
Impact of Persistent Iatrogenic Atrial Septal Defect following MitraClip
 , ,
, ,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Alachkar, M.N.; Alnaimi, A.; Reith, S.; Altiok, E.; Schröder, J.; Marx, N.; Almalla, M. Incidence and clinical relevance of persistent iatrogenic atrial septal defect after percutaneous mitral valve repair. Sci. Rep. 2021, 11, 12700. [Google Scholar] [CrossRef] [PubMed]
- Schueler, R.; Öztürk, C.; Wedekind, J.A.; Werner, N.; Stöckigt, F.; Mellert, F.; Nickenig, G.; Hammerstingl, C. Persistence of iatrogenic atrial septal defect after interventional mitral valve repair with the MitraClip system: A note of caution. JACC Cardiovasc. Interv. 2015, 8, 450–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, T.; McGinty, P.; Bommer, W.; Low, R.I.; Lim, S.; Fail, P.; Rogers, J.H. Prevalence and echocardiographic features of iatrogenic atrial septal defect after catheter-based mitral valve repair with the MitraClip system. Catheter. Cardiovasc. Interv. 2012, 80, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Toyama, K.; Rader, F.; Kar, S.; Kubo, S.; Shiota, T.; Nishioka, T.; Siegel, R.J. Iatrogenic Atrial Septal Defect After Percutaneous Mitral Valve Repair with the MitraClip System. Am. J. Cardiol. 2018, 121, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.; Altiok, E.; Reith, S.; Brehmer, K.; Almalla, M. Functional effect of new atrial septal defect after percutaneous mitral valve repair using the MitraClip device. Am. J. Cardiol. 2014, 113, 1228–1233. [Google Scholar] [CrossRef] [PubMed]
- Lurz, P.; Unterhuber, M.; Rommel, K.-P.; Kresoja, K.-P.; Kister, T.; Besler, C.; Fengler, K.; Sandri, M.; Daehnert, I.; Thiele, H.; et al. Closure of Iatrogenic Atrial Septal Defect after Transcatheter Mitral Valve Repair: The Randomized MITHRAS Trial. Circulation 2021, 143, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Lurz, P.; Unterhuber, M.; Rommel, K.-P.; Kresoja, K.-P.; Kister, T.; Besler, C.; Fengler, K.; Sandri, M.; Daehnert, I.; Thiele, H.; et al. Iatrogenic Atrial Septal Defects Following Transcatheter Mitral Valve Repair and Implications of Interventional Closure. JACC Cardiovasc. Interv. 