
The Positive Effects of Physical Activity on Quality of Life in Parkinson’s Disease: A Systematic Review
 ,
,
Abstract
1. Introduction
2. Materials and Methods
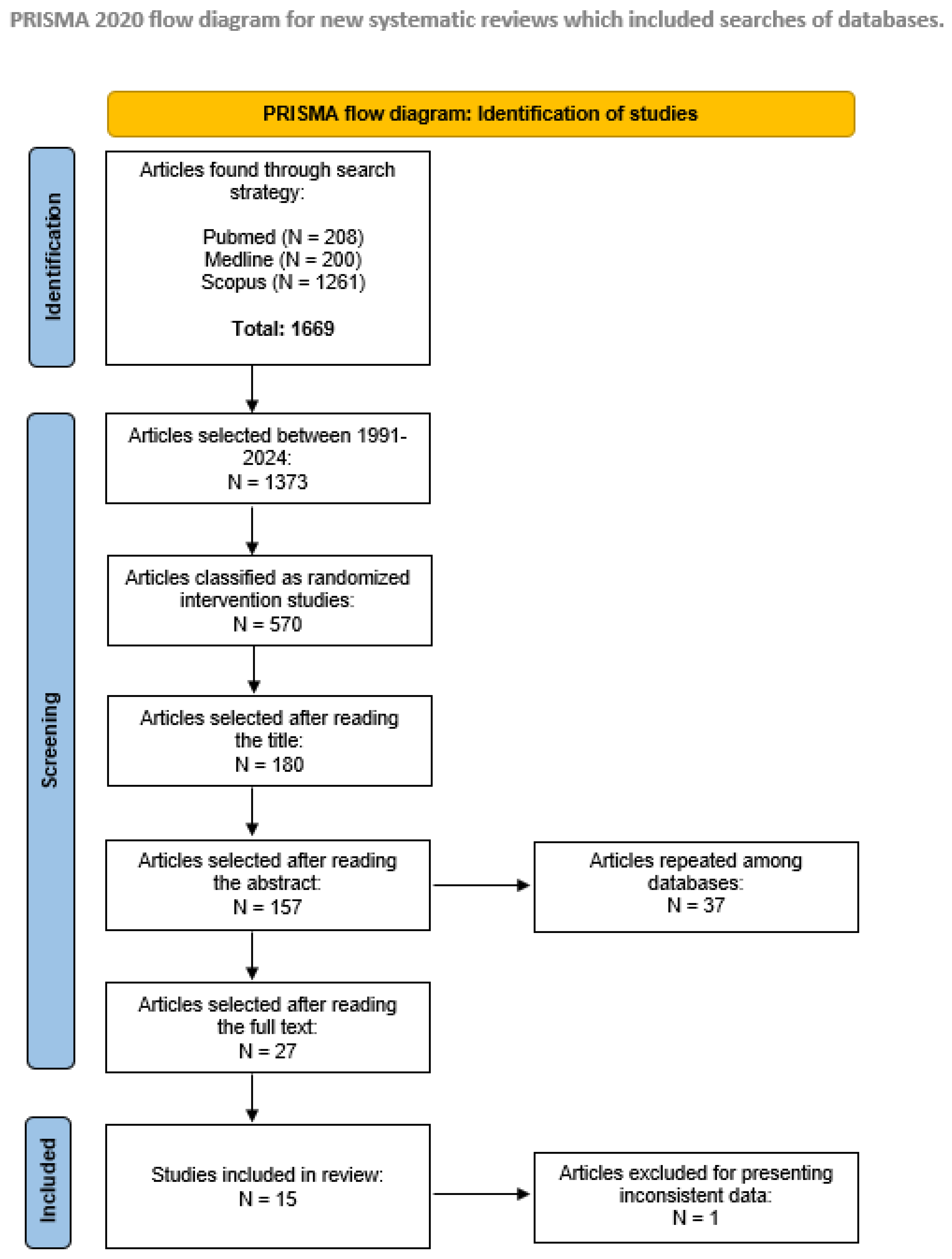
2.1. Literature Search and Selection Criteria
2.2. Outcomes of Interest
- Assessment of motor symptoms: Two-Minute Walk Test (2MWT), 6-Minute Walk Test (6MWT), Berg Balance Scale (BBS); Continuous-Scale Physical Functional Performance Test (CS-PFP), Falls Efficacy Scale International (FES-I), Freezing of Gait Questionnaire (FOG, Functional Reach Test (FRT), Physical Activity Questionnaire (IPAQ), Mini-Balance Evaluation Systems Test (MBEST), Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), Sit-to-Stand Test (STS), Test of Attentional Performance Flexibility (TAPF), Timed Up and Go (TUG).
- Assessment of non-motor symptoms: Fear of Falling Avoidance Behavior Questionnaire (FFABQ), Parkinson’s Disease Non-Motor Symptom Questionnaire (N-MSQ), Parkinson’s Disease Sleep Scale (PDSS), Scales for Outcomes in Parkinson’s Disease (SCOPA)—sleep and gastrointestinal, Parkinson Fatigue Scale (PFS).
- Assessment of affective symptoms: Beck Depression Inventory (BDI), Fatigue Severity Scale (FSS), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), State-Trait Anxiety Inventory (STAI).
- Cognitive assessment: Mini Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Test of Attentional Performance (TAP), Trail Making Test (TMT).
