
Both Alcoholic and Non-Alcoholic Liver Cirrhosis Are Associated with an Increased Risk of HF—A Cohort Study Including 75,558 Patients

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Database
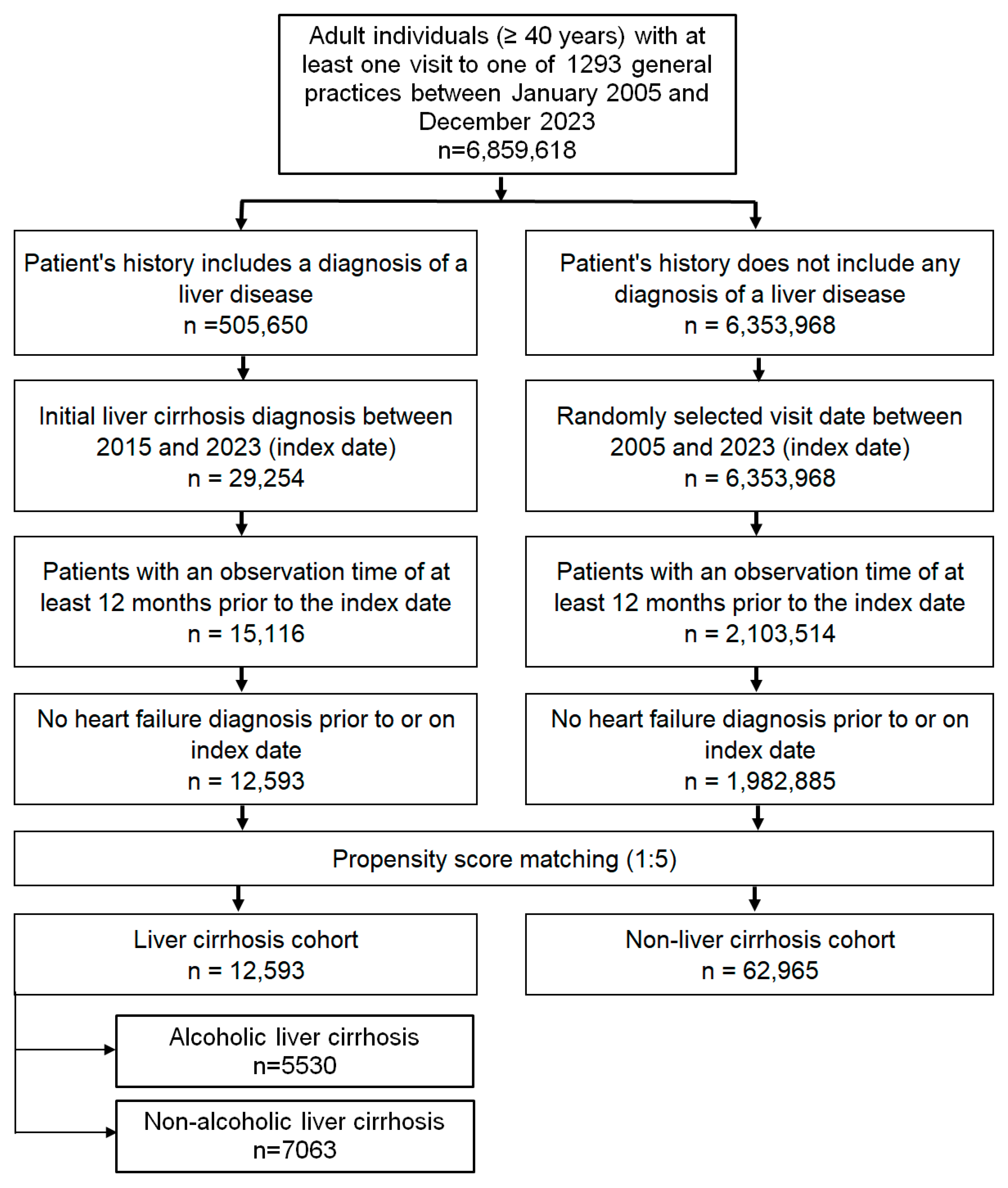
2.2. Study Population
2.3. Study Outcomes
2.4. Statistical Analyses
2.5. Ethical Standards
3. Results
3.1. Baseline Characteristics
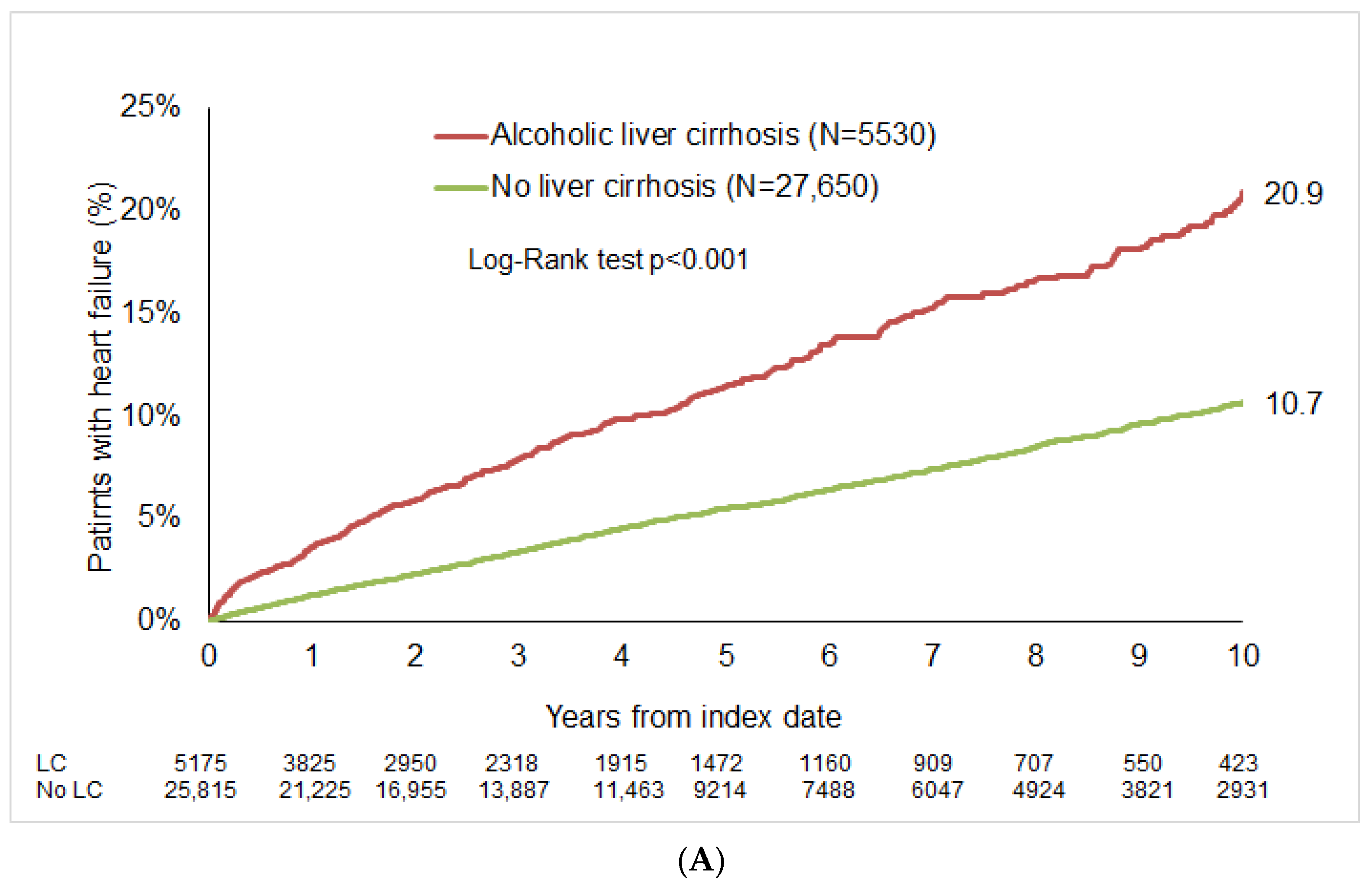
3.2. Cumulative Incidence of HF
3.3. Association Between LC and HF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of liver diseases in the world. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef]
- Lange, C.M.; Trebicka, J.; Gerbes, A.; Canbay, A.; Geier, A.; Merle, U.; Peck-Radosavljevic, M.; Tacke, F.; Vogelmann, T.; Theis, S.; et al. Limited access to liver transplantation and TIPS despite high mortality, healthcare resource use and costs of cirrhosis in Germany. Liver Int. 2023, 43, 2503–2512. [Google Scholar] [CrossRef]
- Wu, H.H.L.; Rakisheva, A.; Ponnusamy, A.; Chinnadurai, R. Hepatocardiorenal syndrome in LC: Recognition of a new entity? World J. Gastroenterol. 2024, 30, 128–136. [Google Scholar] [CrossRef]
- Xanthopoulos, A.; Starling, R.C.; Kitai, T.; Triposkiadis, F. HF and Liver Disease: Cardiohepatic Interactions. JACC Heart Fail. 2019, 7, 87–97. [Google Scholar] [CrossRef]
- Agarwal, P.; Phalke, A.; Rijhwani, P. Incidence of Cardiovascular Dysfunction in Patients with LC—A Hospital Based Observational Study. Int. J. Sci. Res. 2024, 13, 8. [Google Scholar] [CrossRef]
- Pelouch, R.; Praus, R.; Vašatová, M.; Hůlek, P. HF in patients with LC. Cor. Et. Vasa. 2023, 55, e391–e396. [Google Scholar] [CrossRef]
- Chuzi, S.; Tanaka, Y.; Bavishi, A.; Bruce, M.; Van Wagner, L.B.; Wilcox, J.E.; Ahmad, F.S.; Ladner, D.P.; Lagu, T.; Khan, S.S. Association Between End-Stage Liver Disease and Incident HF in an Integrated Health System. J. Gen. Intern. Med. 2023, 38, 2445–2452. [Google Scholar] [CrossRef]