2021, 14, 2685–2694. [Google Scholar] [CrossRef] [PubMed]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Babaliaros, V.C.; Green, J.T.; Lerakis, S.; Lloyd, M.; Block, P.C. Emerging applications for transseptal left heart catheterization: Old techniques for new procedures. J. Am. Coll. Cardiol. 2008, 51, 2116–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blazek, S.; Unterhuber, M.; Rommel, K.-P.; von Roeder, M.; Kresoja, K.-P.; Kister, T.; Besler, C.; Fengler, K.; Sandri, M.; Daehnert, I.; et al. Biventricular physiology of iatrogenic atrial septal defects following transcatheter mitral valve edge-to-edge repair. Cardiovasc. Interv. 2021, 14, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Mauri, L.; Kahwash, R.; Litwin, S.; Ricciardi, M.J.; Van Der Harst, P.; Penicka, M.; Fail, P.S.; Kaye, D.M.; Petrie, M.C.; et al. Transcatheter Interatrial Shunt Device for the Treatment of Heart Failure with Preserved Ejection Fraction (REDUCE LAP-HF I [Reduce Elevated Left Atrial Pressure in Patients With Heart Failure]): A Phase 2, Randomized, Sham-Controlled Trial. Circulation 2018, 137, 364–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz, J.; Sánchez-Quintana, D.; Bossone, E.; Bogaard, H.J.; Naeije, R. Anatomy, Function, and Dysfunction of the Right Ventricle. J. Am. Coll. Cardiol. 2019, 73, 1463–1482. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, T.; Miyasaka, M.; Flint, N.; Manabe, O.; Dawkins, S.; Cheng, R.; Hussaini, A.; Makar, M.; Kar, S.; Nakamura, M. Right-to-left shunt through iatrogenic atrial septal defect after MitraClip procedure. Cardiovasc. Interv. 2020, 13, 1544–1553. [Google Scholar] [CrossRef] [PubMed]
- Silvestry, F.E.; Cohen, M.S.; Armsby, L.B.; Burkule, N.J.; Fleishman, C.E.; Hijazi, Z.M.; Lang, R.M.; Rome, J.J.; Wang, Y.; American Society of Echocardiography; et al. Guidelines for the Echocardiographic Assessment of Atrial Septal Defect and Patent Foramen Ovale: From the American Society of Echocardiography and Society for Cardiac Angiography and Interventions. J. Am. Soc. Echocardiogr. 2015, 28, 910–958. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Iatrogenic ASD Present (n = 108) | Iatrogenic ASD Not Present (n = 208) | Total (n = 316) | p Value | |
|---|---|---|---|---|
| Age, years | 77.9 ± 9.9 | 79.7 ± 8.5 | 79.1 ± 9.1 | 0.101 |
| Sex, n (%) | 0.972 | |||
