


Reference Values for Inward Displacement in the Normal Left Ventricle: A Novel Method of Regional Left Ventricular Function Assessment
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. CMR Image Acquisition
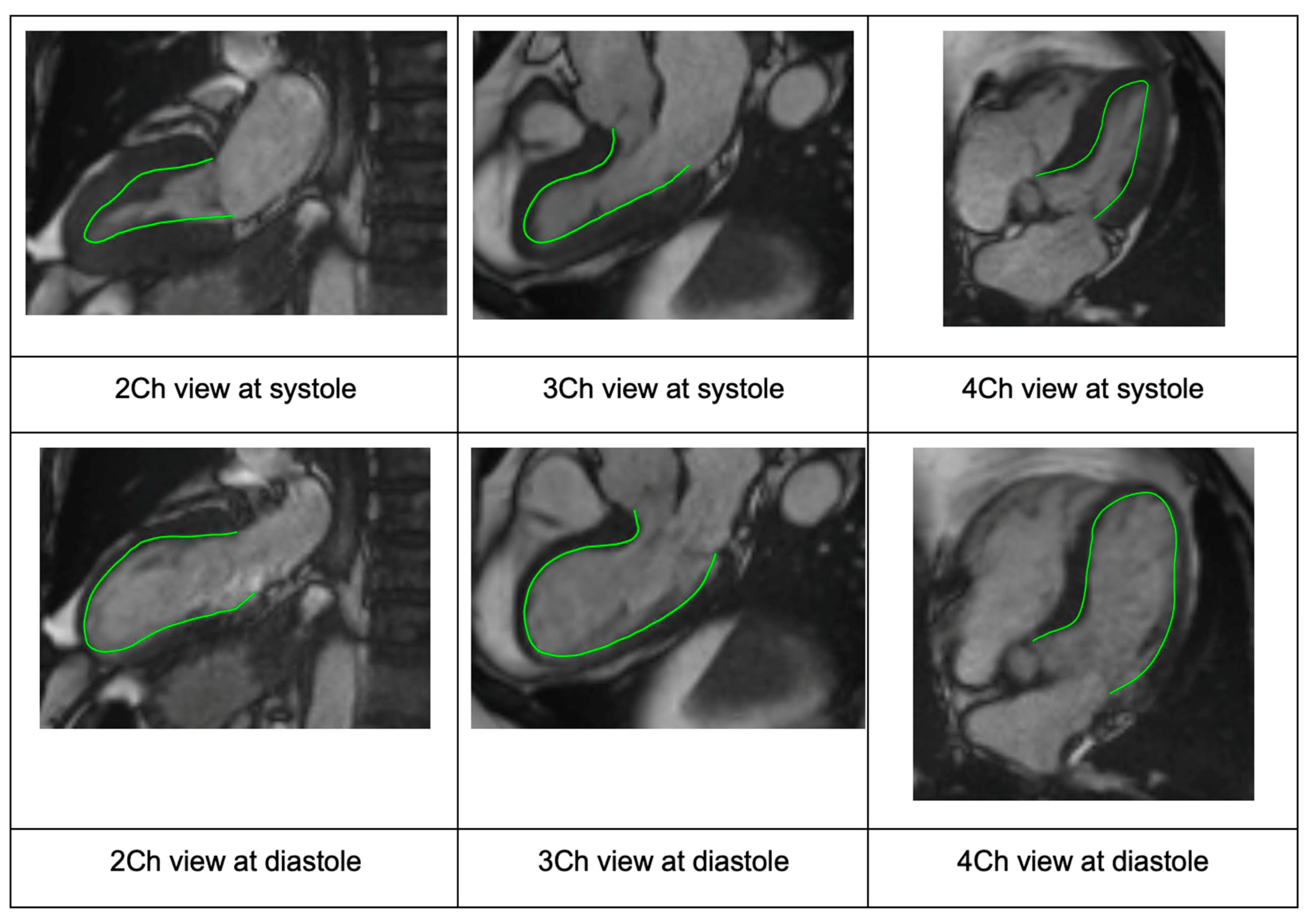
2.3. CMR Analysis
2.4. Inward Displacement
2.5. Statistical Analysis
3. Results
3.1. Subject Selection
3.2. Baseline Characteristics
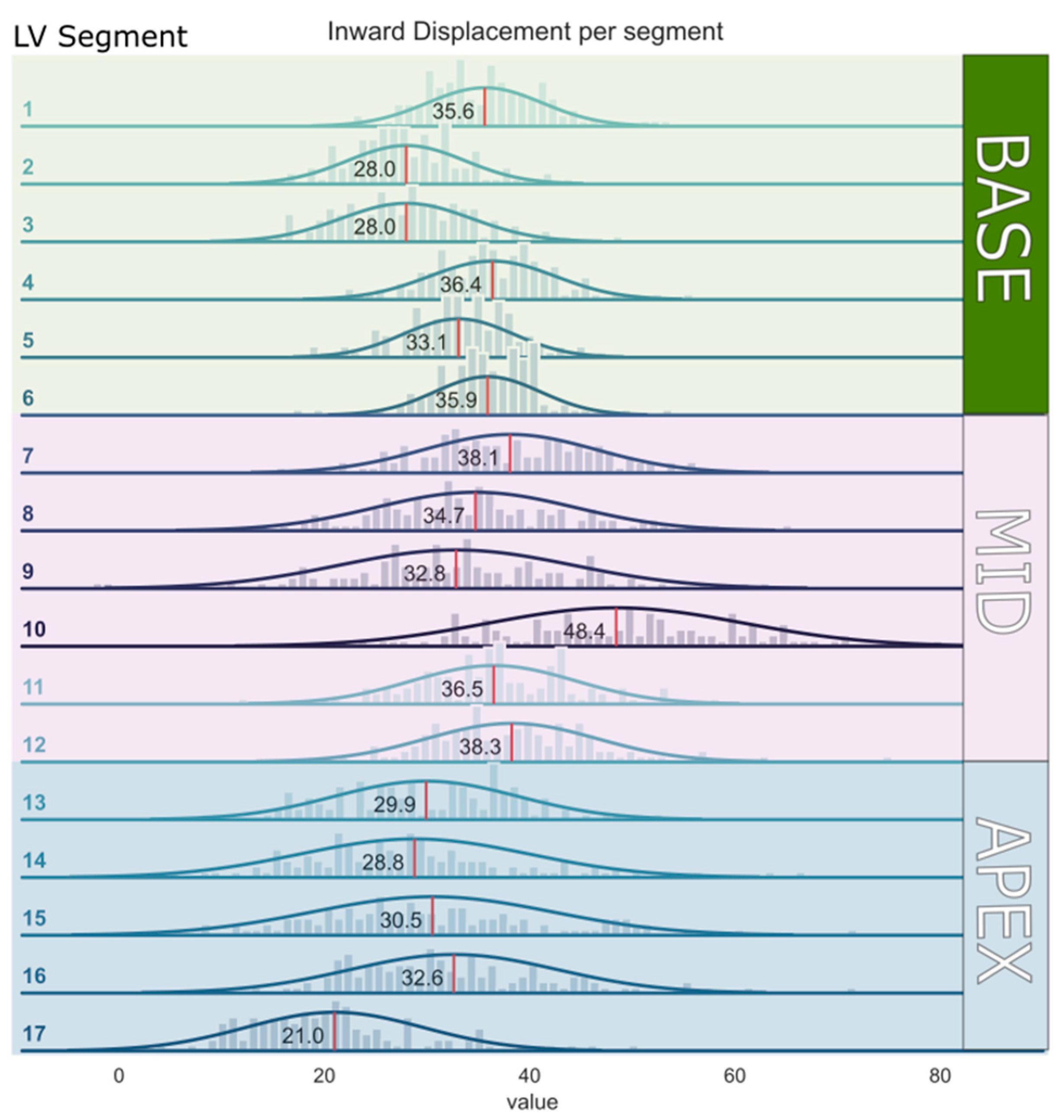
3.3. Segmental InD Values
3.4. Relationship between LV Volumes and InD
3.5. Interobserver Variability
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smistad, E.; Østvik, A.; Salte, I.M.; Melichova, D.; Nguyen, T.M.; Haugaa, K.; Brunvand, H.; Edvardsen, T.; Leclerc, S.; Bernard, O.; et al. Real-Time Automatic Ejection Fraction and Foreshortening Detection Using Deep Learning. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2020, 67, 2595–2604. [Google Scholar] [CrossRef] [PubMed]
- Verdonschot, J.A.J.; Henkens, M.T.H.M.; Wang, P.; Schummers, G.; Raafs, A.G.; Krapels, I.P.C.; van Empel, V.; Heymans, S.R.B.; Brunner-La Rocca, H.P.; Knackstedt, C. A Global Longitudinal Strain Cut-off Value to Predict Adverse Outcomes in Individuals with a Normal Ejection Fraction. ESC Heart Fail 2021, 8, 4343–4345. [Google Scholar] [CrossRef] [PubMed]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Ajmone Marsan, N. Global and Regional Longitudinal Strain Assessment in Hypertrophic Cardiomyopathy: Standardization Is yet to Come. Circ. Cardiovasc. Imaging 2019, 12, e009586. [Google Scholar] [CrossRef] [PubMed]
