
Unrecognized Pulmonary Hypertension in Non-Cardiac Surgical Patients: At-Risk Populations, Preoperative Evaluation, Intraoperative Management and Postoperative Complications


Abstract
:1. Introduction
2. Perioperative Impact
2.1. Perioperative Complications
2.2. Occult PH
2.3. Pathophysiology of Perioperative Right Ventricular Failure
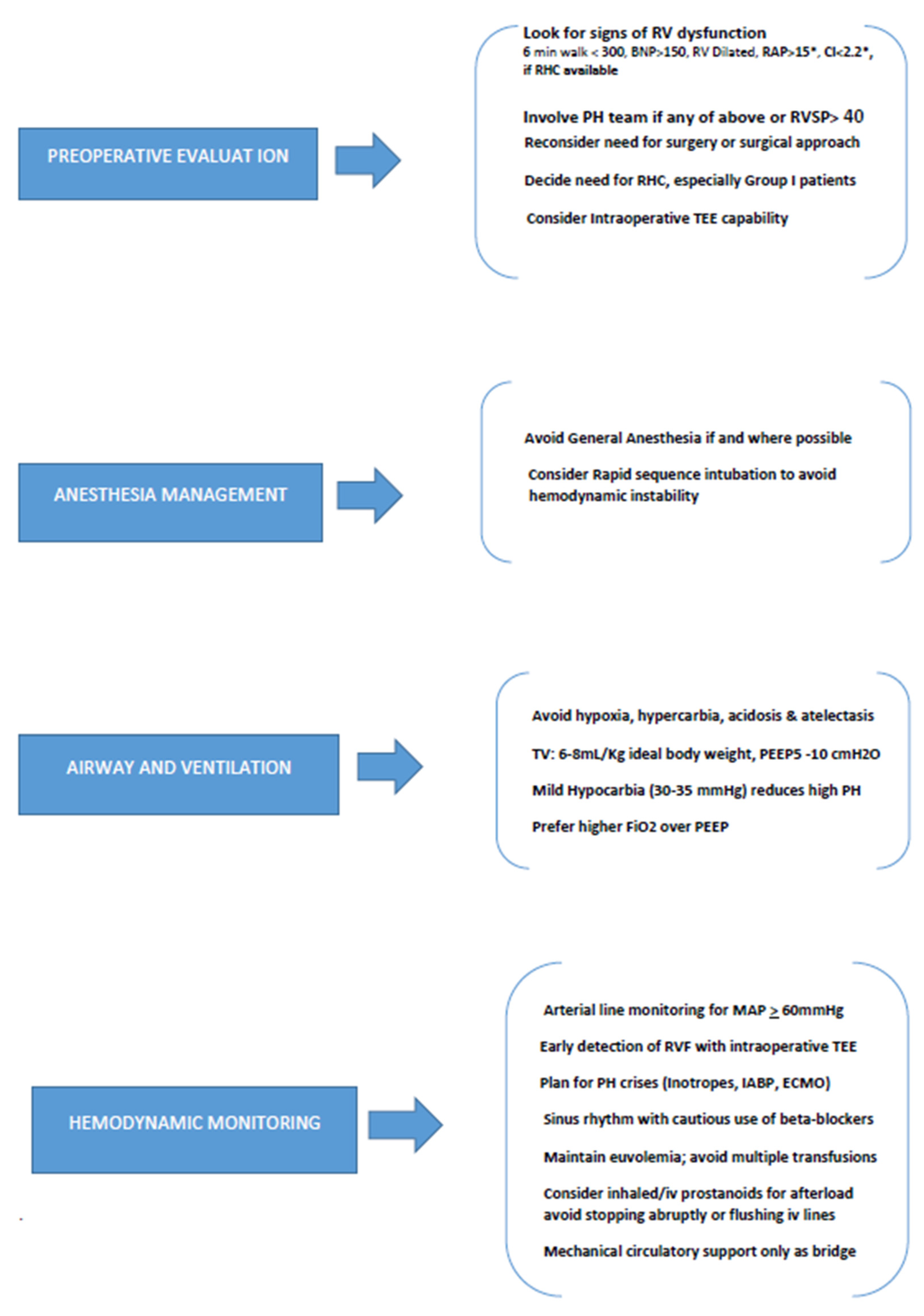
3. Preoperative Evaluation
3.1. Physical Examination
3.2. Preoperative Planning and Investigations
3.3. Preoperative Risk Stratification
4. Intraoperative Management
4.1. Anesthesia and Pulmonary Hypertension
4.2. Cardiopulmonary Monitoring
4.3. Airway Management
4.4. Medication Management
4.5. Pulmonary Hypertensive Crisis
4.6. Perioperative RV Dysfunction
5. Special Surgical Populations
5.1. Liver Transplantation
5.2. Thoracic Surgery
5.3. Orthopedic Surgery
6. Future Directions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wijeratne, D.T.; Lajkosz, K.; Brogly, S.B.; Loigheed, M.D.; Jiang, L.; Housin, A.; Barber, D.; Johnson, A.; Doliszny, K.M.; Archer, S.L. Increasing incidence and prevalence of World Health Organization groups1 to 4 pulmonary hypertension: A population-based study in Ontario, Canada. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e003973. [Google Scholar] [CrossRef]
- Smilovitz, N.R.; Armanious, A.; Bangalore, S.; Ramakrishna, H.; Berger, J.S. Cardiovascular outcomes of patients with pulmonary hypertension undergoing non-cardiac surgery. Am. J. Cardiol. 2019, 123, 1532–1537. [Google Scholar] [CrossRef]
- Ramakrishna, G.; Sprung, J.; Ravi, B.S.; Chandrasekaran, K.; McGoon, M.D. Impact of pulmonary hypertension on the outcomes of non-cardiac surgery. J. Am. Coll. Cardiol. 2005, 45, 1691–1696. [Google Scholar] [CrossRef]
- Kaw, R.; Pasupuleti, V.; Deshpande, A.; Hamieh, T.; Walker, E.; Minai, O.A. Pulmonary hypertension: An important predictor of outcomes in patients undergoing non-cardiac surgery. Respir. Med. 2011, 105, 619–624. [Google Scholar] [CrossRef]
- Minai, O.A.; Venkateshiah, S.B.; Arroliga, A.C. Surgical intervention in patients with moderate to severe pulmonary hypertension. Conn. Med. 2006, 70, 239–244. [Google Scholar]
- Lam, C.S.; Borlaug, B.A.; Kane, G.C.; Enders, F.T.; Rodeheffer, R.J.; Redfield, M.M. Age associated increases in pulmonary artery systolic pressure in the general population. Circulation 2009, 119, 2663–2670. [Google Scholar] [CrossRef]
- Stelfox, H.T.; Ahmed, S.B.; Ribeiro, R.A.; Gettings, E.M.; Pomerantsev, E.; Schmidt, U. Hemodynamic monitoring in obese patients: The impact of body mass index on cardiac output and stroke volume. Crit. Care Med. 2006, 34, 1243–1246. [Google Scholar] [CrossRef]
- Vonk Noordegraaf, A.; Chin, K.M.; Haddad, F.; Hassoun, P.M.; Hemnes, A.R.; Hopkins, S.R.; Kawut, S.M.; Langleben, D.; Lumens, J.; Naeije, R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur. Respir. J. 2019, 53, 1801900. [Google Scholar] [CrossRef]
- Szabo, G.; Soos, P.; Bahrle; Radovits, T.; Weigang, E.; Kékesi, V.; Merkely, B.; Hagl, S. Adaptation of the right ventricle to an increased afterload in the chronically volume overloaded heart. Ann. Thorac. Surg. 2006, 82, 989–995. [Google Scholar] [CrossRef]