- Li, W.; Wen, W.; Xie, D.; Qiu, M.; Cai, X.; Zheng, S.; Huang, Y. Association between non-alcoholic fatty liver disease and risk of incident HF: A meta-analysis of observational studies. Ther. Adv. Chronic. Dis. 2022, 13, 20406223221119626. [Google Scholar] [CrossRef]
- Simon, T.G.; Roelstraete, B.; Hagström, H.; Sundström, J.; Ludvigsson, J.F. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: Results from a nationwide histology cohort. Gut 2022, 71, 1867–1875. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, G.; Kim, H.; Lee, J.; Lee, Y.B.; Jin, S.M.; Hur, K.Y.; Kim, J.H. The association of hepatic steatosis and fibrosis with HF and mortality. Cardiovasc. Diabetol. 2021, 20, 197. [Google Scholar] [CrossRef]
- Hashemi, L.; Pisegna, J.; Budoff, M.; Li, N.; Nguyen, M.T.T.; Ebrahimi, R.; Chu, E.; Streja, E.; Elashoff, D.; Ganz, T. Association of Cirrhosis and Increased Risk of Cardiovascular Events in a VA Patient Population, A Retrospective Cohort Study. Arch. Intern. Med. Res. 2020, 3, 210–229. [Google Scholar] [CrossRef]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef]
- Labenz, C.; Wörns, M.A.; Adarkwah, C.C.; Galle, P.R.; Schattenberg, J.M.; Kostev, K. Proton pump inhibitors increase risk of bone fractures in men with cirrhosis: A population-based study. Aliment. Pharmacol. Ther. 2020, 52, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Luedde, M.; Schmidt, V.J.; Gänsbacher-Kunzendorf, J.; Kostev, K. Association Between Carpal Tunnel Syndrome and Subsequent HF Among Adults in Germany. JAMA Netw. Open. 2023, 6, e2323091. [Google Scholar] [CrossRef]
- Sedighi, J.; Luedde, M.; Gaensbacher-Kunzendorf, J.; Hippe, H.J.; Bauer, P.; Assmus, B.; Sossalla, S.; Kostev, K. Association between sleep disorders and subsequent HF. Int. J. Cardiol. Heart Vasc. 2025, 57, 101618. [Google Scholar] [CrossRef]
- Karki, N.; Kc, S.; Sharma, D.; Jaisi, B.; Khadka, S. Cardiac Dysfunction in Patients with LC. J. Nepal. Health Res. Counc. 2019, 17, 357–361. [Google Scholar] [CrossRef]
