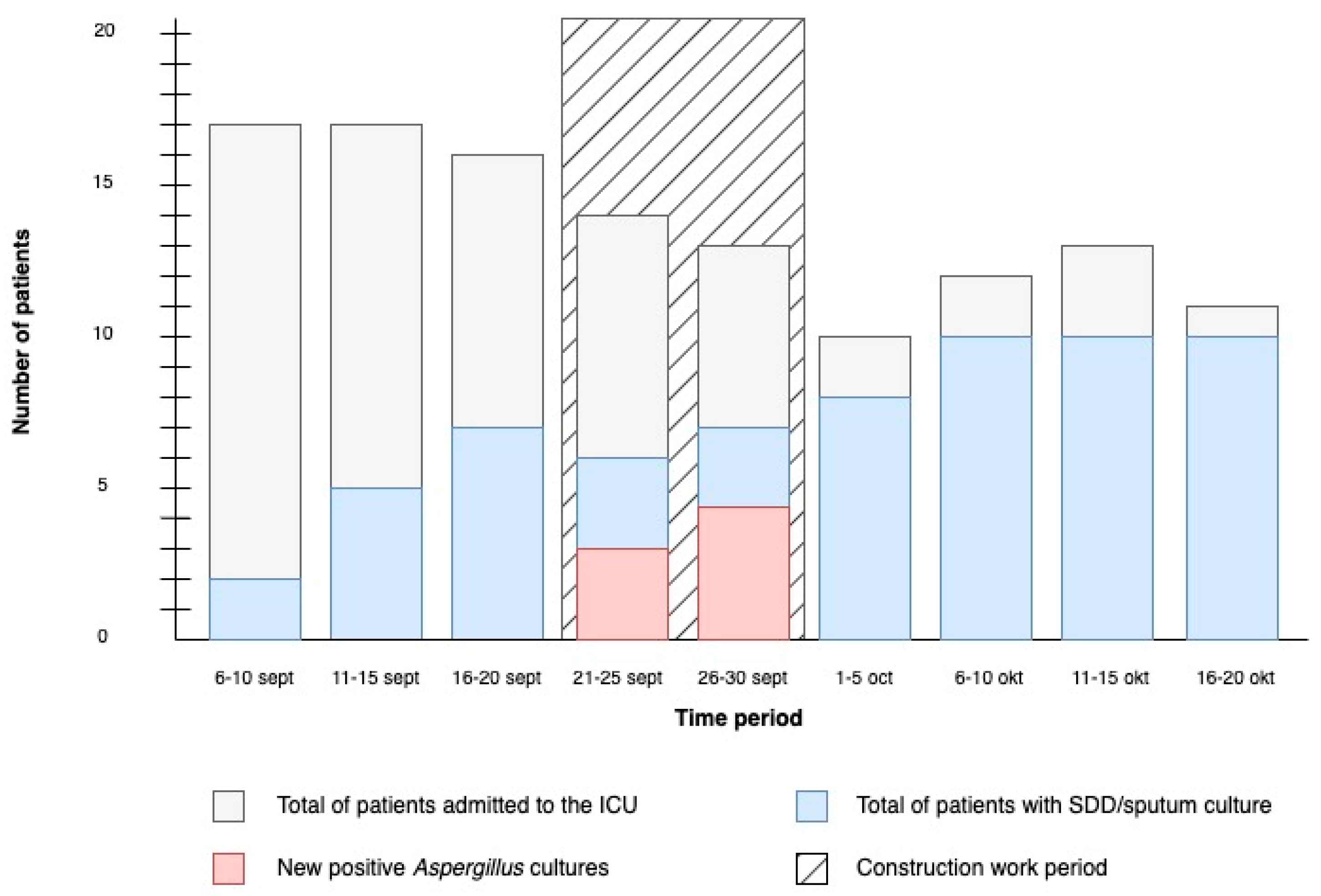
2. Description of the Outbreak
3. Materials and Methods
3.1. Clinical Sample Collection
3.2. Environmental Investigation
3.3. Whole Genome Sequencing and Genotyping
3.3.1. Isolates Culturing and DNA Isolation
3.3.2. Whole Genome Sequencing
3.3.3. STR Typing
3.3.4. Unrelated Sequencing Data Acquisition
3.3.5. Data Analysis
4. Results
4.1. Whole Genome Sequencing and Microsatellite Typing
4.2. Environmental Investigation
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnes, P.D.; Marr, K.A. Aspergillosis: Spectrum of disease, diagnosis, and treatment. Infect. Dis. Clin. North Am. 2006, 20, 545–561. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, D. Current Status of Azole-resistant Aspergillus fumigatus Isolates in East Asia. Med. Mycol. J. 2018, 59, E71–E76. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, D.; Takahashi, H.; Takagi, H.; Watanabe, A.; Kamei, K. Heterogeneity in Pathogenicity-related Properties and Stress Tolerance in Aspergillus fumigatus Clinical Isolates. Med. Mycol. J. 2018, 59, E63–E70. [Google Scholar] [CrossRef] [PubMed]
- Sabino, R.; Simões, H.; Veríssimo, C. Detection of deep fungal infections: A polyphasic approach. J. Med. Microbiol. 2019, 68, 81–86. [Google Scholar] [CrossRef]
- Thompson, G.R., 3rd; Young, J.H. Aspergillus Infections. N. Engl. J. Med. 2021, 385, 1496–1509. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W. Aspergillosis in “nonimmunocompromised” critically ill patients. Am. J. Respir. Crit. Care Med. 2004, 170, 580–581. [Google Scholar] [CrossRef] [PubMed]
- Cornillet, A.; Camus, C.; Nimubona, S.; Gandemer, V.; Tattevin, P.; Belleguic, C.; Chevrier, S.; Meunier, C.; Lebert, C.; Aupée, M. Comparison of epidemiological, clinical, and biological features of invasive aspergillosis in neutropenic and nonneutropenic patients: A 6-year survey. Clin. Infect. Dis. 2006, 43, 577–584. [Google Scholar] [CrossRef]
- Denning, D.W. Invasive aspergillosis. Clin. Infect. Dis. 1998, 26, 781–803. [Google Scholar] [CrossRef]
- Patterson, J.E.; Peters, J.; Calhoon, J.; Levine, S.; Anzueto, A.; Al-Abdely, H.; Sanchez, R.; Patterson, T.; Rech, M.; Jorgensen, J.; et al. Investigation and control of aspergillosis and other filamentous fungal infections in solid organ transplant recipients. Transpl. Infect. Dis. 2000, 2, 22–28. [Google Scholar] [CrossRef]
- Upton, A.; Kirby, K.A.; Carpenter, P.; Boeckh, M.; Marr, K.A. Invasive aspergillosis following hematopoietic cell transplantation: Outcomes and prognostic factors associated with mortality. Clin. Infect. Dis. 2007, 44, 531–540. [Google Scholar] [CrossRef]