2.3. Data Extraction
3. Results
3.1. Participants
3.2. Medication
3.3. Intervention and Activity Type
3.4. Measurement Tools
3.5. Methodology Quality
3.6. Positive Effects on Outcomes of Interest
4. Discussion
4.1. Physical Activity in Parkinson’s Disease and Its Impact in Quality of Life
4.2. Motor Symptom Benefit
4.3. Non-Motor Symptom Benefits
4.4. Benefits of Integrative and Synergistic Therapy
4.5. Potential Therapeutic Mechanisms
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Durcan, R.; Wiblin, L.; Lawson, R.A.; Khoo, T.K.; Yarnall, A.J.; Duncan, G.W.; Brooks, D.J.; Pavese, N.; Burn, D.J.; ICICLE-PD Study Group. Prevalence and duration of non-motor symptoms in prodromal Parkinson’s disease. Eur. J. Neurol. 2019, 26, 979–985. [Google Scholar] [CrossRef] [PubMed]
- De Pablo-Fernandez, E.; Lees, A.J.; Holton, J.L.; Warner, T.T. Prognosis and neuropathologic correlation of clinical subtypes of Parkinson disease. JAMA Neurol. 2019, 76, 470–479. [Google Scholar] [CrossRef]
- Poewe, W.; Seppi, K.; Tanner, C.N.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 17013. [Google Scholar] [CrossRef] [PubMed]
- Schapira, A.H.V.; Chaudhuri, K.R.; Jenner, P. Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, P.G.; Domingues, D.D.; De Carvalho, L.A.; Allodi, S.; Correa, C.L. Neurotrophic factors in Parkinson’s disease are regulated by exercise: Evidence-based practice. J. Neurol. Sci. 2016, 363, 5–15. [Google Scholar] [CrossRef]
- Kadastik-Eerme, L.; Rosenthal, M.; Paju, T.; Muldmaa, M.; Taba, P. Health-related quality of life in Parkinson’s disease: A cross-sectional study focusing on non-motor symptoms. Health Qual. Life Outcomes 2015, 13, 83. [Google Scholar] [CrossRef] [PubMed]
- DeMaagd, G.; Philip, A. Parkinson’s Disease and Its Management: Part 1: Disease Entity, Risk Factors, Pathophysiology, Clinical Presentation, and Diagnosis. Pharm. Ther. 2015, 40, 504–532. [Google Scholar]
- Huang, X.; Ng, S.Y.E.; Chia, N.S.; Setiawan, F.; Tay, K.Y.; Au, W.L.; Tan, E.K.; Tan, L.C.S. Non-motor symptoms in early Parkinson’s disease with different motor subtypes and their associations with quality of life. Eur. J. Neurol. 2019, 26, 400–406. [Google Scholar] [CrossRef]
- Seppi, K.; Ray Chaudhuri, K.; Coelho, M.; Fox, S.H.; Katzenschlager, R.; Lloret, S.P.; Weintraub, D.; Sampaio, C.; the Collaborators of the Parkinson’s Disease Update on Non-Motor Symptoms Study Group on behalf of the Movement Disorders Society Evidence-Based Medicine Committee. Update on treatments for nonmotor symptoms of Parkinson’s disease—An evidence-based medicine review. Mov. Disord. 2019, 34, 180–198. [Google Scholar] [CrossRef]
- Kriebel-Gasparro, A. Parkinson’s disease: Update on medication management. J. Nurse Pract. 2016, 12, e81–e89. [Google Scholar] [CrossRef]
- Fox, S.H.; Katzenschlager, R.; Lim, S.Y.; Ravina, B.; Seppi, K.; Coelho, M.; Poewe, W.; Rascol, O.; Goetz, C.G.; Sampaio, C. The Movement Disorder Society Evidence-Based Medicine Review Update: Treatments for the motor symptoms of Parkinson’s disease. Mov. Disord. 2011, 26, S2–S41. [Google Scholar] [CrossRef] [PubMed]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [PubMed]
- Marquez, D.X.; Aguiñaga, S.; Vásquez, P.M.; Conroy, D.E.; Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Sheppard, B.B.; Petruzzello, S.J.; et al. A systematic review of physical activity and quality of life and well-being. Transl. Behav. Med. 2020, 10, 1098–1109. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Choi, M.; Yoo, Y. A Meta-Analysis of Nonpharmacological Interventions for People With Parkinson’s Disease. Clin. Nurs. Res. 2017, 26, 608–631. [Google Scholar] [CrossRef]
- Song, R.; Grabowska, W.; Park, M.; Osypiuk, K.; Vergara-Diaz, G.P.; Bonato, P.; Hausdorff, J.M.; Fox, M.; Sudarsky, L.R.; Macklin, E.; et al. The impact of Tai Chi and Qigong mind-body exercises on motor and non-motor function and quality of life in Parkinson’s disease: A systematic review and meta-analysis. Park. Relat. Disord. 2017, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Terrens, A.F.; Soh, S.E.; Morgan, P.E. The efficacy and feasibility of aquatic physiotherapy for people with Parkinson’s disease: A systematic review. Disabil. Rehabil. 2018, 40, 2847–2856. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson’s Disease Questionnaire (PDQ-39): Development and validation of a Parkinson’s disease summary index score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The PDQ-8: Development and validation of a short-form Parkinson’s disease questionnaire. Psychol. Health 1997, 12, 805–814. [Google Scholar] [CrossRef]