- Koch, D.G.; Rockey, D.C.; Litwin, S.S.; Tedford, R.J. H2FPEF Scores Are Increased in Patients with NASH Cirrhosis and Are Associated with Post-liver Transplant HF. Dig. Dis. Sci. 2024, 69, 3061–3068. [Google Scholar] [CrossRef] [PubMed]
- Fialla, A.D.; Thiesson, H.C.; Bie, P.; Schaffalitzky de Muckadell, O.B.; Krag, A. Internal dysregulation of the renin system in patients with stable LC. Scand. J. Clin. Lab. Investig. 2017, 77, 298–309. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Wang, Y.; Li, J.; Liu, Y.; Liu, Y.; Wang, Y.; Wang, Y.; Wang, Y.; Wang, Y. Interplay of Liver-Heart Inflammatory Axis and Cannabinoid 2 Receptor in the Development of Hepatic Cardiomyopathy. Hepatology 2019, 70, 1830–1845. [Google Scholar] [CrossRef]
- Domínguez, F.; Adler, E.; García-Pavía, P. Alcoholic cardiomyopathy: An update. Eur. Heart J. 2024, 45, 2294–2305. [Google Scholar] [CrossRef]
- Day, E.; Rudd, J.H.F. Alcohol use disorders and the heart. Addiction 2019, 114, 1670–1678. [Google Scholar] [CrossRef]
- Rasoul, D.; Ajay, A.; Abdullah, A.; Mathew, J.; Lee Wei En, B.; Mashida, K.; Sankaranarayanan, R. Alcohol and HF. Eur Cardiol. 2023, 18, e65. [Google Scholar] [CrossRef]
- Lee, H.; Kim, G.; Choi, Y.J.; Huh, B.W.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Lee, E.J.; Lee, Y.H.; Huh, K.B. Association between Non-Alcoholic Steatohepatitis and Left Ventricular Diastolic Dysfunction in Type 2 Diabetes Mellitus. Diabetes Metab. J. 2020, 44, 267–276. [Google Scholar] [CrossRef]
- Roderburg, C.; Krieg, S.; Krieg, A.; Vaghiri, S.; Mohr, R.; Konrad, M.; Luedde, M.; Luedde, T.; Kostev, K.; Loosen, S.H. Non-Alcoholic Fatty Liver Disease (NAFLD) and risk of new-onset HF: A retrospective analysis of 173,966 patients. Clin. Res. Cardiol. 2023, 112, 1446–1453. [Google Scholar] [CrossRef]
- Pérez-López, F.R.; Larrad-Mur, L.; Kallen, A.; Chedraui, P.; Taylor, H.S. Gender differences in cardiovascular disease: Hormonal and biochemical influences. Reprod. Sci. 2010, 17, 511–531. [Google Scholar] [CrossRef]