- Nicolle, M.C.; Bénet, T.; Thiebaut, A.; Bienvenu, A.-L.; Voirin, N.; Duclos, A.; Sobh, M.; Cannas, G.; Thomas, X.; Nicolini, F.-E.; et al. Invasive aspergillosis in patients with hematologic malignancies: Incidence and description of 127 cases enrolled in a single institution prospective survey from 2004 to 2009. Haematologica 2011, 96, 1685–1691. [Google Scholar] [CrossRef] [PubMed]
- Hadrich, I.; Makni, F.; Sellami, H.; Cheikhrouhou, F.; Sellami, A.; Bouaziz, H.; Hdiji, S.; Elloumi, M.; Ayadi, A. Invasive aspergillosis: Epidemiology and environmental study in haematology patients (Sfax, Tunisia). Mycoses 2010, 53, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Diba, K.; Jangi, F.; Makhdoomi, K.; Moshiri, N.; Mansouri, F. Aspergillus diversity in the environments of nosocomial infection cases at a university hospital. J. Med. Life 2019, 12, 128–132. [Google Scholar] [CrossRef]
- Balajee, S.A.; de Valk, H.A.; Lasker, B.A.; Meis, J.F.; Klaassen, C.H. Utility of a microsatellite assay for identifying clonally related outbreak isolates of Aspergillus fumigatus. J. Microbiol. Methods 2008, 73, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, D.; Takahashi, H.; Watanabe, A.; Takahashi-Nakaguchi, A.; Kawamoto, S.; Kamei, K.; Gonoi, T. Whole-genome comparison of Aspergillus fumigatus strains serially isolated from patients with aspergillosis. J. Clin. Microbiol. 2014, 52, 4202–4209. [Google Scholar] [CrossRef]
- Klaassen, C.H.; Osherov, N. Aspergillus strain typing in the genomics era. Stud. Mycol. 2007, 59, 47–51. [Google Scholar] [CrossRef]
- de Valk, H.A.; Meis, J.F.G.M.; Curfs, I.M.; Muehlethaler, K.; Mouton, J.W.; Klaassen, H.W. Use of a novel panel of nine short tandem repeats for exact and high-resolution fingerprinting of Aspergillus fumigatus isolates. J. Clin. Microbiol. 2005, 43, 4112–4120. [Google Scholar] [CrossRef]
- Di Pilato, V.; Codda, G.; Ball, L.; Giacobbe, D.R.; Willison, E.; Mikulska, M.; Magnasco, L.; Crea, F.; Vena, A.; Pelosi, P.; et al. Molecular Epidemiological Investigation of a Nosocomial Cluster of C. auris: Evidence of Recent Emergence in Italy and Ease of Transmission during the COVID-19 Pandemic. J. Fungi 2021, 7, 140. [Google Scholar] [CrossRef]
- Menu, E.; Criscuolo, A.; Desnos-Ollivier, M.; Cassagne, C.; D’incan, E.; Furst, S.; Ranque, S.; Berger, P.; Dromer, F. Saprochaete clavata Outbreak Infecting Cancer Center through Dishwasher. Emerg. Infect. Dis. 2020, 26, 2031–2038. [Google Scholar] [CrossRef]
- Theodoropoulos, N.M.; Bolstorff, B.; Bozorgzadeh, A.; Brandeburg, C.; Cumming, M.; Daly, J.S.; Ellison, R.T.; Forsberg, K.; Gade, L.; Gibson, L.; et al. Candida auris outbreak involving liver transplant recipients in a surgical intensive care unit. Am. J. Transplant. 2020, 20, 3673–3679. [Google Scholar] [CrossRef]