- De Boer, A.G.; Wijker, W.; Speelman, J.D.; De Haes, J.C. Quality of life in patients with Parkinson’s disease: Development of a questionnaire. J. Neurol. Neurosurg. Psychiatry 1996, 61, 70–74. [Google Scholar] [CrossRef]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Ellis, T.; Rochester, L. Mobilizing Parkinson’s Disease: The Future of Exercise. J. Park. Dis. 2018, 8, S95–S100. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, M.A.; van Wegen, E.; Newman, M.A.; Heyn, P.C. Exercise-induced increase in brain-derived neurotrophic factor in human Parkinson’s disease: A systematic review and meta-analysis. Transl. Neurodegener. 2018, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Bhalsing, K.S.; Abbas, M.M.; Tan, L. Role of Physical Activity in Parkinson’s Disease. Ann Indian Acad. Neurol. 2018, 21, 242–249. [Google Scholar]
- Feng, Y.S.; Yang, S.D.; Tan, Z.X.; Wang, M.M.; Xing, Y.; Dong, F.; Zhang, F. The benefits and mechanisms of exercise training for Parkinson’s disease. Life Sci. 2020, 245, 117345. [Google Scholar] [CrossRef]
- Palasz, E.; Wysocka, A.; Gasiorowska, A.; Chalimoniuk, M.; Niewiadomski, W.; Niewiadomska, G. BDNF as a Promising Therapeutic Agent in Parkinson’s Disease. Int. J. Mol. Sci. 2020, 21, 1170. [Google Scholar] [CrossRef] [PubMed]
- Szuhany, K.L.; Bugatti, M.; Otto, M.W. A meta-analytic review of the effects of exercise on brain-derived neurotrophic factor. J. Psychiatr. Res. 2015, 60, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.C.; Hwang, D.J.; Koo, J.H.; Um, H.S.; Lee, N.H.; Yeom, D.C.; Lee, Y.; Cho, J.Y. Association of exercise-induced autophagy upregulation and apoptosis suppression with neuroprotection against pharmacologically induced Parkinson’s disease. J. Exerc. Nutr. Biochem. 2018, 22, 1–8. [Google Scholar] [CrossRef]
- Shin, M.S.; Kim, T.W.; Lee, J.M.; Ji, E.S.; Lim, B.V. Treadmill exercise alleviates nigrostriatal dopaminergic loss of neurons and fibers in rotenone-induced Parkinson rats. J. Exerc. Rehabil. 2017, 13, 30–35. [Google Scholar] [CrossRef]
- Son, H.G.; Choi, E.-O. The Effects of Mindfulness Meditation-Based Complex Exercise Program on Motor and Nonmotor Symptoms and Quality of Life in Patients with Parkinson’s Disease. Asian Nurs. Res. 2018, 12, 145–153. [Google Scholar] [CrossRef]
- AHRQ. The Mission, Priority Areas of Focus, Customers, and Background of the Agency for Healthcare Research and Quality (AHRQ). 2021. Available online: https://www.ahrq.gov/cpi/about/index.html (accessed on 2 June 2024).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Landers, M.R.; Navalta, J.W.; Murtishaw, A.S.; Kinney, J.W.; Pirio Richardson, S. A high-intensity exercise boot camp for persons with Parkinson disease: A phase II, pragmatic, randomized clinical trial of feasibility, safety, signal of efficacy, and disease mechanisms. Journal of neurologic physical therapy. J. Neurol. Phys. Ther. 2019, 43, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.; Bhimani, R.; Wyman, J.F.; Konczak, J.; Zhang, L.; Mishra, U.; Terluk, M.; Kartha, R.V.; Tuite, P. Effects of yoga on oxidative stress, motor function, and non-motor symptoms in Parkinson’s disease: A pilot randomized controlled trial. Pilot. Feasibility Stud. 2018, 4, 162. [Google Scholar] [CrossRef] [PubMed]
- Ni, M.; Mooney, K.; Signorile, J.F. Controlled pilot study of the effects of power yoga in Parkinson’s disease. Complement. Ther. Med. 2016, 25, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Ni, M.; Signorile, J.F.; Balachandran, A.; Potiaumpai, M. Power training induced change in bradykinesia and muscle power in Parkinson’s disease. Park. Rel. Disord. 2015, 23, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Schenkman, M.; Hall, D.A.; Barón, A.E.; Schwartz, R.S.; Mettler, P.; Kohrt, W.M. Exercise for people in early- or mid-stage Parkinson disease: A 16-month randomized controlled trial. Phys. Ther. 2012, 92, 1395–1410. [Google Scholar] [CrossRef] [PubMed]
- Haas, A.N.; Delabary, M.D.S.; Passos-Monteiro, E.; Wolffenbuttel, M.; Donida, R.G.; Casal, M.Z.; Zanardi, A.P.J.; Rodrigues, L.P.; Martinez, F.G.; Peyré-Tartaruga, L.A. The effects of Brazilian dance, deep-water exercise and nordic walking, pre- and post-12 weeks, on functional-motor and non-motor symptoms in trained PwPD. Arch. Gerontol. Geriatr. 2024, 118, 105285. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chien, H.F.; Francato, D.C.V.; Barbosa, A.F.; Souza, C.O.; Voos, M.C.; Greve, J.M.D.; Barbosa, E.R. Effects of resistance training on postural control in Parkinson’s disease: A randomized controlled trial. Arq. Neuropsiquiatr. 2021, 79, 511–520. [Google Scholar] [CrossRef]
- Tollár, J.; Nagy, F.; Kovács, N.; Hortobágyi, T. A High-Intensity Multicomponent Agility Intervention Improves Parkinson Patients’ Clinical and Motor Symptoms. Arc. Phys. Med. Rehabil. 2018, 99, 2478–2484. [Google Scholar] [CrossRef]
- Volpe, D.; Signorini, M.; Marchetto, A.; Lynch, T.; Morris, M.E. A comparison of Irish set dancing and exercises for people with Parkinson’s disease: A phase II feasibility study. BMC Geriatr. 2013, 13, 54. [Google Scholar] [CrossRef]
- Collett, J.; Franssen, M.; Meaney, A.; Wade, D.; Izadi, H.; Tims, M.; Winward, C.; Bogdanovic, M.; Farmer, A.; Dawes, H. Phase II randomised controlled trial of a 6-month self-managed community exercise programme for people with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 204–211. [Google Scholar] [CrossRef]