- Vitale, C.; Mendelsohn, M.E.; Rosano, G.M. Gender differences in the cardiovascular effect of sex hormones. Nat. Rev. Cardiol. 2009, 6, 532–542. [Google Scholar] [CrossRef]
- Regitz-Zagrosek, V.; Gebhard, C. Gender medicine: Effects of sex and gender on cardiovascular disease manifestation and outcomes. Nat. Rev. Cardiol. 2023, 20, 236–247. [Google Scholar] [CrossRef]
- Noble, N.; Paul, C.; Turon, H.; Oldmeadow, C. Which modifiable health risk behaviours are related? A systematic review of the clustering of Smoking, Nutrition, Alcohol and Physical activity (‘SNAP’) health risk factors. Prev. Med. 2015, 81, 16–41. [Google Scholar] [CrossRef]
- Moon, A.M.; Singal, A.G.; Tapper, E.B. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 18, 2650–2666. [Google Scholar] [CrossRef]
- Matovic Zaric, V.; Pantic, I.; Lugonja, S.; Glisic, T.; Konjikusic, S.; Lolic, I.; Baljosevic, N.; Zgradic, S.; El Mezeni, J.; Vojnovic, M.; et al. Survival of Patients with Alcohol-Related Liver Disease Cirrhosis-Usefulness of the New Liver Mortality Inpatients Prognostic Score. Diagnostics 2024, 14, 2508. [Google Scholar] [CrossRef]
- Wang, P.L.; Djerboua, M.; Flemming, J.A. Cause-specific mortality among patients with cirrhosis in a population-based cohort study in Ontario (2000–2017). Hepatol. Commun. 2023, 7, e00194. [Google Scholar] [CrossRef] [PubMed]
- Olave, M.C.; Gurung, A.; Mistry, P.K.; Kakar, S.; Yeh, M.; Xu, M.; Wu, T.T.; Torbenson, M.; Jain, D. Etiology of cirrhosis in the young. Hum Pathol. 2020, 96, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; Terrault, N.A.; Tacke, F.; Gluud, L.L.; Arrese, M.; Bugianesi, E.; Loomba, R. Global epidemiology of cirrhosis-aetiology, trends and predictions. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 388–398. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | Proportion Among Patients with Alcoholic LC (N, %) N = 5530 | Proportion Among Patients Without LC (N, %) N = 27,650 | SMD | Proportion Among Patients with Non-Alcoholic LC (N, %) N = 7063 | Proportion Among Patients Without LC (N, %) N = 35,315 | SMD |