- Vonberg, R.P.; Gastmeier, P. Nosocomial aspergillosis in outbreak settings. J. Hosp. Infect. 2006, 63, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, H.; Rutala, W.A.; Sickbert-Bennett, E.E.; Weber, D.J. Review of fungal outbreaks and infection prevention in healthcare settings during construction and renovation. Clin. Infect. Dis. 2015, 61, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.P.; Adjidé, C.C.; Bernard, L.; Botterel, F.; Carel, A.; Castel, O.; Derouin, F.; Hoarau, G.; Labussière, H.; Lafaurie, M.; et al. Quantitative assessment of fungal risk in the case of construction works in healthcare establishments: Proposed indicators for the determination of the impact of management precautions on the risk of fungal infection. J. Mycol. Med. 2012, 22, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.; Abdolrasouli, A.; Dunne, K.; Sewell, T.R.; Zhang, Y.; Ballard, E.; Brackin, A.P.; van Rhijn, N.; Chown, H.; Tsitsopoulou, A.; et al. Population genomics confirms acquisition of drug-resistant Aspergillus fumigatus infection by humans from the environment. Nat. Microbiol. 2022, 7, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.J.; Weir, B.S.; Glare, T.; Rhodes, J.; Perrott, J.; Fisher, M.C.; Stajich, J.E.; Digby, A.; Dearden, P.K.; Cox, M.P. A single fungal strain was the unexpected cause of a mass aspergillosis outbreak in the world’s largest and only flightless parrot. iScience 2022, 25, 105470. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Arentshorst, M.; Ram, A.F.; Meyer, V. Using non-homologous end-joining-deficient strains for functional gene analyses in filamentous fungi. Methods Mol. Biol. 2012, 835, 133–150. [Google Scholar]
- Ballard, E.; Melchers, W.J.; Zoll, J.; Brown, A.J.; Verweij, P.E.; Warris, A. In-host microevolution of Aspergillus fumigatus: A phenotypic and genotypic analysis. Fungal Genet. Biol. 2018, 113, 1–13. [Google Scholar] [CrossRef]
- Engel, T.; Verweij, P.E.; van den Heuvel, J.; Wangmo, D.; Zhang, J.; Debets, A.J.M.; Snelders, E. Parasexual recombination enables Aspergillus fumigatus to persist in cystic fibrosis. ERJ Open Res. 2020, 6, 00020-2020. [Google Scholar] [CrossRef]
- Leinonen, R.; Sugawara, H.; Shumway, M. The sequence read archive. Nucleic Acids Res. 2011, 39, D19–D21. [Google Scholar] [CrossRef] [PubMed]
- National Library of Medicine. SRA Toolkit. 2021. Available online: https://trace.ncbi.nlm.nih.gov/Traces/sra/sra.cgi?view=software (accessed on 1 June 2021).