- Wagner, L.; Hauptmann, B.; Hoffmann, A.K.; Jochems, N.; Schmeier, B.; Schrader, A.; Kohlmann, T.; Deck, R. Evaluation of an individualized, tablet-based physiotherapy training programme for patients with Parkinson’s disease: The ParkProTrain study, a quasi-randomised controlled trial. BMC Neurol. 2022, 22, 176. [Google Scholar] [CrossRef] [PubMed]
- van der Kolk, N.M.; Vries, N.M.; Kessels, R.P.; Joosten, H.; Zwinderman, A.H.; Post, B.; Bloem, B.R. Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: A double-blind, randomised controlled trial. Lancet 2019, 18, P998–P1008. [Google Scholar] [CrossRef]
- Kwok, J.Y.Y.; Choi, E.P.H.; Wong, J.Y.H.; Lok, K.Y.W.; Ho, M.-H.; Fong, D.Y.T.; Kwan, J.C.Y.; Pang, S.Y.Y.; Auyeung, M. A randomized clinical trial of mindfulness meditation versus exercise in Parkinson’s disease during social unrest. npj Park. Dis. 2023, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kwok, J.Y.Y.; Kwan, J.C.Y.; Auyeung, M.; Mok, V.C.T.; Lau, C.K.Y.; Choi, K.C.; Chan, H.Y.L. Effects of Mindfulness Yoga vs Stretching and Resistance Training Exercises on Anxiety and Depression for People With Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2019, 76, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Schootemeijer, S.; van der Kolk, N.M.; Ellis, T.; Mirelman, A.; Nieuwboer, A.; Nieuwhof, F.; Schwarzschild, M.A.; de Vries, N.M.; Bloem, B.R. Barriers and Motivators to Engage in Exercise for Persons with Parkinson’s Disease. J. Park. Dis. 2020, 10, 1293–1299. [Google Scholar] [CrossRef]
- International Health Conference. Constitution of the World Health Organization. 1946. Bull. World Health Organ. 2002, 80, 983–984. [Google Scholar]
- Biddiscombe, K.J.; Ong, B.; Kalinowski, P.; Pike, K.E. Physical activity and cognition in young-onset Parkinson’s disease. Acta Neurol. Scand. 2020, 142, 151–160. [Google Scholar] [CrossRef]
- King, L.A.; Wilhelm, J.; Chen, Y.; Blehm, R.; Nutt, J.; Chen, Z.; Serdar, A.; Horak, F.B. Effects of Group, Individual, and Home Exercise in Persons with Parkinson Disease: A Randomized Clinical Trial. J. Neurol. Phys. Ther. 2015, 39, 204–212. [Google Scholar] [CrossRef]
- Gomez-Pinilla, F.; Zhuang, Y.; Feng, J.; Ying, Z.; Fan, G. Exercise impacts brain-derived neurotrophic factor plasticity by engaging mechanisms of epigenetic regulation. Eur. J. Neurosci. 2011, 33, 383–390. [Google Scholar] [CrossRef]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef]
- Sleiman, S.F.; Henry, J.; Al-Haddad, R.; El Hayek, L.; Abou Haidar, E.; Stringer, T.; Ulja, D.; Karuppagounder, S.S.; Holson, E.B.; Ratan, R.R.; et al. Exercise promotes the expression of brain derived neurotrophic factor (BDNF) through the action of the ketone body beta-hydroxybutyrate. eLife 2016, 5, e15092. [Google Scholar] [CrossRef]
- Barber, J.L.; Zellars, K.N.; Barringhaus, K.G.; Bouchard, C.; Spinale, F.G.; Sarzynski, M.A. The Effects of Regular Exercise on Circulating Cardiovascular-related MicroRNAs. Sci. Rep. 2019, 9, 7527. [Google Scholar] [CrossRef]
- Fernandes, J.; Arida, R.M.; Gomez-Pinilla, F. Physical exercise as an epigenetic modulator of brain plasticity and cognition. Neurosci. Biobehav. Rev. 2017, 80, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, F.C.; Rode, M.P.; Vietta, G.G.; Iop, R.D.R.; Creczynski-Pasa, T.B.; Martin, A.S.; Da Silva, R. Expression levels of specific microRNAs are increased after exercise and are associated with cognitive improvement in Parkinson’s disease. Mol. Med. Rep. 2021, 24, 1–10. [Google Scholar] [CrossRef]
- Chaire, A.; Becke, A.; Duzel, E. Effects of Physical Exercise on Working Memory and Attention-Related Neural Oscillations. Front. Neurosci. 2020, 14, 239. [Google Scholar] [CrossRef]
- Pruzin, J.J.; Klein, H.; Rabin, J.S.; Schultz, A.P.; Kirn, D.R.; Yang, H.S.; Buckley, R.F.; Scott, M.R.; Properzi, M.; Rentz, D.M.; et al. Physical activity is associated with increased resting-state functional connectivity in networks predictive of cognitive decline in clinically unimpaired older adults. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2022, 14, e12319. [Google Scholar] [CrossRef] [PubMed]
- van Wijk, B.C.; Beek, P.J.; Daffertshofer, A. Neural synchrony within the motor system: What have we learned so far? Front. Hum. Neurosci. 2012, 6, 252. [Google Scholar] [CrossRef]
- He, X.F.; Liu, D.X.; Zhang, Q.; Liang, F.Y.; Dai, G.Y.; Zeng, J.S.; Pei, Z.; Xu, G.Q.; Lan, Y. Voluntary Exercise Promotes Glymphatic Clearance of Amyloid Beta and Reduces the Activation of Astrocytes and Microglia in Aged Mice. Front. Mol. Neurosci. 2017, 10, 144. [Google Scholar] [CrossRef] [PubMed]
- Kylkilahti, T.M.; Berends, E.; Ramos, M.; Shanbhag, N.C.; Toger, J.; Markenroth Bloch, K.; Lundgaard, I. Achieving brain clearance and preventing neurodegenerative diseases-A glymphatic perspective. J. Cereb. Blood Flow Metab. 2021, 41, 2137–2149. [Google Scholar] [CrossRef]