- Raafs, A.G.; Boscutti, A.; Henkens, M.T.H.M.; van den Broek, W.W.A.; Verdonschot, J.A.J.; Weerts, J.; Stolfo, D.; Nuzzi, V.; Manca, P.; Hazebroek, M.R.; et al. Global Longitudinal Strain Is Incremental to Left Ventricular Ejection Fraction for the Prediction of Outcome in Optimally Treated Dilated Cardiomyopathy Patients. J. Am. Heart Assoc. 2022, 11, e024505. [Google Scholar] [CrossRef] [PubMed]
- Sengeløv, M.; Jørgensen, P.G.; Jensen, J.S.; Bruun, N.E.; Olsen, F.J.; Fritz-Hansen, T.; Nochioka, K.; Biering-Sørensen, T. Global Longitudinal Strain Is a Superior Predictor of All-Cause Mortality in Heart Failure with Reduced Ejection Fraction. JACC Cardiovasc. Imaging 2015, 8, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Spilias, N.; Howard, T.M.; Anthony, C.M.; Laczay, B.; Soltesz, E.G.; Starling, R.C.; Sievert, H.; Estep, J.D.; Kapadia, S.R.; Puri, R. Transcatheter Left Ventriculoplasty. EuroIntervention 2023, 18, 1399–1407. [Google Scholar] [CrossRef] [PubMed]
- Tsugu, T.; Postolache, A.; Dulgheru, R.; Sugimoto, T.; Tridetti, J.; Trung, M.L.N.; Piette, C.; Moonen, M.; Manganaro, R.; Ilardi, F.; et al. Echocardiographic Reference Ranges for Normal Left Ventricular Layer-Specific Strain: Results from the EACVI NORRE Study. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Marwick, T.H.; Leano, R.L.; Brown, J.; Sun, J.P.; Hoffmann, R.; Lysyansky, P.; Becker, M.; Thomas, J.D. Myocardial Strain Measurement With 2-Dimensional Speckle-Tracking Echocardiography. Definition of Normal Range. JACC Cardiovasc. Imaging 2009, 2, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Mirea, O.; Pagourelias, E.D.; Duchenne, J.; Bogaert, J.; Thomas, J.D.; Badano, L.P.; Voigt, J.U.; Hamilton, J.; Pedri, S.; Lysyansky, P.; et al. Variability and Reproducibility of Segmental Longitudinal Strain Measurement: A Report From the EACVI-ASE Strain Standardization Task Force. JACC Cardiovasc. Imaging 2018, 11, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Nabeta, T.; Meucci, M.C.; Westenberg, J.J.M.; Reiber, J.H.; Knuuti, J.; van der Bijl, P.; Marsan, N.A.; Bax, J.J. Prognostic Implications of Left Ventricular Inward Displacement Assessed by Cardiac Magnetic Resonance Imaging in Patients with Myocardial Infarction. Int. J. Cardiovasc. Imaging 2023, 39, 1525–1533. [Google Scholar] [CrossRef] [PubMed]
- de la Pena-Almaguer, E.; Hautemann, D.; Pedrizzetti, G. Computed Tomography Derived Left Ventricular Inward Displacement as a Novel Tool for Quantification of Segmental Wall Motion Abnormalities. Int. J. Cardiovasc. Imaging 2021, 37, 3589–3590. [Google Scholar] [CrossRef] [PubMed]
- Hegeman, R.R.M.J.J.; McManus, S.; van Kuijk, J.-P.; Harb, S.C.; Swaans, M.J.; Klein, P.; Puri, R. Inward Displacement: A Novel Method of Regional Left Ventricular Functional Assessment for Left Ventriculoplasty Interventions in Heart Failure with Reduced Ejection Fraction (HFrEF). J. Clin. Med. 2023, 12, 1997. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S. Standardized Myocardial Segmentation and Nomenclature for Tomographic Imaging of the Heart. Circulation 2002, 105, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Castelvecchio, S.; Frigelli, M.; Sturla, F.; Milani, V.; Pappalardo, O.A.; Citarella, M.; Menicanti, L.; Votta, E. Elucidating the Mechanisms Underlying Left Ventricular Function Recovery in Patients with Ischemic Heart Failure Undergoing Surgical Remodeling: A 3-Dimensional Ultrasound Analysis. J. Thorac. Cardiovasc. Surg. 2021, 165, 1418–1429.e4. [Google Scholar] [CrossRef] [PubMed]