- RIVM. Juno-Assembly Pipeline. 2021. Available online: https://github.com/RIVM-bioinformatics/juno-assembly (accessed on 1 June 2021).
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef] [PubMed]
- Andrews, S. A quality control tool for high throughput sequence data. In FASTQC; Babraham Institute: Cambridge, UK, 2010. [Google Scholar]
- Prjibelski, A.; Antipov, D.; Meleshko, D.; Lapidus, A.; Korobeynikov, A. Using SPAdes De Novo Assembler. Curr. Protoc. Bioinform. 2020, 70, e102. [Google Scholar] [CrossRef] [PubMed]
- Bushnell, B. BBMap. 2021. Available online: https://sourceforge.net/projects/bbmap/ (accessed on 1 June 2021).
- Harris, S.R. SKA: Split Kmer Analysis Toolkit for Bacterial Genomic Epidemiology. bioRxiv 2018. [Google Scholar] [CrossRef]
- Seemann, T. Pairwise SNP Distance Matrix from a FASTA Sequence Alignment. Available online: https://github.com/tseemann/snp-dists (accessed on 1 June 2021).
- Hoang, D.T.; Chernomor, O.; Von Haeseler, A.; Minh, B.Q.; Vinh, L.S. UFBoot2: Improving the Ultrafast Bootstrap Approximation. Mol. Biol. Evol. 2018, 35, 518–522. [Google Scholar] [CrossRef]
- Kalyaanamoorthy, S.; Minh, B.Q.; Wong, T.K.F.; Von Haeseler, A.; Jermiin, L.S. ModelFinder: Fast model selection for accurate phylogenetic estimates. Nat. Methods 2017, 14, 587–589. [Google Scholar] [CrossRef]
- Letunic, I.; Bork, P. Interactive Tree Of Life (iTOL) v5: An online tool for phylogenetic tree display and annotation. Nucleic Acids Res. 2021, 49, W293–W296. [Google Scholar] [CrossRef]
- Hasegawa, K.; Doi, A.; Kuroda, H.; Hasuike, T.; Ogura, A.; Nasu, S.; Nishioka, H.; Tomii, K. A pseudo-outbreak of COVID-19 associated pulmonary aspergillosis: A microbiological investigation of both the patients and the environment. J. Infect. Prev. 2023, 24, 83–88. [Google Scholar] [CrossRef]
- Machida, M. Progress of Aspergillus oryzae genomics. Adv. Appl. Microbiol. 2002, 51, 81–106. [Google Scholar]
- Garcia-Rubio, R.; Monzon, S.; Alcazar-Fuoli, L.; Cuesta, I.; Mellado, E. Genome-Wide Comparative Analysis of Aspergillus fumigatus Strains: The Reference Genome as a Matter of Concern. Genes 2018, 9, 363. [Google Scholar] [CrossRef]
- Meis, J.F.; Chowdhary, A.; Rhodes, J.L.; Fisher, M.C.; Verweij, P.E. Clinical implications of globally emerging azole resistance in Aspergillus fumigatus. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2016, 371, 20150460. [Google Scholar] [CrossRef] [PubMed]
- FMS. Air Monitoring in Operating Theatre and Threatening Rooms. 2023. Available online: https://richtlijnendatabase.nl/richtlijn/luchtbehandeling_in_operatiekamers_en_behandelkamers/startpagina_-_luchtbehandeling_in_operatiekamers_en_behandelkamers.html (accessed on 1 October 2023).