- Scott-Massey, A.; Boag, M.K.; Magnier, A.; Bispo, D.; Khoo, T.K.; Pountney, D.L. Glymphatic System Dysfunction and Sleep Disturbance May Contribute to the Pathogenesis and Progression of Parkinson’s Disease. Int. J. Mol. Sci. 2022, 23, 12928. [Google Scholar] [CrossRef] [PubMed]
- Si, X.; Guo, T.; Wang, Z.; Fang, Y.; Gu, L.; Cao, L.; Yang, W.; Gao, T.; Song, Z.; Tian, J.; et al. Neuroimaging evidence of glymphatic system dysfunction in possible REM sleep behavior disorder and Parkinson’s disease. npj Parkinson’s Dis. 2022, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Country | Total Number of Participants | Groups | Participants | Mean Age (Years) (SD) | Gender (M:F) | Duration of PD (Years) (SD) | Dropouts | |
|---|---|---|---|---|---|---|---|---|---|
| Haas et al., 2023 [38] | Brazil | 83 | InT | BD | 37 | 71.61 (8.89) | 10:21 | 5.6 (5.09) | 6 |
| DWE | 22 | 66.76 (8.97) | 17:4 | 8.0 (4.65) | 1 | ||||
| NW | 35 | 67.87 (11.2) | 23:8 | 7.0 (5.07) | 4 | ||||
| Kwok et al., 2023 [45] | Hong Kong | 68 | InT-MM | 33 | 62.7 (7.7) | 10:23 | N/A | 2 | |
| Control-SRTE | 35 | 66.1 (8.9) | 19:16 | N/A | 1 | ||||
| Wagner et al., 2022 [43] | Germany | 230 | InT-PTP | 93 | 64.1 (9.3) | 62:30 | 7.75 (6.2) | 15 | |
| Control-MKP | 137 | 67.6 (9.3) | 84:51 | 8.23 (5.1) | 8 | ||||
| Chen et al., 2021 [39] | Brazil | 74 | InT | GG | 23 | 63.4 (6.9) | 17:6 | 7.6 (6) | 2 |
| FG | 26 | 63.2 (6.4) | 18:8 | 8.4 (5.9) | 6 | ||||
| Control-SE | 25 | 63.6 (7) | 18:7 | N/A | 4 | ||||
| Landers et al., 2019 [33] | USA | 27 | InT-HIBC | 14 | 63.5 (10.9) | 10:4 | 4.9 (5.1) | 1 | |
| Control-UC | 13 | 64.6 (6.0) | 9:4 | 4.7 (3.9) | 2 | ||||
| Kwok et al., 2019 [46] | Hong Kong | 138 | Int-YP | 71 | 63.7 (8.2) | 37:34 | N/A | 14 | |
| Control-SRTE | 67 | 63.5 (9.3) | 28:39 | N/A | 8 | ||||
| van der Kolk et al., 2019 [44] | The Netherlands | 130 | Int-AIG | 65 | 59.3 (8.3) | 42:23 | 41 months (16–87) | 4 | |
| Control-ACG | 65 | 59.4 (9.3) | 38:27 | 38 months (19–81) | 1 | ||||
| Cheung et al., 2018 [34] | USA | 20 | InT-HY | 10 | 63.5 (8.5) | N/A | 1–5 yrs = 7 6–10 yrs = 2 11–15 yrs = 1 | 0 | |
| Control-WL | 10 | 65.8 (6.6) | N/A | 1–5 yrs = 4 6–10 yrs = 6 11–15 yrs = 0 | 1 | ||||
| Son et al., 2018 [30] | Republic of Korea | 63 | InT-MMBCEP | 33 | NA | 14:19 | <3 yrs = 21 >3 yrs = 12 | 0 | |
| Control-ROTP | 30 | NA | 9:21 | <3 yrs = 24 >3 yrs = 6 | 3 | ||||
| Tollár et al., 2018 [40] | Hungary | 64 | InT-HIAP | 35 | 67.2 (3.4) | 17:18 | 6.7 (2.3) | 0 | |
| Control-NPICG | 29 | 67.6 (4.1) | 12:8 | 7.1 (2.8) | 9 | ||||
| Collett et al., 2016 [42] | United Kingdom | 105 | InT-EG | 54 | 66 (9) | 31:23 | 4.8 (4.1) | 17 | |
| Control-HG | 51 | 67 (7) | 30:21 | 5.3 (4.1) | 11 | ||||
| Ni et al., 2016 [35] | USA | 27 | InT-YP | 15 | 71.2 (6.5) | 11:4 | 6.9 (6.3) | 2 | |
| Control-UC | 12 | 74.9 (8.3) | 6:6 | 5.9 (6.2) | 2 | ||||
| Ni et al., 2016 [36] | USA | 26 | InT-PWT | 14 | 71.6 (6.6) | 9:5 | 6.6 (4.4) | 0 | |
| Control-CON | 12 | 74.9 (8.3) | 4:6 | 5.9 (6.2) | 2 | ||||
| Volpe et al., 2013 [41] | Italy | 24 | InT-ID | 12 | 61.6 (4.5) | 7:5 | 9.0 (3.6) | N/A | |
| Control-PT | 12 | 65.0 (5.3) | 6:6 | 8.9 (2.5) | N/A | ||||
| Schenkman et al., 2012 [37] | USA | 121 | InT-FBF | 39 | 64.5 (10.0) | 24:15 | 4.9 (3.7) | 6 | |
| InT-AE | 41 | 63.4 (11.2) | 26:15 | 3.9 (4.2) | 10 | ||||
| Control-HEG | 41 | 66.3 (10.1) | 26:15 | 4.5 (3.8) | 9 | ||||
| Study | Intervention | Frequency | Length of Session (Minutes) | Duration of Intervention | JADAD Score |
|---|---|---|---|---|---|
| Haas et al., 2023 [38] | BD vs. DWE vs. NW | 24 sessions | BD: 55–65 DWE: 60 NW: 60 | 3 months | 4 |
| Kwok et al., 2023 [45] | MM vs. SRTE | 1 session per week | MM: 90 SRTE: 90 | 2 months | 4 |
| Wagner et al., 2022 [43] | PTP vs. MKP | Up to 3 sessions per week | NA | 9 months | 4 |
| Chen et al., 2021 [39] | GG vs. FG vs. Control | 2 sessions per week | GG: 50 FG: 50 Control: 50 | 3 + 6 months | 3 |
| Landers et al., 2019 [33] | HIBC vs. Control | 3 sessions per week | HIBC: 90 UC: 60 | 2 months | 5 |
| Kwok et al., 2019 [46] | YP vs Control | 1 session per week | YP: 90 Control: 60 | 2 months | 3 |
| van der Kolk et al., 2019 [44] | AIG vs. Control | 3 sessions per week | AE: 30–45 Control: 30 | 6 months | 5 |
| Cheung et al., 2018 [34] | HY vs. Control | 2 sessions per week | HY: 60 Control: NI | 3 months | 3 |
| Son et al., 2018 [30] | MMBCEP vs. Control | 6 sessions in total | MMBCP: 120 Control: NI | 2 months | 3 |
| Tollár et al., 2018 [40] | HIAP vs. Control | 15 sessions over 3 weeks | HIAP: 60 Control: NI | >1 months | 3 |
| Collett et al., 2016 [40] | EG vs. Control | 2 sessions per week | Exercise: 60 Control: 60 | 6 months | 5 |
| Ni et al., 2016 [35] | YP vs. Control | 2 sessions per week | YP: 60 Control: NDT | 3 months | 3 |
| Ni et al., 2016 [36] | PWT vs. Control | 2 sessions per week | PWT: NDT Control: 60 | 3 months | 3 |
| Volpe et al., 2013 [41] | SPG vs. ID | 1 session per week | SPG: 90 ID: 90 | 1 + ½ month | 2 |
