
Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival
 , , ,
, , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
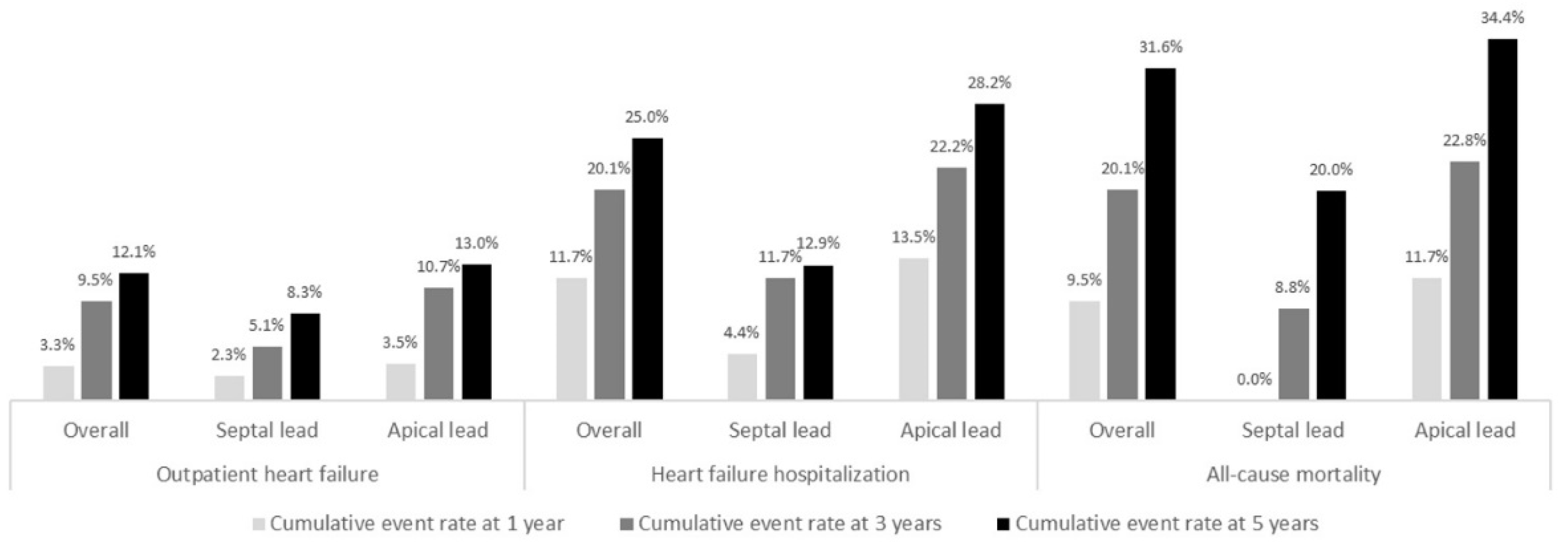
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mond, H.G.; Proclemer, A. The 11th World Survey of Cardiac Pacing and Implantable Cardioverter-Defibrillators: Calendar Year 2009—A World Society of Arrhythmia’s Project. Pacing Clin. Electrophysiol. 2011, 34, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- Tayal, B.; Fruelund, P.; Sogaard, P.; Riahi, S.; Polcwiartek, C.; Atwater, B.D.; Gislason, G.; Risum, N.; Torp-Pedersen, C.; Kober, L.; et al. Incidence of heart failure after pacemaker implantation: A nationwide Danish Registry-based follow-up study. Eur. Heart J. 2019, 40, 3641–3648. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, S.; Epstein, A.E.; Verdino, R.J.; Lin, D.; Goldberg, L.R.; Marchlinski, F.E.; Frankel, D.S. Incidence and predictors of right ventricular pacing-induced cardiomyopathy. Heart Rhythm 2014, 11, 1619–1625. [Google Scholar] [CrossRef]
- Kiehl, E.L.; Makki, T.; Kumar, R.; Gumber, D.; Kwon, D.H.; Rickard, J.W.; Kanj, M.; Wazni, O.M.; Saliba, W.I.; Varma, N.; et al. Incidence and predictors of right ventricular pac-ing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm 2016, 13, 2272–2278. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Bordachar, P.; Ellenbogen, K.A. The Continued Search for Physiological Pacing: Where Are We Now? J. Am. Coll. Cardiol. 2017, 69, 3099–3114. [Google Scholar] [CrossRef] [PubMed]
- Bai, M.; Li, Q.; Jiang, G.; Zhang, L.; Wang, T.; Zhang, Z. Comparison of effectiveness of right ventricular mid-septal pacing vs. apical pacing: A randomized-controlled trials. Eur. Heart J. Suppl. 2016, 18, F12–F18. [Google Scholar] [CrossRef]
- Saito, M.; Kaye, G.; Negishi, K.; Linker, N.; Gammage, M.; Kosmala, W.; Marwick, T.H. Dyssynchrony, contraction efficiency and regional function with apical and non-apical RV pacing. Heart 2015, 101, 600–608. [Google Scholar] [CrossRef]
- Choudhary, D.; Chaurasia, A.K.; Kumar, S.M.; Arulkumar, A.; Thajudeen, A.; Namboodiri, N.; Sanjay, G.; Abhilash, S.; Ajitkumar, V.; Ja, T. Radial left ventricular dyssynchrony by speckle tracking in apical versus non apical right ventricular pacing- evidence of dyssynchrony on medium term follow up. J. Cardiovasc. Thorac. Res. 2016, 8, 20–25. [Google Scholar] [CrossRef]
- Zou, C.; Song, J.; Li, H.; Huang, X.; Liu, Y.; Zhao, C.; Shi, X.; Yang, X. Right Ventricular Outflow Tract Septal Pacing Is Superior to Right Ventricular Apical Pacing. J. Am. Heart Assoc. 2015, 4, e001777. [Google Scholar] [CrossRef]