{kind=link}
{kind=link}
{kind=link}
| Patients | |||||||
|---|---|---|---|---|---|---|---|
| Characteristic | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Age, years | 76 | 88 | 73 | 71 | 69 | 76 | 73 |
| Sex | Male | Male | Female | Female | Female | Male | Male |
| Clinical risk factors for IA | None | None | Prolonged cortico-steroid use | None | None | Prolonged cortico-steroid use | Neutro-penia due to urothelial-carcinoma |
| Reason for ICU admission | COVID-19 | Post-operative care | COVID-19 | Septic shock | COVID-19 | COVID-19 | Septic shock |
| SDD culture for Aspergillus spp. | flavus | fumigatus + flavus | fumigatus | fumigatus | fumigatus | fumigatus + flavus | NA |
| Bronchoalveolar lavage | |||||||
| Fungal culture | Negative | NA | Negative | NA | Positive | Positive | Negative |
| Galactomannan (GMI) | Negative | NA | Negative | NA | Positive (4.33) | Positive (4.32) | Positive (3.73) |
| Diagnosis IA | No, colonization | No, colonization | No, colonization | No, colonization | Yes, probable CAPA | Yes, probable CAPA | Yes, probable IA |
| Outcome | Discharged from ICU | Discharged from ICU | Discharged from ICU | Discharged from ICU | Discharged from ICU | Deceased | Deceased |
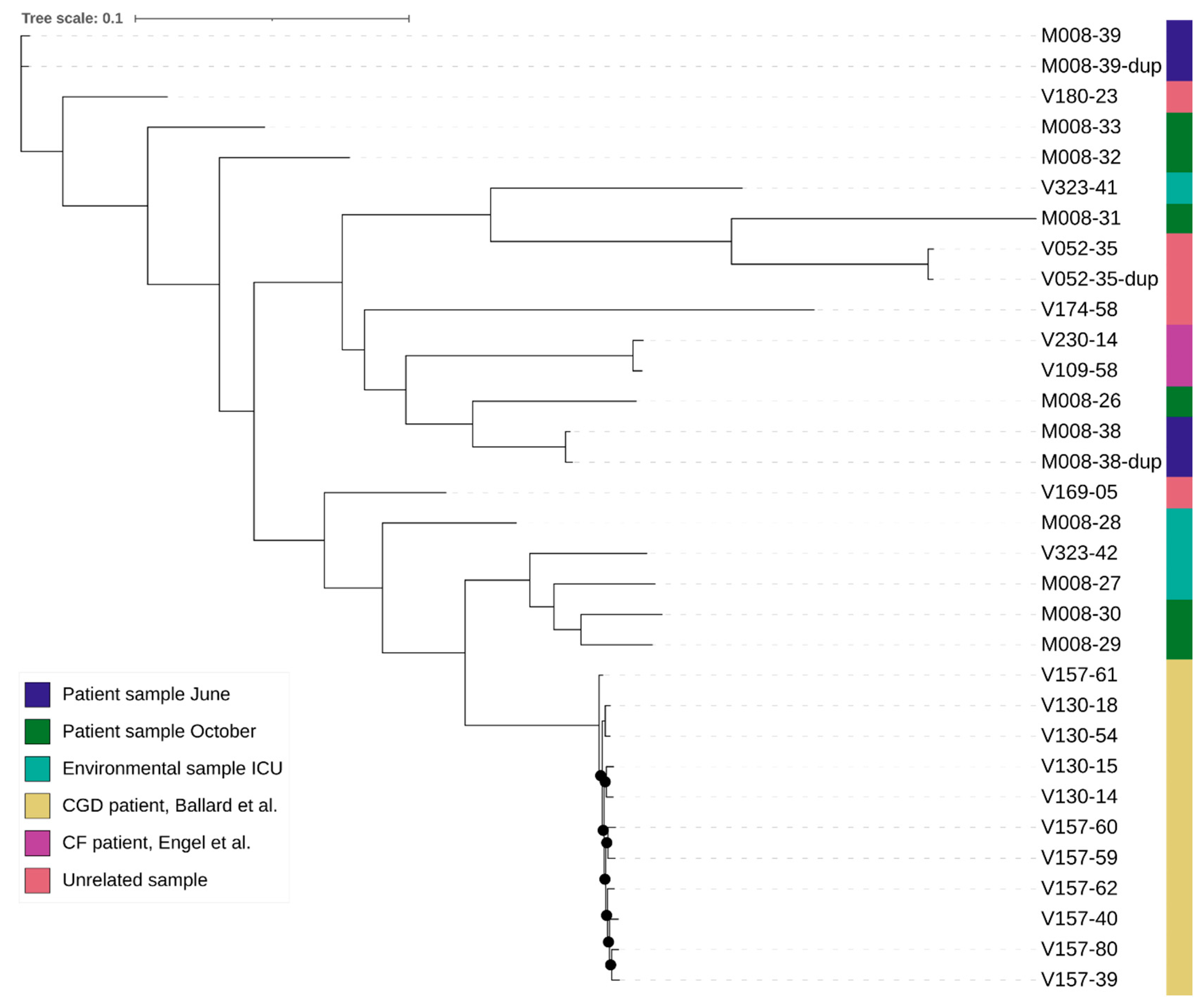
| Sample Name | Origin | Time of Sampling |
|---|---|---|
| V109-58 | CF patient, Engel et al. [30] | 2010 |