| Schenkman et al., 2012 [37] | FBF vs. AE vs. Control | FBF and AE: 3 sessions per week for 4 months, then once a month for rest of study Control: once a month | AE: 40–50 FBF: NDT Control: NDT Individual sessions: NDT for any intervention | 16 months | 5 |
| Study | Instruments | Variable | Pre-Intervention Mean (SD) | Post-Intervention Mean (SD) | p-Value |
|---|---|---|---|---|---|
| Haas et al., 2023 [38] | PDQ-39 | BD | 34.35 (3.21) * | 32.97 (2.16) * | 0.12 |
| DWE | 34.90 (3.52) * | 35.76 (3.39) * | |||
| NW | 31.87 (2.79) * | 27.77 (2.25) * | |||
| Kwok et al., 2023 [45] | PDQ-8 | MM | NA | 36.26 (17.58) | 0.287 |
| SRTE | NA | 28.17 (15.45) | 0.547 | ||
| Wagner et al., 2022 [43] | PDQ-8 | PTP | 26.8 | 27.5 | <0.01 |
| MKP | 29.8 | 33.0 | |||
| Chen et al., 2021 [39] | PDQ-39—Mobility | GG | 34.72 (24.10) | 25.8 (25.16) | 0.019 |
| FG | 30.52 (22.02) | 24.63 (20.63) | |||
| Control | 23.12 (19.51) | 23.52 (17.97) | |||
| Landers et al., 2019 [33] | PDQ-39 | HIBC | NA | 21.1 ± 5.5 | 0.328 |
| Control | NA | 21.7 ± 5.5 | 0.484 | ||
| Kwok et al., 2019 [46] | PDQ-8 | YP | 9.8 (5.0) | 6.0 (4.8) | <0.001 |
| Control | 9.2 (5.3) | 8.8 (5.5) | |||
| van der Kolk et al., 2019 [44] | PDQ-39 | AIG | 24.9 (2.2) * | 26.0 (2.3) * | 0.910 |
| Control | 24.0 (2.2) * | 26.3 (2.3) * | |||
| Cheung et al., 2018 [34] | PDQUALIF | HY | 55 (15.8) | 55 (15.8) | NA |
| Control | 60 (17.5) | 50 (23.6) | |||
| Son et al., 2018 [30] | PDQL | MMBCEP | 136.27 (30.45) | 153.63 (21.66) | 0.006 |
| Control | 147.83 (24.77) | 139.27 (17.84) | |||
| Tollár et al., 2018 [40] | PDQ-39 | HIAP | 30.0 (8.3) | 23.4 (7.2) | <0.001 |
| Control | 30.6 (15.0) | 30.8 (13.8) | |||
| EQ-5D | HIAP | 0.5 (0.1) | 0.5 (0.1) | <0.05 | |
| Control | 0.4 (0.2) | 0.5 (0.1) | |||
| Collett et al., 2016 [42] | EQ-5D | EG | 76 (15.4) | 76 (2) | 0.903 |
| Control | 75 (15) | 62 (3) | |||
| SF-36 | Physical EG | 64 (18) | 68 (3) | 0.397 | |
| Physical Control | 61 (19) | 74 (2) | |||
| Mental EG | 71 (17) | 58 (3) | 0.470 | ||
| Mental Control | 68 (17) | 66 (3) | |||
| Ni et al., 2016 [35] | PDQ-39 | YP | 44.2 (32.5) | NA | 0.016 |
| Control | 34.2 (16.9) | NA | |||
| Ni et al., 2016 [36] | PDQ-39 | PWT | 39.3 (13.4) | NA | 0.028 |
| Control | 35.2 (20.4) | NA | |||
| Volpe et al., 2013 [41] | PDQ-39 | ID | 30.60 (12.06) | 22.16 (10.18) | 0.153 |
| Control | 32.58 (7.59) | 27.61 (7.67) | |||
| Schenkman et al., 2012 [37] | PDQ-39 | FBF | 23.2 (13.6) | 17.2 (2.1) | 0.64 |
| AE | 18.5 (13) | 17.1 (2.3) | |||
| Control | 21.5 (9.6) | 21.0 (2.2) |
| Study | Instruments | Group | Pre-Intervention Mean (SD) | Post-Intervention Mean (SD) | p-Value | |
|---|---|---|---|---|---|---|
| Haas et al., 2023 [38] | Motor symptoms | MDS-UPDRS III | BD | 14.16 (1.24) | 0.78 | |
| DWE | 16.09 (1.19) | 17.62 (1.46) | ||||
| NW | 14.16 (0.99) | 14.65 (1.18) | ||||
| FES-I | BD | 32.00 (1.62) | 30.35 (1.47) | 0.98 | ||
| DWE | 29.76 (1.89) | 31.95 (2.23) | ||||
| NW | 30.00 (1.69) | 32.13 (1.83) | ||||
| STS | BD | 21.53 (1.76) | 14.04 (0.81) | 0.89 | ||
| DWE | 18.04 (1.77) | 16.77 (1.79) | ||||
| NW | 16.25 (0.86) | 17.34 (1.86) | ||||
| TUG-SSS | BD | 14.93 (1.18) | 11.29 (0.66) | 0.76 | ||
| DWE | 12.22 (0.79) | 12.68 (1.89) | ||||
| NW | 13.56 (1.18) | 13.26 (1.10) | ||||
| TUG-FS | BD | 11.70 (0.97) | 9.06 (0.51) | 0.58 | ||
| DWE | 9.38 (0.53) | 9.62 (1.23) | ||||
| NW | 9.72 (0.59) | 9.7 (0.94) | ||||
| 6MWT | BD | 428.71 (22.81) | 434.14 (16.2) | 0.14 | ||
| DWE | 455.95 (19.22) | 478.32 (22.58) | ||||
| NW | 452.13 (17.73) | 477.91 (17.87) | ||||
| Handgrip test | BD | 43.77 (2.52) | 52.93 (3.81) | 0.01 | ||
| DWE | 57.14 (4.63) | 56.33 (3.82) | ||||
| NW | 61.10 (3.62) | 59.86 (2.72) | ||||
| Non-motor symptoms | MoCA | BD | 21.94 (0.95) | 22.35 (0.83) | 0.06 | |
| DWE | 22.81 (1.33) | 24.4 (0.88) | ||||
| NW | 24.27 (0.69) | 24.06 (0.86) | ||||
| Kwok et al., 2023 [45] | Motor symptoms | MDS-UPDRS III | MM | NA | 32.51 (11.44) | 0.09 |
| SRTE | NA | 32.36 (11.91) | 0.01 | |||
| TUG | MM | NA | 12.61 (6.63) | 0.21 | ||
| SRTE | NA | 12.28 (3.83) | 0.12 | |||
| Non-motor symptoms | HADS—Anxiety | MM | NA | 6.66 (3.80) | 0.60 | |
| SRTE | NA | 6.28 (3.82) | 0.10 | |||
| HADS—Depression | MM | NA | 6.91 (3.26) | 0.11 | ||
| SRTE | NA | 6.29 (3.45) | 0.71 | |||
| MoCA—Visuospatial | MM | NA | 4.11 (1.01) | 0.20 | ||
| SRTE | NA | 4.30 (1.21) | 0.42 | |||
| MoCA—Naming | MM | NA | 2.85 (0.37) | 1.00 | ||
| SRTE | NA | 2.85 (0.50) | 0.57 | |||
| MoCA—Attention | MM | NA | 5.45 (0.64) | 0.44 | ||
| SRTE | NA | 5.52 (0.63) | 0.28 | |||
| MoCA—Language | MM | NA | 2.80 (0.41) | 0.66 | ||
| SRTE | NA | 2.83 (0.46) | 0.32 | |||
| MoCA—Abstraction | MM | NA | 1.43 (0.58) | 1.00 | ||
| SRTE | NA | 1.34 (0.60) | 0.37 | |||
| MoCA—Delayed Recall | MM | NA | 4.10 (1.30) | 0.04 | ||
| SRTE | NA | 3.77 (1.25) | 0.01 | |||
| MoCA—Orientation | MM | NA | 5.96 (0.19) | 0.10 | ||
| SRTE | NA | 5.88 (0.42) | 0.04 | |||