- Rimbas, R.C.; Margulescu, A.D.; Siliste, C.; Vinereanu, D. Left ventricular strain analysis reveals better synchrony and diastolic function for septal versus apical right ventricular permanent pacing. Maedica 2014, 9, 232–241. [Google Scholar]
- Kaye, G.C.; Linker, N.J.; Marwick, T.H.; Pollock, L.; Graham, L.; Pouliot, E.; Poloniecki, J.; Gammage, M.; Martin, P.; Pepper, C.; et al. Effect of right ventricular pacing lead site on left ventricular function in patients with high-grade atrioventricular block: Results of the Protect-Pace study. Eur. Heart J. 2015, 36, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Spath, N.B.; Wang, K.; Venkatasumbramanian, S.; Fersia, O.; E Newby, D.; Lang, C.C.; Grubb, N.R.; Dweck, M.R. Complications and prognosis of patients undergoing apical or septal right ventricular pacing. Open Heart 2019, 6, e000962. [Google Scholar] [CrossRef]
- Mizukami, A.; Matsue, Y.; Naruse, Y.; Kowase, S.; Kurosaki, K.; Suzuki, M.; Matsumura, A.; Nogami, A.; Aonuma, K.; Hashimoto, Y. Implications of right ventricular septal pacing for medium-term prognosis: Propensity-matched analysis. Int. J. Cardiol. 2016, 220, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.-A.; Cleland, J.G.F.; Deharo, J.-C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and re-synchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 2013, 34, 2281–2329. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Parakh, N.; Gupta, A.; Juneja, R.; Naik, N.; Yadav, R.; Sharma, G.; Roy, A.; Verma, S.K.; Bahl, V.K. Incidence and predictors of pacemaker-induced cardiomyopathy with comparison between apical and non-apical right ventricular pacing sites. J. Interv. Card. Electrophysiol. 2019, 56, 63–70. [Google Scholar] [CrossRef]
- Molina, L.; Sutton, R.; Gandoy, W.; Reyes, N.; Lara, S.; Limón, F.; Gómez, S.; Orihuela, C.; Salame, L.; Moreno, G. Medium-Term Effects of Septal and Apical Pacing in Pacemaker-Dependent Patients: A Double-Blind Prospective Randomized Study. Pacing Clin. Electrophysiol. 2014, 37, 207–214. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Docherty, K.F.; Jhund, P.S.; Anand, I.; Bengtsson, O.; Böhm, M.; De Boer, R.A.; DeMets, D.L.; Desai, A.S.; Drozdz, J.; Howlett, J.; et al. Effect of Dapagliflozin on Outpatient Worsening of Patients with Heart Failure and Reduced Ejection Fraction: A Prespecified Analysis of DAPA-HF. Circulation 2020, 142, 1623–1632. [Google Scholar] [CrossRef]
- Yusu, S.; Mera, H.; Hoshida, K.; Miyakoshi, M.; Miwa, Y.; Tsukada, T.; Yoshino, H.; Ikeda, T. Selective site pacing from the right ventricular mid-septum: Follow-up of lead performance and procedure technique. Int. Heart J. 2012, 53, 113–116. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yamagata, K.; Ishibashi, K.; Wakamiya, A.; Shimamoto, K.; Ueda, N.; Kamakura, T.; Wada, M.; Inoue, Y.; Miyamoto, K.; Noda, T.; et al. Comparison Between Septal Pacing With the Catheter Delivery System and Apical Pacing With the Stylet Delivery System for Ventricular Lead Placement: A Randomized Controlled Trial. Circ. Arrhythmia Electrophysiol. 2021, 14, e010362. [Google Scholar] [CrossRef] [PubMed]