|---|---|---|---|---|---|---|
| Age (Mean, SD) | 60.0 (10.5) | 59.9 (10.7) | 0.008 | 65.6 (11.4) | 65.8 (11.6) | −0.020 |
| Age < 60 | 2811 (50.8) | 14,177 (51.3) | 2211 (31.3) | 11,065 (31.3) | ||
| Age 60–69 | 1691 (30.6) | 8238 (29.8) | 2150 (30.4) | 10,555 (29.9) | ||
| Age 70+ | 1028 (18.6) | 5235 (18.9) | 2702 (38.3) | 13,695 (38.8) | ||
| Female | 1693 (30.6) | 8564 (31.0) | −0.004 | 3400 (48.1) | 17,136 (48.5) | −0.004 |
| Male | 3837 (69.4) | 19,086 (69.0) | 3663 (51.9) | 18,179 (51.5) | ||
| Number of physician visits per year during the follow-up (Mean, SD) | 9.9 (4.2) | 10.0 (4.1) | −0.030 | 9.9 (4.2) | 10.0 (4.1) | −0.033 |
| Obesity | 649 (11.7) | 3053 (11.0) | −0.007 | 1007 (14.3) | 4691 (13.3) | −0.010 |
| Diabetes mellitus | 1503 (27.2) | 7302 (26.4) | −0.008 | 2513 (35.6) | 12,241 (34.7) | −0.009 |
| Hypertension | 3124 (56.5) | 15,647 (56.6) | 0.001 | 4130 (58.5) | 20,663 (58.5) | 0.000 |
| Dyslipidemia | 1622 (29.3) | 8008 (29.0) | −0.004 | 2217 (31.4) | 11,185 (31.7) | 0.003 |
| Ischemic heart diseases | 719 (13.0) | 3484 (12.6) | −0.004 | 1230 (17.4) | 5819 (16.5) | −0.009 |
| COPD | 987 (17.9) | 4671 (16.9) | −0.010 | 1061 (15.0) | 5017 (14.2) | −0.008 |
| Variable | Proportion Among Patients with Alcoholic LC (N, %) N = 5530 | Proportion Among Patients Without LC (N, %) N = 27,650 | p Value | Proportion Among Patients with Non-Alcoholic LC (N, %) N = 7063 | Proportion Among Patients Without LC (N, %) N = 35,315 | p Value |
|---|---|---|---|---|---|---|
| Diuretics | 2293 (41.5) | 41,192 (15.2) | <0.001 | 2851 (40.4) | 7291 (20.7) | <0.001 |
| Betablockers | 2199 (39.8) | 8163 (29.5) | <0.001 | 2882 (40.8) | 12,170 (34.5) | <0.001 |
| Calcium-channel blockers | 764 (13.8) | 7873 (17.6) | <0.001 | 1303 (18.5) | 7479 (21.2) | <0.001 |
| ACE inhibitors | 1505 (27.2) | 8253 (29.9) | <0.001 | 1922 (27.2) | 11,200 (31.7) | <0.001 |
| Angiotensin II receptor blockers | 671 (12.1) | 5434 (19.7) | <0.001 | 1371 (19.3) | 7762 (22.0) | <0.001 |