| MoCA—Total | MM | NA | 26.77 (2.61) | 0.01 | ||
| SRTE | NA | 26.70 (3.33) | 0.01 | |||
| Wagner et al., 2022 [43] | Motor symptoms | NA | ||||
| Non-motor symptoms | PDSS | PTP | 17.8 | 18.6 | <0.01 | |
| Control | 19.5 | 20.8 | ||||
| Chen et al., 2021 [39] | Motor symptoms | UPDRS III | GG | 29.13 (10.06) | 27.65 (9.92) | 0.01 |
| FG | 29.58 (12.06) | 28.38 (10.05) | ||||
| Control | 26.44 (9.95) | 27.60 (8.12) | ||||
| TUG | GG | 8.70 (3.39) | 7.91 (2.89) | 0.89 | ||
| FG | 8.5 (2.10) | 7.96 (1.93) | ||||
| Control | 8.56 (1.73) | 8.12 (1.88) | ||||
| BBS | GG | 52.09 (4.5) | 52.96 (2.93) | 0.04 | ||
| FG | 51.00 (4.74) | 52.96 (2.82) | ||||
| Control | 52.28 (2.79) | 52.24 (3.07) | ||||
| MBEST | GG | 24.48 (4.24) | 25.70 (4.24) | 0.01 | ||
| FG | 23.69 (4.71) | 25.69 (3.92) | ||||
| Control | 24.92 (4.14) | 25.04 (3.66) | ||||
| Non-motor symptoms | MMSE | GG | NA | 27.4 (1.9) | 0.53 | |
| FG | NA | 26.9 (2.4) | ||||
| Control | NA | 27.5 (2.1) | ||||
| Landers et al., 2019 [33] | Motor symptoms | IPAQ | Vigorous HIBC | 77.8 (35.9) | 168.9 (116.3) | 1.00 |
| Vigorous Control | 33.3 (20.9) | 86.7 (35.2) | 0.03 | |||
| Moderate HIBC | 86.1 (49.6) | 236.1 (127.2) | 0.004 | |||
| Moderate Control | 85.6 (44.8) | 245.6 (195.9) | 0.22 | |||
| Walk HIBC | 135.6 (42.1) | 333.9 (193.8) | 0.45 | |||
| Walk Control | 312.2 (66.2) | 217.8 (80.9) | 0.07 | |||
| Sit HIBC | 507.8 (81.2) | 453.3 (56.7) | 0.73 | |||
| Sit Control | 363.4 (76.5) | 393.3 (97.1) | 0.75 | |||
| MDS-UPDRS III | On HIBC | 25.8 (4.7) | 16.3 (4.8) | 0.02 | ||
| On Control | 35.6 (4.4) | 24.2 (4.5) | 0.05 | |||
| Off HIBC | 32.3 (5.0) | 23.6 (4.5) | 0.05 | |||
| Off Control | 36.5 (5.3) | 35.0 (4.8) | 0.11 | |||
| FFABQ | HIBC | 8.9 (4.3) | 8.5 (4.0) | 0.15 | ||
| Control | 12.3 (4.0) | 11.6 (3.8) | 0.62 | |||
| 6MWT | On HIBC | 491.9 (32.5) | 515.1 (39.7) | 0.02 | ||
| On Control | 418.3 (48.8) | 440.4 (68.5) | 0.01 | |||
| Off HIBC | 456.7 (42.2) | 484.6 (46.4) | 0.05 | |||
| Off Control | 394.6 (45.1) | 442.7 (49.6) | 0.09 | |||
| STS | On HIBC | 11.5 (2.0) | 12.6 (2.2) | 0.15 | ||
| On Control | 7.3 (1.9) | 9.2 (2.0) | 0.03 | |||
| Off HIBC | 9.1 (1.5) | 11.2 (1.7) | 0.15 | |||
| Off Control | 8.0 (1.6) | 9.6 (1.8) | 0.23 | |||
| Non-motor symptoms | PFS | HIBC | 3.2 (0.4) | 2.8 (0.3) | 0.03 | |
| Control | 2.7 (0.4) | 2.8 (0.3) | 0.21 | |||
| Kwok et al., 2019 [46] | Motor symptoms | MDS-UPDRS III | YP Control | 34.9 (14.9) 31.6 (15.6) | 22.4 (11.3) 23.3 (12.8) | 0.002 |
| TUG | YP Control | 17.5 (16.0) 14.1 (6.0) | 12.4 (6.4) 13.5 (16.4) | 0.99 | ||
| Non-motor symptoms | HADS-anxiety | YP Control | 6.3 (3.6) 5.7 (4.0) | 3.0 (3.1) 5.0 (3.5) | <0.001 | |
| HADS-depression | YP Control | 6.7 (3.4) 6.2 (3.6) | 3.5 (2.8) 6.0 (3.7) | <0.001 | ||
| van der Kolk et al., 2019 [44] | Motor symptoms | MDS-UPDRS III | On AIG | 19.4 (1.8) | 21.2 (2.0) | 0.002 |
| On Control | 17.4 (1.8) | 20.3 (2.0) | ||||
| MDS-UPDRS III | Off AIG | 29.5 (2.7) | 29.0 (2.5) | 0.26 | ||
| Off Control | 27.2 (2.7) | 31.4 (2.5) | ||||
| MDS-UPDRS IV | On AIG | 2.7 (0.6) | 3.3 (0.9) | 0.94 | ||
| On Control | 3.1 (0.6) | 3.6 (0.9) | ||||
| MBEST | AIG | 24.3 (0.6) | 24.4 (0.6) | 0.94 | ||
| Control | 24.2 (0.) | 24.5 (0.6) | ||||
| TUG | AIG | 8.3 (0.5) | 8.2 (0.5) | 0.49 | ||
| Control | 8.7 (0.5) | 8.6 (0.5) | ||||
| 6MWT | AIG | 499.4 (18.2) | 510.6 (17.7) | 0.62 | ||
| Control | 486.4 (18.2) | 492.8 (17.7) | ||||
| Pegboard | AIG | 19.5 (0.9) | 18.8 (0.7) | 0.44 | ||
| Control | 19.6 (0.9) | 19.4 (0.7) | ||||
| Finger tapping | AIG | 65.8 (6.4) | 65.7 (6.4) | 0.54 | ||
| Control | 72.6 (6.4) | 73.3 (6.4) | ||||
| Non-motor symptoms | MoCA | AIG | 26.3 (0.4) | 25.7 (0.5) * | 0.70 | |
| Control | 26·3 (0.4) | 25.9 (0.5) * | ||||
| HADS | Depression score AIG | 4.2 (0.5) | 4.5 (0.6) * | 0.55 | ||
| Depression score Control | 3.6 (0.5) | 4.2 (0.6) * | ||||
| Anxiety score AIG | 4.2 (0.6) | 4.1 (0.5) * | 0.74 | |||
| Anxiety score Control | 5.2 (0.6) | 4.2 (0.5) * | ||||
| SCOPA | AIG sleep day | 3.2 (0.6) | 3.5 (0.6) * | 0.20 | ||
| Control sleep day | 4.1 (0.6) | 3.9 (0.6) * | ||||
| AIG sleep night | 4.4 (0.6) | 4.6(0.6)* | 0.85 | |||
| Control sleep night | 4.6 (0.6) | 4.6 (0.6) * | ||||
| AIG gastrointestinal | 1.6 (0.3) | 1.6 (0.3) * | 0.50 | |||
| Control gastrointestinal | 1.6 (0.3) | 1.5 (0.3) * | ||||
| FSS | AIG | 3.7 (0.2) | 3.7 (0.2) * | 0.52 | ||
| Control | 3.9 (0.2) | 3.7 (0.2) * | ||||
| TMT | AIG Part A | 39.1 (2.9) | 35.5 (2.6) * | 0.29 | ||
| Control Part A | 40.3 (2.9) | 37.9 (2.6) * | ||||
| AIG Part B | 95.0 (9.3) | 83.8 (9.1) * | 0.15 | |||
| Control Part B | 92.2 (9.3) | 90.6 (9.1) * | ||||
| TAPF | AIG | −3.5 (2.2) | −3.6 (1.9) * | 0.71 | ||
| Control | −4.4 (2.2) | −5.6 (1.9) * | ||||
| Cheung et al., 2018 [34] | Motor symptoms | UPDRS III | HY | 25.6 (6.9) | 17 (1.7) * | + |
| Control | 24.4 (7.3) | 22.5 (1.8) * | ||||
| Non-motor symptoms | MoCA | HY | 26.9 (2.2) | 28.1 (0.4) | NA | |
| Control | 26.1 (2.4) | 27.5 (0.4) | ||||