- Braganza, M.; Shaw, J.; Solverson, K.; Vis, D.; Janovick, J.; Varughese, R.A.; Thakrar, M.V.; Hirani, N.; Helemersen, D.; Weatherald, J. A prospective evaluation of the diagnostic accuracy of the physical examination for Pulmonary hypertension. Chest 2019, 155, 982–990. [Google Scholar] [CrossRef]
- Aguirre, M.A.; Lynch, I.; Hardman, B. Perioperative management of pulmonary hypertension and right ventricular failure during non-cardiac surgery. Adv. Anesth. 2018, 36, 201–230. [Google Scholar] [CrossRef] [PubMed]
- Rajagopal, S.; Ruetzler, K.; Ghadimi, K.; Horn, E.M.; Kelava, M.; Kudelko, K.T.; Moreno-Duarte, I.; Preston, I.; Bovino, L.L.R.; Smilowitz, N.R.; et al. Evaluation and management of Pulmonary hypertension in Non-cardiac surgery: A Scientific Statement from the American Heart Association. Circulation 2023, 147, 1317–1343. [Google Scholar] [CrossRef] [PubMed]
- Minai, O.A.; Yared, J.P.; Kaw, R.; Subramaniam, K.; Hill, N.S. Perioperative risk and management in patients with Pulmonary hypertension. Chest 2013, 144, 329–340. [Google Scholar] [CrossRef]
- Price, L.C.; Wort, S.J.; Finney, S.J.; Marino, P.S.; Brett, S.J. Pulmonary vascular and right ventricular dysfunction in adult critical care: Current and emerging options for management: A systematic literature review. Crit. Care 2010, 14, R169. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, R.; Pritzker, M.; De Marco, T. Performance of the REVEAL pulmonary arterial hypertension prediction model using non-invasive and measured evaluated parameters. J. Heart Lung Transplant. 2014, 33, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Nowroozpoor, A.; Malekmohammad, M.; Seyyedi, S.R.; Hashemian, S.M. Pulmonary hypertension in intensive care units: An updated review. Tanaffos 2019, 18, 180–207. [Google Scholar]
- Meyer, S.; McLaughlin, V.V.; Seyfarth, H.J.; Bull, T.M.; Vizza, C.D.; Gomberg-Maitland, M.; Preston, I.R.; Barberà, J.A.; Hassoun, P.M.; Halank, M.; et al. Outcomes of non-cardiac, non-obstetric surgery in patients with PAH: An international prospective survey. Eur. Respir. J. 2013, 41, 1302–1307. [Google Scholar] [CrossRef]
- Davenport, D.L.; Ferraris, V.A.; Hosokawa, P.; Henderson, W.G.; Khuri, S.F.; Mentzer, R.M. Multivariate predictors of postoperative cardiac adverse events after general and vascular surgery: Results from the Patient Safety in Surgery Study. J. Am. Coll. Surg. 2007, 204, 1199–1210. [Google Scholar] [CrossRef]
- Harvey, D.; Levett, D.Z.H. Exercise testing for pre-operative evaluation. In Clinical Exercise Testing; Palane, P., Laveneziana, P., Neder, J.A., Eds.; European Respiratory Society: Sheffield, UK, 2018; pp. 251–279. [Google Scholar]
- Benza, R.L.; Miller, D.P.; Gomberg-Maitland, M.; Frantz, R.P.; Foreman, A.J.; Coffey, C.S.; Frost, A.; Barst, R.J.; Badesch, D.B.; Elliott, C.G.; et al. Predicting survival in pulmonary arterial hypertension: Insights from the registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 2010, 122, 164–172. [Google Scholar] [CrossRef]
- Augoustides, J.G.; Kulp, K.; Smith, S. Rebound pulmonary hypertension and cardiogenic shock after withdrawal of inhaled prostacyclin. Anesthesiology 2004, 100, 1023–1025. [Google Scholar] [CrossRef]