- Asgeirsson, D.; Hedström, E.; Jögi, J.; Pahlm, U.; Steding-Ehrenborg, K.; Engblom, H.; Arheden, H.; Carlsson, M. Longitudinal Shortening Remains the Principal Component of Left Ventricular Pumping in Patients with Chronic Myocardial Infarction Even When the Absolute Atrioventricular Plane Displacement Is Decreased. BMC Cardiovasc. Disord. 2017, 17, 208. [Google Scholar] [CrossRef] [PubMed]
- Pahlm, U.; Seemann, F.; Engblom, H.; Gyllenhammar, T.; Halvorsen, S.; Hansen, H.S.; Erlinge, D.; Atar, D.; Heiberg, E.; Arheden, H.; et al. Longitudinal Left Ventricular Function Is Globally Depressed within a Week of STEMI. Clin. Physiol. Funct. Imaging 2018, 38, 1029–1037. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 120) |
|---|---|
| Age (y) | 50.7 ± 16.9 |
| Male (%) | 50% |
| Patient weight (kg) | 72.0 ± 13.3 |
| Patient height (cm) | 172.2 ± 9.1 |
| BSA (m2) | 1.8 ± 0.2 |
| EDV * (mL) | 146.1 ± 33.0 |
| ESV * (mL) | 48.9 ± 15.7 |
| EF * (%) | 66.8 ± 5.4 |
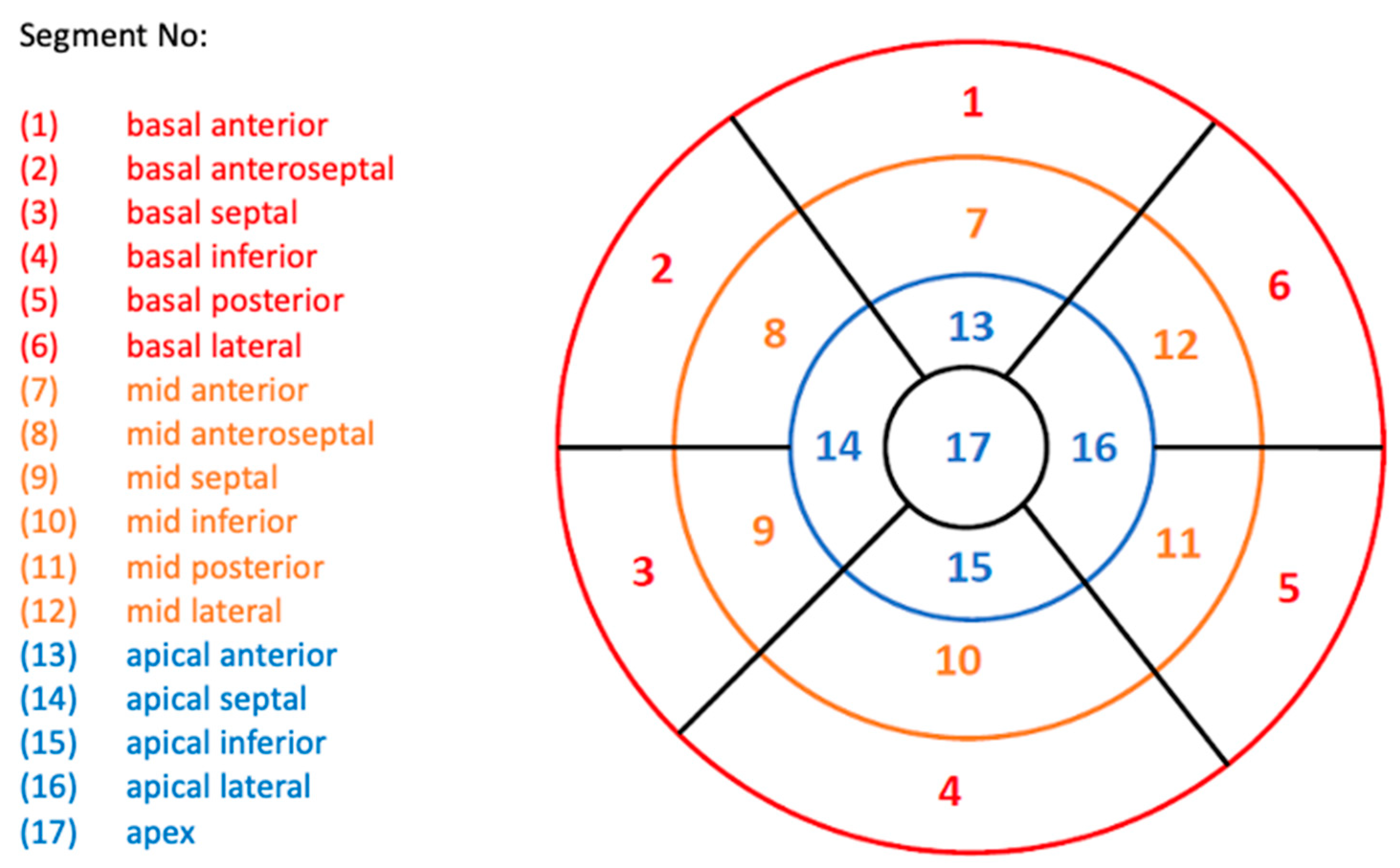
| Segment | Region | Mean (%) | SD (%) |
|---|---|---|---|
| Segment 1 | Basal anterior | 35.6 | 5.6 |
| Segment 2 | Basal anteroseptal | 28.0 | 5.7 |
| Segment 3 | Basal inferoseptal | 28.0 | 6.4 |
| Segment 4 | Basal inferior | 36.4 | 6.1 |
| Segment 5 | Basal inferolateral | 33.1 | 5.3 |
| Segment 6 | Basal anterolateral | 35.9 | 5.1 |
| Segment 7 | Mid-anterior | 38.1 | 8.4 |
| Segment 8 | Mid-anteroseptal | 34.7 | 9.7 |
| Segment 9 | Mid-inferoseptal | 32.8 | 11.4 |
| Segment 10 | Mid-inferior | 48.4 | 12.4 |
| Segment 11 | Mid-inferolateral | 36.5 | 7.9 |
| Segment 12 | Mid-anterolateral | 38.3 | 8.3 |
| Segment 13 | Apical anterior | 29.9 | 8.9 |
| Segment 14 | Apical septal | 28.8 | 11.2 |
| Segment 15 | Apical inferior | 30.5 | 11.7 |
| Segment 16 | Apical lateral | 32.6 | 10.1 |
| Segment 17 | Apex | 21.0 | 8.6 |
| Average | All segments | 33.4 | 4.3 |