| V230-14 | CF patient, Engel et al. [30] | 2017 |
| V130-14 | CGD patient, Ballard et al. [29] | 2011 |
| V130-15 | CGD patient, Ballard et al. [29] | 2011 |
| V130-18 | CGD patient, Ballard et al. [29] | 2011 |
| V130-54 | CGD patient, Ballard et al. [29] | 2011 |
| V157-39 | CGD patient, Ballard et al. [29] | 2013 |
| V157-40 | CGD patient, Ballard et al. [29] | 2013 |
| V157-59 | CGD patient, Ballard et al. [29] | 2013 |
| V157-60 | CGD patient, Ballard et al. [29] | 2013 |
| V157-61 | CGD patient, Ballard et al. [29] | 2013 |
| V157-62 | CGD patient, Ballard et al. [29] | 2013 |
| V157-80 | CGD patient, Ballard et al. [29] | 2013 |
| M008-27 | Environmental sample ICU | October 2020 |
| M008-28 | Environmental sample ICU | October 2020 |
| V323-41 | Environmental sample ICU | October 2020 |
| V323-42 | Environmental sample ICU | October 2020 |
| NRRL-4585 | Outlier | does not apply |
| M008-38 * | Patient sample June | June 2020 |
| M008-39 * | Patient sample June | June 2020 |
| M008-26 | Sample October patient 1 | October 2020 |
| M008-29 | Sample October patient 2 | October 2020 |
| M008-30 | Sample October patient 3 | October 2020 |
| M008-31 | Sample October patient 4 | October 2020 |
| M008-32 | Sample October patient 5 | October 2020 |
| M008-33 | Sample October patient 6 | October 2020 |
| V052-35 * | Unrelated patient sample | 2006 |