| Lipid lowering drugs | 902 (16.3) | 6369 (23.0) | <0.001 | 1534 (21.7) | 9657 (27.4) | <0.001 |
| SGLT2 inhibitors | 86 (1.6) | 662 (2.4) | <0.001 | 244 (3.5) | 948 (2.7) | <0.001 |
| Alcoholic LC | Non-Alcoholic LC | |||
|---|---|---|---|---|
| Patient Subgroup | HR (95% CI) * | p Value | HR (95% CI) * | p Value |
| Total | 2.07 (1.85–2.31) | <0.001 | 1.70 (1.56–1.82) | <0.001 |
| Age < 60 | 3.54 (2.91–4.29) | <0.001 | 2.43 (1.97–3.01) | <0.001 |
| Age 60–69 | 2.13 (1.75–2.58) | <0.001 | 2.05 (1.75–2.40) | <0.001 |
| Age 70+ | 1.43 (1.18–1.72) | <0.001 | 1.54 (1.37–1.73) | <0.001 |
| Female | 1.63 (1.32–2.03) | <0.001 | 1.47 (1.29–1.67) | <0.001 |
| Male | 2.26 (1.99–2.57) | <0.001 | 1.91 (1.71–2.13) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostev, K.; Sedighi, J.; Sossalla, S.; Konrad, M.; Luedde, M. Both Alcoholic and Non-Alcoholic Liver Cirrhosis Are Associated with an Increased Risk of HF—A Cohort Study Including 75,558 Patients. J. Cardiovasc. Dev. Dis. 2025, 12, 295. https://doi.org/10.3390/jcdd12080295
Kostev K, Sedighi J, Sossalla S, Konrad M, Luedde M. Both Alcoholic and Non-Alcoholic Liver Cirrhosis Are Associated with an Increased Risk of HF—A Cohort Study Including 75,558 Patients. Journal of Cardiovascular Development and Disease. 2025; 12(8):295. https://doi.org/10.3390/jcdd12080295
Chicago/Turabian StyleKostev, Karel, Jamschid Sedighi, Samuel Sossalla, Marcel Konrad, and Mark Luedde. 2025. "Both Alcoholic and Non-Alcoholic Liver Cirrhosis Are Associated with an Increased Risk of HF—A Cohort Study Including 75,558 Patients" Journal of Cardiovascular Development and Disease 12, no. 8: 295. https://doi.org/10.3390/jcdd12080295
APA StyleKostev, K., Sedighi, J., Sossalla, S., Konrad, M., & Luedde, M. (2025). Both Alcoholic and Non-Alcoholic Liver Cirrhosis Are Associated with an Increased Risk of HF—A Cohort Study Including 75,558 Patients. Journal of Cardiovascular Development and Disease, 12(8), 295. https://doi.org/10.3390/jcdd12080295