| Region | Mean (%) | SD (%) |
|---|---|---|
| Base | 32.8 | 4.1 |
| Mid | 38.1 | 5.8 |
| Apex | 28.6 | 7.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hegeman, R.R.M.J.J.; McManus, S.; Tóth, A.; Ladeiras-Lopes, R.; Kitslaar, P.; Bui, V.; Dukker, K.; Harb, S.C.; Swaans, M.J.; Ben-Yehuda, O.; et al. Reference Values for Inward Displacement in the Normal Left Ventricle: A Novel Method of Regional Left Ventricular Function Assessment. J. Cardiovasc. Dev. Dis. 2023, 10, 474. https://doi.org/10.3390/jcdd10120474
Hegeman RRMJJ, McManus S, Tóth A, Ladeiras-Lopes R, Kitslaar P, Bui V, Dukker K, Harb SC, Swaans MJ, Ben-Yehuda O, et al. Reference Values for Inward Displacement in the Normal Left Ventricle: A Novel Method of Regional Left Ventricular Function Assessment. Journal of Cardiovascular Development and Disease. 2023; 10(12):474. https://doi.org/10.3390/jcdd10120474
Chicago/Turabian StyleHegeman, Romy R. M. J. J., Sean McManus, Attila Tóth, Ricardo Ladeiras-Lopes, Pieter Kitslaar, Viet Bui, Kayleigh Dukker, Serge C. Harb, Martin J. Swaans, Ori Ben-Yehuda, and et al. 2023. "Reference Values for Inward Displacement in the Normal Left Ventricle: A Novel Method of Regional Left Ventricular Function Assessment" Journal of Cardiovascular Development and Disease 10, no. 12: 474. https://doi.org/10.3390/jcdd10120474
APA StyleHegeman, R. R. M. J. J., McManus, S., Tóth, A., Ladeiras-Lopes, R., Kitslaar, P., Bui, V., Dukker, K., Harb, S. C., Swaans, M. J., Ben-Yehuda, O., Klein, P., & Puri, R. (2023). Reference Values for Inward Displacement in the Normal Left Ventricle: A Novel Method of Regional Left Ventricular Function Assessment. Journal of Cardiovascular Development and Disease, 10(12), 474. https://doi.org/10.3390/jcdd10120474