| Female | 35 (32.4%) | 67 (32.2%) | 102 (32.3%) | |
| Male | 73 (67.6%) | 141 (67.8%) | 214 (67.7%) | |
| Height, cm | 169.9 ± 10.7 | 168.6 ± 9.9 | 169.0 ± 10.2 | 0.245 |
| Weight, Kg | 77.6 ± 19.5 | 78.7 ± 19.1 | 78.4 ± 19.2 | 0.613 |
| Body Mass Index, Kg/m2 | 26.6 ± 5.1 | 27.5 ± 5.4 | 27.2 ± 5.3 | 0.136 |
| Smoking, n (%) | 4 (3.7%) | 4 (1.9%) | 8 (2.5%) | 0.339 |
| Hypertension, n (%) | 94 (87.0%) | 182 (87.5%) | 276 (87.3%) | 0.907 |
| Diabetes, n (%) | 26 (24.1%) | 51 (24.6%) | 77 (24.4%) | 0.912 |
| Prior Myocardial infarction, n (%) | 33 (30.6%) | 58 (27.9%) | 91 (28.9%) | 0.583 |
| Prior PCI, n (%) | 25 (23.1%) | 61 (29.3%) | 86 (27.2%) | 0.242 |
| Prior CABG, n (%) | 35 (32.4%) | 62 (29.8%) | 97 (30.7%) | 0.635 |
| STS Risk (for isolated mitral valve repair) | 7.5 ± 5.2 | 7.6 ± 5.7 | 7.5 ± 5.5 | 0.939 |
| Pacemaker, n (%) | 14 (13.0%) | 34 (16.3%) | 48 (15.2%) | 0.427 |
| Prior Stroke, n (%) | 12 (11.1%) | 23 (11.1%) | 35 (11.1%) | 0.989 |
| Prior Peripheral artery disease, n (%) | 32 (29.6%) | 53 (25.5%) | 85 (26.9%) | 0.430 |
| End stage kidney disease, n (%) | 3 (2.8%) | 7 (3.4%) | 10 (3.2%) | 0.777 |
| Atrial Fibrillation, n (%) | 77 (71.3%) | 134 (64.4%) | 211 (66.8%) | 0.219 |
| Six-minute walk distance, m | 326.4 ± 110.9 | 299.9 ± 107.6 | 308.1 ± 109.1 | 0.101 |
| NYHA FC, n (%) | 0.923 | |||
| Class I | 1 (0.9%) | 4 (1.9%) | 5 (1.6%) | |
| Class II | 22 (20.4%) | 39 (18.8%) | 61 (19.3%) | |
| Class III | 67 (62.0%) | 128 (61.5%) | 195 (61.7%) | |
| Class IV | 18 (16.7%) | 37 (17.8%) | 55 (17.4%) | |
| NTproBNP, pg/ml | 2198.0 (4958.0) | 1958.0 (3409.0) | 2020.0 (4147.5) | 0.162 |
| Degenerative Mitral valve disease, n (%) | 92 (85.2%) | 177 (85.1%) | 269 (85.1%) | 0.983 |
| Iatrogenic ASD Present (n = 108) | Iatrogenic ASD Not Present (n = 208) | p Value | |
|---|---|---|---|
| Six-Minute Walk Test, m | 322.2 ± 131.9 | 305.0 ± 121.1 | 0.397 |
| NYHA FC, n (%) | 0.276 | ||
| Class I | 30 (40.0%) | 60 (39.0%) | |
| Class II | 31 (41.3%) | 50 (32.5%) | |
| Class III | 12 (16.0%) | 36 (23.4%) | |
| Class IV | 2 (2.7%) | 8 (5.2%) | |
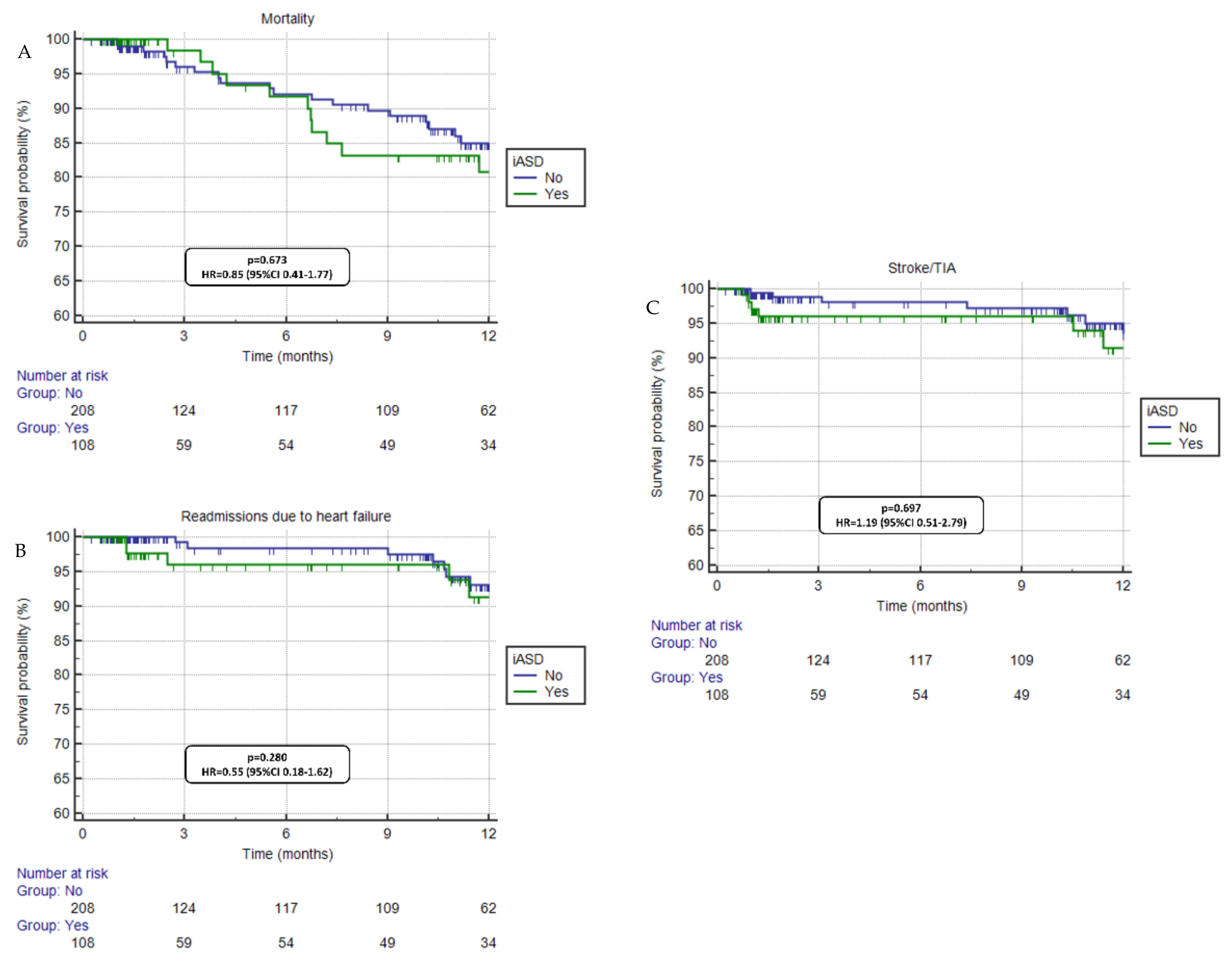
| Readmission due to Heart Failure, n (%) | 7 (6.5%) | 8 (3.9%) | 0.280 |
| Stroke/TIA | 7 (6.5%) | 17 (8.2%) | 0.697 |