| V169-05 | Unrelated patient sample | 2014 |
| V174-58 | Unrelated patient sample | 2015 |
| V180-23 | Unrelated patient sample | 2015 |
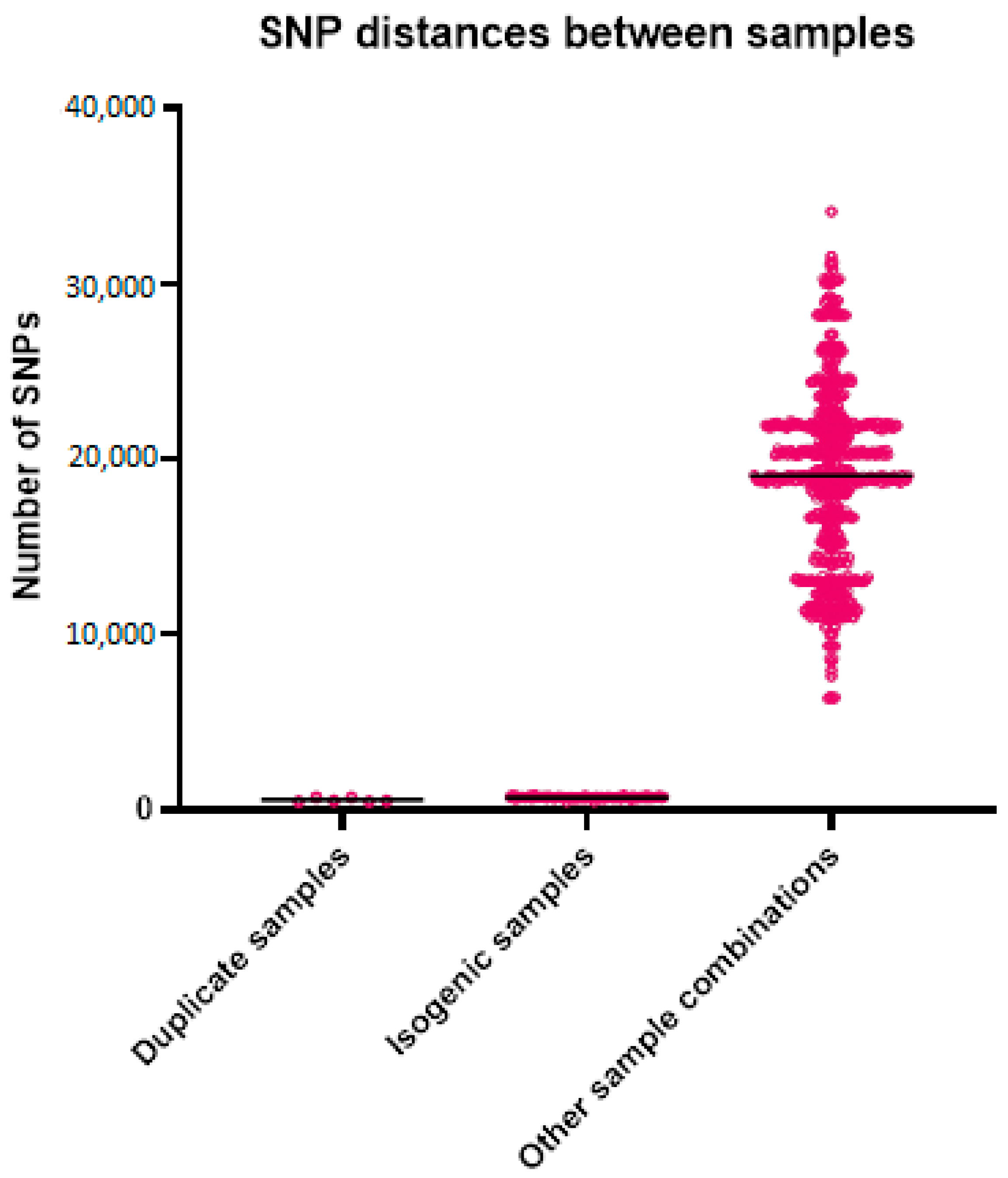
| Duplicate Samples | Isogenic Samples | Other Sample Combinations | |
|---|---|---|---|
| Number of values | 6 | 112 | 874 |
| Minimum | 469 | 451 | 6330 |
| Maximum | 705 | 863 | 34,104 |
| Range | 236 | 412 | 27,774 |
| Mean | 563 | 696 | 19,055 |
| Std. Deviation | 112 | 64 | 5244 |
| Std. Error of Mean | 46 | 6.0 | 177 |
| Sample | STR2 | STR3 | STR4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| A | B | C | A | B | C | A | B | C | |
| M008-38 | 22 | 18 | 15 | 102 | 11 | 17 | 21 | 10 | 9 |
| M008-38-dup | 22 | 18 | 15 | 102 | 11 | 16 | 21 | 10 | 9 |
| M008-39 | 24 | 18 | 12 | 52 | 7 | 11 | 9 | 8 | 5 |
| M008-39-dup | 24 | 18 | 12 | 52 | 7 | 11 | 9 | 8 | 5 |
| M008-30 | 17 | 27 | 4 | 28 | 9 | 20 | 6 | 7 | 5 |
| M008-28 | 28 | 16 | 11 | 28 | 10 | 20 | 6 | 7 | 6 |
| M008-27 | 17 | 10 | 5 | 37 | 9 | 27 | 7 | 7 | 9 |
| M008-26 | 22 | 18 | 17 | 27 | 19 | 16 | 8 | 16 | 7 |
| M008-33 | 17 | 24 | 11 | 25 | 10 | 8 | 25 | 8 | 7 |
| M008-29 | 10 | 10 | 5 | 29 | 20 | 19 | 7 | 6 | 5 |
| M008-31 | 13 | 19 | 8 | 25 | 8 | 9 | 6 | 8 | 25 |