- Hassan, H.J.; Housten, T.; Balasubramanian, A.; Simpson, C.E.; Damico, R.L.; Mathai, S.C.; Hassoun, P.M.; Steppan, J.; Leary, P.J.; Kolb, T.M. A novel approach to perioperative risk assessment for patients with pulmonary hypertension. ERJ Open Res. 2021, 7, 00257–02021. [Google Scholar] [CrossRef]
- Albert, S.G.; Sitaula, S. Etomidate, adrenal insufficiency and mortality associated with severity of illness: A meta-analysis. J. Intensive Care Med. 2021, 36, 1124–1129. [Google Scholar] [CrossRef]
- Gopalratnam, K.; Odeyemi, Y.; del Valle, K.T.; Frank, R.D.; Jentzer, J.C.; Gajic, O.; DuBrock, H.M. Characteristics and Outcomes of Critically Ill patients with pulmonary hypertension who undergo endotracheal intubation and mechanical ventilation. J. Intensive Care Med. 2023. [Google Scholar] [CrossRef]
- Reich, D.L.; Hossain, S.; Krol, M.; Baez, B.; Patel, P.; Bernstein, A.; Bodian, C.A. Predictors of hypotension after induction of general anesthesia. Anesth. Analg. 2005, 101, 622–628. [Google Scholar] [CrossRef]
- Schulte-Sasse, U.; Hess, W.; Tarnow, J. Pulmonary vascular responses to nitrous oxide in patients with normal and high pulmonary vascular resistance. Anesthesiology 1982, 57, 9–13. [Google Scholar] [CrossRef]
- Wood, C.; Balciunas, M.; Lordan, J.; Mellor, A. Perioperative management of pulmonary hypertension, a review. J. Crit. Care Med. 2021, 7, 83–96. [Google Scholar] [CrossRef]
- Fayad, A.; Shillcutt, S.; Meineri, M.; Ruddy, T.D.; Ansari, M.T. Comparative effectiveness and harms of intraoperative transesophageal echocardiography in noncardiac surgery: A systematic review. Semin. Cardiothorac. Vasc. Anesth. 2018, 22, 122–136. [Google Scholar] [CrossRef] [PubMed]
- Tretter, J.T.; Redington, A.N. The forgotten ventricle? The left ventricle in right-sided congenital heart disease. Circ. Cardiovasc. Imaging 2018, 11, e007410. [Google Scholar] [CrossRef] [PubMed]
- Brovman, E.Y.; Gabriel, R.A.; Dutton, R.P.; Urman, R.D. Pulmonary artery catheter use during cardiac surgery in the United States, 2010 to 2014. J. Cardiothorac. Vasc. Anesth. 2016, 30, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Blaise, G.; Langleben, D.; Hubert, B. Pulmonary arterial hypertension: Pathophysiology and anesthetic approach. Anesthesiology 2003, 99, 1415–1432. [Google Scholar] [CrossRef]
- Pinsky, M.R. Cardiovascular issues in respiratory care. Chest 2002, 128, 592s–597s. [Google Scholar] [CrossRef] [PubMed]
- White, R.J.; Torres, F.; Allen, R.; Jerjes, C.; Pulido, T.; Yehle, D.; Howell, M.; Laliberte, K.; Marier, J.-F.; Tapson, V.F. Pharmacokinetics of oral treprostinil sustained release tablets during chronic administration to patients with pulmonary arterial hypertension. J. Cardiovasc. Phramacol. 2013, 61, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Hoeper, M.M.; Granton, J. Intensive care unit management of patients with severe pulmonary hypertension and right heart failure. Am. J. Crit. Care Med. 2011, 184, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Ventetuolo, C.E.; Klinger, J.R. Management of acute right ventricular failure in the intensive care unit. Ann. Am. Thorac. Soc. 2014, 11, 811–822. [Google Scholar] [CrossRef]