| Mortality, n (%) | 12 (11.1%) | 21 (10.1%) | 0.673 |
| Iatrogenic ASD Present | Iatrogenic ASD Not Present | p-Value | |
|---|---|---|---|
| MV mean gradient (mmHg) | 4.6 ± 2.2 | 4.3 ± 2.1 | 0.289 |
| LVEF (%) | 51.1 ± 14.0 | 51.3 ± 13.9 | 0.933 |
| LVEDV (mL) | 149.4 ± 69.6 | 142.3 ± 69.5 | 0.482 |
| LVESV (mL) | 82.7 ± 56.1 | 76.0 ± 56.1 | 0.410 |
| RVEDA (cm2) | 25.3 ± 6.9 | 29.9 ± 9.2 | 0.073 |
| RVSP (mmHg) | 48.7 ± 14.4 | 45.5 ± 14.5 | 0.042 |
| TAPSE (mm) | 15.2 ± 4.6 | 15.4 ± 5.5 | 0.875 |
| Mitral valve regurgitation (%) | 0.779 | ||
| Trivial | 7.1 | 4.6 | |
| Mild | 44.4 | 41.8 | |
| Moderate | 37.4 | 48.5 | |
| Severe | 11.1 | 5.2 | |
| Tricuspid valve regurgitation (%) | 0.215 | ||
| Trivial | 15.6 | 15.7 | |
| Mild | 40.6 | 47.6 | |
| Moderate | 26.0 | 25.7 | |
| Severe | 17.7 | 11.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chao, C.-J.; Seri, A.; Abraham, B.; Farina, J.M.; Fennelly, E.; Campany, M.; Pereyra, M.; Said, E.F.; Kenyon, C.; Fath, A.R.; et al. Impact of Persistent Iatrogenic Atrial Septal Defect following MitraClip. J. Cardiovasc. Dev. Dis. 2023, 10, 1. https://doi.org/10.3390/jcdd10010001
Chao C-J, Seri A, Abraham B, Farina JM, Fennelly E, Campany M, Pereyra M, Said EF, Kenyon C, Fath AR, et al. Impact of Persistent Iatrogenic Atrial Septal Defect following MitraClip. Journal of Cardiovascular Development and Disease. 2023; 10(1):1. https://doi.org/10.3390/jcdd10010001
Chicago/Turabian StyleChao, Chieh-Ju, Amith Seri, Bishoy Abraham, Juan M. Farina, Evelyn Fennelly, Megan Campany, Milagros Pereyra, Ebram F. Said, Courtney Kenyon, Ayman R. Fath, and et al. 2023. "Impact of Persistent Iatrogenic Atrial Septal Defect following MitraClip" Journal of Cardiovascular Development and Disease 10, no. 1: 1. https://doi.org/10.3390/jcdd10010001
APA StyleChao, C.-J., Seri, A., Abraham, B., Farina, J. M., Fennelly, E., Campany, M., Pereyra, M., Said, E. F., Kenyon, C., Fath, A. R., Smith, S., Buckner-Petty, S., Rayfield, C. A., Fortuin, D., Sweeney, J. P., Yang, E. H., Ayoub, C., Eleid, M. F., Alkhouli, M., ... Arsanjani, R. (2023). Impact of Persistent Iatrogenic Atrial Septal Defect following MitraClip. Journal of Cardiovascular Development and Disease, 10(1), 1. https://doi.org/10.3390/jcdd10010001