- Witt, C.M.; Lenz, C.J.; Shih, H.H.; Ebrille, E.; Rosenbaum, A.N.; Van Zyl, M.; Aung, H.; Manocha, K.K.; Deshmukh, A.J.; Ms, D.O.H.; et al. Right ventricular pacemaker lead position is associated with differences in long-term outcomes and complications. J. Cardiovasc. Electrophysiol. 2017, 28, 924–930. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | Overall (n = 251) | Septal (n = 47) | Apical (n = 204) | p Value |
|---|---|---|---|---|
| Age (years), mean (SD) | 76.5 (11.3) | 72.2 (11.4) | 77.4 (11.1) | 0.004 |
| Men | 129 (51.4%) | 32 (68.1%) | 97 (47.5%) | 0.008 |
| BMI (Kg/m2), mean (SD) | 28.0 (5.2) | 26.6 (4.3) | 28.4 (5.4) | 0.01 |
| Hypertension | 190 (75.7%) | 31 (66.0%) | 159 (77.9%) | 0.07 |
| Dyslipidemia | 131 (52.2%) | 27 (57.4%) | 104 (51.0%) | 0.26 |
| Diabetes mellitus | 80 (32.0%) | 16 (34.0%) | 64 (31.5%) | 0.43 |
| Insulin-treated | 23 (9.3%) | 2 (4.5%) | 21 (10.3%) | 0.23 |
| Smoker | 53 (21.1%) | 11 (23.4%) | 42 (20.6%) | 0.40 |
| Coronary artery disease | 48 (19.1%) | 14 (29.8%) | 34 (16.7%) | 0.04 |
| Heart failure | 92 (36.7%) | 15 (31.9%) | 77 (37.7%) | 0.28 |
| Atrial fibrillation | 101 (40.2%) | 26 (55.3%) | 75 (36.8%) | 0.02 |
| Peripheral artery disease | 9 (3.6%) | 2 (4.3%) | 7 (3.4%) | 0.78 |
| Chronic kidney disease | 66 (26.3%) | 9 (19.1%) | 57 (27.9%) | 0.15 |
| Hemoglobin (g/dL), mean (SD) | 12.9 (1.8) | 13.5 (1.8) | 12.7 (1.7) | 0.01 |
| Serum creatinine, median (IQR) | 0.98 (0.80–1.34) | 0.90 (0.78–1.22) | 1.00 (0.80–1.40) | 0.14 |
| Medication prior to pacemaker implantation | ||||
| Antiplatelet | 89 (36.0) | 10 (22.7%) | 79 (38.9%) | 0.03 |
| Vitamin K antagonist | 49 (19.8) | 13 (29.5%) | 36 (17.7%) | 0.06 |
| Novel oral anticoagulant | 27 (10.9) | 8 (18.2%) | 19 (9.4%) | 0.09 |
| Beta-blocker | 59 (23.8) | 9 (20.5%) | 50 (24.5%) | 0.36 |
| Ivabradine | 1 (0.4) | 1 (2.3%) | 0 | 0.18 |
| Cardiac glycoside | 7 (2.8%) | 2 (4.5%) | 5 (2.5%) | 0.45 |
| ACE-I/ARB | 142 (57.3%) | 21 (47.7%) | 121 (59.3%) | 0.38 |
| MRA | 10 (4.0%) | 0 | 10 (4.9%) | 0.13 |
| Loop diuretic | 88 (35.5%) | 12 (27.3%) | 76 (37.3%) | 0.14 |
| LVEF (%), mean (SD) | 54.1 (7.5) | 53.7 (7.5) | 54.2 (7.6) | 0.71 |
| LVEF < 50% | 36 (17.0%) | 10 (24.4%) | 26 (15.2%) | 0.12 |
| RV systolic dysfunction | 12 (5.7%) | 2 (5.0%) | 10 (5.8%) | 0.84 |
| Severe LVH | 6 (2.8%) | 0 | 6 (3.5%) | 0.23 |
| Large pericardial effusion | 2 (1.0%) | 0 | 2 (1.2%) | 0.49 |
| Severe AS | 9 (4.3%) | 2 (5.0%) | 7 (4.1%) | 0.80 |
| Significant MS | 2 (0.9%) | 0 | 2 (1.2%) | 0.49 |