- Braun, E.B.; Palin, C.A.; Hogue, C.W. Vasopressin during spinal anesthesia in a patient with primary pulmonary hypertension treated with intravenous epoprostenol. Anesth. Analg. 2004, 99, 36–37. [Google Scholar] [CrossRef]
- Hill, N.S.; Roberts, K.R.; Preston, I.R. Postoperative pulmonary hypertension. Respir. Care. 2009, 54, 958–968. [Google Scholar] [CrossRef] [PubMed]
- Malay, M.B.; Ashton, J.L.; Dahl, K.; Savage, E.B.; Burchell, S.A.; Ashton, R.C., Jr.; Siacca, R.R.; Oliver, J.A.; Landry, D.W. Heterogeneity of the vasoconstrictor effect of oxytocin in septic shock. Crit. Care Med. 2004, 32, 1327–1331. [Google Scholar] [CrossRef]
- Kieler-Jensen, N.; Lundin, S.; Ricksten, S.E. Vasodilator therapy after heart transplantation: Effects of inhaled nitric oxide and intravenous prostacyclin, prostaglandin E1, and sodium nitroprusside. J. Heart Lung Transplant. 1995, 14, 436–443. [Google Scholar] [CrossRef]
- Hoeper, M.M.; Galie, N.; Murali, S.; Olschewski, H.; Rubenfire, M.; Robbins, I.M.; Farber, H.W.; Mclaughlin, V.; Shapiro, S.; Pepke-Zaba, J.; et al. Outcome after cardiopulmonary resuscitation in patients with pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2002, 165, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Sarabi, M.; Deschamps, A.; Delisle, S.; Ased, H.; Haddad, F.; Lamarche, Y.; Perrault, L.P.; Lambert, J.; Turgeon, A.F.; Denault, A.Y. Aerosolized vasodilators for the treatment of pulmonary hypertension in cardiac surgical patients: A systematic review and meta-analysis. Anesth. Analg. 2017, 125, 393–402. [Google Scholar] [CrossRef]
- Krowka, M.J.; Swanson, K.L.; Frantz, R.P.; McGoon, M.D.; Wiesner, R.H. Portopulmonary hypertension: Results from a 10-year screening algorithm. Hepatology 2006, 44, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- DuBrock, H.M.; Goldberg, D.S.; Sussman, N.L.; Bartolome, S.D.; Kadry, Z.; Salgia, R.J.; Mulligan, D.C.; Kremers, W.K.; Kawut, S.M.; Krowka, M.J.; et al. Predictors of wait-list mortality in portopulmonary hypertension. Transplantation 2017, 101, 1609–1615. [Google Scholar] [CrossRef] [PubMed]
- DuBrock, H.M.; Salgia, R.J.; Sussman, N.L.; Bartolome, S.D.; Kadry, Z.; Mulligan, D.C.; Jenkins, S.; Lackore, K.; Channick, R.N.; Kawut, S.M.; et al. Portopulmonary hypertension: A survey of practice patterns and provider attitudes. Transplant. Direct 2019, 5, e456. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.F.; Ueda, K. Pulmonary hypertension in thoracic surgical patients. Curr. Opin. Anaesthesiol. 2010, 23, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Heerdt, P.M.; Stowe, D.F. Single-lung ventilation and oxidative stress: A different perspective on a common practice. Curr. Opin. Anaesthesiol. 2017, 30, 42–49. [Google Scholar] [CrossRef]
- Memtsoudis, S.G.; Ma, Y.; Chiu, Y.L.; Walz, J.M.; Voswinckel, R.; Mazumdar, M. Perioperative mortality in patients with pulmonary hypertension undergoing major joint replacement. Anesth. Analg. 2010, 111, 1110–1116. [Google Scholar] [CrossRef]
- McGlothlin, D.P.; Granton, J.; Klepetko, W.; Beghetti, M.; Rosenzweig, E.B.; Corris, P.A.; Horn, E.; Kanwar, M.K.; McRae, K.; Roman, A.; et al. ISHLT consensus statement: Perioperative management of patients with pulmonary hypertension undergoing surgery. J. Heart Lung Transplant. 2022, 41, 1135–1194. [Google Scholar] [CrossRef]