| M008-32 | 24 | 21 | 13 | 22 | 8 | 26 | 8 | 8 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiel, S.J.P.; Hendriks, A.C.A.; Eijkenboom, J.J.A.; Bosch, T.; Coolen, J.P.M.; Melchers, W.J.G.; Anröchte, P.; Camps, S.M.T.; Verweij, P.E.; Zhang, J.; et al. Aspergillus Outbreak in an Intensive Care Unit: Source Analysis with Whole Genome Sequencing and Short Tandem Repeats. J. Fungi 2024, 10, 51. https://doi.org/10.3390/jof10010051
Hiel SJP, Hendriks ACA, Eijkenboom JJA, Bosch T, Coolen JPM, Melchers WJG, Anröchte P, Camps SMT, Verweij PE, Zhang J, et al. Aspergillus Outbreak in an Intensive Care Unit: Source Analysis with Whole Genome Sequencing and Short Tandem Repeats. Journal of Fungi. 2024; 10(1):51. https://doi.org/10.3390/jof10010051
Chicago/Turabian StyleHiel, Stephan J. P., Amber C. A. Hendriks, Jos J. A. Eijkenboom, Thijs Bosch, Jordy P. M. Coolen, Willem J. G. Melchers, Paul Anröchte, Simone M. T. Camps, Paul E. Verweij, Jianhua Zhang, and et al. 2024. "Aspergillus Outbreak in an Intensive Care Unit: Source Analysis with Whole Genome Sequencing and Short Tandem Repeats" Journal of Fungi 10, no. 1: 51. https://doi.org/10.3390/jof10010051
APA StyleHiel, S. J. P., Hendriks, A. C. A., Eijkenboom, J. J. A., Bosch, T., Coolen, J. P. M., Melchers, W. J. G., Anröchte, P., Camps, S. M. T., Verweij, P. E., Zhang, J., & Dommelen, L. v. (2024). Aspergillus Outbreak in an Intensive Care Unit: Source Analysis with Whole Genome Sequencing and Short Tandem Repeats. Journal of Fungi, 10(1), 51. https://doi.org/10.3390/jof10010051