| Severe MR | 1 (0.5%) | 0 | 1 (0.6%) | 0.63 |
| Severe TR | 3 (1.4%) | 1 (2.5%) | 2 (1.2%) | 0.52 |
| Pacemaker indication | ||||
| Sinus node disease | 38 (15.1%) | 3 (6.4%) | 35 (17.2%) | 0.04 |
| Atrioventricular block | 174 (69.3%) | 40 (85.1%) | 134 (65.7%) | 0.006 |
| Tachycardia-bradycardia syndrome | 39 (15.5%) | 4 (8.5%) | 35 (17.2%) | 0.10 |
| QRS duration (milliseconds), mean (SD) | 116.0 (25.8) | 112.5 (22.6) | 116.6 (26.4) | 0.36 |
| Dual-chamber pacemaker | 170 (67.7%) | 25 (53.2%) | 145 (71.1%) | 0.02 |
| Radiation time, median (IQR) | 3.2 (1.6–5.5) | 3.3 (2.3–5.5) | 3.1 (1.6–5.5) | 0.53 |
| In-hospital mortality | 7 (2.8%) | 1 (2.1%) | 6 (2.9%) | 0.76 |
| Follow-Up | Overall (n = 244) | Septal (n = 46) | Apical (n = 198) | p Value |
|---|---|---|---|---|
| Follow-up time, median (IQR) | 5.2 (3.0–5.5) | 5.3 (5.1–5.5) | 5.1 (2.6–5.4) | 0.01 |
| QRS duration during RV pacing (milliseconds), mean (SD) | 171.1 (21.1) | 159.0 (13.3) | 173.9 (21.6) | <0.001 |
| Pacemaker complications | ||||
| Pocket infection | 2 (0.8%) | 1 (2.1%) | 1 (0.5%) | 0.26 |
| Pocket hematoma | 2 (0.8%) | 1 (2.1%) | 1 (0.5%) | 0.26 |
| Subclavian vein thrombosis | 1 (0.4%) | 0 | 1 (0.5%) | 0.63 |
| Diaphragm stimulation requiring lead repositioning | 1 (0.4%) | 1 (2.1%) | 0 | 0.19 |
| Pacemaker related endocarditis | 1 (0.4%) | 1 (2.1%) | 0 | 0.19 |
| Heart failure | 89 (37.1%) | 11 (23.9%) | 78 (40.2%) | 0.03 |
| Outpatient | 29 (12.1%) | 4 (8.7%) | 25 (12.9%) | 0.31 |
| Hospitalization | 60 (25.0%) | 7 (15.2%) | 53 (27.3%) | 0.06 |
| Time-to-heart failure, median (IQR) | 1.5 (0.6–3.3) | 2.9 (0.9–4.5) | 1.5 (0.6–3.2) | 0.16 |
| All-cause mortality | 83 (34.2%) | 9 (19.6%) | 74 (37.6%) | 0.01 |
| Time-to-death, median (IQR) | 2.6 (0.9–4.2) | 3.1 (2.0–4.4) | 2.3 (0.8–4.3) | 0.31 |
| RV pacing percentage | 84 (16–99) | 85 (18–98) | 84 (16–99) | 0.99 |
| RV pacing percentage ≥ 40% | 139 (66.5%) | 29 (70.7%) | 110 (65.5%) | 0.33 |
| LVEF (%), mean (SD) | 50.9 (9.9) | 50.1 (9.2) | 51.2 (10.2) | 0.56 |
| LVEF < 50% | 48 (35.6%) | 15 (45.5%) | 33 (32.4%) | 0.12 |
| Upgrade to CRT | 6 (2.5%) | 3 (6.5%) | 3 (1.5%) | 0.05 |
| Medication during follow-up | ||||
| Antiplatelet | 76 (32.3%) | 11 (25.0%) | 65 (34.0%) | 0.17 |
| Vitamin K antagonist | 41 (17.4%) | 13 (29.5%) | 28 (14.7%) | 0.02 |
| Novel oral anticoagulant | 55 (23.4%) | 14 (31.8%) | 41 (21.5%) | 0.11 |
| Beta-blocker | 96 (40.9%) | 19 (43.2%) | 77 (40.3%) | 0.43 |
| Ivabradine | 4 (1.7%) | 2 (4.5%) | 2 (1.0%) | 0.11 |
| Cardiac glycoside | 18 (7.7%) | 3 (6.8%) | 15 (7.9%) | 0.82 |
| ACE-I/ARB | 113 (48.3%) | 25 (56.8%) | 88 (46.3%) | 0.14 |
| ARNI | 5 (2.1%) | 2 (4.5%) | 3 (1.6%) | 0.22 |
| MRA | 17 (7.2%) | 4 (9.1%) | 13 (6.8%) | 0.60 |