| BDI | HY | 8.8 (5.9) | 8.9 (1.1) | NA | ||
| Control | 7.1 (5.0) | 8.6 (1.2) | ||||
| PDSS | HY | 112.3 (22.2) | 112.2 (4.1) | NA | ||
| Control | 107.2 (23.2) | 106.3 (4.3) | ||||
| Son et al., 2018 [30] | Motor symptoms | 6MWT | MMBCEP | 373.96 (70.03) | 438.68 (60.32) | <0.001 |
| Control | 373.44 (59.47) | 378.46 (59.47) | ||||
| Shoulder suppleness | MMBCEP | 124.93 (18.7) | 137.71 (14.12) | 0.01 | ||
| Control | 129.51 (12.3) | 129.24 (11.81) | ||||
| Chair stand test | MMBCEP | 12.72 (4.69) | 15.23 (4.00) | 0.01 | ||
| Control | 13.61 (4.60) | 12.95 (4.18) | ||||
| 2.45 m walk test | MMBCEP | 6.94 (1.87) | 5.17 (1.67) | <0.001 | ||
| Control | 7.86 (1.92) | 7.45 (1.92) | ||||
| Non-motor symptoms | GDS | MMBCEP | 14.25 (7.53) | 10.85 (6.41) | <0.001 | |
| Control | 17.25 (7.07) | 16.24 (6.07) | ||||
| STAI | MMBCEP State | 40.37 (4.77) | 38.14 (9.33) | <0.001 | ||
| Control State | 40.73 (8.67) | 46.78 (7.79) | ||||
| MMBCEP Trait | 42.63 (5.33) | 38.23 (10.26) | 0.01 | |||
| Control Trait | 41.74 (7.42) | 45.15 (9.06) | ||||
| MoCA | MMBCEP | 22.87 (2.54) | 25.86 (3.17) | <0.001 | ||
| Control | 21.48 (5.13) | 21.44 (5.13) | ||||
| PDSS | MMBCEP | 16.13 (8.17) | 10.14 (4.90) | 0.002 | ||
| Control | 12.63 (6.19) | 14.15 (5.09) | ||||
| Tollár et al., 2018 [40] | Motor symptoms | MDS-UPDRS M-EDL | HIAP | 19.3 (5.5) | 12.0 (3.7) | <0.001 |
| Control | 18.9 (7.9) | 18.6 (7.6) | ||||
| TUG | HIAP | 16.1 (3.7) | 9.9 (2.7) | <0.001 | ||
| Control | 18.6 (4.2) | 18.2 (4.0) | ||||
| Non-motor symptoms | BDI | HIAP | 17.0 (5.3) | 13.9 (5.0) | <0.001 | |
| Control | 18.0 (10.6) | 17.7 (9.8) | ||||
| Collett et al., 2016 [42] | Motor symptoms | MDS-UPDRS III | EG | 16.7 (10.1) | 17.7 (1.1) | + |
| Control | 19.9 (9.9) | 19.2 (1.2) | ||||
| 2MWT | EG | 146.6 (23.9) | 144.6 (2.5) | NA | ||
| Control | 137.7 (22.9) | 137.9 (2.6) | ||||
| TUG | EG | 9.4 (2.0) | 10.1 (0.3) | NA | ||
| Control | 10.1 (2.1) | 10.6 (0.3) | ||||
| Nine-hole peg test | EG | 24.9 (5.4) | 26.2 (0.6) | NA | ||
| Control | 26.8 (5.9) | 25.7 (0.6) | ||||
| Non-motor symptoms | N-MSQ | EG | 8.4 (5.0) | 8.9 (0.4) | NA | |
| Control | 8.6 (4.2) | 8.0 (0.4) | ||||
| FSS | EG | 3.6 (1.4) | 3.6 (0.1) | NA | ||
| Control | 3.9 (1.4) | 3.4 (0.2) | ||||
| Ni et al., 2016 [35] | NA | |||||
| Ni et al., 2016 [36] | Motor symptoms | MDS-UPDRS III | PWT | 32.9 (12.0) | NA | 0.72 |
| Control | 27.6 (7.8) | NA | ||||
| Non-motor symptoms | MMSE | PWT | 29.1 (0.9) | NA | 0.88 | |
| Control | 29.4 (1.1) | NA | ||||
| Volpe et al., 2013 [41] | Motor symptoms | UPDRS III | ID | 24.58 (3.87) | 17.42 (3.85) | <0.001 |
| Control | 23.92 (3.50) | 21.00 (3.07) | ||||
| TUG | ID | NA | NA | 0.007 | ||
| Control | NA | NA | ||||
| BBS | ID | 36.08 (9.20) | 46.08 (6.75) | 0.051 | ||
| Control | 34.08 (9.14) | 38.92 (9.97) | ||||
| FOG | ID | 11.42 (2.78) | 4.92 (2.07) | 0.001 | ||
| Control | 10.75 (3.39) | 10.16 (4.47) | ||||
| Non-motor symptoms | MMSE | ID | 26.5(1.4) | NA | NA | |
| Control | 26.3(1.8) | NA | ||||
| Schenkman et al., 2012 [37] | Motor symptoms | UPDRS III | FBF | 35.5 (13.9) | 23.7 (1.7) | 0.72 * |
| AE | 34.6 (13.0) | 21.9 (1.8) | ||||
| Control | 37.5 (13.7) | 24.2 (1.8) | ||||
| UPDRS Total | FBF | 35.5 (13.9) | 32.6 (2.4) | 0.62 * | ||
| AE | 34.6 (13.0) | 31.4 (2.4) | ||||
| Control | 37.5 (13.7) | 35.6 (2.4) | ||||
| FRT | FBF | 12.9 (3) | 13.6 (0.5) | 0.46 | ||
| AE | 13.6 (3.1) | 13.8 (0.5) | ||||
| Control | 12.5 (3.1) | 13.4 (0.5) | ||||
| CS-PFP | FBF | 48.9 (17.2) | 52.9 (2.4) | 0.221 | ||
| AE | 49.6 (15.4) | 50.5 (2.4) | ||||
| Control | 44.6 (15.9) | 49.6 (2.4) | ||||
| Non-motor symptoms | UPDRS I | FBF | 9.4 (4.9) | 7.6 (0.8) | 0.54 * | |
| AE | 8.5 (4.8) | 7.8 (0.8) | ||||
| Control | 9.6 (4.8) | 9.5 (0.8) | ||||
| MMSE | FBF | 28.8 (1.1) | 28.8 (1.1) | 0.21 | ||
| AE | 28.3 (1.8) | 28.3 (1.8) | ||||
| Control | 28.8 (1.5) | 28.8 (1.5) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bispo, D.P.C.F.; Lins, C.C.S.A.; Hawkes, K.L.; Tripp, S.; Khoo, T.K. The Positive Effects of Physical Activity on Quality of Life in Parkinson’s Disease: A Systematic Review. Geriatrics 2024, 9, 94. https://doi.org/10.3390/geriatrics9040094
Bispo DPCF, Lins CCSA, Hawkes KL, Tripp S, Khoo TK. The Positive Effects of Physical Activity on Quality of Life in Parkinson’s Disease: A Systematic Review. Geriatrics. 2024; 9(4):94. https://doi.org/10.3390/geriatrics9040094
Chicago/Turabian StyleBispo, Dharah P. C. F., Carla C. S. A. Lins, Kelly L. Hawkes, Shae Tripp, and Tien K. Khoo. 2024. "The Positive Effects of Physical Activity on Quality of Life in Parkinson’s Disease: A Systematic Review" Geriatrics 9, no. 4: 94. https://doi.org/10.3390/geriatrics9040094
APA StyleBispo, D. P. C. F., Lins, C. C. S. A., Hawkes, K. L., Tripp, S., & Khoo, T. K. (2024). The Positive Effects of Physical Activity on Quality of Life in Parkinson’s Disease: A Systematic Review. Geriatrics, 9(4), 94. https://doi.org/10.3390/geriatrics9040094