{kind=link}
| 1. | Patients with hemodynamic signs of RV failure (CVP > 15; low CO), hypoxia, or dyspnea at rest should not be taken for surgery. |
| 2. | Patients with moderately severe PH should not undergo liver transplantation (for POPH) or joint replacement surgery. |
| 3. | Avoid GA if and wherever possible. |
| 4. | Avoid intubation if possible, especially in group 1 PH, by using PAP, inhaled pulmonary vasodilators and or, high-flow nasal cannula. |
| 5. | Avoid volume overloading and hypotension. |
| 6. | Do not flush the lines infusing pulmonary vasodilators. |
| 7. | Do not abruptly stop pulmonary vasodilators. |
| 8. | Mechanical circulatory support should only be used as a bridge therapy or where recovery is expected. |
| 1. | Is the surgery necessary or alternative procedure/approach plausible? |
| 2. | Can the patient be moved to a center of excellence in PH care? |
| 3. | Decide the need for RHC before surgery, especially in patients with group 1 PH. |
| 4. | Is the anesthesia plan modifiable? |
| 5. | Neuraxial anesthesia should be utilized slowly or in combination with epidural anesthesia with arterial line monitoring. |
| 6. | Decide about perioperative cardiopulmonary monitoring. Is intraoperative TEE with expertise in procedure available? |
| 7. | Plan for perioperative pulmonary hypertensive crisis (e.g., Inotropes, IABP, ECMO) and discuss high-risk cases with transplant teams before going for Non-Cardiac Surgery. |
| 8. | Use lower tidal volumes (6–8 mL/Kg of ideal body weight) and PEEP (5–10 cm H2O). |
| 9. | Use PAP and supplemental oxygen wherever necessary. |
| 10. | Maintain normal sinus rhythm during the intraoperative period; avoid beta-blockers and calcium channel blockers if RV failure is suspected. |
| 11. | Maintain euvolemia and hemodynamics; avoid multiple blood products at the same time. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaw, R.K. Unrecognized Pulmonary Hypertension in Non-Cardiac Surgical Patients: At-Risk Populations, Preoperative Evaluation, Intraoperative Management and Postoperative Complications. J. Cardiovasc. Dev. Dis. 2023, 10, 403. https://doi.org/10.3390/jcdd10090403
Kaw RK. Unrecognized Pulmonary Hypertension in Non-Cardiac Surgical Patients: At-Risk Populations, Preoperative Evaluation, Intraoperative Management and Postoperative Complications. Journal of Cardiovascular Development and Disease. 2023; 10(9):403. https://doi.org/10.3390/jcdd10090403
Chicago/Turabian StyleKaw, Roop K. 2023. "Unrecognized Pulmonary Hypertension in Non-Cardiac Surgical Patients: At-Risk Populations, Preoperative Evaluation, Intraoperative Management and Postoperative Complications" Journal of Cardiovascular Development and Disease 10, no. 9: 403. https://doi.org/10.3390/jcdd10090403
APA StyleKaw, R. K. (2023). Unrecognized Pulmonary Hypertension in Non-Cardiac Surgical Patients: At-Risk Populations, Preoperative Evaluation, Intraoperative Management and Postoperative Complications. Journal of Cardiovascular Development and Disease, 10(9), 403. https://doi.org/10.3390/jcdd10090403