| Loop diuretic | 120 (51.0%) | 19 (43.2%) | 101 (52.9%) | 0.16 |
| SGLT2 inhibitor | 10 (4.3%) | 4 (9.1%) | 6 (3.1%) | 0.08 |
| GLP-1 receptor agonist | 2 (0.9%) | 1 (2.3%) | 1 (0.5%) | 0.26 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR 95% CI | p Value | HR 95% CI | p Value | |
| Age (years) | 1.04 (1.01–1.06) | 0.002 | 1.01 (0.99–1.04) | 0.46 |
| Men | 1.25 (0.82–1.89) | 0.30 | 1.59 (0.95–2.65) | 0.08 |
| Hypertension | 1.53 (0.89–2.63) | 0.12 | - | - |
| Dyslipidemia | 1.65 (1.07–2.55) | 0.02 | - | - |
| Diabetes mellitus | 1.57 (1.03–2.40) | 0.04 | - | - |
| Smoker | 1.62 (1.03–2.56) | 0.04 | - | - |
| Coronary artery disease | 1.97 (1.23–3.15) | 0.005 | 1.66 (0.95–2.91) | 0.08 |
| Heart failure | 3.84 (2.50–5.89) | <0.001 | 3.22 (1.88–5.5) | <0.001 |
| Atrial fibrillation | 1.60 (1.05–2.42) | 0.03 | - | - |
| Chronic kidney disease | 1.97 (1.25–3.09) | 0.003 | - | - |
| Hemoglobin (g/dL) | 0.85 (0.76–0.96) | 0.008 | - | - |
| Serum creatinine (mg/dL) | 1.13 (0.97–1.31) | 0.11 | - | - |
| LVEF < 50% | 2.55 (1.55–4.22) | <0.001 | 1.46 (0.76–2.79) | 0.26 |
| RV systolic disfunction | 1.26 (0.46–3.46) | 0.65 | - | - |
| Severe AS | 6.20 (2.66–14.42) | <0.001 | 10.88 (3.25–36.44) | <0.001 |
| Significant MS | 1.71 (0.24–12.35) | 0.60 | - | - |
| Severe MR | 4.35 (0.60–31.64) | 0.15 | - | - |
| Severe TR | 1.68 (0.41–6.86) | 0.47 | - | - |
| RVA pacing | 2.08 (1.11–4.00) | 0.02 | 3.32 (1.48–7.46) | 0.004 |
| RV pacing percentage | 1.00 (0.99–1.01) | 0.90 | 1.00 (0.99–1.01) | 0.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias-Frias, A.; Costa, R.; Campinas, A.; Alexandre, A.; Sá-Couto, D.; Sousa, M.J.; Roque, C.; Vieira, P.; Lagarto, V.; Reis, H.; et al. Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival. J. Cardiovasc. Dev. Dis. 2022, 9, 444. https://doi.org/10.3390/jcdd9120444
Dias-Frias A, Costa R, Campinas A, Alexandre A, Sá-Couto D, Sousa MJ, Roque C, Vieira P, Lagarto V, Reis H, et al. Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival. Journal of Cardiovascular Development and Disease. 2022; 9(12):444. https://doi.org/10.3390/jcdd9120444
Chicago/Turabian StyleDias-Frias, André, Ricardo Costa, Andreia Campinas, André Alexandre, David Sá-Couto, Maria João Sousa, Carla Roque, Pinheiro Vieira, Vitor Lagarto, Hipólito Reis, and et al. 2022. "Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival" Journal of Cardiovascular Development and Disease 9, no. 12: 444. https://doi.org/10.3390/jcdd9120444
APA StyleDias-Frias, A., Costa, R., Campinas, A., Alexandre, A., Sá-Couto, D., Sousa, M. J., Roque, C., Vieira, P., Lagarto, V., Reis, H., & Torres, S. (2022). Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival. Journal of Cardiovascular Development and Disease, 9(12), 444. https://doi.org/10.3390/jcdd9120444